CONTACT TRACING RISK ASSESSMENT PROFILE (CT RAP) FOR PUBLIC GROUND TRANSPORT - RKI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CONTACT TRACING RISK ASSESSMENT PROFILE (CT‐RAP) FOR PUBLIC GROUND TRANSPORT WP 7: Contact Tracing in Ground Transport CONTACT Oliver Mohr, MohrO@rki.de Julia Hermes, HermesJ@rki.de Tim Eckmanns, EckmannsT@rki.de Gérard Krause, KrauseG@rki.de Robert Koch Institute Postfach 65 02 61, 13302 Berlin, Germany
Authors and colleagues supporting this report
Oliver Mohr, Mona Askar, Julia Hermes, Susanne
Schink, Tim Eckmanns, Gabriele Poggensee,
Gérard Krause
Acknowledgements
We would like to thank all PH experts who participated in the expert survey and the consultation
process including the Delphi‐Method, and our colleagues from the department of infectious disease
epidemiology at RKI (Robert Koch Institute) who supported our work. In the following, experts
contributing to REACT WP 7 are named alphabetically.
Preben Aavitsland, Adamma Aghaizu, Lindsey Barr, Christophe Bayer, Dounia Bitar, Katrine Borgen,
Bonita Brodhun, Silke Buda, Mike Catchpole, Ágnes Csohán, Gabriella De Carli, Lena Fiebig, Regina
Görgen, Udo Götsch, René Gottschalk, Walter Haas, Barbara Hauer, Wiebke Hellenbrand, Kojima
Kazunobu, Peter Kreidl, Andrea Kurcz, Heinrich Lehmann, Yanina Lenz, Emily MacDonald, Maria
Martin, Wilhelmine Meeraus, Daniel Menucci, Paulina Miśkiewicz, Philip Monk, Fortune Ncube,
Barbara Pawlak, Garyphallia Poulakou, Marc Salter, Anette Siedler, Corien Swaan, Gail Thomson, Ed
Velasco, Maria Wadl, Ole Wichmann, Andrzej Zielinski
2TABLE OF CONTENTS
CONTACT TRACING RISK ASSESSMENT PROFILE (CT‐RAP) FOR PUBLIC GROUND TRANSPORT............ 1
TABLE OF CONTENTS ............................................................................................................................... 3
ABBREVIATIONS ...................................................................................................................................... 4
EXECUTIVE SUMMARY............................................................................................................................. 5
INTRODUCTION ....................................................................................................................................... 7
Background information ..................................................................................................................... 7
Legal and regulatory issues ................................................................................................................. 7
Objective of the tool ........................................................................................................................... 9
METHODOLOGY..................................................................................................................................... 11
Information gathering....................................................................................................................... 11
Data on European passenger transport............................................................................................ 11
Structured literature review ............................................................................................................. 11
Compilation of pathogen‐specific epidemiological attributes.......................................................... 12
Survey on knowledge and practices on contact tracing............................................................... 13
Structured expert consultations................................................................................................... 13
STRUCTURE AND USE OF THE CT‐RAP................................................................................................... 15
Structure of the tool ......................................................................................................................... 15
Use of the tool................................................................................................................................... 15
Risk Assessment Profile (RAP)........................................................................................................... 15
Principal considerations/requirements ............................................................................................ 15
Example............................................................................................................................................. 16
Tuberculosis ...................................................................................................................................... 21
Factsheet ...................................................................................................................................... 21
Disease specific considerations .................................................................................................... 22
Contact Tracing – Risk Assessment Profile for Tuberculosis ........................................................ 23
Background information............................................................................................................... 24
References “tuberculosis” ............................................................................................................ 32
Meningococcal disease ..................................................................................................................... 37
Factsheet ...................................................................................................................................... 37
Disease specific considerations .................................................................................................... 38
Contact Tracing – Risk Assessment Profile for Meningococcal Disease....................................... 39
Background information............................................................................................................... 40
References “meningococcal disease”........................................................................................... 47
Measles ............................................................................................................................................. 50
Factsheet ...................................................................................................................................... 50
Disease specific considerations .................................................................................................... 51
Contact Tracing – Risk Assessment Profile for Measles * ............................................................ 52
Background information............................................................................................................... 53
References “measles”................................................................................................................... 56
REFERENCES .......................................................................................................................................... 57
3ABBREVIATIONS
CDC Centers for Disease Control and Prevention
CCDR Canada Communicable Disease Report
CSF Cerebrospinal fluid
CT Contact Tracing
CT‐RAP Contact Tracing – Risk Assessment Profile
EAHC Executive Agency for Health and Consumers
ECDC European Centre for Disease Prevention and Control
EC European Commission
EU European Union
Eurostat Statistical Office of the European Union, Luxemburg
HIV Human Immunodeficiency Virus
HEPA High‐Efficiency Particulate Air filter (in passenger aircraft cabin)
HNIG Human Normal Immunoglobulin
HVAC heating, ventilation, air conditioning (a type of ventilation system)
IGRA Interferon‐Gamma Release Assay
IHR (2005) International Health Regulations (year of becoming operative)
MDR‐TB Multidrug‐resistant tuberculosis: defined as resistance to at least isoniazid and rifampin
NICE UK National Institute for Health and Clinical Excellence
PEP Post Exposure Prophylaxis
PH Public Health
PHEIC PH emergency of international concern
RAGIDA Risk assessment guidelines for infectious diseases transmitted on aircraft
RAP Risk Assessment Profile
REACT Response to Emerging infectious disease: Assessment and development of Core capacities and Tools
RKI Robert Koch Institute
SARS Severe Acute Respiratory Syndrome
SSPE Subacute Sclerosing PanEncephalitis
TB Tuberculosis
TST Tuberculin Skin Test
WHO World Health Organization
WP Work Package
XDR‐TB Extensively drug‐resistant tuberculosis; resistance to at least isoniazid and rifampin (i.e. multidrug‐
resistant TB or MDR‐TB) plus resistance to any fluoroquinolones and any of one of the second‐line anti‐
TB injectable drugs: amikacin, kanamycin or capreomycin
VHF Viral Hemorrhagic Fever
4INTRODUCTORY REMARKS
The REACT (Response to Emerging infectious disease: Assessment and development of Core
capacities and Tools) project is a collaborative European project. The project is funded by EAHC
(Executive Agency of Health & Consumer Protection) within the Health Programme 2008‐2013 of the
European Commission.
The general objective of the project is to provide evidence and tools for the response to emerging
public health threats which are likely to be applicable and acceptable throughout the EU for
responding rapidly and co‐ordinately to public health threats in Europe.
The project consortium is composed of five Associated Partners and thirteen Collaborative Partners,
which are predominantly European public health institutes. The REACT project is divided into four
core work packages that target areas of infectious disease control in need of further coordination
throughout Europe. Work package 7, led by the Robert Koch Institute (RKI), was established with the
objective of creating a risk assessment tool to support contact tracing after exposure to infectious
diseases in public ground transport.
EXECUTIVE SUMMARY
The exposure to infectious diseases in public transport may put passengers at risk of infection and of
developing a disease.
Contact tracing (CT) is defined as the identification of persons who may have been exposed to an
infectious disease by another infected person and ensuring that they are aware of their exposure
[compare, e.g., (1;2)].
CT after potential exposure to infectious diseases on international flights is widely discussed (3‐5)
and for specific diseases guidelines determining if it is appropriate to initiate CT of persons exposed
on air crafts are available (3;4;6). For public ground conveyances no recommendations or guidance to
whether contact investigations should be undertaken have yet been published, in addition the
frequency of transmission of communicable diseases during travel by rail or bus/coach remains
largely unknown. However, analysis of European passenger transport data demonstrates that public
ground transport contributes substantially to overall public passenger transport. The potential risk of
infection in this setting can be illustrated by the following two incidents of passengers being exposed
to infectious diseases:
A case of invasive meningococcal disease with fatal outcome in a Swiss student visiting Berlin
(Germany) in 2008 demonstrated how co‐passengers were exposed and put at risk of infection by
joint over‐night travel in the same sleeping compartment as the meningococcal case (7).
Visitors to the FIFA World Cup events in Germany in 2006 were exposed to measles on public
transport travelling between the different competition sites. The largest measles outbreak reported
in Germany led the Pan American Health Organisation (PAHO) and various European national public
health institutes to issue travel warnings for international visitors (8).
This REACT risk assessment tool combines evidence retrieved from scientific literature with expert
knowledge to provide support for decision making by local public health institutions.
Scientific and non‐scientific literature was systematically reviewed in order to find evidence on
infectious disease transmission in ground transport and to evaluate environmental and other
potentially relevant factors for disease transmission. The total number of relevant articles reporting
on disease transmission in ground transport was very low. Publications reported on transmission of
5tuberculosis (TB), meningococcal disease and measles only. In none of the selected articles potential
factors influencing disease transmission were systematically evaluated. Since the comprehensive and
structured literature search revealed only limited evidence of infectious disease transmission on
ground transport, structured expert input was sought for further information gathering. The
integration of expert knowledge into an evidence‐based guidance document for practical use has
proven to be challenging. In order to reach consensus on the potential influences on decision making
we decided to gather expert experience through the Delphi‐Method, a structured survey in multiple
rounds.
On the basis of Osgood’s semantic differential scale proposed in 1957, the REACT project developed
a “Contact Tracing‐Risk Assessment Profile” (CT‐RAP) to be used as a risk assessment tool for the
decision on CT. The results of the expert consultation process (including the Delphi‐Method) are
displayed in the CT‐RAP for TB and meningococcal disease. The CT‐RAP for measles underwent the
same consultation process, but the Delphi‐Method was not applied. The CT‐RAP aims to give a
disease specific overview on relevant epidemiological criteria and their associated values, which are
positioned on scales according to their relevance for decision making on CT. The background
information includes disease specific considerations and fact sheets, and the rationale for the
selection of Epi Criteria related values. Further infectious diseases selected to be relevant for CT on
public ground transport might undergo the same Delphi‐Process for developing further disease‐
specific CT‐RAP’s. This document aims to show the necessary methodological steps in a transparent
manner.
CT of passengers on public ground transport is a resource intensive process, hence it is of importance
to conduct a comprehensive risk assessment of each individual case and setting and take into
account criteria and related values suggested in this guidance document.
Taking into account the logistical hurdles and probable limited effectiveness, few circumstances
considered on a case‐by‐case basis would justify CT in ground transport.
6INTRODUCTION
This document is based on information from the following sources: analysis of European passenger
data, comprehensive and structured literature review, compilation of pathogen specific
epidemiology, structured expert consultations including the application of the Delphi‐Method, and
an expert survey.
Scientific evidence combined with expert experience led to the development of a semi‐quantitative
tool; the rating of values on scales as presented in a CT‐RAP cannot deliver binding recommendations
but provides the public health expert with orientation.
Prior to making the decision to CT on ground transport, epidemiologists should take into account
that the CT‐RAP’s provided in this document cannot cover every aspect or factor potentially
influencing decision making, e.g., the epidemiological situation in each country.
This document describes the tool and its rationale. It focuses on the transmission of infectious
diseases on public ground transport. In the chapter “Methodology” the development of this tool and
the methodical steps used for information gathering are explained. The chapter “Structure and use of
the tool” provides the user with instructions and one virtual example describing one event in public
ground transport related to the exposure to TB demonstrates how to use the CT‐RAP.
Background information
Europe is well connected by public transport networks that allow high mobility. Passengers using
means of public transport may be at risk of infection and disease when they are exposed to
infectious passengers. In 2007, the share of performance in public ground transport such as
bus/coach, tram, metro, and railway of total transport performance of passengers in Europe was
nearly twice as high (15.7%) as the share of air transport performance (8.8%) according to Eurostat
(9). Whereas guidelines exist on CT after exposure to selected infectious diseases during air travel
(6;10), no guidance documents are available on CT for public ground transport.
Legal and regulatory issues
The need for a timely risk assessment of infectious disease incidents with a possible public health
impact and the recommendation to implement CT has been expressed by several international
regulations.
EU Decision 2119
According to the EU decision 2119, Member States “… must provide information on communicable
diseases through the appropriate designated structures and/or authorities, in accordance with
Article 4 of Decision No 2119/98/EC of the European Parliament and of the Council of 24 September
1998 setting up a network for the epidemiological surveillance and control of communicable diseases
in the community (3), which requires timely scientific analysis in order for effective Community
action to be undertaken”.
International Health Regulations
On 15 June 2007, the International Health Regulations (2005) (IHR (2005)) came into effect. This
legally‐binding agreement by 194 countries across the globe, including all Member States of WHO,
provides a new framework to coordinate the management of events that may constitute a public
emergency of international concern (PHEIC). It is meant to improve the capacity of all countries to
detect, assess, notify and respond to public health (PH) threats.
7States Parties to the IHR (2005) must strengthen PH capacities at designated airports, ports and
ground crossings in both routine circumstances and when responding to events that may constitute a
PHEIC.
Health measures implemented by state parties regarding international travel and CT on arrival or
departure of international travellers are addressed in Article 23 of the IHR (2005) as well as in Article
18, which provides detailed advice on WHO recommendations with respect to persons that may be
issued in response to PHEIC. In Article 45, the treatment of personal data in the context of CT is
regulated (please find the legal text of articles 18, 23 and 45 IHR (2005) below).
Article 18, IHR (2005) Recommendations with respect to persons, baggage, cargo, containers,
conveyances, goods and postal parcels
1. Recommendations issued by WHO to States Parties with respect to persons may include the
following advice:
– no specific health measures are advised;
– review travel history in affected areas;
– review proof of medical examination and any laboratory analysis;
– require medical examinations;
– review proof of vaccination or other prophylaxis;
– require vaccination or other prophylaxis;
– place suspect persons under public health observation;
– implement quarantine or other health measures for suspect persons;
– implement isolation and treatment where necessary of affected persons;
– implement tracing of contacts of suspect or affected persons; *
– refuse entry of suspect and affected persons;
– refuse entry of unaffected persons to affected areas; and
– implement exit screening and/or restrictions on persons from affected areas.
Article 23, IHR (2005) Health measures on arrival and departure
Health measures on arrival and departure
1. Subject to applicable international agreements and relevant articles of these Regulations, a
State Party may require for public health purposes, on arrival or departure:
(a) with regard to travellers:
(i) information concerning the traveller’s destination so that the traveller may be
contacted;
(ii) information concerning the traveller’s itinerary to ascertain if there was any
travel in or near an affected area or other possible contacts with infection or
contamination prior to arrival, as well as review of the traveller’s health
documents if they are required under these Regulations; and/or *
(iii) a non‐invasive medical examination which is the least intrusive examination that
would achieve the public health objective;
(b) inspection of baggage, cargo, containers, conveyances, goods, postal parcels and human
remains.
2. On the basis of evidence of a public health risk obtained through the measures provided in
paragraph 1 of this Article, or through other means, States Parties may apply additional
health measures, in accordance with these Regulations, in particular, with regard to a
suspect or affected traveller, on a case‐by‐case basis, the least intrusive and invasive
medical examination that would achieve the public health objective of preventing the
international spread of disease.
3. No medical examination, vaccination, prophylaxis or health measure under these
Regulations shall be carried out on travellers without their prior express informed consent
Highlighting by REACT
8or that of their parents or guardians, except as provided in paragraph 2 of Article 31, and in
accordance with the law and international obligations of the State Party.
4. Travellers to be vaccinated or offered prophylaxis pursuant to these Regulations, or their
parents or guardians, shall be informed of any risk associated with vaccination or with non‐
vaccination and with the use or non‐use of prophylaxis in accordance with the law and
international obligations of the State Party. States Parties shall inform medical practitioners
of these requirements in accordance with the law of the State Party.
5. Any medical examination, medical procedure, vaccination or other prophylaxis which
involves a risk of disease transmission shall only be performed on, or administered to, a
traveller in accordance with established national or international safety guidelines and
standards so as to minimize such a risk.
Article 45, IHR (2005) Treatment of personal data
1. Health information collected or received by a State Party pursuant to these Regulations from
another State Party or from WHO which refers to an identified or identifiable person shall
be kept confidential and processed anonymously as required by national law.
2. Notwithstanding paragraph 1, States Parties may disclose and process personal data where
essential for the purposes of assessing and managing a public health risk, but States Parties,
in accordance with national law, and WHO must ensure that the personal data are:
(a) processed fairly and lawfully, and not further processed in a way incompatible with that
purpose;
(b) adequate, relevant and not excessive in relation to that purpose;
(c) accurate and, where necessary, kept up to date; every reasonable step must be taken to
ensure that data which are inaccurate or incomplete are erased or rectified; and
(d) not kept longer than necessary.
3. Upon request, WHO shall as far as practicable provide an individual with his or her personal
data referred to in this Article in an intelligible form, without undue delay or expense and,
when necessary, allow for correction.
Objective of the tool
It was our objective to develop a tool to facilitate and support the risk assessment and the decision
process of public health officials with regard to the initiation of CT after exposure to TB,
meningococcal disease, and measles on public ground transport.
This document focuses on the methodological approach in order to provide the basis for the
development of specific CT‐RAP’s for further infectious diseases seen as relevant for CT on public
ground transport.
Outlook
For a European application the tool calls for further development by ECDC and may be validated
through an international expert panel, e.g., through a web‐based survey (Delphi‐Method) to reach
consensus.
The methodological approach to develop the CT‐RAP may not only be applied to other infectious
diseases in public ground transport, but also support decision making on CT in other means of
transport (e.g. aircrafts) or settings (schools etc).
910
METHODOLOGY
Information gathering
Information from various sources was collected that substantiate evidence on the likelihood of
transmission of infectious diseases during trips by public ground transport. We obtained information
through the following methods:
Gathering of statistical data on passenger flow on public ground transport in Europe
(Eurostat)
A systematic review of peer‐reviewed scientific literature, non‐scientific literature and grey
literature regarding evidence for infectious disease transmission in public ground
conveyances
A compilation of pathogen‐specific epidemiological attributes for selected diseases
A standardized paper‐based survey with experts in infectious disease epidemiology at two
scientific conferences
Structured expert consultations including the Delphi‐Method with infectious disease
epidemiologists
Data on European passenger transport
We examined European passenger transport data to provide an overview on the scope of passenger
flow in public ground conveyances. Data and statistics on European passenger transport were
obtained and provided by Eurostat (9) and the European Commission Directorate General for Energy
and Transport (11).
Structured literature review
A structured literature review was carried out in order to compile, select, analyse, and evaluate
available publications on the evidence on transmission of infectious diseases followed by CT in public
ground conveyances.
In May and June 2009 a systematic review of scientific literature was carried out using the database
SCOPUS, which is an abstract and citation database of published research and web sources, the
review was updated in December 2010 for the period January 2009 until 13th December 2010. We
searched scientific literature on transmission of infectious diseases and contact tracing in public
ground conveyances. The following keywords were used: “contact tracing”, “contact investigation”,
“passenger tracing”, “infection”, “infectious disease”, “transmission”, “exposure”, “railway”, “bus”,
“school bus”, “coach”, “tram”, “tramway”, “metro”, “subway”, and “underground”. We combined
the means of public ground transport with the following disease or symptom: “tuberculosis”,
“mycobacterium tuberculosis”, “meningitis”, “meningococcal disease”, “avian influenza”, “viral
hemorrhagic fever”, “VHF”, “SARS”, “plague”, “bubonic plague”, “gastroenteritis”, “diarrhea”,
“rubella”, “Lassa fever”, “measles”, “diphtheria”, and “small pox”.
Three reviewers screened all hits for potential relevance to CT and transmission of infectious disease
in public ground transport; English titles, keywords, and/or abstracts of all hits were reviewed. The
full text of each potentially relevant paper was obtained and reviewed for events of infectious
disease transmission followed by CT on public ground transport. The search was limited to studies on
human beings. The following data were retrieved from each study; publication details (year, authors,
11location), means of transport, pathogen, diagnostic tests, number of infected persons, number of
tested contacts, transmission rate, and number of cases with active disease. The publications were
evaluated on factors potentially influencing transmission of infectious disease such as single trip
exposure, cumulative exposure related to repetitive trips (e.g., school bus, commuter bus), duration
of travel, and environmental factors (ventilation and air conditioning systems, seating position,
distance to contact person). Bibliographies of potentially relevant publications were checked for
additional studies.
In a first step titles, abstracts, or both, of all scientific publications were screened to assess relevance
to CT and exposure to infectious diseases in public ground transport. In a second step, potentially
relevant publications were selected; inclusion criteria were events or cases of infectious diseases
where CT in public ground conveyances was undertaken. The full text of each paper was obtained
and evaluated on scientific evidence concerning the transmission of infectious diseases and CT.
Selected data from each study included publication details, means of transport, diagnostic tests,
number of infected persons, number of tested contacts, transmission rate, and number of cases with
active disease.
In addition to the search for scientific publications we performed a structured search for grey and
non‐scientific literature through the search engines Google News, Google Scholar, Genios, and World
News.
Compilation of pathogen‐specific epidemiological attributes
We collected guidelines, position papers, and peer‐reviewed literature on disease‐specific
epidemiological parameters, such as infectiousness of index case during exposure, symptoms of
index case during exposure period, duration of exposure of contact person to index case during
travel, proximity of contact person to index case during exposure in conveyance, quality of contact
between index case and contact person, susceptibility of contact person, administration of Post‐
Exposure Prophylaxis (PEP), and information on environmental factors potentially influencing the
transmission of infectious disease.
12Survey on knowledge and practices on contact tracing
A paper‐based standardised questionnaire was used to gather information on personal experience,
knowledge, best practices, and gaps from infectious diseases epidemiologists concerning CT in public
passenger transport in Europe in a quantitative approach. The survey was piloted at the EuroEpi
conference which took place in Warsaw in August 2009, and distributed at the ESCAIDE conference in
Stockholm in October 2009.
Structured expert consultations
At the 1st General Meeting in Berlin in January 2009 four international experts were nominated for
this work package to provide scientific and technical input. It was decided to select experts covering
a wide range of areas, namely: expert in infectious disease epidemiology working for an international
public health agency, expert in infectious disease epidemiology working for a national European
public health institute, expert in infectious disease epidemiology working for a local public health
institute, expert in security/health issues working for an international public transport association.
The experts participated in two structured round table consultations and work sessions in the frame
of the 1st REACT General Meeting in Berlin in January 2009, the 1st REACT Expert Workshop in London
in March 2009 and the 2nd REACT Expert Workshop in Warsaw in June 2010. In addition to the
nominated work package experts we consulted RKI experts.
Step 1: Selection of infectious diseases
In a first step, we consulted the four nominated experts (1st Expert Workshop) and conducted
a survey in order to gather information enabling us to identify those infectious diseases that
require CT and to define a set of potential factors that might have an influence on the
transmission of infectious diseases in public ground conveyances. It was decided to exclude
food‐borne pathogens and vector‐borne pathogens. The following infectious diseases were
selected: TB, meningococcal disease, viral haemorrhagic fever & Lassa fever, and measles.
Step 2: Selection of criteria & associated values
After the selection of general factors potentially influencing CT during the 1st Expert
Workshop, the factors chosen were then refined and adapted to the specific diseases
selected for the tool. The factors of potential influence were defined as epidemiological
criteria (Epi Criteria) that should be considered in the risk assessment tool. For each of these
Epi Criteria different pathogen specific values were defined based on evidence through
scientific literature and RKI infectious disease expert consultations.
Step 3: Development of the CT‐RAP
We developed a risk assessment tool which aims to visualise criteria/values relevant to
decide whether or not to initiate CT in public ground conveyances in CT after exposure to an
infectious disease. This tool is based on Osgood’s bi‐polar “Semantic differential scale” from
1957 (12). We modified the scale and designed disease specific CT‐RAP’s which include Epi
Criteria and their associated values relevant for CT in public ground transport. For each
infectious disease a disease‐specific CT‐RAP was needed.
13Step 4: Ranking of values through the Delphi‐Method
In cooperation with internal RKI experts, a set of possible values for each Epi Criterion was
defined for TB, meningococcal disease and measles.
For example, the Epi Criterion “proximity of contact person(s) to index case during exposure
in conveyance” for meningococcal disease is characterised by two defined values: “proximity
to index case ≤ 1 metre” or “proximity to index case > 1 metre”. The values were ranked and
then ranged on scales according to their relevance for CT. The the midpoint of each scale
represents a neutral position while the two endpoints represent a high or a low indication on
the decision on whether or not to start CT. If CT‐RAP’s values cluster predominantly around
the neutral midline, there is neither a high nor a low indication for conducting CT.
At the 2nd Expert Workshop in Warsaw in June 2010 international infectious disease experts
nominated at the 1st General Meeting by each of the four work packages of the REACT
project were asked to define the position of values on the scale of the CT‐RAP´s for TB an
meningococcal disease by using the Delphi‐Method – a structured survey in multiple rounds
in order to reach consensus among a panel of experts. The CT‐RAP for measles underwent
the same consultation process, but the Delphi‐Method was not applied. The Delphi‐Method
determines and refines the anonymous judgement of a group of experts. Anonymous
opinions of all members of the group are collected using a formal questionnaire in several
rounds. Each round is followed by a controlled group‐feedback. Finally, the group opinion is
analyzed based on individual opinions of the final round (13). The Delphi‐Method enables a
heterogeneous group of experts to express their collective experience and know‐how (14).
After a first anonymous vote by each expert defining the position of values on the CT‐RAP
scales for a specific disease, the results of the positioning were compiled and presented in
the plenary expert session. A second individual and anonymous voting round offered the
experts the opportunity to rearrange their primary voting on the placement of each value.
Step 5: Adjustments and refinements
To facilitate real‐life application of the tool, the results of the Delphi‐Meetings were adjusted
without compromising the expert input. For example, closely ranked values were combined
to maximise user‐friendliness.
14STRUCTURE AND USE OF THE CT‐RAP
Structure of the tool
This document provides the user with the concept of a risk assessment tool to support decision
making on CT after exposure to TB, meningococcal disease, and measles. The sections dedicated to
the specific diseases in this chapter display disease specific CT‐RAP’s and disease specific
considerations concerning CT. The CT‐RAP’s are followed by disease specific background information
which include fact sheets and the scientific rationale for the selection of Epi Criteria, as well as the
selection and ranking of associated related values.
Use of the tool
The user is invited to chart on the CT‐RAP all available information by selecting the appropriate value
of each Epi Criterion according to the specific event and setting. A single decision algorithm
containing information considered to be decisive whether or not to initiate CT precedes the Epi
Criteria wherever appropriate.
The two endpoints of the bipolar scales represent a high (on the right hand side) or a low (on the left
hand side) indication whether or not to start CT. The values selected may cluster on either side of the
neutral midline or around the midline according to the particular details of the case. If CT‐RAP’s
values are predominantly positioned around the neutral midline, there is neither a high nor a low
indication for conducting CT. If most of the criteria’s values in the CT‐RAP are marked on the right
end of the scale, the result can be interpreted as indication to start the CT process. In contrast,
profiles with predominantly marked values on the left end of the scale indicate an overall low
indication for CT. The whiskers of the values demonstrate the variability of expert opinions defined
through the Delphi‐Method.
The tool may also be used when some criteria/values are not known. We are well aware that
information such as “susceptibility of contact persons”, the “quality of contact between index case
and contact person” or other information may not be available. If there is no information available
on a criterion, the neutral midline scale position of the respective criterion has to be chosen.
The CT‐RAP supports decision making on whether or not to start CT based on the most hazardous
value of each Epi Criterion of any given event, illustrated by an example: Following a situation during
which a young adolescent index case with meningococcal disease has had contacts of varying quality
to other male and female adolescents, including very close interactions as well as brief conversation,
the most closely involved “quality of contact” value should be chosen, which is “contact to oral
secretions”.
This document provides the user with the rationale for the disease specific selection and ranking of
the criteria and associated values potentially relevant for contact investigations in public ground
transport. Further background information is provided through disease specific factsheets. The
rationale combines evidence retrieved from scientific literature, compiled pathogen‐specific
epidemiologic attributes, and expert experience in a transparent manner.
Risk Assessment Profile (RAP)
Principal considerations/requirements
15CT of passengers exposed to infectious diseases during public ground travel should only be
undertaken following a careful risk assessment based on the criteria and values ranked on the scales
of the respective disease specific CT‐RAP.
Feasibility of following up contact persons who have been exposed to an infectious disease during
public ground travel is limited by the anonymous nature of ground transport, where no passenger
data are collected and the potentially poor response among contacts. The results of our survey
targeting infectious disease epidemiologists revealed that the access to contact details of passengers
and access to information of travel (e.g., seating position) were seen as major challenge. CT in public
ground transport requires human and financial resources and might be time‐consuming as well.
When deciding on CT the means of public ground transport has to be considered. Especially short‐
distance transport in urban settings makes contact investigations impracticable.
Results of the REACT expert consultations suggest that political and media interest may influence or
trigger decision making on CT in any specific setting, even though the importance of those criteria is
regarded as limited. We could not retrieve scientific publications describing political or media
influence on CT in public transport.
To our knowledge, specific guidelines or guidance documents on CT in public ground travel do not
exist. Where applicable we cited guidelines and/or guidance documents on CT in aircrafts assuming
that the risk of infectious disease transmission in public ground transport is at least not lower than in
air travel (15‐17).
Through the Delphi‐Method some of the values were positioned around the neutral midline of the
CT‐RAP indicating limited relevance for decision making.
Example
In order to demonstrate the correct use of the CT‐RAP, let us consider a case of TB exposure during a
bus trip requiring the decision on whether or not to initiate CT:
A group of 38 residents of Strasbourg (France) goes on a day‐trip to the world famous Christmas
market at Nuremberg (Germany). They spend the day (approx. 6 h) roaming the market in small
groups; the round trip on the bus takes a total of approximately 9.5 h. While on the bus, the group
enjoys a sing along of Christmas carols. All passengers remain in their assigned seats throughout the
trip. A 69 year‐old male passenger falls ill five days after the trip and is diagnosed with sputum smear
positive TB another 12 days later.
Example ‐ Information summary
Index patient:
• Sputum smear positive TB
• 69 year‐old male, otherwise healthy during the previous 12 months
• Onset of symptoms: five days after the trip
• Diagnosis: 17 days after the trip (today)
• His wife and 4 year‐old grandson (both on the trip) are currently being examined
Group characteristics and additional information:
• Group size: 39 persons (38 passengers including index case, 1 bus driver)
• Time spent in bus: 9.5 hours
16• Activity: conversation, singing
• Age range: 10 months ‐ 82 years
• No information available on individuals’ health status
• The bus is equipped with central heating, the windows remained closed
• The travel agent keeps a list of contact addresses, including telephone numbers
Example ‐ Applying the particularities of the case to the CT‐RAP
Having gathered above facts about the index patient, situation and possible contact persons, we
enter the information into the CT‐RAP for TB in the following three steps:
a) First, the algorithm assesses potential knock‐out criteria.
b) If the question of whether or not initiate CT continues to be pertinent, please continue by
selecting the appropriate value for each criterion by adding a tick mark. In case there is
information missing, please mark the “Neutral Position” instead.
For the particular circumstances of the bus trip, the following values (in bold) were selected:
1) SYMPTOMS OF THE INDEX CASE DURING EXPOSURE PERIOD (SYM)
Please select the value presenting the worst symptom during exposure
Sym (I) Cough
Sym (II) Unspecific symptoms OR asymptomatic
2) INFECTIOUSNESS OF INDEX CASE DURING EXPOSURE (INF)
Please select the most infectious value
Inf (I) No treatment OR inadequate drug treatment OR < 2 weeks of adequate
drug treatment
Inf (II) > 2 weeks of appropriate drug treatment and improvement of symptoms
in the absence of any suspicion or proof of multidrug resistant TB
3) DRUG RESISTANCE PATTERN OF INDEX CASE (R)
Please select the drug resistance pattern
We have no information on the drug resistance pattern of our index patient (yet), thus
we mark the “neutral position”.
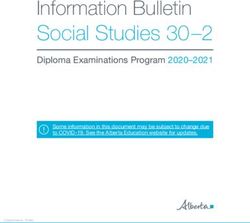
The CT‐RAP for TB will thus look as follows:
17CT-RAP: Tuberculosis
Does the
No index patient have
contact
tracing NO infectious pulmonary
TB?
YES
Please continue CT-RAP
Low Indication for CT Neutral Position High Indication for CT
1. Symptoms of index case during exposure (Sym)
Please select the value representing the worst symptom during exposure
Sym (I) Cough
Sym (II) Unspecific symptoms OR
asymptomatic Sym (II) Sym (I)
2. Infectiousness of index case during exposure (Inf)
Please select the most infectious value
Inf (I) No treatment OR inadequate
drug treatment OR < 2 weeks
of adequate drug treatment
Inf (II) > 2 weeks of appropriate drug
treatment and improvement
of symptoms in the absence of
any suspicion or proof of Inf (II) Inf (I)
multidrug resistant TB
3. Drug resistance pattern of index case (R)
Please select the drug resistance pattern no information
R (I) Extensively drug-resistant
pulmonary TB OR multidrug
R (II)
resistant pulmonary TB
Pulmonary TB without drug
R (II) R (I)
resistance
Please continue with the remaining items in a likewise manner completing the CT‐RAP as best as
possible with the information that is available to you.
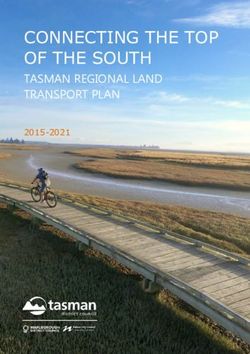
18c) Next, draw a line linking all values that were just selected.
The CT‐RAP will look as follows:
CT-RAP: Tuberculosis
Does the
No index patient have
contact
tracing NO infectious pulmonary YES
TB?
Please continue CT-RAP
Low Indication for CT Neutral Position High Indication for CT
1. Symptoms of index case during exposure (Sym)
Please select the value representing the worst symptom during exposure
Sym (I) Cough
Sym (II) Unspecific symptoms OR
asymptomatic Sym (II) Sym (I)
2. Infectiousness of index case during exposure (Inf)
Please select the most infectious value
Inf (I) No treatment OR inadequate
drug treatment OR < 2 weeks
of adequate drug treatment
Inf (II) > 2 weeks of appropriate drug
treatment and improvement
of symptoms in the absence of
any suspicion or proof of Inf (II) Inf (I)
multidrug resistant TB
3. Drug resistance pattern of index case (R)
Please select the drug resistance pattern no information
R (I) Extensively drug-resistant
pulmonary TB OR multidrug
R (II)
resistant pulmonary TB
Pulmonary TB without drug
R (II) R (I)
resistance
4. Transmission to other contact person(s) (Trans)
Please select the value representing any evidence of transmission no information
Trans (I) Evidence of transmission
Trans (II) No evidence of transmission
Trans (II) Trans (I)
5. Quality of contact between index case and contact person(s) (Q)
Please select the value representing the closest interaction
Q (I) Face-to-face conversation with
Q (II)
index case
No social interaction
Q (II) Q (I)
6. Proximity of contact person(s) to index case during exposure (Prox)
Please select the closest distance of any passenger to the index case
Prox (I)
Prox (I) Proximity ≤ 1 m
Prox (II) Proximity > 1 m
Prox (II)
7. Duration of exposure of contact person(s) to index case (Dur)
Please select the longest duration of contact between any passenger and the index case
Dur (I) Duration ≥ 8 h
Dur (II) Duration < 8 h
Dur (II) Dur (I)
8. Susceptibility of contact person(s) (Sus)
Please select the value representing the most susceptible individual among the passengers
Sus (I) < 5 years of age, HIV
infection, substance abuse,
silicosis, diabetes mellitus,
immunosuppressive treatment
Sus (II) Sus (I)
Sus (II) Immunocompetent
9. Environmental factors in means of transport (E)
Please select the value representing the environmental factors
E (I) No external ventilation (with or E (I)
E (II)
without circulation)
External ventilation (with air
exchange) E (II)
Low Indication for CT Neutral Position High Indication for CT
19Example ‐ Outcome:
The connecting line of the CT‐RAP encourages us to consider CT. Although we lack information on
two criteria (“Drug resistance pattern”, “Transmission to other person(s)”), several other criteria
favour to follow‐up on this incident, namely the prolonged contact time in a relatively confined,
poorly ventilated space and the fact that we know of susceptible persons among the passengers (at
least one 10 month‐old child, unknown health status of all others).
20Tuberculosis
Factsheet
Etiological agent
Mycobacterium tuberculosis
Transmission
Transmission of TB occurs through airborne transmission via inhalation of “droplet nuclei” (1‐5 µm).
Risk of transmission is highest in smear positive pulmonary TB, whereas smear negative/culture
positive cases are less infectious.
Infectiousness
A person needs to inhale a sufficient number of Mycobacterium tuberculosis bacilli to be infected.
Infectiousness is related to the presence of cough and sputum (18) and the number of bacilli in the
sputum (19‐21). The extent and character of the pulmonary lesions determine the number of bacilli
reaching the air passages. Cavitary pulmonary TB results in the release of a larger number of bacilli
(22;23).
Incubation period
A median incubation period of about six weeks is required for a first manifest immunological
response, e.g. a positive Tuberculin Skin Test (TST) or IGRA (Interferon‐Gamma Release Assay) test
(24). The risk of progression to tuberculosis is highest in the first two years after infection.
Morbidity
The WHO estimates that up to one‐third of the world's population is infected with the TB bacillus
(25). In immunocompetent persons approximately 10% of people who are infected with TB bacilli
develop active TB at some time during their life. Reports suggest that 1 in 7.8 contacts will develop
active TB without prophylaxis (26). Left untreated, each person with active infectious TB disease is
estimated to infect on average between 10 and 15 people every year (25).
Mortality
In 2009, there were globally an estimated 1.7 million deaths from TB (including 380,000 people with
HIV, equal to 4,700 deaths a day) (27;28). Concerning Europe, TB mortality rates in recent years
mirrored notification rates in their geographical distribution across European countries (2008:
EU/EEA: 1.8/100,000, WHO Euro Region: 7.6/100,000) (29).
Incidence & prevalence
In 2009, there were an estimated 9.4 (range 8.9 million – 9.9 million) million incident cases of TB
(including 1.1 million cases among people with HIV). The estimated global incidence rate fell to 137
cases per 100,000 population in 2009, after peaking in 2004 at 142 cases per 100,000. There were an
estimated 14 million prevalent cases (range, 12 million–16 million) (27;28). Across the European
Region 461,645 TB cases (52.2 per 100,000 population) were reported in 2008 by 50 of the 54
countries of the European Region representing approximately 6% of TB cases reported worldwide to
WHO (30).
MDR and XDR Tuberculosis
Multidrug‐resistant TB (MDR‐TB) is a form of TB resistant to at least the two most important first‐line
anti TB drugs rifampicin and isoniazid. MDR‐TB is difficult and expensive to treat. Patients remain
infectious for longer and rates of default, failure and death are higher. Extensively drug‐resistant TB
(XDR‐TB) occurs when resistance to the most efficient second‐line drugs develops on top of MDR‐TB
21(additional resistance to one of the fluoroquinolones and one of the i.v. second line drugs amikacin,
kanamycin or capreomycin). XDR‐TB decreases chances of survival and successful treatment further.
There were an estimated 500,000 new MDR‐TB cases in 2007 worldwide. Just over 1% of cases are
estimated to have received treatment in 2008 based on WHO's recommended standards. 5% of all TB
cases are estimated to have MDR‐TB. Based on data from more than 100 countries collected during
the last decade, 27 countries account for 85% of all MDR‐TB cases. XDR‐TB has been found in 57
countries to date. In 2008, WHO reported the highest rates of MDR‐TB ever recorded, with peaks of
up to 22% in new TB cases in some settings of the former Soviet Union. In the same region, 1 in 10
cases of MDR‐TB is XDR‐TB (31).
Disease specific considerations
No specific guidelines on CT in public ground transport linked to the transmission of TB were found.
CT should only be considered when the index case has confirmed infectious pulmonary TB. Infectious
pulmonary TB is defined as culture or molecular probe confirmed case with positive sputum smear
microscopy (including induced sputum or bronchoalveoloar lavage) and the time elapsed between
exposure and diagnosis of the case is shorter than three months (5).
Transmission from children younger than 10 years old is unusual due to the fact that children rarely
present with productive cough and sputum smear‐positivity, although it has been reported in
association with the presence of pulmonary forms of the disease typically reported in adults (32).
22Contact Tracing – Risk Assessment Profile for Tuberculosis
CT-RAP: Tuberculosis
Does the
No index patient have
contact
tracing NO infectious pulmonary YES
TB?
Please continue CT-RAP
Low Indication for CT Neutral Position High Indication for CT
1. Symptoms of index case during exposure (Sym)
Please select the value representing the worst symptom during exposure
Sym (I) Cough
Sym (II) Unspecific symptoms OR
asymptomatic Sym (II) Sym (I)
2. Infectiousness of index case during exposure (Inf)
Please select the most infectious value
Inf (I) No treatment OR inadequate
drug treatment OR < 2 weeks
of adequate drug treatment
Inf (II) > 2 weeks of appropriate drug
treatment and improvement
of symptoms in the absence of
any suspicion or proof of Inf (II) Inf (I)
multidrug resistant TB
3. Drug resistance pattern of index case (R)
Please select the drug resistance pattern
R (I) Extensively drug-resistant
pulmonary TB OR multidrug
resistant pulmonary TB
R (II) Pulmonary TB without drug R (II) R (I)
resistance
4. Transmission to other contact person(s) (Trans)
Please select the value representing any evidence of transmission
Trans (I) Evidence of transmission
Trans (II) No evidence of transmission
Trans (II) Trans (I)
5. Quality of contact between index case and contact person(s) (Q)
Please select the value representing the closest interaction
Q (I) Face-to-face conversation with
index case
Q (II) No social interaction Q (II) Q (I)
6. Proximity of contact person(s) to index case during exposure (Prox)
Please select the closest distance of any passenger to the index case
Prox (I)
Prox (I) Proximity ≤ 1 m
Prox (II) Proximity > 1 m
Prox (II)
7. Duration of exposure of contact person(s) to index case (Dur)
Please select the longest duration of contact between any passenger and the index case
Dur (I) Duration ≥ 8 h
Dur (II) Duration < 8 h
Dur (II) Dur (I)
8. Susceptibility of contact person(s) (Sus)
Please select the value representing the most susceptible individual among the passengers
Sus (I) < 5 years of age, HIV
infection, substance abuse,
silicosis, diabetes mellitus,
immunosuppressive treatment
Sus (II) Sus (I)
Sus (II) Immunocompetent
9. Environmental factors in means of transport (E)
Please select the value representing the environmental factors
E (I) No external ventilation (with or E (I)
without circulation)
E (II) External ventilation (with air
exchange) E (II)
Low Indication for CT Neutral Position High Indication for CT
23Background information
Facts on TB relevant for CT in public ground transport were retrieved from various sources such as
scientific publications on contact investigations, reviews, publications, books, guidelines, REACT
surveys, REACT expert consultations, and other documents (e.g., recommendations or position
papers from institutions such as WHO, CDC, RKI).
1 SYMPTOMS OF INDEX CASE DURING EXPOSURE (SYM)
Ranking on the scale
I. Cough
II. Unspecific symptoms such as weakness or fatigue, weight loss, no appetite,
chills, fever, night sweats OR asymptomatic
Rationale for the ranking
Symptoms of TB depend on where the bacterial growth occurs. Usually tuberculosis bacteria grow in
the lungs; pulmonary TB may cause symptoms such as a cough that lasts three weeks or longer, pain
in the chest, as well as coughing up blood or sputum. Other symptoms are: weakness or fatigue,
weight loss, no appetite, chills, fever and night sweats. Symptoms of TB disease located in other parts
of the body depend on the area affected (33). The level of infectiousness is related to the patient’s
ability to aerolize bacilli and to the number of bacilli that are aerolized (19‐21) and the presence of
cough (18), which is of practical relevance for the transmission for M. tuberculosis. Respiratory
manoeuvres such as coughing, sneezing, talking, and singing produce aerosols. The larger the
physical force of the manoeuvre, the higher the number of expelled droplets and the smaller their
size, the quicker they evaporate to droplet nuclei (34‐36). The extent and character of the pulmonary
lesions decisively determines the number of bacilli reaching the air passages. Cavitary pulmonary TB
results in the release of larger number of bacilli (6). A study demonstrated that culture‐positive
cough aerosols in patients with pulmonary TB were associated with cough frequency (37). With
limited exceptions, only patients with bacteriologically confirmed pulmonary TB can transmit their
infections with smear‐positive cases (acid‐fast bacillus can be seen under the microscope)
being more contagious than smear‐negative but culture‐positive cases (when bacterial load
is not large enough for bacteria to be seen in the sputum without prior growing on special
media) (32;38).
Source
The definition and ranking of values of the Epi Criteria “symptoms of index case during exposure” in
the pictorial profile is based on information from the following sources:
Scientific publications on events/contact investigations in ground conveyances
Scientific reviews, publications, and books
Disease specific or general guidelines
REACT Expert Consultation & REACT Survey
Other documents (recommendations, position papers)
24You can also read