Corporate Presentation - Targeted Medicines for the Ear - Investor Relations ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Targeted Medicines for the Ear
Corporate Presentation
May 7, 2020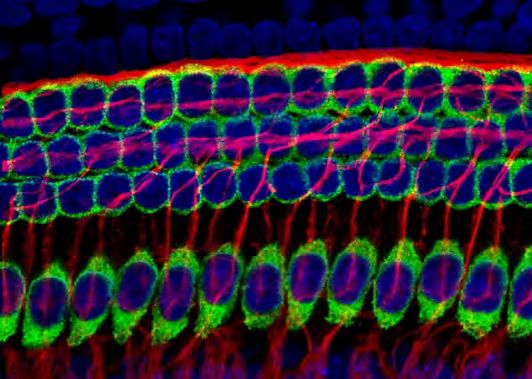
Forward-Looking Statements
Safe Harbor Statement
These slides and the accompanying oral presentation (the “Presentation”) contain forward-looking statements within the meaning of the Private Securities Litigation
Reform Act of 1995. Forward-looking statements generally relate to future events or future financial or operating performance of Otonomy, Inc. (“Otonomy”). Forward-
looking statements in this Presentation include, but are not limited to, statements relating to timing of results, patient recruitment, trial design, and conduct of ongoing
clinical trials; expectations regarding an additional trial needed for registration and FDA approval; expectations regarding market opportunity, development activity and
potential benefits of pre-clinical and clinical programs; expectations regarding the potential benefits and opportunities of, and activity under, the collaboration
agreement between AGTC and Otonomy; and expectations regarding operating expenses for 2020 and cash runway. Otonomy’s expectations regarding these matters
may not materialize, and actual results in future periods are subject to risks and uncertainties. Actual results may differ materially from those indicated by these
forward-looking statements as a result of these risks and uncertainties, including but not limited to: delays and disruption resulting from the COVID-19 pandemic and
governmental responses to the pandemic, including current and future impacts to Otonomy’s operations, the manufacturing of its product candidates, the progression
of its current clinical trials, enrollment in its current and future clinical trials and patient conduct and compliance; Otonomy’s ability to accurately forecast financial
results; Otonomy’s ability to obtain additional financing; Otonomy’s dependence on the regulatory success and advancement of its product candidates; the
uncertainties inherent in the drug development process, including, without limitation, Otonomy’s ability to adequately demonstrate the safety and efficacy of its product
candidates, the nonclinical and clinical results for its product candidates, which may not support further development, and challenges related to patient enrollment in
clinical trials; the integrity of patient-reported outcomes in its current and future clinical trials; the risks of the occurrence of any event, change or other circumstances
that could give rise to the termination of the collaboration agreement between AGTC and Otonomy, or that could impact Otonomy’s ability to repay or comply with the
terms of the loan provided by Oxford Finance LLC; side effects or adverse events associated with Otonomy's product candidates; Otonomy’s ability to successfully
commercialize its product candidates, if approved; competition in the biopharmaceutical industry; Otonomy’s dependence on third parties to conduct nonclinical studies
and clinical trials, to supply raw materials, and for the manufacture of its product candidates; Otonomy’s ability to protect its intellectual property related to its product
candidates in the United States and throughout the world; expectations regarding potential therapy benefits, market size, opportunity, and growth; expectations
regarding, and risks and challenges that could impact reimbursement; Otonomy’s ability to manage operating expenses; implementation of Otonomy’s business model
and strategic plans for its business, products and technology; general economic and market conditions; and other risks. Information regarding the foregoing and
additional risks may be found in the section entitled "Risk Factors" in Otonomy’s Annual Report on Form 10-K filed with the Securities and Exchange Commission (the
"SEC") on February 27, 2020, Otonomy’s Quarterly Report on Form 10-Q filed with the SEC on May 7, 2020, and Otonomy’s future reports to be filed with the SEC.
This Presentation is dated as of May 7, 2020 and based on information available to Otonomy as of that date, and Otonomy undertakes no obligation to update any
forward-looking statements, whether as a result of new information, future events or otherwise, except as required by applicable law.
2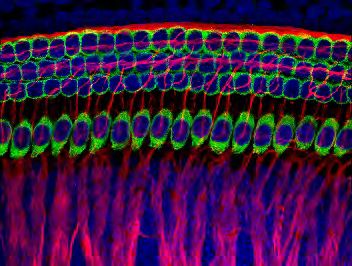
Otonomy is the Leader in Neuroscience for the Ear
Large number of Significant unmet Local delivery is Value creation through
patients impacted by need with high disease essential for effective ADVANCING
neurotology conditions burden and drug treatments MULTIPLE
1 IN 8 WITH NO FDA SUSTAINED- PROGRAMS
MODERATE TO APPROVED EXPOSURE TO CLINICAL
SEVERE DRUG TECHNOLOGY CATALYSTS
HEARING LOSS, TREATMENTS PIONEERED BY
TINNITUS, OR OTONOMY
VERTIGO1
1ClearView Healthcare Partners analysis 3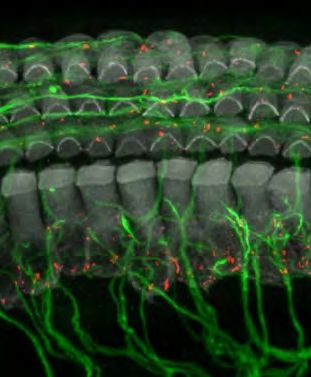
Broadest Pipeline Targeting Largest Market Opportunities
Note: program updates
including timeline to Vertigo OTIVIDEX®: successful Phase 3 trial completed;
trial results to be ~11 M additional Phase 3 trial ongoing
provided in June 2020
Total Market Potential Tinnitus OTO-313: Phase 1/2 trial ongoing;
by Condition1: ~7.8 M patient enrollment completed
~39 M in U.S.
OTO-413: Phase 1/2 trial ongoing
Hearing Preclinical Programs:
Loss • OTO-510 for cisplatin-induced hearing loss
~20.5 M • OTO-6XX for severe hearing loss
• Gene Tx collaboration for congenital hearing loss
1ClearView Healthcare Partners analysis based on patients with moderate to severe symptoms 4
Otonomy Driving Neurotology Towards Market Inflection Point
Local Drug Delivery Revolutionized
Treatment of Retinal Disorders and Similar Market Opportunity for
Created Blockbuster Market Treatment of Neurotology Conditions
# of Intravitreal • Intratympanic (IT) delivery provides high inner ear
Injections (in M) > $10B Global Market drug level and minimizes systemic exposure
3.5
3.0 • Otonomy pioneered sustained-exposure formulation
2.5 technology that is key to IT drug delivery
2.0
• Simple, office-based procedure already performed
1.5 by many ENTs using steroid solutions off-label
1.0
• Opportunity to establish SOC treatments beginning
0.5
with OTIVIDEX for Ménière’s Disease
0.0
2000 2005 2010 2015
Source: Medicare 5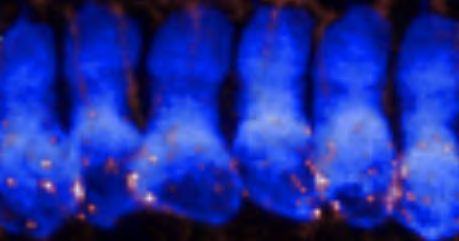
Ménière’s Disease is Chronic, Debilitating Condition
Severe vertigo attacks plus hearing loss and tinnitus
Typical patient High disease burden: No FDA approved
diagnosed in their
Significantly impacts drug treatments
40’S AND 50’S quality of life and work patients treated with low salt diet
(i.e., working parent age) and diuretics (no data), off-label
productivity1,2,3 use of oral and repeat IT steroids
1Tyrrell, et. al. Ear & Hearing. (2016); 2Anderson, John & Harris, Jeffrey. Otology & Neurotology. (2001); 3Arroll, et. al. Otology & Neurotology. (2012) 6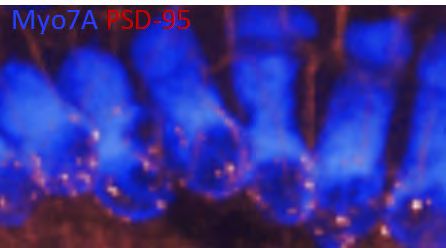
OTIVIDEX: Successful Phase 3 Study Completed (AVERTS-2)
% Reduction in Vertigo Frequency
From Baseline to Month 3
• Single IT injection of sustained-
Change In Mean 80%
exposure dexamethasone
Monthly Definitive 60% formulation
Vertigo Days (DVD)
40%
68% • p value = 0.029 for primary
10 Placebo 20% 40% endpoint (all 174 patients enrolled)
OTIVIDEX 0%
8 • Statistical significance for multiple
Placebo OTIVIDEX
secondary endpoints
6
2.5 day Responder Analysis
80%
lower • AVERTS-1 trial in U.S. did not
4 than
placebo 60% achieve statistical significance due
2 6.2 day clinical to high placebo response
benefit for 40% 73%
OTIVIDEX group 59% • FDA Type C meeting completed:
0 55%
Baseline Month 1 Month 2 Month 3 20% 36% 38% one additional trial for registration
21%
0%
≥ 50% ≥ 75% 100%
reduction reduction reduction
Note: Definitive Vertigo Day (DVD) is a day with at least one vertigo episode lasting a minimum of 20 minutes 7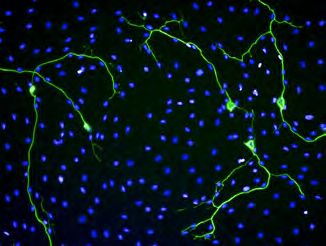
Consistent Vertigo Results Across Multiple OTIVIDEX Trials
% Reduction in Vertigo Frequency From Baseline to Month 3
2.7 days 1.4 days 2.6 days 2.5 days Reduction in Monthly DVDs
vs. Placebo in Month 3
80% p = 0.002
p = 0.030 p = 0.014
60%
Placebo response = 40-43%
40% except for AVERTS-1
73% 73%
68%
61% 58%
55%
20% 42% 43% 43% 40% Placebo
OTIVIDEX
0%
Phase 1b Phase 2b Phase 2b AVERTS-1 AVERTS-2
DVD ≥ 2 DVD ≥ 2 DVD = 4-22 DVD = 4-22 DVD = 4-22
(n = 30) (n = 154) (n = 97) (n = 165) (n = 105)
Note: p values shown for Count of DVD by Poisson Regression Analysis; AVERTS-2 based on 111 patients enrolled through Month 3 (105 with daily diary information) 8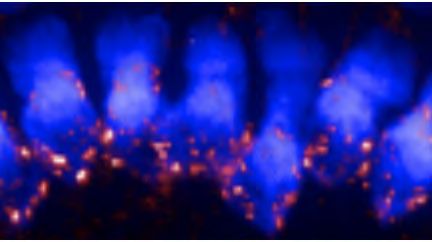
Comparable Vertigo Response in AVERTS-2 and Phase 2b
Change In Mean Monthly % Reduction in Vertigo Frequency From
Definitive Vertigo Days (DVD) Baseline to Month 3: Responder Analysis
10
80%
8 p = 0.014
60%
AVERTS-2 6
2.5 day
40%
(Phase 3) 4 lower
59%
73%
than 55%
n = 105 placebo 20%
2 6.2 day 36% 38%
clinical benefit 21%
0 0%
Placebo OTIVIDEX Placebo OTIVIDEX
10 80%
8 p = 0.002 60%
Phase 2b 6
(4-22 DVD) 2.6 day 40% 73%
4 lower 64%
n = 97 than 58%
20% 44% 42%
2 6.2 day placebo
27%
clinical benefit
0 0%
Baseline Month 1 Month 2 Month 3 ≥ 50% ≥ 75% 100%
reduction reduction reduction
Note: p values shown for Count of DVD by Poisson Regression Analysis 9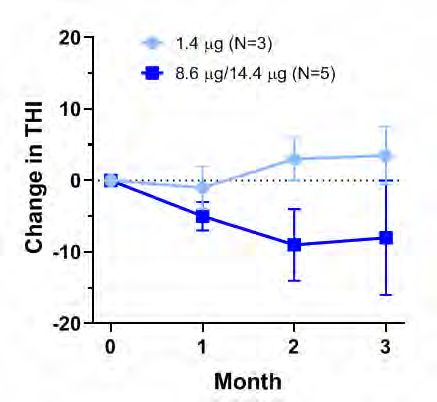
Additional Phase 3 Trial Leverages Prior Clinical Experience
Single OTIVIDEX Treatment Designed to Improve Vertigo for 3 Months
One
Three Month
Month
Follow-up
Lead-in Single IT injection:
OTIVIDEX or placebo
Trial Design Patient Criteria Primary Endpoint in Phase 3
• Same basic trial design • Key enrollment criteria is active • Count of DVD for OTIVIDEX vs.
used across all trials vertigo: require 4-22 Definitive placebo in Month 3
• Focus on vertigo, which Vertigo Days (DVD) during one
is most debilitating month lead-in
symptom • Patients report vertigo via daily
• 160 patient target with telephone diary
1:1 randomization
10Patient Enrollment Ongoing for OTIVIDEX Phase 3 Trial
Changes made to manage patient expectation bias and placebo response
Refined site selection Emphasizing recruitment of Careful management of
criteria (no commercial well-characterized Ménière’s clinical site communication
CRO trial sites) patients known to investigators with study subjects
(no advertising) (placebo response training)
• Trial includes clinical sites in the U.S. and Europe
• Other aspects of program “registration ready”
11OTIVIDEX Market Opportunity is Significant
Current Landscape1 OTIVIDEX Market Potential
> 850K Patients in U.S. with
• Expect to be first FDA-approved drug
Ménière’s Disease to treat Ménière’s Disease
• Opportunity to develop market and
build Ménière’s patient community
~ 280K Patients See
Physician During Year • Expand number of patients seeking
treatment and % treated with steroids
~ 50% Treated • Repeat use for chronic condition
Off-label use of
with
oral and/or repeat
Steroid
IT steroid injections • ~ $500M U.S. sales potential2
1 IMS patient-centric data; 2LEK survey and analysis 12Persistent and Chronic Tinnitus Affects Millions
Tinnitus is perception of hearing noise when there is no sound
Can severely impact
~ 10% OF
ABILITY TO SLEEP
U.S. ADULTS
experience tinnitus OR RELAX,
leads to anxiety and depression
~ 8M report
MODERATE NO FDA-APPROVED
DRUG TREATMENTS
#1 service-related disability in TO SEVERE or standard of care for this condition
U.S. MILITARY1 bothersome level2
1United States Department of Defense; 2ClearView Healthcare Partners analysis (2018) 13Rationale for NMDA Receptor Antagonist to Treat Tinnitus
Normal Damage → Tinnitus Tinnitus Treatment
Hair Cell
Excessive
Glutamate
Glutamate
Release
Gacyclidine
SGNs
Over-
Excitation
During normal hearing, hair cells release Cochlear injury (e.g., from noise or trauma) Inhibition of over-excited SGNs
glutamate to activate NMDA receptors on can produce excessive glutamate release with a selective NMDA receptor
spiral ganglion neurons (SGNs) to relay and over-activation of the NMDA receptor antagonist can reduce tinnitus
sound information to the brain sub-type leading to tinnitus
14OTO-313 Has Attractive Profile for Tinnitus Treatment
Pilot Clinical Study Demonstrated
• OTO-313 is sustained-exposure formulation Dose-Dependent Improvement in
of gacyclidine – weeks of exposure from TINNITUS HANDICAP INVENTORY (THI)
single IT injection
• Gacyclidine is a potent and selective NMDA
receptor antagonist
• Preclinical data shows inhibition of
Improved
spontaneous neuronal activity in SGNs and
POC in tinnitus model
• Effect of gacyclidine on tinnitus demonstrated
in pilot clinical study
In open-label Phase 1 study conducted by NeuroSystec,
gacyclidine was infused into the cochlea for 48 hours
15Patient Enrollment Completed for OTO-313 Phase 1/2 Trial
Randomized, double-blinded, placebo-controlled safety and exploratory efficacy
study of OTO-313 given as a single intratympanic injection in subjects with tinnitus
• Successfully completed initial patient cohort for safety and tolerability assessment
• 35 patients with unilateral, persistent tinnitus of cochlear origin enrolled in exploratory efficacy cohort
• Inclusion required that patient’s tinnitus severity exceeded specified level
• Randomized 1:1 for single intratympanic injection of OTO-313 or placebo
Cohort 1
(n = 8) Screening 4 Week Follow-up (Completed)
Cohort 2 Screening & Lead-in 8 Week Follow-up
(n = 35)
16Exploratory Efficacy Endpoints in Phase 1/2 Clinical Trial
• Tinnitus Functional Index (TFI):
o Validated clinical instrument that assesses tinnitus
severity and functional impact on patient
o Can be used to measure treatment-related changes
o Switched to completion by patient at-home
• Tinnitus Loudness Rating Scale (via phone diary)
• Tinnitus Annoyance Rating Scale (via phone diary)
• Patient Global Impression of Change (PGIC)
17Large, Untapped Market Opportunity for OTO-313
Current Landscape1 OTO-313 Market Potential
~ 31M in U.S. with • No drug treatments approved by FDA;
Subjective Tinnitus current therapies help patients cope but
do not treat tinnitus pathophysiology
• Opportunity to create SOC treatment
~ 8M with Moderate to
Severe Tinnitus • Initial focus on patients early after onset
• Buy-and-bill model; disease burden
1.5M “New” supports pricing comparable to CGRP’s
Tinnitus
Pts/Yr2
• > $1B U.S. sales potential1
1Clearview Healthcare Partners analysis; 2IMS patient-centric data: patients treated for tinnitus in a single year with no tinnitus diagnosis in prior 2 years 18Hearing Loss is a Large and Growing Problem Worldwide
Hearing Loss is 4th Leading Cause of Disability Globally1
Most prevalent neurologic health issue:
NO EFFECTIVE
> 360M PEOPLE TREATMENTS
have disabling hearing loss2 and no approved drugs
for hearing loss
Common causes include: Leads to Social Isolation,
lower QOL,
AGING, NOISE, AND HIGHER High economic burden:
OTOTOXIC RATES OF MEDICAL COSTS
DRUGS AND DEMENTIA AND + IMPACT
GENETICS DEPRESSION of lower work productivity
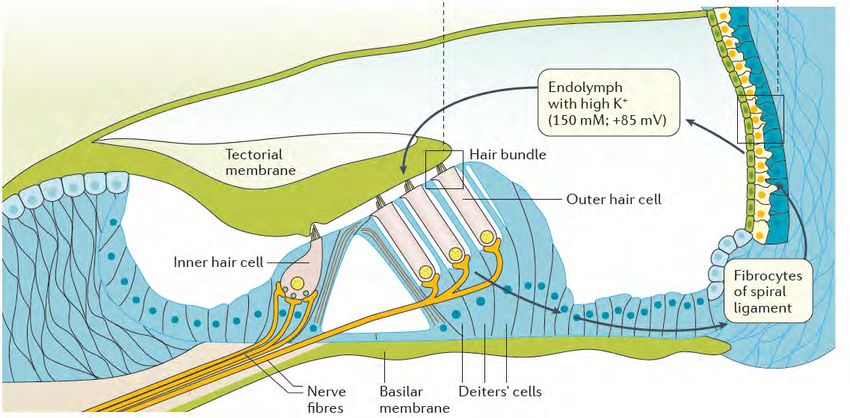
1Wilson, et al. Lancet. (2017); 2World Health Organization, Global Estimates on Prevalence of Hearing Loss, (2012) 19Addressing Multiple Hearing Loss Pathologies
Damage to cochlea hair cells due to Recent research has identified damage to
noise, aging, or exposure to ototoxic synaptic connections as an underlying pathology
chemicals results in hearing loss in noise and age-related hearing loss that
detectable in standard hearing test manifests as speech-in-noise hearing difficulty
Intact synapses
(called puncta) shown
as colored dots
3 rows of
outer and
1 row of
inner hair
cells
Hearing Loss 1) Repair damaged synaptic connections (OTO-413)
Pathologies 2) Repair or regenerate cochlear hair cells (OTO-6XX)
Targeted by 3) Protect inner ear from ototoxic chemicals (OTO-510)
Otonomy 4) Congenital hearing loss (GJB2 collaboration with AGTC)
Figure from Moser and Starr, Nature Reviews: Neurology (2016) 20Otonomy’s Programs Target Broad Hearing Loss Populations
Illustrative
Cochlear Synaptopathy Hair Cell Pathology
• Problem hearing in presence Speech- Hearing • Hearing loss detected in
of background noise In-Noise Threshold standard test (hear tones in
Difficulty Deficit
• Normal standard hearing test quiet setting)
• U.S. prevalence1 ≈ 9M • U.S. prevalence2-5 ≈ 42M
Mixed Pathology
• Loss/damage to synapses & hair cells
OTO-413 Target OTO-6XX Target
Patient Population • Speech-in-noise hearing difficulty & Patient Population
hearing threshold deficit
• Subset of 42M with threshold deficit
1Tremblay et al., Ear Hear, 2015; 2Hoffman et al., JAMA Otolaryngol HNS, 2017; 3Nash et al., Arch Otolaryngol HNS, 2011
4Morton 21
et al., N Engl J Med, 2006; 5Brooke et al., JAMA Otolaryngol HNS, 2017; Analysis by ClearView Healthcare PartnersOTO-413: Sustained-Exposure Formulation of BDNF
Promotes SGN survival Increases SGN neurite outgrowth
Control BDNF
Therapeutic Effects of
Brain-Derived
Neurotrophic Factor
(BDNF) in the Cochlea
Reconnects SGNs with hair cells after chemical synaptopathy
Control Synaptopathy Synaptopathy + BDNF
22OTO-413 Proof-of-Concept in Synaptopathy Animal Model
Hot Topic at 2018 Society for Neuroscience Meeting
Synapse Count Normalized with Auditory Function Improved
OTO-413 Following Noise Damage Across Range of Sound Frequencies
Naïve
Noise + Vehicle
Noise + OTO-413
23Enrolling Patients in Phase 1/2 Clinical Trial for OTO-413
Phase 1/2 Ascending Dose Safety and Exploratory Efficacy Study
Three Month
Screening
Follow-up
IT injection:
OTO-413 or placebo
Trial Design
• ≈ 40 patients with speech-in-noise hearing deficit
• Safety, tolerability and PK
Exploratory Efficacy Endpoints
• Auditory brainstem response (ABR)
• Speech-in-noise tests
• Hearing handicap questionnaire
24OTO-6XX: Hair Cell Regeneration
Hair cell regeneration model
Naïve Damage only Damage + OTO-6XX Compound
Myo7a: Hair Cells
Indication Otonomy Program / Status
• Multiple possible indications in which severe • Non-mammalian species able to regenerate
hearing loss is due to hair cell death hair cells; knowledge of pathways involved
• May result from a variety of insults and provides targets
significantly affects ability to communicate • POC in hair cell regeneration model
• Selected candidate for development
25Need for Cisplatin-Induced Hearing Loss (CIHL) Protection
~ 500K
patients treated with platinum- > 80% OF CHILDREN
based cancer chemotherapies treated with platinum agents
each year in U.S. including experience hearing loss1
~ 5K CHILDREN
CIHL impacts
Agents, especially
cisplatin, are
SPEECH DEVELOPMENT,
OTOTOXIC ACADEMIC PERFORMANCE,
AND SOCIALIZATION
LIFE-LONG IMPACT
highlighted at recent patient symposium
1Landier, et al. Journal of Clinical Oncology. (2014) 26OTO-510 Initially Targeting Children Receiving Cisplatin
• Established clinical feasibility of CIHL POC Animal Model
conducting pediatric CIHL trial in pilot
study using OTIVIDEX *** p < 0.001
• Identified therapeutic target with higher
level of otoprotection than steroids in
nonclinical studies
• Proof-of-concept demonstrated in CIHL
animal model
• Preclinical development continuing for
small molecule otoprotectant in
sustained-exposure formulation Cisplatin OTO-5XX + Cisplatin
27Mutations in the Gap Junction Beta-2 (GJB2) gene are the
most common cause of congenital hearing loss
• In developed countries, about 1 out of 500
children are born with or develop hearing loss
prior to language development (”prelingual”)
• Genetic mutations are the most common
cause of prelingual hearing loss
• GJB2 accounts for ~30% of congenital hearing
loss cases
• Patients with GJB2 mutations often have
severe-to-profound hearing loss in both ears
• Typically identified by newborn screening that
is routine in US and EU
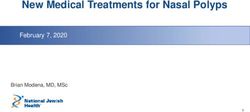
Reference: Shearer et al, “Hereditary Hearing Loss and Deafness Overview” (2017) 28GJB2 gene encodes gap junction protein Connexin 26
that is involved in ion channel homeostasis
• Connexin 26 is expressed in non-sensory cell types within the cochlea
• Mutations in GJB2 gene impair gap junctions that control potassium
homeostasis leading to hair cell dysfunction and hearing loss
• Goal: otic delivery of GJB2 therapy to achieve high local concentration of gene
(low systemic exposure) to restore functional gap junctions and hearing
Connexin 26 expression
Fibrocytes
Spiral
limbus
Support cells
Figure reference: Korver et al, Nature Reviews Disease Primers (2017) 29 29Otonomy and AGTC established strategic collaboration to
develop gene therapy for GJB2 mutations
• Co-development and co-commercialization partnership
• Equal sharing of program costs and proceeds
• Leverages complementary experience, expertise and resources
AGTC OTIC
AAV vector design and manufacturing √
Inner ear drug delivery √
Preclinical development √ √
Clinical development & regulatory √ √
• Opportunity to add other targets to collaboration
30Financial Update and Guidance
Operating Expenses1
• 1Q20 Results: Non-GAAP Op Exp = $10.1M and GAAP Op Exp = $11.5M
• 2020 Financial Guidance: Non-GAAP Op Exp of $35-$38M and GAAP Op Exp of $45-$48M
Cash Runway
• Cash, cash equivalents and short-term investments as of March 31, 2020 totaled $48.6M
• Long-term debt: $15M term loan completed with Oxford Finance in December 2018
• Current capital will fund operations into 2021 and through results for the ongoing OTIVIDEX,
OTO-313 and OTO-413 clinical trials
1Primary adjustment from GAAP to Non-GAAP is stock-based compensation expense; reconciliation can be found on our web-site www.otonomy.com 31Multiple Upcoming Clinical Trial Catalysts
Expected Timing Program Milestone
✓ 2Q19 Initiate OTO-313 Phase 1/2 trial
✓ 3Q19 Initiate OTO-413 Phase 1/2 trial
OTO-313 Phase 1/2 trial results
Note: program updates
including timeline to
trial results to be
OTIVIDEX Phase 3 trial results
provided in June 2020
OTO-413 Phase 1/2 trial results
32Otonomy is Leading the Way in Neurotology
Applying Expertise in To Address Large
Neuroscience and Patient Populations with
Otic Drug Delivery No Drug Treatments
Funding in Place to
Achieve Clinical
Catalysts for
Multiple Programs
33You can also read