COVID-19 STRATEGIC PREPAREDNESS AND RESPONSE PLAN - 2021 EDITION Reinforcing the collective readiness and response in the WHO Eastern ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVID-19 STRATEGIC Reinforcing the collective
PREPAREDNESS AND readiness and response
in the WHO Eastern
RESPONSE PLAN Mediterranean Region
2021 EDITION

COVID-19 STRATEGIC Reinforcing the collective
PREPAREDNESS AND readiness and response
in the WHO Eastern
RESPONSE PLAN Mediterranean Region
2021 EDITION
WHO Library Cataloguing in Publication Data
Names: World Health Organization. Regional Office for the Eastern Mediterranean
Title: COVID-19 strategic preparedness and response plan: reinforcing the collective readiness and response in the WHO Eastern
Mediterranean Region, 2021 edition / World Health Organization. Regional Office for the Eastern Mediterranean
Description: Cairo: World Health Organization. Regional Office for the Eastern Mediterranean, 2021
Identifier: WHO-EM/CSR/383/E
Subjects: COVID-19 - epidemiology | Betacoronavirus | Disease Outbreaks | Disaster Planning | Civil Defense | Health Information
Management | Eastern Mediterranean Region
Classification: NLM WC 506.4
© World Health Organization 2021
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike
3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided
the work is appropriately cited. In any use of this work, there should be no suggestion that WHO endorses any specific
organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license
your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add
the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization
(WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding
and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the
World Intellectual Property Organization.
Suggested citation. COVID-19 strategic preparedness and response plan: reinforcing the collective readiness and response
in the WHO Eastern Mediterranean Region – 2021 edition. Cairo: WHO Regional Office for the Eastern Mediterranean; 2021.
Licence: CC BY-NC-SA 3.0 IGO.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for
commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or
images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the
copyright holder. The risk of claims resulting from infringement of any third-party- owned component in the work rests solely
with the user.
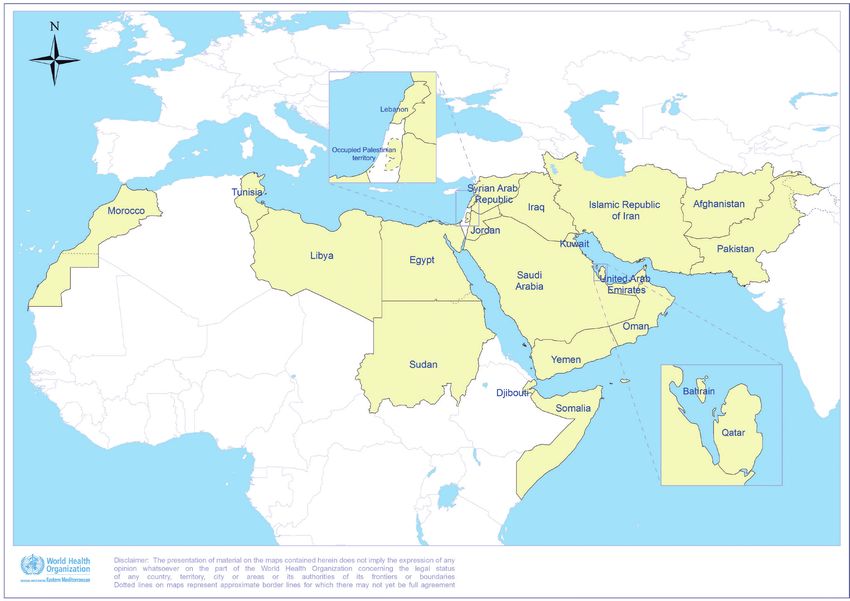
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the
expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps
represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of
certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in
preference to others of a similar nature that are not mentioned.
Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable
precautions have been taken by the World Health Organization to verify the information contained in this publication. However,
the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for
the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for
damages arising from its use.
Document WHO-EM/CSR/383/E
COVID-19 strategic preparedness and response plan – 2021 edition iv
4
CONTENTS
Foreword from the Regional Director vi
1. Purpose of the document 1
2. Global situation 2
3. Situation in the Eastern Mediterranean Region 4
3.1 Epidemiological situation 4
3.1.1 Evolution of the COVID-19 epidemic in the Region 4
3.1.2 Current situation in the Region (as at 28 February) 6
3.2 Risk assessment of COVID-19 in the Region 9
3.3 Operational context 10
3.3.1 Humanitarian settings and vulnerable groups 10
3.3.2 Effects on health systems and essential services 11
3.3.3 Social and economic effects 12
3.3.4 Public health and social measures 12
3.3.5 Vaccines 13
3.3.6 Regional contribution to global research, development and innovation 14
3.4 Regional collaboration and coordination 14
4. Key lessons learned for leveraging the COVID-19 response in the Region in 2021 16
4.1 Partnership and coordination 16
4.2 Communications (external and internal) 16
4.3 Operations support and logistics 16
4.4 Health operations and technical expertise 17
4.5 Health information management and surveillance 17
4.6 International Health Regulations and social measures 18
4.7 Research and knowledge management 18
4.8 Essential health services and systems 18
4.9 COVID-19 vaccine 19
5. Beyond COVID-19 20
6. Strategic preparedness and response plan for COVID-19 in the Eastern Mediterranean 21
Region in 2021
6.1 Goal 21
6.2 Regional strategic objectives 21
Areas of work and priority activities for COVID-19 preparedness and response in 2021 23
7. Budget summary by pillar (2021) 32
8. Monitoring and evaluation 33
Annex 1. 34
COVID-19 SPRP M&E framework for 2021: Proposed indicators
WHO EASTERN MEDITERRANEAN REGION v
FOREWORD FROM THE REGIONAL DIRECTOR
Over the past year, all three levels of the World Health Based on the experience of the past year, we will also
Organization (WHO) have worked with countries to provide aggressively scale up fragmented data systems, improve
guidance and oversight to ensure a streamlined and data sharing by countries, and strengthen infection
coordinated response to COVID-19 by national authorities, prevention and control policies. This will be key in light
partners, communities and the private sector. The of the growing number of variants appearing around the
Organization has built experience and gained insights into world, which need to be identified and detected. The longer
what worked best and what did not work so well in the the pandemic goes on, the more such variants are expected
COVID-19 strategic preparedness and response plan for to emerge, perhaps undermining the effectiveness of the
2020. vaccines we have just started to celebrate rolling out.
Looking ahead, and building on this wealth of experience, The coming period in our Region will be challenging for
the regional COVID-19 strategic preparedness and response us all, and making sure that we reduce fear, stigma and
plan for 2021 lays out the coordinated action required hesitancy will be critical to our efforts. One year into
at national and regional levels to overcome challenges, the pandemic, we understand that COVID-19 fatigue has
address inequities and work towards ending the COVID-19 set in, and that we now face a new threat – not just of
pandemic. misinformation and disinformation, but of communities
desperate to go back to pre-COVID-19 times.
The revised plan brings together the collective actions
needed to suppress transmission, reduce exposure, address In addition to the public health risks that the virus presents,
misinformation and disinformation, protect the vulnerable we are understandably concerned about the economic,
through vaccination, reduce mortality and morbidity, and social and political costs of the pandemic. We also should
accelerate equitable access to new COVID-19 vaccines and not forget other emergencies in our Region – crises that are
tools. The Incident Management Support Team (IMST) will characterized by years of conflict, and the consequent social
continue to ensure coordination, planning, financing and and political disruptions that have further devasted the lives
monitoring for the response across all countries and at a of millions.
regional level, providing operational support, including for
logistics and supply chains, as well advocating for countries We cannot defeat COVID-19 as a divided region, or by
to conduct research and innovation. politicizing the pandemic. Using “Health as a Bridge to
Peace” we hope that our shared goal of saving lives and
COVID-19 vaccines are finally within reach. To work towards ending the pandemic will allow for countries to come
defeating COVID-19, we need open, fair and equitable together to work for the common good. COVID-19 has
sharing of vaccines. But even after we overcome the initial shown us that the virus can only be beaten through
challenges of limited supplies, uneven access and staggered solidarity, coordination and collaboration, allowing us to
roll-out, a range of well-designed programme strategies will achieve our regional vision of Health for All, by All.
be needed to drive up acceptance and uptake of vaccines in
the countries of the Region.
Dr Ahmed Al-Mandhari
WHO Regional Director for the Eastern Mediterranean
COVID-19 strategic preparedness and response plan – 2021 edition vi
6
1. PURPOSE OF THE DOCUMENT On 30 January 2020, the coronavirus disease 2019 the Region’s Vision 2023, and WHO’s Thirteenth General (COVID-19) outbreak was declared a public health Programme of Work 2019–2023. emergency of international concern. Four days later, the World Health Organization (WHO) global COVID-19 strategic Building on successful strategies in 2020 and lessons preparedness and response plan (SPRP) was published, learned, this document was developed by the WHO Regional followed by the first edition of the SPRP for the Eastern Office for the Eastern Mediterranean to help to guide the Mediterranean Region to accelerate regional readiness. public health response to COVID-19 in the Region in 2021. It The present document is the third edition of the regional sets the regional strategic priorities that WHO will support in SPRP, serving as an update to the July 2020 edition and 2021 to reinforce collective readiness and response to the aligned with the most recent version of the global SPRP, COVID-19 pandemic. The WHO Eastern Mediterranean Region COVID-19 strategic preparedness and response plan – 2021 edition 1
2. GLOBAL SITUATION
On 31 December 2019, WHO was alerted to several Africa and 1.4% from the Western Pacific. The country
cases of pneumonia of unknown origin in Wuhan, Hubei most affected is the United States of America with 28
province, China. One week later, on 7 January 2020, 174 978 cumulative cases and 506 760 associated deaths
Chinese authorities confirmed that they had identified a (CFR 1.8%), followed by India which reported a total of 11
new type of coronavirus as the cause of the pneumonia 096 731 cases and 157 051 associated deaths (CFR 1.4%)
cluster. The novel coronavirus belongs to the same family of and Brazil with 10 455 630 cases and 252 835 associated
coronaviruses that cause illnesses ranging from the common deaths (CFR 2.4%). The highest incidence rates are reported
cold to more severe diseases such as Middle East respiratory from Andorra (14 confirmed cases per 100 population),
syndrome (MERS) and severe acute respiratory syndrome followed by Montenegro and the Czech Republic (both
(SARS). The illness caused by this novel coronavirus is with 13 confirmed cases per 100 population) and Gibraltar
referred to as coronavirus disease 2019 (COVID-19). (12 confirmed cases per 100 population). The highest
CFRs are reported in Yemen (27.7%) followed by Mexico
Since January 2020, COVID-19 has spread across the world, (8.9%), while the lowest CFRs are reported from Singapore
disrupting even the most resilient health systems and (0.05%) and Mongolia (0.08%). Globally, 144 countries
services. Global incidence rates slowed down after the have self-reported community transmission while 43
implementation of public health and social measures, countries have self-reported sporadic or no cases.1 The
but with premature lifting of some social measures and overall epidemiological data vary among WHO regions,
the probable impact of the emergence of variants of countries and territories, and within countries. The observed
concern, incidence increased at the end of 2020 and into trends may not always represent the evolving and real
2021. As at 28 February 2021, over 113 million COVID-19 epidemiological situations due to incomplete reporting.
cases have been reported globally, with over 2.5 million Countries have different capacities in detection, confirmation
reported deaths (case fatality ratio (CFR) 2.2%) (Fig. 1). and reporting of COVID-19 cases. The response capacities in
Of these cases, 44.5% were reported from the Region of terms of case investigation, contact tracing, quarantine, case
the Americas, 34.1% from Europe, 11.9% from South-East management and isolation, among other factors, contribute
Asia, 5.6% from the Eastern Mediterranean, 2.5% from to the varying incidence and mortality rates.
Fig. 1. Global and regional trends in COVID-19 cases, 28 February 2021
6000
Eastern Mediterranean Region
African Region
5000
The Americas
European Region
Number of cases (in thousands)
4000
South-East Asia Region
Western Pacific Region
3000
2000
1000
0
2020_01
2020_02
2020_03
2020_04
2020_05
2020_06
2020_07
2020_08
2020_09
2020_10
2020_11
2020_12
2020_13
2020_14
2020_15
2020_16
2020_17
2020_18
2020_19
2020_20
2020_21
2020_22
2020_23
2020_24
2020_25
2020_26
2020_27
2020_28
2020_29
2020_30
2020_31
2020_32
2020_33
2020_34
2020_35
2020_36
2020_37
2020_38
2020_39
2020_40
2020_41
2020_42
2020_43
2020_44
2020_45
2020_46
2020_47
2020_48
2020_49
2020_50
2020_51
2020_52
2020_53
2021_01
2021_02
2021_03
2021_04
2021_05
2021_06
2021_07
2021_08
1
WHO coronavirus disease (COVID-19) dashboard (https://covid19.who.int/, accessed 1 March 2021).
WHO EASTERN MEDITERRANEAN REGION 2
For reasons that are not completely understood, males are data, in the first three months of the pandemic health
slightly more affected than females especially in terms of care worker infections slightly exceeded 10% of reported
disease severity and case fatality (51% of cases and 57% cases, declining to less than 5% by early June 2020 and to
of deaths). However, females are often disproportionately approximately 2.5% by September 2020. In addition, the
affected by the social and economic consequences of heavy burden placed on health workers involved in the
response measures. Women also suffer from loss or limited response and within the wider health system has had a
accessibility to reproductive and sexual health services, negative impact on their health and well-being.3
antenatal care and other maternal health services. There
are reports from several countries of increased incidence of Vaccinations against COVID-19 have started and are ongoing
gender-based violence.2 in many countries worldwide. As at 9 February 2021, Our
World in Data reported that 134.65 million vaccine doses
Regarding age groups, adults aged 25–55 years are the had been administered globally and at least 65 countries
most affected, but disease severity and risk of death are had initiated vaccination campaigns.6 The majority of these
associated with increased age. Elderly populations are more countries were in Europe and North America, although
at risk of severe symptoms and death, with over 80% of vaccination efforts are starting in Africa, South America,
deaths occurring in individuals aged above 65 years. The South and South-East Asia, and the Eastern Mediterranean
COVID-19 pandemic has taken a toll on the mental, social (13 countries in the Eastern Mediterranean Region had
and economic well-being of individuals and communities. begun vaccination by 28 February 2021).
It has been estimated that most COVID-19 infections As SARS-CoV-2 variants have become a significant concern
originate from relatively few individuals in high-transmission globally, WHO established the SARS-CoV-2 Virus Evolution
events or settings.3,4 Transmission mainly occurs among Working Group to assess the levels of risk and impacts of
close contacts of infected persons in indoor spaces and can mutations on public health. Implementing or improving
be amplified by poor ventilation. Secondary attack rates are sequencing capacity at the national level has become a
higher in household settings (recent estimates from two priority in this regard.
meta-analyses5 suggest household secondary attack rate is
approximately 17–21%), and outbreaks have been reported Health systems and delivery of regular health services
from a number of settings, including long-term living have been severely affected by the COVID-19 pandemic
facilities, prisons, religious or social events, as well as food and financial hardship has increased due to demand for
processing plants. COVID-19-related services. To ensure equitable access
to diagnostics, therapeutics and vaccines, health system
Data show that about 7.7% of cases worldwide are among capacities such as financing, workforce planning, clinical
health care workers, although there are wide variations care, logistics and supply chain management must be
among countries, with changes over time. Based on WHO strengthened.
2
Gender and COVID-19: advocacy brief, 14 May 2020. Geneva: World Health Organization; 2020 (https://apps.who.int/iris/bitstream/handle/10665/332080/
WHO-2019-nCoV-Advocacy_brief-Gender-2020.1 eng.pdf?sequence=1&isAllowed=y, accessed 21 February 2021.
3
Endo A, Abbott S, Kucharski AJ, Funk S. Estimating the overdispersion in COVID-19 transmission using outbreak sizes outside China. Wellcome Open Res.
2020;5:67. doi:10.12688/wellcomeopenres.15842.3.
4
Koh WC, Naing L, Chaw L, Rosledzana MA, Alikhan MF, Jamaludin SA, et al. What do we know about SARS-CoV-2 transmission? A systematic review and
meta-analysis of the secondary attack rate and associated risk factors. PLoS ONE. 2020;15(10):e0240205. doi:10.1371/journal.pone.0240205.
5
COVID-19 strategic preparedness and response plan, 1 February 2021 to 31 January 2022. Geneva: World Health Organization; 2021 (https://www.who.int/
publications/i/item/WHO-WHE-2021.02, accessed 21 February 2021).
6
COVID-19 data explorer: COVID-19 vaccine doses administered per 100 people [online database]. Oxford: Our World in Data; 2021 (https://ourworldindata.
org/coronavirus-data-explorer?tab=map&zoomToSelection=true&country=®ion=World&vaccinationsMetric=true&interval=total&perCapita=true&smoothin
g=0&pickerMetric=total_cases&pickerSort=desc, accessed 10 February 2021).
COVID-19 strategic preparedness and response plan – 2021 edition 33. SITUATION IN THE EASTERN MEDITERRANEAN REGION
3.1 Epidemiological situation
3.1.1 Evolution of the COVID-19 epidemic in the Region
The first cases of COVID-19 in the Eastern Mediterranean restrictions and other mobility measures were imposed by
Region were reported by the United Arab Emirates on 29 countries in the Region, the proportion of locally acquired
January 2020 among travellers coming from Wuhan, China. infections increased. Most of the Region showed a slow start
By the end of February 2020, 11 countries in the Region had to the outbreak in the first three months of the pandemic;
reported confirmed cases of COVID-19. In the subsequent however, in May 2020 disease transmission accelerated
weeks, the Region witnessed an increasing number of and rapid local and community spread were subsequently
countries with confirmed cases, and all 22 countries and observed in many countries.7 This could be attributed
territories had recorded COVID-19 cases by 10 April 2020. to easing of public health and social measures such as
travel restrictions and partial or full lockdowns, which
Most of the new cases recorded in the first three weeks were relaxed during the holy month of Ramadan in many
of the pandemic were imported and linked to countries/ countries, and to social gatherings during this month.
cities highly affected by COVID-19 outbreaks. When travel
The Region’s cumulative cases surpassed 6.4 million on 28 February 2021.
From the first reported COVID-19 case, it took 150 days to reach 1 million cases.
From there:
1 to 2 million cases 72 days
2 to 3 million cases 52 days
3 to 4 million cases 30 days
4 to 5 million cases 38 days
5 to 6 million cases 42 days
On 28 February 2021, COVID-19 deaths reached 144 947.
From the first reported death, it took 90 days to reach 10 000 deaths.
From there:
10 000 to 50 000 deaths 102 days
50 000 to 100 000 deaths 90 days
7
Al-Mandhari A, Brennan R, Abubakar A, Hajjeh R. Tackling COVID-19 in the Eastern Mediterranean Region. Lancet. 2020;396(10265):1786–8.
doi:10.1016/S0140-6736(20)32349-7.
WHO EASTERN MEDITERRANEAN REGION 4Two waves of the pandemic were observed in 2020 across Generally, countries in the Region have shown mixed
the Region: the first peak was reached in week 25 (starting patterns of resurgence, decrease or stabilization in the last
on 14 June) with 138 844 new confirmed cases and six months. The curve has fluctuated in recent weeks, with
3435 deaths, followed by a gradual decrease in reported 12 countries reporting an increase in numbers of cases until
cases and deaths. In week 35 (starting on 23 August) a February 2021 (Fig. 2). The trend in COVID-19 deaths has
significant increase in the number of confirmed cases and shown the same pattern, with a sharp increase since mid-
deaths was observed across the Region. COVID-19 cases October 2020, declining from mid-November and plateauing
increased sharply from mid-October 2020 and reached a since the beginning of 2021. The Islamic Republic of Iran,
peak in mid-November 2020. This increase was initially Lebanon, Tunisia, Pakistan and Egypt have been the main
due to a resurgence of cases in the Islamic Republic of contributors to the number of deaths since the beginning of
Iran, Jordan and Morocco, surpassing the number of cases 2021 (Fig.3).
reported during the mid-June 2020 peak. The second wave
peaked in week 47 (starting on 16 November), where the
highest weekly number of cases since the beginning of the
pandemic was reported (251 094 cases, 6300 deaths). Then,
a gradual decrease in the number of confirmed cases was
observed until the end of 2020.
Fig. 2. Weekly distribution of COVID-19 cases and CFR in the Eastern Mediterranean Region,
29 January 2020–28 February 2021
300 000 16
Cases 14
250 000
CFR (%)
12
200 000
Number of cases
10
CFR (%)
150 000 8
6
100 000
4
50 000
2
0 0
5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 1 2 3 4 5 6 7 8
2020 2021
Epidemiological weeks
Fig. 3. Weekly distribution of COVID-19 deaths in the Eastern Mediterranean Region,
29 January 2020–28 February 2021
7000
6000
5000
Number of deaths
4000
3000
2000
1000
0
5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 1 2 3 4 5 6 7 8
2020 2021
Epidemiological weeks
COVID-19 strategic preparedness and response plan – 2021 edition 53.1.2 Current situation in the Region (as at 28 February)
The Eastern Mediterranean Region (home to 9% of the attack rates have been reported from Bahrain (7.2 cases
world’s population) has the fourth highest number of cases per 100 population), followed by Qatar (5.7 cases per 100
and deaths among the six WHO regions. As at 28 February population) and Lebanon (5.5 cases per 100 population);
2021, a total of 6 421 085 cases of COVID-19 and 144 these countries also have among the highest testing rates in
947 associated deaths (CFR 2.3%) have been reported, the Region.
representing 5.6% of the cases and 5.7% of the deaths
reported globally. Since the beginning of the outbreak, the The regional CFR is 2.3%, ranging from 0.2% to 27.7%
Islamic Republic of Iran has reported the highest number (median CFR = 1.8%). The highest CFRs are reported by
of cases in the Region (1 631 169 cases; 25.4% of the total Yemen (27.7%) followed by the Syrian Arab Republic
for the Region) followed by Iraq (695 489; 10.8%) and (6.6%). The lowest CFRs are reported by Qatar (0.2%)
Pakistan (581 365; 9.1%). The Islamic Republic of Iran has followed by the United Arab Emirates (0.3%) and Bahrain
also reported the highest number of cumulative associated (0.4%), a result of better quality health care systems,
deaths (60 073; CFR 3.7%) followed by Iraq (13 406; increased testing capacity, adequate hospital and intensive
CFR 1.9%) and Pakistan (12 896; CFR 2.2%). The highest care capacity and trained staff.
Fig. 4. COVID-19 cumulative incidence per 100 000 population and total deaths per country,
Eastern Mediterranean Region, 28 February 2021
Lebanon Syrian Arab
Republic
Occupied Palestinian
territory
Islamic Republic
Jordan Iraq of Iran
Morocco Afghanistan
Tunisia
Kuwait Pakistan
Libya Egypt
United Arab
Saudi Arabia Emirates
Oman
Sudan Yemen
Djibouti
Incidence per million Deaths per million Somalia
Bahrain
< 100 < 50
100–1000 50–100 Qatar
1001–10 000 101–500
10 001–50 000
> 500
> 50 000
The trends in incidence and mortality vary across the Region COVID-19 transmission patterns have evolved over time,
(Fig. 4), in part due to variations in detection, diagnostics, with 16 countries currently self-reporting community
reporting and response capacities of Member States, as well transmission, five countries (Afghanistan, Bahrain, Djibouti,
as demographic differences. Moreover, response capacities Egypt, Morocco) self-reporting clusters of cases, and one
are most variable at the subnational level, contributing to country self-reporting sporadic cases (Saudi Arabia).
some uncertainty on numbers of cases reported nationally.
The implementation of public health and social measures
coupled with their intensity, coverage and public adherence
also contribute to this variation.
WHO EASTERN MEDITERRANEAN REGION 6In terms of testing, a total of 97 602 151 laboratory- transmissibility and/or reduced virus neutralization among
confirmed PCR tests have been conducted across the Region humans. These variants include the SARS-CoV-2 VOC
since the start of the pandemic, including 3 272 018 tests 202012/01, the VOC linked to infections among farmed
in week 8 of 2021, which showed a 2% increase compared mink, the SARS-CoV-2 501Y.V2 and most recently SARS-
to the previous week (3 197 386). Countries in the Region CoV-2 B1.1.248. Out of 14 countries in the Region with
have adapted different testing strategies, despite WHO’s SARS-CoV-2 genome sequencing capacity, 13 have reported
recommendation to follow the COVID-19 case definitions8. VOCs (as at 28 February 2021) including Bahrain, Iran
As a result of different testing strategies and capacities, (Islamic Republic of), Iraq, Jordan, Kuwait, Lebanon, Libya,
Jordan, Lebanon and Gulf Cooperation Council (GCC) Morocco, occupied Palestinian territory, Oman, Pakistan,
countries have reported the highest numbers of tests per Saudi Arabia and the United Arab Emirates.
capita, while countries with complex emergencies such
as Afghanistan, Somalia, Sudan, Syrian Arab Republic and Data from the Region’s case database of 2 015 925 records
Yemen reported the lowest number of tests per capita in show that, as is the case globally, males are more affected
the Region. The number of tests per 100 000 population than females, with a male to female ratio of 1.8 to 1.0.
varies from 40 to 310 057, with a regional median of 13 This ratio varies among countries, ranging from 1.1 in Egypt
467 tests. The cumulative test positivity ratio is also widely to 4.0 in Qatar. COVID-19 is more prevalent among adults,
variable, ranging from 1% to 25% with a median of 10.4%. with about two thirds of COVID-19 cases in the Region
The lowest test-positivity ratio has been reported from being reported among those aged 25–55 years, and the
Bahrain, Saudi Arabia and the United Arab Emirates, while most affected age group being 25–35 years of age. The risk
Afghanistan, Syrian Arab Republic and Tunisia reported the of death increases with age, with the highest frequency
highest positivity ratio. of deaths reported among those over 55 years of age.
Increased rates of severe and complicated disease, with
Over the past few months, several SARS-CoV-2 variants more adverse long-term outcomes, are also associated with
of concern (VOC) have been identified and preliminary older age.
evidence suggests that they may have increased
© WHO/EMRO
8
WHO COVID-19: case definitions: updated in Public health surveillance for COVID-19, published 16 December 2020. Geneva: World Health Organization; 2020
(https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2020.2).
COVID-19 strategic preparedness and response plan – 2021 edition 7The risk of COVID-19 infection among frontline health care To estimate the burden of COVID-19 in the Region, sero-
workers is higher than in the general population. Early epidemiological investigations are being conducted in
reports suggested that health care workers accounted for multiple countries to complement surveillance data
7–10% of all reported infections in the Region during the and guide the public health response, often with WHO
first three months of the pandemic. However, data on health support. In 2020, several countries reported their findings
care-associated infections are limited. In the Region, around in peer-reviewed journals or shared data with WHO. Most
2% of case report forms reported through the regional nationwide surveys conducted between June and December
platform, Eastern Mediterranean Flu (EMFLU), referred to 2020 in the Region estimated the prevalence of SARS-CoV-2
cases among health care workers. Underreporting and lack antibodies at 10%, which is consistent with the observations
of appropriate surveillance mechanisms to report infections from global nationwide studies. Notably, low-income
among the health workforce have likely contributed to countries and countries with complex emergencies have
an underestimation of health worker infections. The 14 reported higher estimates of prevalence in their populations,
country support missions by WHO during 2020 consistently up to 25% nationally and 30% subnationally (although
found deficiencies in infection prevention and control (IPC) these countries have reported the lowest numbers of cases
governance and practice as one of the most consistent in the Region). The highest rates of antibody prevalence
findings. were reported in health care workers and migrant workers
(specifically “craft and manual workers”).
© WHO/EMRO
WHO EASTERN MEDITERRANEAN REGION 83.2 Risk assessment of COVID-19 in the Region
WHO continues to assess the risks of COVID-19 at global, major impact on vaccine efficacy, although there is some
regional, country and community levels. The collection concern. WHO is working closely with countries in the
and analysis of epidemiological surveillance data from all Region to enhance genomic surveillance in order to detect
countries in the Region has significantly improved over and monitor mutations and their implications for disease
time, and the availability of these data has allowed WHO to transmissibility, diagnostics, vaccines, therapeutics and
conduct risk assessments on a regular basis to inform the overall public health responses.
public health response. While understanding of the SARS-
CoV-2 virus continues to grow regarding the epidemiology, The COVID-19 vaccine roll-out has started in many
pathophysiology, diagnosis and management of the virus countries and territories of the Region, and a decrease
and associated disease, much remains unknown, such in cases has been observed in the United Arab Emirates
as the source, the evolution of the virus over time, the since its deployment. Despite these positive preliminary
duration of human immunity, the impact of the vaccines observations, it is still too early for the vaccination
on new variants, and the long-term impacts of infection programme to impact COVID-19 transmission considering
on health. However, the availability of genetic sequencing the challenges it faces, including new variants. Delays in
data has provided valuable information on the biology vaccine procurement, distribution and administration could
and evolution of SARS-CoV-2. Combining the sequencing potentially alter the course of transmission at the population
and epidemiological data provides real-time knowledge level in the months to come. Efforts to ensure rapid and
and understanding of the emergence of new variants and fair vaccine deployment among priority groups are being
the impact on diagnostics and vaccines. WHO has been pursued through the COVAX Facility. Maintaining public
working with a global network of public health experts health and social measures alongside vaccination is still
to continuously assess the evolving situation and provide essential to limit transmission and reduce the morbidity and
recommendations to Member States. mortality associated with COVID-19. However, pandemic
fatigue could adversely affect the continued acceptance
One major public health concern is the reported VOC in of and compliance with public health and social measures
recent months. Several SARS-CoV-2 VOC have been identified by the population. The regional and country-level risks for
and preliminary evidence suggests that they may have COVID-19 remain very high given the evolving situation of
increased transmissibility or be associated with reduced COVID-19 across the Region, preparedness and response
virus neutralization among humans. Nonetheless, there is capacities of Member States and the numerous challenges
no strong evidence to date that these new variants have faced.
© WHO/EMRO
COVID-19 strategic preparedness and response plan – 2021 edition 93.3 Operational context
3.3.1 Humanitarian settings and vulnerable groups
The Eastern Mediterranean Region is home to nearly Additionally, as at 2019, there are 46 million professional
600 million people living across 22 socioeconomically and low-income labour migrants in the Region (of which
and geopolitically diverse countries and territories. Nine 22 million are from the Region), with differential access
countries of the Region are directly impacted by complex to and coverage of health services.10 Migrants and forcibly
humanitarian emergencies, and 43% of people in need of displaced populations, refugees in particular, are often
humanitarian assistance globally are located in the Region excluded from national programmes for health promotion,
(101 million people in total). As of 2019, the Region hosted disease prevention, treatment and care, as well as from
275 032 asylum-seekers, 11.8 million refugees (half being financial protection schemes for health, social services
Palestinian), 18.7 million internally displaced persons and and social protection. This exclusion could affect early
370 478 stateless persons.9 These populations are often detection, testing, diagnosis, contact tracing and treatment
vulnerable to poor health due to the conditions they live for COVID-19. In addition, it increases the risk of COVID-19
in and their limited access to needed quality health care. spreading within these populations, where the outbreak can
In addition, those who can access health care services are remain undetected.
often faced with financial hardship.
Moreover, due to limitations imposed by the pandemic,
the role of public health and humanitarian partners has
been further challenged. In a global survey conducted in
November 2020, health cluster partners reported facing
increased operational constraints in terms of insufficient
funding, human resources capacity and supplies in
safely delivering both COVID-19 response activities and
essential health services. Existing fragile health systems
in the Region have led to suboptimal disease surveillance
and preparedness and response capacities, making
countries particularly vulnerable to the emergence and
rapid transmission of novel pathogens. The COVID-19
pandemic has further exacerbated public health risks and
vulnerabilities especially among women and children in
© WHO/EMRO
emergency countries, requiring concerted efforts to address
the double burden of maintaining essential health services
in an emergency context and responding to COVID-19 as the
pandemic continues to evolve.
9
Population statistics [online database]. New York, NY: United Nations High Commissioner for Refugees; 2020 (https://www.unhcr.org/refugee-statistics,
accessed 1 March 2021; last update in December 2020).
10
World migration report 2020. Geneva: International Organization for Migration; 2019 (https://publications.iom.int/system/files/pdf/wmr_2020.pdf,
accessed 1 March 2021).
WHO EASTERN MEDITERRANEAN REGION 103.3.2 Effects on health systems and essential services
The pandemic has had a major impact on essential To ensure continuity of services, WHO has established a
health services. Lockdown measures imposed early on dedicated pillar on essential health services as part of the
in the pandemic, mobility limitations, the fear of getting SPRP to provide regular and tailored support to countries.
COVID-19 infection and closure of some services has led Numerous guidance documents and protocols have been
to less utilization of and accessibility to essential health published to guide countries in ensuring the continuity
services. The supply chain of various essential medicines of essential care. In this regard, the operational guidance
and vaccines was disrupted, leading to major shortages on maintaining essential services serves as the main
and further impacting the management of chronic illnesses. guidance12,13 alongside capacity-building materials and
Many gaps were highlighted in health system design and community-based guidance and assessment tools.
implementation, including coordination mechanisms,
supportive institutional arrangements, capacities and Countries in the Region have adopted a range of
supportive legislations, funding and equitable financing approaches to ensure continuity of health services, including
arrangements, qualified health workforce mix, and access to telemedicine and eHealth, capacity-building, supply chain
quality medicines and medical products. strengthening, modalities to reactivate and improve
access to services at primary and secondary care levels,
WHO has conducted various global surveys to better assess streamlining health care, and improving IPC across the
the impact of the pandemic on essential health services. A continuum of health care delivery.
rapid assessment was conducted in mid-202011 to which 13
countries of the Region responded (59%). The assessment
reported frequent disruption of essential health services
in the Eastern Mediterranean Region, with an average
disruption of 75% – higher than all other WHO regions (PAHO
was not included in the survey). An assessment in May
2020 shed light on the impact of the COVID-19 pandemic
on services for noncommunicable diseases (NCDs). With
responses from 19 (86%) countries in the Region, the most
common reasons for discontinuing or reducing services
were the closure of outpatient clinics and cancellation of
elective care (47%), insufficient staffing (26%) and NCD
clinical staff being deployed to provide COVID-19 relief
(32%). About half of the countries surveyed had partially
or completely disrupted NCD services. Similarly, results
© WHO/EMRO
of a rapid assessment on mental health and psychosocial
services (MHPSS) showed widespread disruption of these
services in the Region, despite the mental toll that COVID-19
and associated public health and social measures have taken
on individuals.
11
Pulse survey on continuity of essential health services during the COVID-19 pandemic: interim report, 27 August 2020. Geneva: World Health Organization;
2020 (https://www.who.int/publications/i/item/WHO-2019-nCoV-EHS_continuity-survey-2020.1, accessed 1 March 2021).
12
Analysing and using routine data to monitor the effects of COVID-19 on essential health services: practical guide for national and subnational decision-
makers. Interim guidance, 14 January 2021. Geneva: World Health Organization; 2021 (https://apps.who.int/iris/bitstream/handle/10665/338689/WHO-
2019-nCoV-essential_health_services-monitoring-2021.1-eng.pdf?sequence=1&isAllowed=y, accessed 21 February 2021).
13
Maintaining essential health services: operational guidance for the COVID-19 context. Interim guidance, 1 June 2020. Geneva: World Health Organization;
2020 (https://www.who.int/publications/i/item/WHO-2019-nCoV-essential-health-services-2020.1, accessed 21 February 2021).
COVID-19 strategic preparedness and response plan – 2021 edition 113.3.3 Social and economic effects
The COVID-19 pandemic has uncovered and intensified effects on gender inequalities: violence against women
existing social and health inequities. Evidence shows clear and girls has increased, girls have less access to online
socioeconomic inequities in rates of infection and mortality education than boys, and women have taken on more
from COVID-19 that reflect existing social, economic and unpaid household and caring roles with lockdown measures
geographic inequities. Moreover, containment measures in place. Mental health disorders have increased for a
have had significant effects on health inequities by variety of reasons such as financial pressures, social isolation
deteriorating the social determinants of health. and anxiety about the pandemic. While the challenges
are substantial and increasing, they also enable the
In countries of the Region, levels of food insecurity, identification of gaps to reduce inequities in the future. The
malnutrition and poverty substantially increased during Commission on Social Determinants of Health in the Eastern
2020. In some instances, this was associated with Mediterranean Region has recommended for Member States
containment measures and related decreases in income to position social justice at the heart of decision-making,
due to unemployment, reductions in working hours and and to foster a whole-of-society endeavour to improve
inadequate social protection mechanisms to provide health and reduce inequities.
sufficient support. The pandemic has also had significant
3.3.4 Public health and social measures
Since the beginning of the COVID-19 pandemic, countries and other education settings, and closure of public and
have been implementing public health measures to prevent social services. Levels of implementation, enforcement and
or slow the transmission of COVID-19, including individual, adherence to these measures have varied across countries
environmental or community measures in the form of and territories in the Region.
surveillance, response and social interventions. Various
social measures have been implemented by countries such The implementation of such measures can have
as mandating physical distancing, mandating mask-wearing considerable social and economic costs. Daily monitoring,
in public places, movement and travel restrictions, banning recording and analysis of these measures show that the
of gatherings and mass gathering events, closure of schools implementation of social measures is mostly not based
on an objective, evidence-based risk assessment, but
rather focuses on the epidemiological and socioeconomic
situations. In some countries of the Region, the
decision-making process has been skewed towards the
socioeconomic situation.
The Regional Office for the Eastern Mediterranean will
continue to raise awareness and disseminate WHO guidance
on performing risk assessments to inform decisions related
to public health and social measures. The Regional Office
has developed a dashboard that includes three layers of
data (public health and social measures, epidemiological
data and movement data) extracted from the Google daily
© WHO/EMRO
monitoring reports in the context of COVID-19. Monitoring,
recording and analysing of data from the dashboard,
including for modelling purposes, will continue to guide and
inform regional and national decisions.
WHO EASTERN MEDITERRANEAN REGION 123.3.5 Vaccines
Alongside public health and social measures to slow the included in the NDVPs. However, the inclusion of migrants
spread of the virus and reduce transmission, safe and could be challenging due to limited accessibility to vaccines.
efficacious vaccines are a powerful tool to rapidly control A monitoring mechanism to evaluate the implementation of
the pandemic if a large proportion of the global population the NDVPs should be ensured. Eligibility, target groups and
is vaccinated against COVID-19. Through the global solidarity review processes are yet to be developed in collaboration
initiatives, WHO has brought together public and private with humanitarian organizations. Formal approval of
sector donors, pharmaceutical and research companies, and Gavi is ongoing for allocation of the 5% buffer stock for
other experts to rapidly invest and support the development humanitarian use.
of COVID-19 vaccines. Within a few months of the pandemic,
several vaccines had reached phase 3 clinical trials and were The regional working group on COVAX has organized
showing promising results. By December 2020, the first several orientation webinars and virtual trainings targeting
vaccine was approved by regulatory authorities in different the Regional Immunization Technical Advisory Group,
countries and showed a high efficacy rate. the national immunization technical advisory groups,
WHO country offices, programme managers, and the
Safe and effective vaccines for COVID-19 are now available Expanded Programme on Immunization (EPI) focal persons.
and are already proving to be powerful tools in the global Furthermore, the Regional Review Committee, consisting of
effort to control the pandemic. All 22 countries and WHO and UNICEF regional staff members, headquarters staff
territories of the Eastern Mediterranean Region have joined members and partner organizations, with four to five people
the COVAX Facility and committed to global coordination per country panel, was established to review applications to
for the fair and equitable distribution of COVID-19 vaccines. COVAX. Several challenges have been identified in terms of
Of these countries, 11 were considered self-financing concerns regarding the delay of COVAX vaccines compared
countries (high-income countries) and 11 were eligible for to other vaccines, public acceptance of vaccine, and logistics
the Advanced Market Commitment (AMC) funded through support particularly in low-capacity and disrupted health
official development assistance ( low- and middle-income e systems.
countries, according to the World Bank classifications).
By 28 February 2021, 15 countries in the Region had
completed their readiness assessment using the COVID-19
Vaccine Introduction Readiness Assessment Tool (VIRAT/
VRAF 2.0). Eleven AMC countries had submitted their vaccine
request form to the COVAX Facility and outlined their needs
with respect to technical assistance, but none had reported
readiness regarding the ultra-cold chain. Development of
a national deployment and vaccination plan (NDVP) had
started in 14 countries in the Region and WHO is providing
technical assistance in finalizing the plans. Twenty-one
countries had provided emergency use authorization for at
least one vaccine. Thirteen countries had started COVID-19
© WHO/EMRO
vaccination and more than 11 million doses had been
administered to target populations. As many countries in
the Region are facing humanitarian crises, populations in
fragile, conflict and vulnerable settings are prioritized and
COVID-19 strategic preparedness and response plan – 2021 edition 133.3.6 Regional contribution to global research, development and innovation
In line with the COVID-19 Research and Development formally enrolled in the global Unity Studies initiative to
Blueprint, countries in the Region have continued to further the understanding of transmission patterns, severity,
accelerate innovative research to help contain the clinical features and risk factors for infection.
pandemic, facilitate care for those affected and contribute
to global research platforms. Ten of the 22 countries and Other countries also continue to conduct epidemiological
territories in the Region have joined the global quest research and publish in peer-reviewed journals. The Region
for an effective treatment: the WHO Solidarity trial. For has also been a hub of technological innovation, including
vaccine development, more than four countries have been the development of mobile applications for contact tracing,
involved in independent vaccine trials in collaboration with the creation of home-made cloth masks, the use of robots
manufacturers. For diagnostics, all countries in the Region for IPC in hospitals, innovative biomedical equipment, and
have been using commercial PCR tests and providing regular the use of digital health applications to maintain essential
feedback on their effectiveness. This role has been further health services. Additionally, the development and use
amplified since the emergence of the new variants and of mathematical models for decision-making on public
their detection. Three countries have also contributed to health and social measures, as well as to assess their
the evaluation of rapid immunoassay tests through sero- epidemiological impact, has been a highlight innovation
epidemiological studies. Moreover, eight countries have throughout the COVID-19 response.
3.4 Regional collaboration and coordination
Supported by WHO, all 22 countries and territories of the countries. The Regional Director has established mechanisms
Region have activated a national multisectoral coordination for engaging experts from the Region and beyond, as
mechanism to facilitate efficient and comprehensive well as other United Nations agencies, academia and the
response activities, with the active engagement of local media. The Regional Director also engages with United
partners and donors. Many countries have established Nations resident/humanitarian coordinators in the Region
a dedicated multidisciplinary committee to lead the through regular meetings to ensure their support to the
coordinated response reflecting, in most instances, a whole- COVID-19 response at the country level. In agreement with
of-government approach. Health clusters are utilized in nine ministers of health, a Ministerial Group on COVID-19 was
countries and lead the response with humanitarian partners established consisting of seven countries (Egypt, the Islamic
in the field to ensure adequate COVID-19-related service Republic of Iran, Lebanon, Morocco, Oman, Saudi Arabia
delivery and to ensure the continuity of essential health and Somalia). A dedicated technical working group held
services. a series of consultative meetings, during which countries
shared country-specific experiences highlighting successes,
In the WHO Eastern Mediterranean Region, the Regional challenges and lessons learned on COVID-19 response. As
Director closely engages with ministers of health on a daily a result, key recommendations were provided to guide
basis to update countries on new guidance and global and strategic plans for 2021 to strengthen preparedness and
regional concerns, build consensus and foster evidence- response in the Region.
based decisions, in addition to sharing experiences across
WHO EASTERN MEDITERRANEAN REGION 14A regional network of 35 technical and operational partners IMST has provided and continues to provide a management
was established that convenes virtually on a biweekly and coordination platform to escalate areas of concern
basis to coordinate support for country-level responses across the Region, tailoring the required support needed
and exchange updates. WHO has also continued to act as to overcome challenges and address needs. For 2021,
the health cluster lead in the response to the pandemic the IMST has revisited its structure to improve internal
at global, regional and national levels. In addition, WHO coordination across its different response pillars and
continues to leverage the capacities of the Global Outbreak improve monitoring and reporting. A vaccine pillar has been
Alert and Response Network (GOARN) and emergency added to IMST as pillar 10. This has fostered the integration
medical team initiatives to support country operations across and internal coordination between vaccine-preventable
the Region and globally. diseases and immunization (VPI), research, vaccine safety
and risk communication and community engagement
Within WHO’s Regional Office, the regional Incident (RCCE) components of the pillar. Pillar 10 will promote
Management Support Team (IMST) was established a comprehensive and integrated approach to COVID-19
in January 2020 and rapidly expanded to involve all response and facilitate the uptake of COVID-19 vaccines in
departments and expertise to tailor and address the regional different countries.
needs to curb and prevent further spread of COVID-19. The
© WHO/EMRO
COVID-19 strategic preparedness and response plan – 2021 edition 154. KEY LESSONS LEARNED FOR LEVERAGING THE COVID-19
RESPONSE IN THE REGION IN 2021
4.1 Partnership and coordination
• Coordination mechanisms were in place in many to ensure accountability, responsiveness and equitable
countries to support the response, including accountable access to quality health care. Furthermore, building
whole-of-government approaches to decision-making. trust between governments and communities at both
The most effective mechanisms were those in which national and subnational levels needs improvement,
the highest levels of government were fully engaged as demonstrated by non-compliance to public health
and followed the evidence-based guidance provided by measures. Collaborative governance and promoted
public health experts. However, these mechanisms need leadership skills and capacities in health decision-
to be better structured, maintained and strengthened making need to be strengthened for a whole-of-
through adjustments to their structure and operations government and whole-of-society approach.
using the lessons learned, such as optimizing the use of
emergency operations centres. • There is a need to better identify and acknowledge
specificities of the response in fragile, conflict and
• Governance arrangements and capacities demonstrated vulnerable settings. This will allow guidelines, response
gaps in delivering essential public health functions mechanisms and funding to be better tailored to enable
including gaps in coordination, oversight and adequate and timely response to COVID-19, and future
regulations, as well as in preparedness and response pandemics, in areas already affected by crises.
4.2 Communications (external and internal)
• The production of clear credible information and • Maintaining regular, timely and proactive
messaging, alongside ensuring its wide dissemination communications to highlight WHO’s position to key
via social media platforms and improving coordination stakeholders on key platforms raised the Region’s
with the media, is critical to fight misinformation/ profile, increased the number of followers, generated
disinformation and empower individuals, communities media coverage and established the Regional Office
and populations to adapt appropriate risk-reducing as a credible source of information, including by other
behaviours and improve knowledge, perceptions and WHO regions who use our materials on their platforms.
practices.
4.3 Operations support and logistics
• Maintaining a pre-positioned repository of essential delivery dates, as well as technical details such as
health commodities proved critical to the acute phase quantities, weights, volumes and expiry dates, is critical
of the response and enabled WHO to immediately and to WHO’s response.
rapidly distribute personal protective equipment (PPE)
and other essential medicines. • Expanding logistics capabilities across the Region,
in coordination with Member States, is required to
• The increased supply chain management requirements maintain current service delivery levels and to improve
associated with the COVID-19 response revealed the national-level distribution of supplies.
need to have qualified logistics/supply coordinators
based in all WHO country offices to facilitate the delivery • The digitalization of the COVID-19 Supply Chain System,
of medical supplies. established to centralize procurement and distribution
to help to overcome acute shortages of essential
• Increasing the visibility of supply chain data including supplies caused by the pandemic, should be explored to
financial commitments, physical locations and expected enhance WHO’s resilience to future health shocks.
WHO EASTERN MEDITERRANEAN REGION 16You can also read

















































