Covid-19 update 2020 DANIEL RODRIGUE, M.D. LEXINGTON INFECTIOUS DISEASE CONSULTANTS - Baptist Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Covid-19 update
2020
DANIEL RODRIGUE, M.D.
LEXINGTON INFECTIOUS DISEASE CONSULTANTS
5/12/20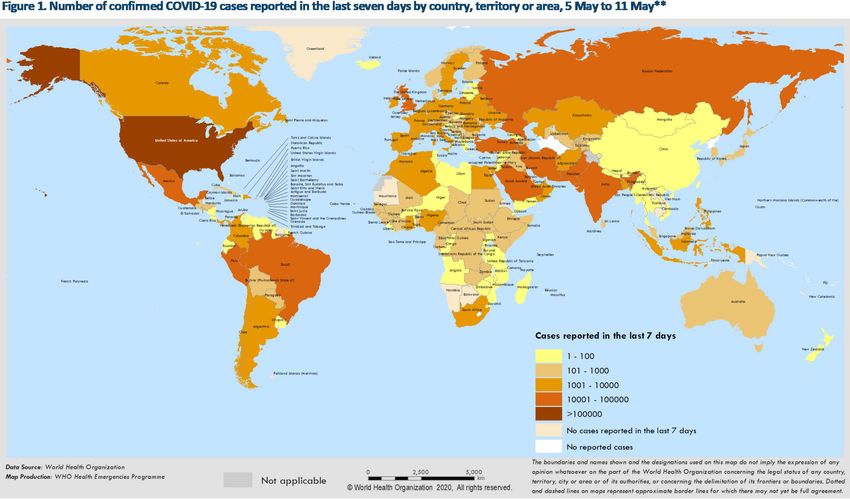
Covid-19 update
Thank you to family, health care workers, administrators, public
health, public servants, people of Kentucky
Covid-19 update objectives
Review latest epidemiology of Covid-19 outbreak
Review selected immunology of Covid-19
Review selected clinical aspects of Covid-19, general, HIV,
selected peds
Review current treatment of Covid-19
I have nothing to disclose
Covid-19 epidemiology
Cases > global 4.0 million to date, 278,892 deaths, Russia
increased incidence, behind US, Spain, UK, India
Case fatality rate 2%, with highest risk factors for age > 60,
comorbidities (obesity, HTN, COPD, DM, CAD, CKD, cancer); 5
d incubation (2-14 d), ?race (AA), ?gender (male)
Probable bat origin by genetic sequence
WHO.int 5/11/205/12/20
Covid-19 epidemiology
Most important transmission routes are droplet, contact,
and less aerosol. No good evid for vertical trans in preg
SARS-CoV-2 found in BAL (93% one study),
nasopharyngeal > nasal, oropharyngeal (less 32-40%,
and 92% in another small study, saliva being validated),
stool (29-53%), sputum (72% in one study), urine
(uncommon), blood uncommon (related to severity?),
not semen
SARS-CoV-2 found on (door handles, cell phones...)
Surfaces up to 9 d (usually less than 4 d), cardboard 24 h
and be disinfected w/ solutions > 60-70% ethanol, or a dilute bleach
solution, for at least 1 min (5 tablespoons bleach per gallon). Aerosol for at
least 3 h.
Influenza Other Respi Viruses. 2020;00:1–2; Lancet 2020;395:809; J Hosp Infect 1/31/20; NEJM 3/15/20;
JAMA 3/11/20; Gastroenterology 2/27/20 Xiao F, et al.MMWR 4/3/20, Kimball A
Covid-19 viral dynamics
18 patients were evaluated in Wuhan,
including 1 who never had symptoms)
within 2 family clusters
Measured sequential PCR in nasal and oral
specimens related to onset of symptoms
and found there was a high viral load from
the onset of symptoms, and in the 1
asymptomatic patient that was as high as
the symptomatic patients
PCR decreased over time with a sharp
decline by day 7-9 of illness, then a gradual
decline at 2 weeks from onset of illness.
NEJM 2020;382;12Covid-19 diagnostic tests
Reverse transcriptase polymerase chain assay (rT PCR)
Serologic diagnosis for IgM, IgA, IgG, qualitative and quantitative
Antigen test most recent FDA emergency use authorization (EUA) for
the Sofia 2 SARS antigen FIA (Quidel corporation) for point of care
testing in a laboratory certified under the Clinical Laboratory
Improvement Amendment of 1988 (CLIA), or CLIA waved as of May
8, 2020. 15 min test.
Assay is a lateral flow immunofluorescent sandwich assay used
with the Sofia 2 Instrument to qualitatively detect the
nucleocapsid protein from SARS-CoV-2 in NP and nasal
specimens, after swabs added to viral transport medium.
Sensitivity was 80%, specificity was 100% (based on 143 samples
for FDA EUA approval). A neg test needs to be confirmed by a
molecular test.Covid-19 serologic test
performance
Abbot Architect (high throughput ELISA) IgG Sens 100% (88/88), Spec 99.6% (1066/1070), PPV at prev
5% 92.9%
Autobio (lateral flow) IgM Sens 85.4% (346/405), IgM Spec 99.7% (311/312), IgG Sens 86.2% (349/405),
Spec 99.4% (310/312), Combined Sens 88.1%, Spec 99%, PPV at prev 5% is 82.9%
Bio-Rad Platelia (ELISA) Pan-IG Sens 92.2 (47/51), Spec 99.6 (684/687), PPV at 5% prev was 91.7%
Cellex (lateral flow) combined IgM/IgG Sens 93.8% (120/128), and Spec 96% (240/250), PPV at 5%
was 55.2%
Chembio Diagnostic Systems (lat flow) IgM Sens 77.4 (24/31), IgG Sens 87.1% (27/31), Combined Sens
93.5%, Spec 94.4%, PPV at 5% prev is 46.8%
Diasorin LIAISON (ELISA) IgG Sens 97.6%, Spec 99.3%, PPV 88% at 5%
EUROIMMUN (ELISA) IgG Sens 90%, Spec 100%, PPV 100%
Mount Sinai Hospital (ELISA) Combined Sens 92.5%, Spec 100%, PPV 100%
Ortho-Clinical Diagnostics VITROS (ELISA) IgG Sens 87.5%, Spec 100%, PPV 100%
ROCHE Elecsys (ELISA) Pan-Ig Sens 100%, Spec 99.8%, PPV at 5% prev, 96.5%
WADSWORTH New York (ELISA) Pan-Ig Sens 88%, Spec 98.8%, PPV at 5% prev 79.4%
FDA.gov 5/10/20Predictive value of screening antibody Covid-
19 test w/ 95%, sensitivity and 95% specificity
Positive test in this setting not useful and more likely false positiveCovid-19 epidemiology
Superspreading events important. Spring
Festival, Wuhan, Mardi Gras, New Orleans,
church events, California. Maintain high
vigilance as recurrent outbreaks occur
(Singapore, China reports).
Planning for contingencies with reopening
and loosening of restrictions, with
surveillance for resurgence of cases. What
happens in fall with schools, sporting
events?
Every 1 person with Covid-19 probably
infects 2.2-2.68 persons (R)
Lancet 2/27/20, 1/30/20, Lancet 1/31/20, Lancet Resp Med 2/3/20; Int J
Trav Med 2020,Covid-19 and structural
vulnerability in the US, and waves
First wave of infection with limited community transmission to a
immunologically naïve population, reaching elderly and frail living in
conglomerate settings. Feb to March 2020, 140 nursing homes,
March to April 2020, > 2500 nursing home fueled by visitors and
contacts w/ HCW, and group gatherings
Second wave of transmission early March to present with sustained
community transmission in cities with large population density, high
prev of chronic disease, all states involved by Mid-March, service
industry, day laborers, immigrants, delayed lockdown, insurance
Third wave early April to present increasing in prisons/jails, high prev
of chronic disease, conglomerate populations in crowded facilities,
and workers also going back into community
Am. J. Trop. Med. Hyg., 00(0), 2020, pp. 1–3, Solis, J, et alCovid-19 and prison systems
Prisons amplify outbreak. Crowding, poor sanitation, and increased
population w/ risk factors for serious outcome. 11% of US inmates
age 55 y or older. 1918 Spanish Flu, ½ of the inmates of San
Quentin’s 1900 inmates became ill. 400 inmates at Green River
Correctional Complex, 57 (to > 200 by report 5/11/20) inmates at
FMC, and 3 employees on 5/7/20 positive. Marion Correctional
Institution in Ohio with 2000/2500 inmates positive for Covid-19
3/15/20 1st Covid case at Riker’s Island, NY, then 200 cases in 2
weeks. New York City, 378 cases of Covid-19 among inmates of city
jail, 10% infection rate
2.2 million persons in prison in the US, up to 10.6 million cycle through
the system per year with average LOS 25 d. International issue.
July 2020, Vol 110, No. 7 AJPH, Lancet 5/2/20, Vol 395:1411, JAMA 4/28/20, E1, MMWR / May 8, 2020 / Vol. 69Covid-19 and meat and poultry
workers
Covid-19 cases among US workers in 115 meat and
poultry processing facilities reported by 19 states
130,000 workers, 4,913 cases (3%, but ranged from 0.6%
to 18.2%), and 20 deaths reported; nationwide industry
employs about 500,000 workers
Risk increased related to workplace physical distancing,
hygiene, crowded living, and transportation conditions
MMWR / May 8, 2020 / Vol. 69 / No. 18Reorganizing the meat packing plant for Covid-19,
Tyson Foods, Waterloo, Iowa 5/10/20, NYT
5/12/20
RodrigueHCW and Covid-19 in US 2/12-4/9/20
9282 US HCW reported, 3% of
reported cases in US, but
underestimated as data
incomplete; in those states with
more complete reporting, 11%
were HCW
Median age 42, 73% female, and
8-10% were hospitalized, and age
and comorbidities important
National workforce of about 18
million HCW
MMWR / April 17, 2020 / Vol. 69 / No. 15Lancet 5/7/20, doi.org/10.1016/ S0140-6736(20)31100-4
Covid-19 HCW infection review
Incidence is variable across many different reports from 3.8% to
38.9%. Prevalence by seropositivity ranged from 0.3% to 40% in 6
studies. Highest in an outbreak in Vietnam without isolation ward.
Risk factors for HCW include suboptimal handwashing, improper
PPE, having a diagnosed family member.
Risk reduction most consistent w/ proper use of masks (surgical and
N95). Most studies found assoc between use of gloves, gowns, eye
protection, or shoe covers, and decreased risk for HCW infection.
Ann IM 5/5/20, Chou R, et al.Covid-19 US epidemiology
1.3 million cases in the US, 79.756 deaths, 50 states, 5
jurisdictions (4/27/20), WHO Pandemic called on 3/11/20, US
State of Emergency called 3/13/20
First death in US was patient from California in Santa Clara
County now identified by medical examiner 2/6/20, sent
samples to CDC (died at home), at that time US cases
numbered in the 10’s. Reported 4/21/20. Community
transmission was earlier than previously thought.
States with largest numbers include New York, New Jersey,
California, Michigan, Massachusetts, Florida, Illinois,
Louisiana, Georgia, Texas, Washington, Penn. Not a
simultaneous outbreak in terms of surge/peaks.
NEJM 2020, Feb 28, CDC.gov 5/10/20; kycovid19.ky.gov, 4/1/20; 4/21/20 Santa
Clara County Public Health DeptCovid-19 US epidemiology
15.7% of resp specimens testing positive at public health labs and
10.2% at clinical labs, 18.0% at commercial labs (cumulative
4,882,263 tests done 3/1/20 to 5/2/20)
Covid-19 associated hospitalization rates since 3/1/20 overall
cumulative of 50.3 per 100,000, with up to 162.2 per 100,000 for
persons age 65 or older, and 79.0 for persons 50-64 y old.
COVID-NET surveillance system in 99 counties in 14 states. Among
patients hospitalized, 75% were > = 50 y, and 89% had one or more
chronic conditions including HTN (50%), obesity (48%), chronic lung
disease (35%), DM (28%), cardiovascular dz (28%)
COVID view 5/8/20CDC.gov 3/15/20
CDC.gov 5/11/20
Covid-19 outbreak, United States, May 11, 2020 CDC.gov 5/11/20
First case KY reported on 3/6/20. 6677 cases, 104,001 tested now in KY as of 5/11/20, 311 deaths. KY declares a state of emergency 3/6/20. Peak cases estimated 4/16-5/1/20. 74% white, 15% black, 6% Asian, 13% Hispanic, 47% male
Covid-19 cases per 100,000, days since 100th case, 5/10/20
https://github.com/CSSEGISandData/COVID-19Epidemic curve model Covid-19 Kentucky 2020, IHME model, 5/8/20
Kentucky Covid-19 infections and testing 3/1/20 to 8/1/20
Kentucky Covid-19 deaths, estimate 5/8/29, IHME, 703 by 8/4/20
Ebola and Flu SARS-CoV-2 Measles
1-2 people 2-3 people
12-18 people
R○ is a function of 3 primary parameters including the duration of contagiousness after a person
becomes infected, the likelihood of infection per contact between a susceptible person and an
infectious person, and the contact rate.
Emerg Infect Dis 2019;25:1Covid-19 anatomy
Acta Pharm Sine 2/18/20
Covid-19 pathogenesis
SARS-Cov-2 enters the cell by attachment of
the viral spike S proteins to ACE-2 receptor on
cell, and the S protein is primed by a serine
protease TMPRSS2
ACE2 receptors are abundantly present in
humans in the epithelia of lung and GI tract,
but also other tissues and organs, and oral
tract
Cell 2020 Mar 4; Picture from Nature 3/5/20; J of Pathol 2004;203:631Clinical Rheumatology https://doi.org/10.1007/s10067-020-05073-9
Fu et al. J Transl Med (2020) 18:164
Interleukin 6 (IL-6) signaling cascade. Fernanda I Arnaldez et al. J Immunother Cancer 2020;8:e000930
Inflammation in Covid-19
Similar to SARS and MERS, patients with Covid-19 with
increased plasma concentrations of inflammatory
cytokines including TNFalpha, IL-2,7,10, granulocyte (G-
CSF), monocyte chemoattractant protein 1,
macrophage inflamm prpotein 1 alpha, interferon-
gamma-inducible protein 10
Lung path with infiltrating monocytes, lymphocytes, and
plasma cells, w/ CD3, CD4, CD20, CD79a, CD5, CD38,
and CD68.
Inflammatory monocytes in peripheral blood with CD14,
CD16 phenotype, and large amounts of IL-6 from these
cells.IL-6
IL-6 is a small polypeptide prod by all stromal cells and
immune system cells (B, T, macrophage, monocytes,
dendritic cells, mast cells, fibroblasts, endothelial,
keratinocytes, mesangial cells, tumor cells)
Main activators of IL-6 expression are Il-1B, and TNF-
alpha, as well as Toll-like receptors, prostaglandins,
adipokines, stress, and other cytokines.
IL-6 binds to its receptor IL-6R forming a complex, then
binds membrane protein gp130 to initiate intracellular
signal transduction. Can have a soluble IL-6R.
Next step is activation of JAK-STATA pathway, and RAS-
RAF pathway, SRC-YAP-NOTCH pathway, and AKT-P13K
pathway .IL-6
IL-6 promotes T cell population expansion and
activation, and B cell differentiation, regulate acute
phase response, affect hormone-like properties of
vascular disease, lipid metab, insulin resist, mitochond
activity, neuroendocrine system, and neuropsych
behavior.
doi.org/10.1016/j.ijantimicag.2020.105954Fu et al. J Transl Med (2020) 18:164
Adapted doi.org/10.1016/j.jaut.2020.102433
Covid-19 clinical symptoms signs
Dysgeusea,
Kawasaki anosmia, rashes,
neurologic
syndromes, eye
findings,
conjunctivitisCovid-19 clinical
Symptoms are not easily distinguished from other viral
illness, incubation period about 5 days (2-14 d)
Viral syndrome, fever, cough, loss of taste (dysgeusea),
and smell (anosmia) can be presenting signs (up to
30%), diarrhea, fatigue, sob. 1st week (5-10 d) usually
milder (viral load high, dev ab) into 2nd week tipping
point, where you can develop severe illness (watching
RR, sob, hypoxia). Viral load decreasing toward end of
2nd week.
Onset to hospital admission about 4-7 d; can develop
the fever after admission.
Lancet. 2020;395(10223):497-50, Lancet. 2020;395(10224):565-574; N Engl J Med. 2020;382(8):727-7336, Lancet
2020; 295:200; BMJ 2020;368:m606; JAMA 323:1061 March; ENT UK, Laryngoscope 2007;117:272Covid-19 patient hospital day 1, illness day 3, KY
Ann IM 5/6/20, Wichman DCovid-19 and outcome of
immunosuppressed child/adults
A series of 110 immunosuppressed
patients, and seem to be less of a
factor in outcome, compared to
other chronic diseases (DM,
obesity, etc)
No large series of HIV patients with
Covid-19. Small series from
Germany 33 patients without
significant outcomes related to
HIV (median CD4 count 670/mm3).
42% admitted to hospital, 91%
recovered. 3 died (one age 82
yo, one w/ CD4 69, and another
w/ severe COPD, DM2, and HTN).
doi.org/10.1101/2020.04.28.20073767; doi.org/10.1016/j.jinf.2020.04.026, J Infect, Minotti, CCovid-19 and cancer
Review from 5/2/20 discussed various aspects regarding Cancer
care and Covid-19
Some data reported on adverse outcomes among cancer patients
infected with Covid-19 with a mortality rate of 28.6% in one series of 28
patients in China compared w/ 2.3% for other Covid-19 patients.
Recommended institutional guidelines regarding cancer care, and
accessing oncology society guidelines available from European Society
of Medical Oncology, American Society of Clinical Oncology, National
Comprehensive Cancer Network to mitigate the neg effects of Covid-
19 on the diagnosis and treatment of cancer patients
Curr Oncol Rep (2020) 22:53, Ann Oncol 2020, Zhou, et al in pressFramework for prioritizing management of cancer patients in Covid-19 pandemic Curr Oncol Rep (2020) 22:53
Covid-19 and children
One meta-analysis from Chinese data generally not a severe illness
in children. Most obtain their illness from family members. Little
evidence for perinatal transmission, and inconclusive regarding
breast milk transmission. Most not hospitalized. Most common
manifestations include viral syndromes w/ fever, sore throat, dry
cough, and URI symptoms. Uncommon for severe disease. Can be
asymptomatic. Most common underlying condition include
asthma, cardiac dz, immunosuppression, DM, obesity, CKD/dialysis
Reason for less severe disease unclear but may be related to their
immune system, level of ACE2 receptorsCovid-19 and peds MMWR / April 10, 2020 / Vol. 69 / No. 14
Covid-19 and Kawasaki
disease in children
Most common cause of childhood acquired heart
disease in industrialized nations, about 1/6000 children,
but more common in Asia (1/1000 in Japan), 2.5 times
higher in Asian children. Winter and spring increase, and
multisx disease.
Acquired vasculitis, typically 50% of cases of KD in those <
2 yo, and 80% in those < 5 yo. Classic KD with fever 5 d,
and 4/5 clinical criteria in absence of other dx (including
conjunctivitis, lip/tongue/mouth erythema, trunk macpap
rash, and swelling hands/feet, lymph node swelling)
Noted increase in ICU cases in France in April, 2020, and
also reported in UK, NYC, and LA county. Pediatric
multisx inflammatory syndrome potentially assoc with
Covid-19.Covid-19 clinical summary general
Symptoms not specific. Labs not diagnostic, but more often with
normal WBC. CBC often with lymphopenia (40% in one study)
Labs associated with increased risk of mortality included
lymphopenia (< 0.8 absolute count), CRP > 100, leukocytosis,
elevated absolute neutrophil/lymphocyte > 20, elevated ferritin >
300-500 ug/L, creatinine, procalcitonin, elevated LDH > 245 U/L, d-
dimer > 1 ug/ml, IL-6 > 11 pg/ml, ALT in one study; SOFA score > 4
Median duration of viral shedding 20 d, higher viral load in
nonsurvivors (Lancet article 295:200)
Most adults < 60 y, 2 week illness, but 3-6 weeks for severe dz.
Cough can persist 12-19d, fever 4-15 d, Any symptom may persist up
to 24 days (variable).
Lancet. 2020;395:497-50, Lancet. 2020;395:565-574; N Engl J Med. 2020;382(8):727-7336, Lancet
2020; 295:200; Lancet 3/9/20, Zhou; NEJM 2/28/20, Guan W; Chin Med J, DOI:
10.1097/CM9.0000000000000824, Deng Y.Representative clinical timeline with PCR
and antibody titers Covid-19
PCR viral
1.2
respiratory
Mild disease 5-14 d Sev ere disease 7-days to w eeks
1
IgM IgG
0.8 Asx or presx 3-5
days
0.6
0.4
Viral response Hyperimmune
0.2 response, cytokine
0
1/1/20
1/2/20
1/3/20
1/4/20
1/5/20
1/6/20
1/7/20
1/8/20
1/9/20
1/10/20
1/11/20
1/12/20
1/13/20
1/14/20
1/15/20
1/16/20
1/17/20
1/18/20
1/19/20
1/20/20
1/21/20
1/22/20
1/23/20
1/24/20
1/25/20
1/26/20
Mild SevereCovid-19 severe disease and death
Progression to severe disease usually within end of 1st week
to second week (8-14 d), and of those with ARDS mortality
ranges depending on series (18-50%). AKI (7%), acute
cardiac injury (12%), ICU admission (5-30%, probably less),
secondary infection not common about 5%. Severe illness
in 10-15% of cases, more common in older age group (> 60
y and espec > 80 y), and those with comorbidities.
Cause of death ARDS, thromboembolic dz, myocarditis,
sepsis. Prospective autopsy study of 12 consecutive deaths
found DVT in 58% in whom venous thromboembolism not
suspected. All patients had high conc of SARS-CoV-2 in
lung, and 5/12 w/ evidence of virus in lung, kidney, heart
Lancet 2/21/20, Trav Med and Infect Dis 3/11/20, Ann IM 5/6/20, doi.org/10.7326/M20-2003Covid-19 clinical monitoring
O2 saturation, RR, vitals
Typical labs to follow include:
Daily CBC with differential, complete metabolic panel, CPK,
CRP, ferritin, procalcitonin level, lactic acid, D-dimer daily if
elevated, LDH daily if elevated, troponin and repeat if
elevated on admit. EKG baseline, fibrinogen/PT/PTT.
Admission acute hepatitis serology, HIV, UA, blood cx if
indicated (2 sets)
IL6 if hospitalized with risk factors for poor outcome based on
age and chronic illness
Radiographic studies, do not need repeat CT scans unless
clinically indicatedCovid-19 predicting who gets
severe
CALL scoring system (Comorbidities, Age, Lymphocyte count, LDH),
if score 4-6 points then less likely severe disease
Other markers RR > 24, lymphopenia (< 0.8 absolute count), CRP >
100, leukocytosis, elevated absolute neutrophil/lymphocyte > 20,
elevated ferritin > 300-500 ug/L, creatinine, procalcitonin, elevated
LDH > 245 U/L, d-dimer > 1 ug/ml, IL-6 > 11 pg/ml, ALT in one study;
SOFA score > 4
New York series of 4103 patient, 1999 hospitalized, 292 died, 445
patients (22%) required mech vent, 162/445 (36%) died. Strongest
critical illness risks were associated w/ admit O2 sat < 88%, d-dimer >
2500, ferritin >2500, CRP > 200. Some not as focused on admitting
features but monitoring CRP during hospital stay
CID 4/9/20, Ji D; https://doi.org/10.1101/2020.04.06.20054890; .
doi.org/10.1101/2020.04.08.20057794; doi.org/10.1101/2020.04.23.20076653Covid-19 treatment general
measures
Shorten length of stay for patients, and consider discharge with
telemedicine follow-ups
Chose medications, laboratories, procedures with the the goal of
providing most effective care and minimizing exposure in order to
protect other patients, and health care personnel
Once a day medications if possible
Minimizing blood draws, and radiographic tests
Continue delivering care to those without Covid-19
Watch for moral injury, PTSD, increased stress levels among HCW,
and build capacity for relieving HCW/backup now, not before the
increase in casesCovid-19 treatment
Supportive care
Oxygen may be required, especially in high risk populations with
ventilator use in as many as 6.1% reported from Wuhan, but less
in Singapore study. 41% of hospitalized patient require O2, and
70% of severe cases.
In Italy, 9-11% of their patients between 3/1/20 and 3/11/20
required ICU care. Ventilators became a scarce resource.
John Hopkins estimated US with 160,000 ventilators, and 8,900 in
national stockpile, and a previous study modeling pandemic like
1957 influenza estimated a need for 64,000 vents, and 1918 flu,
740,000 vents
Be careful about urge to focus on vents and ICU at expense of
general capacity, public health. Effect of public health
measures such as social distancing, vs need for ventilators.
Ann IM, 5/7/20, Halpern S et alCovid-19 treatment
Antibiotic use common because of difficulty in
distinguishing bacterial infection and were used in 53% of
non-severe, and > 90% of severe disease. Secondary
bacterial infections in one study of critically ill patients
11%, and Zhou (15%), but meta-analysis 6%.
Anticoagulation treatment in patients w/ elevated d
dimers, either with enhanced prophylactic
anticoagulation or full anticoagulation depending on
coagulopathy, with attention to bleeding (higher risk if
age > 40 y, hep fail, GFR < 30 ml/m, ICU, CCU, central
venous cath, RA, CA, male, PUD, bleeding 3 mo prior, plt
< 50)
Lancet 4 9 29 doi.org/10.1016/S2352-3026(20)30109-5MMWR March 18, 2020 vol 69
Covid-19 time course respiratory
failure
Early on with relatively good compliance despite poor oxygenation.
High minute ventilation, ground glass on CT w/ interstitial rather than
alveolar edema. Pts not overtly dyspneic. (Type L, low lung
elastance, high compliance), and low response to PEEP.
May transition to more typical ARDS (because of severity, host, or
suboptimal management) w/ extensive CT consolidation, low
compliance, higher lung weight, and high PEEP response (type H).
Active coagulation cascade, with widespread micro- and macro-
thromboses in lung, w/ high d-dimers.
Disproportionate endothelial damage disrupts vasoregulation,
promotes V/Q mismatch, and fosters thrombogenesis. Increased
resp drive may intensify tidal strains and energy loads incr injury.
JAMA 4/24/20, Gattinoni, LJAMA 4/24/20, Gattinoni, L
Covid-19 and treatment lessons
from history
As of 5/2/20, clinicaltrials.gov listed 681 interventional trials for potential
therapy for Covid-19, and another 437 observational studies listed
Previous responses to national emergencies led to Manhattan Project In
WWII, mass production of penicillin, polio vaccine in the 1950’s
promoted by Joe DiMaggio and Lucille Ball
But pressurized research also led scientists to unknowingly formulate
vaccines that infected tens of thousands of Gis with hepatitis,
accelerated vaccine development w/ the onset of the swine flu
threatening the US, and the resulting Guillain-Barre disease related to
the flu vaccine
Caution in using medRxiv non peer-reviewed data to drive treatment
decisions. Difficult to balance the tensions between doing something,
and practicing evidence based medicine.
Annals IM, May 7, 2020, Doroshow D, et al.Covid-19 treatment 5/12/20
Nature Rev 2020;19:149, JID 2017;216:203; Roche
Steroids may prolong viral shedding if used early; but
may have role in ARDS, shock in ICU, and cytokine storm
No FDA approved treatment but under investigation
(NIH, IDSA guidelines 5/12/20, work in progress)
Remdesivir, convalescent plasma, Tocilizumab IL-6
inhibitor, steroids in ARDS/cytokine syndrome,
favipiravir, hydroxychloroquine, sarilumab trial, monoclonal
ab to IL-6, lopinavir-ritonavir
Vaccines about 15 under development 12-18 mo awayCovid-19 treatment Remdesivir
5/12/20
Remdesivir (investigational)
Gillead , initially developed for Ebola, inhibits RNA-
dependent RNA polymerase with in-vitro activity
against MERS, SARS, and animal models, and invitro vs
SARS CoV-2
Numerous trials and compassionate use at 200 mg IV
x 1, then 100 mg IV daily x 5-10 d
ADR include increased liver enzymes, potential drug-
drug interactions with meds metabolized through
cytochrome system
https://www.ahfscdi.com 3/27/20, UW, UMICH; AAC 3/23/20 Li H, et al;
https://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1922083117/-/DCSupplementalCovid-19 treatment Remdesivir
5/12/20
Remdesivir trial compassionate use NEJM 4/10/20, 61
patients with some acute hypoxic resp failure received
10 d course of 200 mg IV x 1, then 100 mg IV daily,
1/25/20 through 3/7/20
57% were on mech ventilation, 8% ECMO
Median f/u of 18 d, 68% improved oxygenation, 57%
were extubated, 47% were discharged. 13% died, and
mortality was 18% among patients with mech ventilation,
and 5% among those not on mech ventilator
NEJM 4/10/20, Grein J et al.Covid-19 treatment Remdesivir
5/12/20
Interim analysis of > 1000 patients and pulm involvement resulted in
faster recovery time (11 d vs 15 d with placebo), not signif change in
mort (8 vs 11.6%).
Chinese study of 237 patients with severe Covid-19, time to
improvement not different (median 21 d, vs 23 w/ placebo). No diff
in mortality at 28 d, or time to viral clearance. Among those who
received treatment within 10 d of sx onset, there were trends toward
lower mort and more rapid improvement with remdesivir. Most pts
with other therapies which confounded the findings.
Gillead press release reported 5 d similar outcome (recovery and
discharge, 65%, 60%) to 10 d of remdesivir (54%, 52%), and mort at
day 14 of 8 and 11%.
https://doi.org/10.1016/S0140-6736(20)31022-9 , Lancet 4 29 20Covid-19 hydroxychloroquine
5/12/20
Hydroxychloroquine—routine use no longer recommended outside
of a clinical trial, although if used, would be in patients with SpO2 < 94%
on RA, Cr clearance < 50 mg/min, ALT or AST > 5x ULN, and non-
pregnant adult. Consider also if have significant risk factors for
progression. Doses used include adult 400 mg bid loading, then 200 mg
bid for 5 d course. NIH, IDSA guidelines 5/12/20 rec use in clinical trial.
Premature discontinuation of high dose trials in Brazil. VA retrospect
study w/ 368 patients reported incr risk of death in HC treated pts w/ no
change in vent use. Open label trial in China 150 pts using high dose
HC without benefit in viral seroconversion at 28 d, or survival, w/
increased toxicity. New York city report 5/11/20 no diff in outcomes with
HC (sample of 1438 patients). Another NYC 1876 pt, 59% treated w/ HC,
no assoc w/ intubation or death.
Cardiac toxicity primary concern. Qtc prolongation, monitor, and can
cause dizziness, HA, loss of appetite, nausea, vomiting, monitor EKG
Qtc, and while no dose adjust in renal, monitor Qtc, retinal tox usually
w/ longstanding use.
https://doi.org/10.1101/2020.04.16.20065920; 2020:2020.04.10.20060558; JAMA. doi:10.1001/jama.2020.8630;
NEJM 5/7/20, Geleris JFu et al. J Transl Med (2020) 18:164
Covid-19 immune mod treatment
5/12/20
Immune modulators—potentially for cytokine storm
patients, who are worsening in the absence of other inf
Tocilizumab IL-6 inhibitor (humanized anti-IL6 antibody) being
evaluated in trials for treatment of moderate to severe COVID-
19, approved 2017 for other illnesses including RA, CAR-T…(half
life 14-21 d)
Monitor for hyperinflammatory cytokine syndrome with IL-6 levels
ChinaXiv:202003.00026v1
(usually > 3x ULN), ferritin (>300 ug/L and doubling over 24h, or >
600 ug/L at presentation, and LDH > 250 U/L), low platelets, CRP
elevation (> 10, or 100 in high sens), PCT (to eval for bacterial
infxn), fibrinogen, elevated D-dimer (> 1-5 mg/L)
Xu X, et a,
15/21 patients treated in Wuhan, China improved (not peer-
reviewed data), also received steroids, Kaletra…Covid-19 immune mod treatment
5/12/20
Tocilizumab trial in France open label study randomized
129 pts at Assistance Publique-Hospitaux de Paris in mod
to severely ill patients w/ 65 tocilizumab plus SOC, vs 64
patients w/ SOC reported lower proportion in toci arm
who died or required mech ventilation (4/27/20)
Tocilizumab reported used in 15 patients single center in
China w/ steroid, and reported less success, and possible
need to repeat doses as IL-6 increased in 4 patients after
admin.
DOI: 10.1002/jmv.25801, J Virol 3/26/20; Assistance Publique-Hospitaux de Paris press release 4/27/20Covid-19 immune mod treatment
5/12/20
100 prospective patients from Spedali Civili University Hospital in
Brescia Italy, 3/9 to 3/20 w/ Covid received Tocilizumab 8 mg/kg
every 12 h x 2 doses
88% male, median age 62 yo, 43 in ICU, 57 others in general ward
(no ICU available)
37/57 (65%) improved and were able to stop NIV, 10 died. Of 43
patients in ICU, 32 (74%) improved. 17 taken off vent, 10 died (24%)
77 (77%) of all patients improved. 23 (23%) worsened. In the 10 d
follow-up, 2 developed sepsis and died, and one w/ GI perf.
https://doi.org/10.1016/j.autrev.2020.102568, Toniati, P, et al.Covid-19 immune mod treatment
5/12/20
25 patients from Quatar, 92% male,
58 yo median age, w/ chronic dz,
received tocilizumab and followed
for 14 d.
Invasive vent from 21 (84%) at day 1,
to 7 (28%) on day 14.
doi: 10.1002/jmv.25964Covid-19 and steroids
5/12/20
Pathogenesis of Covid-19 is a result of viral receptor, viral replication,
and host immune response
ARDS meta-analysis of 9 RCT prior to Covid-19 were mixed but led to
recommendations by SCCM, and ESICM to use for patients with
mod to severe ARDS. Guidelines in septic shock 2017 guidelines rec
use for at least 3 d or longer in those not responding to fluid and
vasopressor.
Meta-analysis of 1781 critically ill Covid-19 pts without diff in mort,
and another meta-analy by Lu reported increased secondary
infection, but did decrease fever (13,815 pts); another meta-analy
of 5270 pts by Yang report incr mort. Steroids prolonged SARS viral
shedding in past, and incr mort in MERS.
https://doi.org/10.1016/j.jinf.2020.03.062
https://doi.org/10.1101/2020.04.17.20069773 https://doi.org/10.1101/2020.04.17.20064469Covid-19 convalescent plasma
5/12/20
Ongoing evaluation
Data from previous SARS outbreaks, MERS, Spanish Flu,
Swine flu meta-analysis show some survival benefit, used
in Ebola as well
Duration
of critical care support, and ICU stay not
much change
Hospital stay may shorten
Studies of variable quality
Use earlier than later also the general message
JID 2015:211 (1 January) • Mair-Jenkins et alCovid-19 convalescent plasma
5/24/20
5 critically ill patients with ARDS, mechanically vent treated in
Shenzhen Third People’s Hospital (1/20/20-3/25/20)
Age 36-65, 2 women, minimal chronic disease (HTN, mitral dz in 1 Pt)
Donors were at least 10 d without sx, ABO compatible, screened for
Sars-CoV-2, other resp viruses, hepatitis B, C, HIV, syphilis, and had a
serum specific Ab titer > 1:1000, and neutralizing Ab titer > 40. 400
ml obtained from donor and given the same day to recipient.
Patients received plasma between 10-22 d after admission
Clinical improvement with improvement in temp, SOFA scores, viral
load, and ARDS resolved in 4 patients at 12 d after transfusion, and 3
patients discharged from hospital (LOS 53, 51, 55 d). Pts also on
steroids and other rx including lop/rit, interferon, favipiravir
JAMA online 3/27/20, Shen C, et alhttps://www.pnas.org/cgi/doi/10.1073/pnas.2004168117 CP = Convalescent plasma
Covid-19 immune
therapy
Need evidence of antibody titers, not all
convalescent donors have same titers and some
previous evidence that titers make a difference
Some adverse effects could include mild fever,
allergic reactions to life-threatening
bronchospasm, transfusion related lung injury,
and circulatory overload in patients with
cardiorespiratory disorders, antibody dependent
enhancement of infection (ADE)
Coordinating potential donors from
convalescent patients w/ resolved sx, negative
PCR NP, and defined SARS-Cov-2 neutralizing ab Human monoclonal ab block ACE2
titer > 1:80; Mayo Clinic Expanded Access inhib, Chen X, et al, Cell Mol Immun
received $26 mill grant BARDA 5/4/20
Hyperimmune glob, monoclonal antibodies
JAMA 3/27/20, Roback, JD, et al, Antiviral Ther 2018; 23:617;
https://doi.org/10.1038/s41423-020-0426-7, FDA guidedance 5/1/20Covid-19 and lopinavir/ritonavir,
interferon beta 1-b/ribavirin
127 patients in a randomized open label, phase 2, recruited from
Hong Kong (86 combo, 41 control)
Showed shorter duration to neg PCR NP swab (7 d vs 12 d), clin
improvement (shorter time to complete alleviation of sx (4 d vs 8 d),
shorter LOS (9 d vs 15 d).
Used interferon beta-1b early (within 7 d of sx onset), and may also
be a lesson for use of lopinavir/ritonavir to use early where previous
study initiated within 14 d of symptom onset
https://doi.org/10.1016/ S0140-6736(20)31042-4 Lancet, Hung, I, et al.Draft subject to change soon
Representative clinical timeline with PCR
and antibody titers Covid-19 4/28/20
PCR viral
1.2
respiratory
Mild disease 5-14 d Sev ere disease 7-days to w eeks
1
IgM IgG
0.8 Asx or presx 3-5
days
0.6
0.4
Viral response Hyperimmune
0.2 response, cytokine
0
1/1/20
1/2/20
1/3/20
1/4/20
1/5/20
1/6/20
1/7/20
1/8/20
1/9/20
1/10/20
1/11/20
1/12/20
1/13/20
1/14/20
1/15/20
1/16/20
1/17/20
1/18/20
1/19/20
1/20/20
1/21/20
1/22/20
1/23/20
1/24/20
1/25/20
1/26/20
Antivirals—
Conv Immune control steroids,
Remdesivir, other,
Plasma
Mild tocilizumab, sarilumab, JAK
Severe
HDC?Hospital moves forward Covid-19
5/12/20
Identify by screening of patients, staff
Create process for eval of patients including PCR screening of
preop patients (24-48 h prior to procedure)
Isolate by protection of health care personnel and
patients
Personal Protective Equipment (PPE) (N95, nonsterile gloves, full-
face shield, goggles, gown, surgical mask), hand hygiene,
masking HCW, and patients
Engineering controls (airborne isolation rooms, physical barriers,
maintained ventilation systems, signs, environmental cleaning)
Administrative controls (Limit to no visitors, elective procedures
closed 3/18/20, now reopening in May, with ongoing surveillanceClinics move forward Covid-19
5/12/20
Identify at risk patients to call before presenting to clinic,
especially if they have respiratory symptoms, utilize
telehealth.
Mask patients and health care staff in clinic. Hand
hygiene. Environmental and administrative controls.Covid-19 Phase I reopening
April 27, 2020, all non-urgent and non-emergent healthcare
services, diagnostic radiology and lab services resume in hospital
outpatient, healthcare clinics and med offices, PT and chiropractic
areas, optometry, and dental office (with enhanced aerosol
protection).
Non-urgent invasive procedures and surgeries excluded
No waiting room, utilize non-traditional alternatives (call ahead,
waiting in car…)
Maintain social distance, and continue screening HCW, masking,
enhanced hand hygiene, and patient masks. No visitor w/ some
exceptions, and all are screenedCovid-19 Phase II reopening
May 6 outpatient ambulatory invasive surg resumes
Preprocedural Covid-19 testing per professional
association guidance and KDPH
One hospital in Lexington, KY with a 1/300 preop
positive for Covid-19, another w/ 1/600 as of 5/11/20
Maintain 14 d supply PPE through commercial vendor
Hospitals maintain 30% bed capacity for surge including
ICU and total bedsCovid-19 Phase III reopening
May 13 assuming no surge, resume non-emergent, non-
urgent inpatient surgery at 50% volume
Preprocedural Covid-19 testing per professional
association guidance and KDPH
Maintain 14 d supply PPE
Maintain 30% bed capacity hospitalCovid-19 Phase IV reopening
May 27 resume non-emergent and non-urgent elective surgery at
at volume determined by each facility
Continue preprocedural Covid-19 testing
Maintain 14 d supply of PPE based on projected burn rate for each
facility
Maintain 30% bed capacityControversies w/ Covid-19
Risk benefit measures for control will continue to be debated and
relate to local amount of disease burden (ie masks…)
Absence of disease does not imply no disease going forward
Absence of disease does not imply time to abandon infection control
measures, but also needs an ongoing assessment of risks and benefits of
those measures.
Infection control measures remain important going forward
The level of those measures taken will be affected by susceptibility of
population, availability of an effective vaccine, and therapeutics, as
well as health care capacity
Learning curve going forwardCovid-19 and the new normal
5/12/20
Vaccine and therapeutics and innovative work continue
Public health measures continue
Masking and hand hygiene in school settings, office
and work settings depending on disease incidence
and prevalence
Testing, and transmission disruption
Surveillance
Community cooperation, public, private partnership
Cent for Am Progress, Emmanuel Z, 4/3/20; Am Ent Instit, Gottlieb S, 4/10/20; Rockefeller
Foundation White Paper, 4/21/20, Allen, D, et al; Duke Margolis Center, McClellan M, 4/7/20You can also read