Cystic Fibrosis: Liver Disease - D.Westaby
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Bush A, Alton EWFW, Davies JC, Griesenbach U, Jaffe A (eds): Cystic Fibrosis in the 21st Century.
Prog Respir Res. Basel, Karger, 2006, vol 34, pp 251–261
Cystic Fibrosis: Liver Disease
D.Westaby
Chelsea and Westminster Hospital, and Imperial College Medical School, London, UK
Abstract prospective studies suggest that approximately 20–25% of
CF patients will develop liver disease but only 6–8% of
Evidence of chronic liver disease is found in 25% of these will have established cirrhosis [2, 3], the majority of
patients with cystic fibrosis (CF) and is the cause of liver which will present in the first 20 years of life. With the vast
decompensation in 2–3%. Liver injury is secondary to bile improvements in the care of pulmonary complications of
duct plugging and secondary bile-acid-related toxicity; almost CF as well as the availability of lung transplantation, it
all cases present in the first two decades of life. The marked might have been anticipated that the prevalence of liver dis-
variation in the presence and severity of disease may be due ease in a more elderly adult population would increase, but
to modifier genes. Most cases are detected on routine screen- this does not appear to be the case.
ing and only a small proportion present with variceal bleeding,
ascites or persistent jaundice. Abnormalities of liver function
tests have a low sensitivity and specificity and the presence of Pathogenesis
established cirrhosis will be diagnosed on imaging. There is
some evidence that the biliary liver disease of CF responds to The pathogenesis of chronic liver disease in CF is illus-
ursodeoxycholic acid, although the degree of benefit remains trated in figure 1. The characteristic hepatic lesion in CF is
uncertain. Liver transplantation has been successfully under- focal biliary cirrhosis consistent with that seen in partial bil-
taken in the presence of isolated liver decompensation with iary obstruction (fig. 2). The plugging of intra-hepatic bile
maintained pulmonary function. Specific complications of cir- ducts is similar to that seen in the pancreatic ducts of CF
rhosis including variceal haemorrhage, ascites and encephalop- patients [4]. CF transmembrane conductance regulator
athy are managed by standard techniques applicable to all (CFTR) has been localized to the apical membrane of the
types of cirrhosis. There is accumulating evidence that estab- cells lining the intra-hepatic bile ducts [5]. The abnormali-
lished compensated cirrhosis does not adversely affect the ties of chloride transport inhibit the hydration of the
outcome from lung transplantation. canalicular-produced bile, resulting in increased viscosity.
In addition, intra-hepatic biliary epithelial cells produce
excessive mucus composed of proteoglycans, which
Liver involvement is well recognized in cystic fibrosis increases the viscosity of CF bile [6]. The initial focal distri-
(CF) and may also be an occasional dominant manifesta- bution of cirrhotic changes in CF can be explained by early
tion. Estimates of the prevalence of liver disease depend patchy plugging of the intra-hepatic ducts; with increasing
upon the tools and definitions used, the earliest from post- ductular involvement, the process becomes more diffuse,
mortems suggesting that in excess of 70% of adults in the producing a fully established biliary cirrhosis with pan liver
third decade had some evidence of focal biliary cirrhosis involvement. Whether biliary duct obstruction is alone
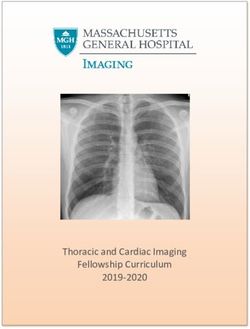
(the pathognomic lesion of CF liver disease) [1]. Recent sufficient to account for this process remains controversial.Pathogenesis of chronic liver
disease in cystic fibrosis
Biliary epithelial cell
Cystic fibrosis transmembrane
conductance regulator (CFTR)
Genetic determined dysfunction
Abnormal ductular secretion
Inspissated bile
Bile duct obstruction
• Hydrophobic bile acid retention
• Modifying genes
• Immune mechanisms
Focal biliary cirrhosis
Fig. 1. Pathogenesis of chronic liver disease in cystic fibrosis. Fig. 2. Post mortem liver showing the typical multifocal nodularity
of cystic fibrosis related cirrhosis.
A study of CF liver disease based on both light and electron
microscopy demonstrated features more in keeping with a [11]. It has been proposed that other factors such as environ-
destructive bile duct lesion than obstruction alone [7]; the mental, nutritional or non-CFTR genetic influences may be
authors suggested a bile-related toxin as the most likely important. Mutations in the alpha-1-antitrypsin, mannose-
explanation for these findings. Changes in the composition binding lectin (MBL) [12] and glutathione-S-transferase
of the bile acid pool have also been suggested as possible [13] genes may act as independent risk factors for CF liver
causes [8]. Although studies have shown no significant dif- disease (chapter 10). It has also been suggested that obstruc-
ference in the serum bile acid profile between those with tion of the common bile duct as it passes through the dis-
and without evidence of liver disease, the crude measures eased pancreas may contribute to liver disease as biliary
used may not accurately reflect the exposure of the hepato- cirrhosis is a recognized complication of long-term bile duct
cyte to potentially hepatotoxic bile acids. Bile salt output obstruction in chronic pancreatitis of other causes [14]
remains normal or modestly reduced in CF, although the although some studies have not confirmed this [15]. The
total volume of bile is significantly decreased [8, 9]. Thus a presence of a sub-population of lymphocytes, cytotoxic to
high concentration of bile acid is generated within the intra- hepatocytes and directed towards the liver-specific lipopro-
hepatic bile ducts. If there is partial or complete ductal tein, suggests that immune mechanisms might also be
obstruction, bile acid reflux could occur, exposing the hepa- involved in the pathogenesis of CF liver disease [16].
tocyte to a high concentration of potentially toxic lipophilic
bile acids, either primary (chenodeoxycholic acid) or sec-
ondary (deoxycholic and lithocholic acids). Clinical Features
Although these hypotheses provide a possible aetiologi-
cal basis for chronic CF liver disease, they fail to account for Deep cholestasis secondary to common bile duct
the absence of liver involvement in the majority of patients obstruction with inspissated bile may be the earliest mani-
or the wide spectrum of severity in those in whom this does festation of CF [17, 18]. Fatty infiltration of the liver may
occur. Speculation that with time the vast majority of sometimes produce massive hepatomegaly and abdominal
patients with CF will develop liver disease has not been sub- distension, complicated by hypoglycaemia [19, 20].
stantiated [10] and attempts to correlate the CFTR genotype Evidence of underlying cirrhosis may occur at any time, but
with development of liver disease have been unsuccessful new diagnoses are most frequently made during the first
252 Westabytwo decades of life. Historically, many cases of established Table 1. The ultrasound scoring system
chronic liver disease were detected as part of routine follow-
up in patients with an established diagnosis of CF [21], Score 1 2 3
hepato-splenomegaly being the commonest presentation. Hepatic parenchyma Normal Coarse Irregular
Abnormal liver function tests are common in CF; they may Liver edge Smooth – Nodular
be of no significance, but might also be the only indicator Periportal fibrosis None Moderate Severe
of underlying chronic liver disease. Many large centres
have established routine surveillance including sequential
ultrasound scanning (see below), which has identified a
small proportion of patients with no other clinical or labo- transferase levels. Markers of a biliary component such as
ratory evidence of liver disease. Variceal bleeding may be alkaline phosphatase and ␥-glutamine transpeptidase may
the presenting feature of established portal hypertension be more helpful, particularly when they are elevated by a
and may occur in the absence of any other signs of decom- factor of 3–4, sustained over a period of months [26].
pensation. As in other types of biliary cirrhosis, portal However, it must be remembered that a small proportion of
hypertension may occur in a pre-cirrhotic phase because of patients with established cirrhosis will have entirely normal
the pre-sinusoidal component to portal vascular resistance. liver function tests [10, 26]. The most important role for
Signs of decompensated biliary cirrhosis (jaundice, ascites standard liver function tests is to initiate a search for possi-
or encephalopathy) are very unusual presenting features. In ble underlying liver disease, specifically, liver imaging.
general, the clinical picture is one of very slowly progres-
sive liver disease (as seen in other biliary cirrhotic disease Ultrasound Scanning
such as primary biliary cirrhosis or primary sclerosing The availability of high quality transabdominal ultra-
cholangitis [22, 23]). The natural history is, in fact, usually sound scanning has provided a means of detecting liver dis-
interrupted by mortality related to pulmonary disease. ease cheaply and readily. In experienced hands ultrasound
Controversy remains as to whether the adverse effect of can both diagnose diffuse cirrhosis and detect focal disease
liver disease in CF is restricted to the 2–3% of patients with [27]. Splenomegaly, a dilated portal vein and collateral ves-
overt liver decompensation and the 1–2% with variceal sels are all important markers of portal hypertension [27].
bleeding, or it confers an adverse prognosis per se. One The use of doppler studies allows the detection of portal or
large study showed a decline in the prevalence of liver dis- splenic vein thrombosis, the incidence of which is
ease in the third decade, raising the possibility of premature increased in CF, most commonly as a consequence of asso-
mortality in those with the complication [10]. A large time- ciated chronic pancreatitis. An ultrasound scoring system
dependent, multivariate analysis reported liver disease as has been developed for the detection of chronic CF liver
an independent risk factor for mortality in addition to pul- disease in adults (table 1) [28] based on irregularity of the
monary function and nutrition [24], although the mecha- parenchyma and liver edge and periportal fibrosis (fig. 3).
nism has not been fully explained. The systemic and
pulmonary haemodynamic abnormalities seen in all types Magnetic Resonance Imaging
of cirrhosis are also present in patients with CF liver dis- A recent study has investigated the use of magnetic res-
ease [25]; the low peripheral vascular resistance, high car- onance imaging (MRI) and magnetic resonance cholan-
diac out-put and increased pulmonary shunting might giopancreatography (MRCP) in the documentation of CF
adversely affect patients with advanced pulmonary disease, liver disease [29]. These techniques have produced excel-
although prospective studies will be required to determine lent definition of the cirrhotic liver and the collateral circu-
whether this is the case. lation associated with portal hypertension (fig. 4). The
MRCP technique has allowed visualization of the biliary
tree required in the detection and management of common
Investigations bile duct stones. With improving resolution, MRCP may
also define the intra-hepatic biliary tree and the abnormali-
Liver Function Tests ties of calibre characteristic of CF-related liver disease [30].
Standard liver function tests have reasonable sensitivity
but poor specificity, which is not surprising as they may be Radionuclide Imaging
influenced by many factors such as infection, hypoxemia Derivatives of iminodiacetic acid (IDA) labelled with
and medications. This is particularly the case with amino technetium-99m provide an alternative means of assessing
Cystic Fibrosis: Liver Disease 253Fig. 3. Hepatic ultrasound showing marked nodularity of the liver
surface characteristic of established cirrhosis.
Fig. 5. A cholangiogram obtained at ERCP showing the calibre
irregularities of the intrahepatic biliary tree (arrowed).
similar to the picture in primary sclerosing cholangitis
Fig. 4. A TW2 abdominal MRI scan with fast spin echo.The nodular
surface of the cirrhotic liver is arrowed. Enlarged spleen (SPL) and
(fig. 5) [15]. These changes were first detected by trans gall
large portal venous collateral vessels (col). bladder or endoscopic contrast cholangiography [15, 32]
and are highly specific for established chronic liver disease,
not being described in patients without this on the basis of
the biliary tree [31]. IDA, when injected systemically, is ultrasound evidence [15]. Endoscopic retrograde cholan-
taken up by hepatocytes and then cleared rapidly into bile. giography (ERCP) is an invasive procedure which is no
In established cirrhosis there are documented delays in longer considered an appropriate investigative technique
hepatocyte uptake and excretion, at the levels of both the for evaluating CF-related liver disease. With the increasing
intra- and extra-hepatic biliary trees, which may be one of resolution of MRI/MRCP there is every expectation that
the earliest abnormalities seen in those susceptible to the these intra-hepatic ductular changes will be adequately
development of the biliary cirrhosis [32]. The advent of delineated by this non-invasive technique. Endoscopy has a
quantitative IDA imaging raises the possibility of monitor- role in the management of common bile duct stones and a
ing objectively the degree of hepatocyte and biliary impair- small proportion of patients in whom there is evidence of
ment and response to therapy [33]. common bile duct obstruction at the level of the head of the
pancreas. Histological assessment forms a fundamental
Invasive Techniques basis for most aspects of hepatology. However, in CF liver
The characteristic intra-hepatic bile ductular change disease the initial focal nature of the changes may result in
associated with established CF cirrhosis is irregularity of considerable sampling error. Ultrasound-guided biopsy
calibre caused by areas of stricture and dilatation and is may reduce this risk if focal nodularity can be detected.
254 WestabyThere has been understandable reluctance to carry out liver disease, need for liver transplantation or associated mortal-
biopsy in patients with CF on the basis that management ity. A small study has evaluated the effect of UDCA on liver
was seldom changed and it carries the risk of pneumotho- histology [47]. Using a scoring system based on bile duct
rax. The imaging techniques described above, carried out in proliferation, fibrosis, inspissation of bile and inflamma-
experienced hands may well provide sufficient diagnostic tory changes, a significant histological benefit was con-
information for the vast majority of patients. Liver biopsy firmed after 1 or 2 years. There are clearly insufficient data
can then be reserved for a very small proportion of patients upon which to base clear management guidelines [48]. It is
in whom other possible causes of liver damage need to be highly unlikely that this drug is capable of reversing
excluded. advanced liver disease and as such there is considerable
justification for focussing further studies on the introduc-
tion of this drug in patients with early imaging evidence of
Management liver disease [26]. More objective therapy may evolve as
risk factors predicting the development liver disease are
Bile Acid Therapy identified. In the meantime it is likely that treatment with
Ursodeoxycholic acid (UDCA) is a hydrophilic bile UDCA will continue as the drug is well tolerated with very
acid, comprising 3% of the total bile acid pool in humans, few adverse effects.
which has been used extensively in cholestatic disorders
[34], although the mechanism of action is unclear and is
probably multi-factorial. Evidence points towards protec- Liver Transplantation
tion of cholangiocytes against the cytotoxic influence of
hydrophobic bile acid [35]. In patients with primary biliary Liver transplantation has been an important strategy for
cirrhosis and primary sclerosing cholangitis there has also advanced chronic liver disease with survival rates in excess
been evidence of reduced inflammatory reaction around the of 80% at 1 year and as high as 60% at 10 years. The crite-
intra-hepatic bile ducts with UDCA therapy [36, 37]. ria for inclusion of patients for liver transplantation have
UDCA has been shown to have a stimulatory effect upon gradually expanded with increased experience. As for other
biliary secretion by increasing the number and activity of types of cirrhosis, features of advanced liver decompensa-
carrier proteins in the apical cell membrane [38] and it may tion are standard including encephalopathy, poorly con-
protect the hepatocyte against hydrophobic bile-acid- trolled ascites and progressive jaundice. The use of liver
induced apoptosis [39]. A possible immuno-regulatory transplantation in CF was initially discounted based on
effect has been proposed related to the reversal of aberrant fears that the required immunosuppression would increase
expression of HLA class-1 molecules on hepatocytes [40]. the risk of overwhelming pulmonary sepsis. However, ben-
A number of studies have evaluated UDCA in patients with eficial results in several small series of patients undergoing
CF liver disease. Initial uncontrolled data suggested both liver transplantation have encouraged wider application
bio-chemical and clinical improvement [41, 42] and the [49, 50] and in fact, many patients demonstrated significant
optimum dose appeared to be between 15 and 20 mg/kg improvements in pulmonary function after this procedure,
[43, 44]. Attention has been paid to the need for taurine possibly related to resolution of splenomegaly or ascites,
supplementation as part of UDCA therapy. Taurine defi- which impair diaphragmatic function, reduction of intra-
ciency is frequently observed in patients with CF secondary pulmonary shunting or the immunosuppressive agents
to malabsorption and faecal loss of taurine-conjugated bile used. However, a number of pulmonary contra-indications
salts and increases the proportion of glycol-conjugated bile to liver transplantation remain, including severely compro-
acids, which are potentially hepatotoxic. However, a single mised lung function or frequent exacerbations of pul-
study showed no additional affect upon liver function, but monary infection. Infection with organisms such as
there was a degree of nutritional benefit [42]. A small Burkholderia cepacia or other multi-resistant bacteria may
unblinded controlled trial was the first to report both bene- be considered relative contra-indications. A persistently
fits in liver biochemistry and improvement in biliary excre- raised arterial CO2 indicating underlying ventilatory failure
tion of IDA derivatives with UDCA [45]. A further would also represent an absolute contra-indication to single
placebo-controlled trial has also confirmed improvement in organ liver transplantation. In appropriately selected CF
biochemistry and a general illness score [46]. However, patients, survival following isolated liver transplantation in
neither of these trials has been of sufficient power or dura- the short and medium term (up to 5 years) appears to be sim-
tion to allow assessment of the risk of decompensated liver ilar to that in other types of cirrhosis [51]. The importance
Cystic Fibrosis: Liver Disease 255micronutrients, fat-soluble vitamins and clotting factors
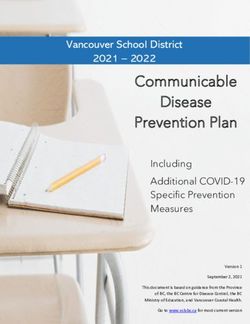
100 Patients with variceal bleeding n⫽ 18
Cohort without liver disease n⫽36
[56], which may be further compounded by the contraindi-
cation to gastrostomy in patients with established portal
80
hypertension and ascites.
Survival probability (%)
60 Jaundice
Jaundice is occasionally seen as a consequence of bile
40 duct obstruction in infancy and resolves when the plugging
of the common bile duct is relieved. As a complication of
20 cirrhosis it is unusual [15], is considered a poor prognostic
feature and requires investigation to exclude other possible
0 treatable causes, such as sepsis, drug toxicity or haemolysis.
0 50 100 150 200 250 Trans-abdominal ultrasound scanning is essential to exclude
Time (months) bile duct obstruction, from either stones or a distal common
bile duct stricture (see above). For those patients in whom
Fig. 6. A Kaplan-Meier survival analysis for patients from the time jaundice represents the advanced stage of chronic liver dis-
of first variceal bleed compared to a cohort without liver disease. ease UDCA has been shown to improve liver function and
may lead to at least transient resolution of the jaundice.
of portal hypertension and variceal bleeding as indicators Variceal Bleeding
for liver transplantation is controversial. There are a num- This represents the commonest serious complication of
ber of groups who use the presence of portal hypertension chronic liver disease, but occurs infrequently, with a preva-
and the history of variceal bleeding as specific risk factors lence of under 2%. There is a well-recognized relationship
incorporated in scoring systems to identify those suitable between the severity of the underlying liver disease and the
for isolated liver transplantation [52]. However, in our large risk of first haemorrhage. Variceal bleeding should be man-
personal experience, we observed long-term survival fol- aged using the same principles as in any other cirrhotic
lowing variceal bleeding to be comparable to that of the group of patients [57]. Initial resuscitation is critical.
general CF population [author’s unpubl. data]. This likely Replacement of blood loss is essential to maintain systemic
reflects the success of new endoscopic techniques for man- haemodynamics and protect against renal impairment.
aging variceal bleeding (fig. 6) and the absence of other There is a high risk of sepsis during an episode of variceal
serious complications such as persistent ascites and bleeding and prophylactic antibiotics covering a broad
encephalopathy. There remains a small but important group cross-section of gastro-intestinal-related bacteria are bene-
of patients with advanced liver disease and pulmonary dis- ficial [58]. Injection sclerotherapy via fibre optic
ease of such severity that liver transplantation alone would endoscopy was established as the first therapeutic tech-
not be feasible, in whom there are a number of reports of nique to improve survival but has now been replaced by
heart, lung, liver or lung/liver transplantation [51, 53, 54], banding ligation (fig. 7) [59]. Success in controlling bleed-
one demonstrating 1-year survival of up to 70% [53], ing has been reported in 85–90% and in experienced hands
although medium- and long-term data are not available. the complication rate associated with banding ligation has
With a shortage of donor organs there has been some reluc- been small [59]. Proton pump inhibitors [60] and sucralfate
tance to use those available in such a high-risk undertaking. [61] are beneficial in the management of the mucosal
ulceration associated with endoscopic therapy and also
reduce the risk of early re-bleeding. There is a significant
Management of Complications risk of early rebleeding (approximately 30%) and repeated
banding ligation may be required. Both vasopressin and
Most CF patients with cirrhosis never develop specific somatostatin analogues modulate portal blood flow and
complications and with the exception of UDCA, no spe- pressure by reducing splanchic inflow and, in the case of
cific therapy needs to be considered. However, some care somatostatin, by a direct effect on the portal circulation
should be taken with respect to nutritional requirements as itself. The vasopressin analogue tri-glycyl-lysine vaso-
patients with established cirrhosis have an increased resting pressin (glypressin) was the first pharmacological agent to
energy expenditure [55] and may have deficiencies of be reported to produce a survival benefit in active variceal
256 Westabystudies suggest that glypressin is the most effective agent
[63]. The major role for pharmacological agents is to buy
time for endoscopic therapy. There is also some evidence
that continuing these agents for 4–5 days after endoscopic
therapy reduces the risk of early rebleeding [64]. In the
presence of life-threatening bleeding, balloon tamponade
[65] has been shown to be effective. It is at best a very
uncomfortable and unpleasant experience for the patient
and in the presence of significant pulmonary disease is
associated with a high risk of complications, particularly
aspiration. The most commonly used rescue procedure for
persistent bleeding is the creation of a portal systemic
shunt. Initial surgical shunts were highly effective at the
expense of a marked reduction in liver blood flow and high
morbidity and mortality from liver failure [66]. Over the
last decade it has been possible to create a portal systemic
a shunt by a radiological technique termed a ‘trans-jugular
intra-hepatic portal systemic shunt (TIPPS)’. Because this
is a much less invasive procedure, operative morbidity and
mortality are small and the benefits with respect to arrest-
ing bleeding and preventing re-bleeding were maintained
[67]. However, hopes that this intra-hepatic shunt might
maintain a higher level of blood flow to the liver as com-
pared to shunt surgery have not been realized. Post-proce-
dural liver decompensation, specifically encephalopathy, is
well recognized and represents the major drawback. There
is however a small but important rescue role for this
approach in patients in whom there has been a failure to
control bleeding following the endoscopic technique and
this has been successfully applied in CF patients [68]. Non-
selective -adrenoreceptor blockade has been shown to be
effective for preventing recurrent variceal bleeding as well
as reducing the risk of the first variceal haemorrhage in
those patients who are known to have high risk oesophageal
varices [69]. Drugs such as propranolol and nadolol have
been widely used in this setting. However, in the presence
of pulmonary complications of CF there are concerns
that these drugs might precipitate bronchoconstriction.
Endoscopic techniques have also been evaluated to prevent
the first variceal bleed in high risk patients and in the case
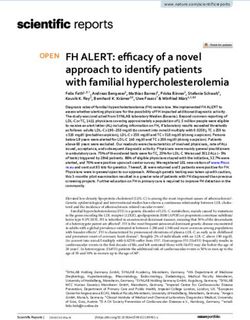
Fig. 7. (a) A diagrammatic representation of banding ligation for
oesophageal varices. (b) endoscopic view of strangulated oeso-
of banding ligation there is some accumulating evidence of
phageal varices after banding ligation. benefit [70].
Ascites
The accumulation of a transudate within the peritoneal
bleeding [62]. This drug is easy to administer as an intra- cavity is a well-recognized complication of cirrhosis and
venous bolus and appears to have few cardiovascular side portal hypertension and is a poor prognostic factor. In CF
effects (the major drawback of vasopressin). Somatostatin liver disease it is a feature of advanced disease and decom-
and its analogue, octreotide, have benefit in active bleeding pensation (which may not be the case for variceal bleed-
with few associated side effects although comparative ing). For those cases in whom clinically significant and
Cystic Fibrosis: Liver Disease 257persisting ascites develops, the management is that applied
in any case of underlying cirrhosis [71].
Encephalopathy
Hepatic encephalopathy is an extremely infrequent com-
plication in patients with CF. It has only been described in
patients with very advanced liver disease, often complica-
ting some other adverse event such as ventilatory failure,
sepsis, gastro-intestinal haemorrhage or persistent consti-
pation. Where there is a clearly defined precipitating factor
there may be expectation that the disturbed cerebration may
revert promptly when the acute situation is resolved. More
prolonged encephalopathy in the absence of a specific pre-
cipitant is an extremely poor prognostic factor. As with
other complications of cirrhosis management is not differ-
ent to that used more widely in the hepatological field [72].
Splenomegaly and Hypersplenism
Gross splenomegaly may occur in patients with CF
related-cirrhosis. This may be the cause of abdominal pain,
which on occasions may be severe (usually as a conse-
quence of a splenic infarct). In most circumstances there is
no indication for specific treatment, and simple non-opiate
analgesia (avoiding non-steroidal inflammatory drugs) is
sufficient. Pain alone is a very unusual indication for
splenectomy. In the small proportion of patients with very
Fig. 8. A cholangiogram obtained at ERCP showing multiple stones
large spleens there may be impairment of diaphragmatic in the biliary tree as well as in the gallbladder.
function. Low platelet counts due to hypersplenism are fre-
quently encountered, and in the rare instance in which
spontaneous bleeding occurs is an indication for splenec-
tomy [73] or partial splenectomy [74]. Alternative Extra-Hepatic Biliary Disease in Cystic Fibrosis
approaches have been to embolize the splenic artery to
reduce splenic size. TIPPS has also been used as a means of Abnormalities of the extra-hepatic biliary system, the
reducing portal hypertension in this setting. pathogenesis of which is similar to that of intra-hepatic bil-
iary disease, are commonly observed in CF. Approximately
25% of patients have non-functioning gallbladders and at
Influence of Liver Disease upon Organ post mortem 30% have micro-gallbladders (⬍1.5 cm in
Transplantation length and ⬍0.5 cm in width) [27]. Stenosis or atresia of
the cystic duct is also a common finding. At post mortem
There is now evidence from a small series that patients 24% of adult CF patients were found to have gallstones
with well compensated cirrhosis tolerate lung transplanta- [27] (fig. 8). A reduced prevalence in younger patients sug-
tion without difficulty and have not presented problems gests increasing risk with age which is typical of the pattern
with decompensation. Furthermore there is no evidence seen in the general population. These stones are almost
that variceal bleeding has been precipitated [75]. In our always radiolucent and the majority are of cholesterol ori-
own series, 5 patients with established cirrhosis and portal gin [76]. Analysis of stones removed from patients with CF
hypertension have undergone heart/lung or lung transplan- has shown a composition including calcium bilirubinate as
tation without specific liver related complications. For well as proteinaceous material. The most likely stimulus for
those patients in whom there is evidence of liver disease but stone formation is the low volume, high viscosity bile that
not fully established cirrhosis there should be no con- follows on from the failure to hydrate the canalicular-pro-
traindication to lung transplantation. duced bile. Complications of gallstones are commonly seen
258 Westabyin CF including biliary colic, cholecystitis and extra- selected cases in which gallbladder function is still main-
hepatic bile duct obstruction. The management of gall- tained this may represent an alternative approach.
stones in CF is similar to that in the general population
[77]. Laparoscopic cholecystectomy is generally well toler-
ated in CF even in the presence of quite severe pulmonary Hepatobiliary Malignancy
disease. The endoscopic approach offers a minimally inva-
sive means of managing common bile duct stones and in It is now well recognized that patients with CF have an
our own experience this has been extremely well tolerated increased risk of gut-related malignancy [78]. We have
with a very low risk of complications. The use of UDCA to observed a single case of a gallbladder cancer in a patient
dissolve gallbladder stones has not been specifically presenting at the age of 40 with biliary colic. There has
reported in CF and it is likely that in the presence of a dis- recently been another single case report of a hepatocellular
eased gallbladder this would not be successful. However, in carcinoma in a patient with CF-related cirrhosis [79].
References
1 Vawter GF, Shwachman H: Cystic fibrosis in young adults with cystic fibrosis with and study on incidence, risk factors, and outcome.
adults: An autopsy study. Pathol Annu 1979; without chronic liver disease. Hepatology Hepatology 2002;36:1374–1382.
14(pt 2):357–382. 1992;15:660–664. 22 Pares A, Rodes J: Natural history of primary
2 Corbett K, Kelleher S, Rowland M, Daly L, 12 Salvatore F, Scudiero O, Castalso G: Geno- biliary cirrhosis. Clin Liver Dis 2003;7:
Drumm B, Canny G, Greally P, Hayes R, type-phenotype correlation in cystic fibrosis: 779–794.
Rourke B: Cystic fibrosis-associated liver dis- The role of modifier genes. Am J Med Genet 23 Farrant JM, Hayllar KM, Wilkinson ML,
ease: A population-based study. J Pediatr 2002;111:88–95. Karani J, Portman BC, Westaby D, Williams R:
2004;145:327–332. 13 Henrion-Caude A, Flamant C, Roussey M, Natural history and prognostic variables in pri-
3 Lamireau T, Monnereau S, Martin S, Marcotte Housset C, Flahault A, Fryer AA, Chadelat K, mary sclerosing cholangitis. Gastroenterology
JE, Winnock M, Alvarez F: Epidemiology of Strange RC, Clement A: Liver disease in 1991;100:1710–1717.
liver disease in cystic fibrosis: A longitudinal paediatric patients with cystic fibrosis is asso- 24 Hayllar KM, Williams SG, Wise AE, Pouria S,
study. J Hepatol 2004;41:920–925. ciated with glutathione S-transferase P1 poly- Lombard M, Hodson ME, Westaby D: A prog-
4 Marino CR, Gorelick FS: Scientific advances morphism. Hepatology 2002;36:913–917. nostic model for the prediction of survival in
in cystic fibrosis. Gastroenterology 1992;103: 14 Gaskin KJ, Waters DL, Howman-Giles R, de cystic fibrosis. Thorax 1997;52:313–317.
681–693. Silva M, Earl JW, Martin HC, Kan AE, Brown 25 Williams SG, Samways J, Innes JA, Guz A,
5 Cohn JA, Strong TV, Picciotto MR, Nairn AC, JM, Dorney SF: Liver disease and common- Geddes DM, Hodson ME, Westaby D:
Collins FS, Fitz JG: Localization of the cystic bile-duct stenosis in cystic fibrosis. N Engl J Systemic haemodynamic changes in patients
fibrosis transmembrane conductance regulator Med 1988;318:340–346. with cystic fibrosis with and without chronic
in human bile duct epithelial cells. Gastro- 15 Nagel RA, Westaby D, Javaid A, Kavani J, liver disease. J Hepatol 1996;25:900–908.
enterology 1993;105:1857–1864. Meire HB, Lombard MG, Wise A, Williams R, 26 Lenaerts C, Lapierre C, Patriquin H, Bureau
6 Bhaskar KR, Turner BS, Grubman SA, Hodson ME: Liver disease and bile duct N, Lepage G, Harel F, Marcotte J, Roy CC:
Jeffereson DM, LaMont JT: Dysregulation of abnormalities in adults with cystic fibrosis. Surveillance for cystic fibrosis-associated
proteoglycans production by intrahepatic bil- Lancet 1989;ii:1422–1425. hepatobiliary disease: Early ultrasound
iary epithelial cells bearing defective (delta- 16 Mieli-Vergani G, Psacharopoulos HT, changes and predisposing factors. J Pediatr
F508) cystic fibrosis transmembrane Nicholson AM, Eddleston AL, Mowat AP, 2003;143:343–350.
conductance regulator. Hepatology 1998;27: Williams R: Immune responses to liver mem- 27 McHugo JM, McKeown C, Brown MT, Weller
7–14. brane antigens in patients with cystic fibrosis P, Shah KJ: Ultrasound findings in children
7 Lindblad A, Hultcrantz R, Strandvik B: Bile- and liver disease. Arch Dis Child 1980;55: with cystic fibrosis. Br J Radiol 1987;60:
duct destruction and collagen deposition: 696–701. 137–141.
A prominent ultrastructural feature of the 17 Vlaman HB, France NE, Wallis PG: Pro- 28 Williams SG, Evanson JE, Barrett N, Hodson
liver in cystic fibrosis. Hepatology 1992;16: longed neonatal jaundice in cystic fibrosis. ME, Boulthee JE, Westaby D: An ultrasound
372–381. Arch Dis Child 1971;46:805–809. scoring system for the diagnosis of liver disease
8 Robb TA, Davidson GP, Kirubakaran C: 18 Furuya KN, Roberts EA, Canny GJ, Phillips in cystic fibrosis. J Hepatol 1995;22:513–521.
Conjugated bile acids in serum and secretions MJ: Neonatal hepatitis syndrome with paucity 29 King LJ, Scurr ED, Murugan N, Williams SG,
in response to cholecystokinin/secretin stimu- of interlobular bile ducts in cystic fibrosis. Westaby D, Healy JC: Hepatobiliary and pan-
lation in children with cystic fibrosis. Gut J Pediatr Gastroenterol Nutr 1991;12:127–130. creatic manifestations of cystic fibrosis: MR
1985;26:1246–1256. 19 Roy CC, Weber AM, Morin CL, Lepage G, imaging appearances. Radiographics 2000;20:
9 Weizman Z, Durie PR, Kopelman HR, Vessely Brisson G, Yousef I, Lasalle R: Hepatobiliary 767–777.
SM, Forstner GG: Bile acid secretion in cystic disease in cystic fibrosis: A survey of current 30 Durieau I, Pellet O, Simonot L, Durupt S,
fibrosis: Evidence for a defect unrelated to fat issues and concepts. J Pediatr Gastroenterol Bellon G, Durand DV, Minh VA: Sclerosing
malabsorption. Gut 1986;27:1043–1048. Nutr 1982;1:469–478. cholangitis in adults with cystic fibrosis: A mag-
10 Scott-Jupp R, Lama M, Tanner MS: Prevalence 20 Treem WR, Stanley CA: Massive hepato- netic resonance cholangiographic prospective
of liver disease in cystic fibrosis. Arch Dis megaly, steatosis, and secondary plasma car- study. J Hepatol 1999;30:1052–1056.
Child 1991;66:698–701. nitine deficiency in an infant with cystic 31 Krishnamurthy S, Krishnamurthy GT:
11 Duthie A, Doherty DG, Williams C, Scott- fibrosis. Pediatrics 1989;83:993–997. Technetium-99m-iminodiacetic acid organic
Jupp R, Warner JO, Tanner MS, Williamson R, 21 Colombo C, Battezzati PM, Crosignani A, anions: Review of biokinetics and clinical
Mowat AP: Genotype analysis for delta F508, Morbito A, Costantini D, Padoan R, Glunta A: application in hepatology. Hepatology 1989;9:
G551D and R553X mutations in children and Liver disease in cystic fibrosis: A prospective 139–153.
Cystic Fibrosis: Liver Disease 25932 O’Brien S, Keogan M, Casey M, Duffy G, high-dose ursodeoxycholic acid in cystic 58 Garcia-Tsao G: Bacterial infections in cirrho- McErlean D, Fitzgerald MX, Hegarty JE: fibrosis-related cholestatic liver disease: sis. Can J Gastroenterol 2004;18:405–406. Biliary complications of cystic fibrosis. Gut Results of a randomized study with 10-year 59 Vlavianos P, Westaby D: Management of acute 1992;33:387–391. follow-up. Scand J Gastroenterol 1997;32: variceal haemorrhage. Eur J Gastroenterol 33 Colombo C, Castellani MR, Balistreri WF, 369–373. Hepatol 2001;13:335–342. Seregni E, Assaisso ML, Giunta A: Scinti- 45 O’Brien S, Fitzgerald MX, Hegarty JE: A con- 60 Gimson A, Polson R, Westaby D, Williams R: graphic documentation of an improvement in trolled trial of ursodeoxycholic acid treatment Omeprazole in the management of intractable hepatobiliary excretory function after treat- in cystic fibrosis related liver disease. Eur J esophageal ulceration following injection ment with ursodeoxycholic acid in patients Gastroenterol 1992;4:857–863. sclerotherapy. Gastroenterology 1990;99: with cystic fibrosis and associated liver dis- 46 Colombo C, Battezzati PM, Podda M, 1829–1831. ease. Hepatology 1992;15:677–684. Bettinardi N, Giunta A: Ursodeoxycholic acid 61 Polson RJ, Westaby D, Gimson AE, hayes PC, 34 Paumgartner G, Beuers U: Ursodeoxycholic for liver disease associated with cystic fibro- Stellon AJ, Hayllar K, Williams R: Sucralfate acid in cholestatic liver disease: Mechanisms sis: A double-blind multicenter trial. The for the prevention of early rebleeding follow- of action and therapeutic use revisited. Italian group for the Study of Ursodeoxy- ing injection sclerotherapy for oesophageal Hepatology 2002;36:525–531. cholic Acid in cystic fibrosis. Hepatology varices. Hepatology 1989;10:79–82. 35 Van Nieuwkerk CM, Elferink RP, Groen AK, 1996;23:1484–1490. 62 Ioannou G, Doust J, Rockey DC: Terlipressin Ottenhoff R, Tytgat GN, Dingemans KP, Van 47 Lindblad A, Glaumann H, Strandvik B: A two for acute oesophageal variceal haemorrhage. Den Bergh Weerman MA, Offerhaus GJ: year prospective study of the effect of Cochrane Database Syst Rev 2003;(1): Effects of urodeoxycholate and cholate feed- ursodeoxycholic acid on urinary bile acid CD002147. ing on liver disease in FVB with a distrupted excretion and liver morphology in cystic 63 Nevens F: Review article: A critical compari- mdr2 P-glycoprotein gene. Gastroenterology fibrosis-associated liver disease. Hepatology son of drug therapies in currently used thera- 1996;111:165–171. 1998;27:166–174. peutic strategies for variceal haemorrhage. 36 Poupon RE, Balkau B, Eschwege E, Poupon 48 Cheng K, Ashby D, Smyth R: Ursodeoxy- Aliment Pharmacol Ther 2004;20(suppl 3): R: A multicenter, controlled trial of ursodiol cholic acid for cystic fibrosis related liver dis- 18–22. for the treatment of primary bi-cirrhosis. ease. Cichrane Database Syst Rev 2000;(2): 64 de Franchis R: Somatostatin, somatostatin UDCA-PBC study group. N Engl J Med 1991; CD00222. analogues and other vasoactive drugs in the 324:1548–1554. 49 Noble-Jamieson G, Barnes N, Jamieson N, treatment of bleeding oesophageal varices. 37 Beuers U, Spengler U, Kruis W, Aydemir U, Friend P, Calne R: Liver transplantation for Dig Liver Dis 2004;36(suppl 1):S93–S100. Wiebecke B, Heldwein W, Weinzierl M, Pape hepatic cirrhosis in cystic fibrosis. J R Soc 65 Vlavianos P, Gimson AE, Westaby D, Williams GR, Sauerbruch T, Paumgartner G: Urso- Med 1996;89(suppl 27):31–37. R: Balloon tamponade in variceal bleeding: deoxycholic acid for treatment of primary 50 Mack DR, Traystman MD, Colombo JL, Use and misuse. BMJ 1989;298:1158. sclerosing cholangitis: A controlled trial. Sammut PH, Kaufman SS, Vanderhoof JA, 66 Stern RC, Stevens DP, Boat TF, Doershuk CF, Hepatology 1992;16:707–714. Antonson DL, Markin RS, Shaw BW Jr, Izant RJ Jr, Matthews LW: Symptomatic hepatic 38 Fickert P, Zollner G, Fuchsbichler A, Langnas AN: Clinical denouement and muta- disease in cystic fibrosis: Incidence, course, Stumptner C, Pojer C, Zenz R, Lammert F, tion analysis of patients with cystic fibrosis and outcome of portal systemic hunting. Stieger B, Meier PJ, Zatloukal K, Denk H, undergoing liver transplantation for biliary Gastroenterology 1976;70:645–649. Trauner M: Effects of ursodeoxycholic and cirrhosis. J Pediatr 1995;127:881–887. 67 Luketic VA, Sanyal AJ: Esophageal varices. II cholic acid feeding on hepatocellular tran- 51 Milkiewicz P, Skiba G, Kelly D, Weller P, TIPS (transjugular intrahepatic portosystemic expression in mouse liver. Gastroenterology Bonser R, Gur U, Mirza D, Buckels J, shunt) and surgical therapy. Gastroenterol Clin 2001;121:170–183. Stableforth D, Elias E: Transplantation for North Am 2000;29:387–421. 39 Qiao L, Yacoub A, Studer E, Gupta S, Pei XY, cystic fibrosis outcome following early liver 68 Pozler O, Krajina A, Vanicek H, Hulek P, Grant S, Hylemon PB, Dent P: Inhibition of transplantation. J Gastroenterol Hepatol 2002; Zizka J, Michl A, Elias P: Transjugular intra- the MAPK and P13K pathways enhances 17:208–213. hepatic portosystemic shunt in five children UDCA-induced apoptosis in primary rodent 52 Noble-Jamieson G, Barnes ND: Liver trans- with cystic fibrosis: Long term results. hepatocytes. Hepatology 2002;35:779–789. plantation for cirrhosis in cystic fibrosis. Hepatogastroenterology 2003;50:1111–1114. 40 Calmus Y, Gane P, Rouger P, Poupon R: J Pediatr 1996;129:314. 69 Abraczinskas DR, Ookubo R, Grace ND, Hepatic expression of class I and class II 53 Couetil JP, Soubrane O, Houssin DP, Dousset Groszmann RJ, Bosch J, Garcia-Tsao G, major histocompatibility complex molecules BE, Chevalier PG, Guinvarch A, Loulmet D, Richardson CR, Matloff DS, Rodes J, Conn in primary biliary cirrhosis: Effect of urso- Achkar A, Carpentier AF: Combined heart- HO: Propranolol for the prevention of first deoxycholic acid. Hepatology 1990;11: lung-liver, double lung-liver, and isolated liver esophageal variceal haemorrhage: A lifetime 12–15. transplantation for cystic fibrosis in children. commitment? Hepatology 2001;34:1096–1102. 41 Colombo C, Setchell KD, Podda M, Transpl Int 1997;10:33–39. 70 Schepke M, Kleber G, Nurnberg D, Willert J, Crosignani A, Roda A, Curcio L, Ronchi M, 54 Dennis CM, McNeil KD, Dunning J, Stewart Koch L, Veltzke-Schlieker W, Hellerbrand C, Giunta A: Effects of ursodeoxycholic acid S, Friend PJ, Alexander G, Higenbottam TW, Kuth J, Schanz S, Kahl S, Fleig WE, therapy for liver disease associated with cystic Calne RY, Wallwork J: Heart-lung-liver trans- Sauerbruch T: German study group for the fibrosis. J Pediatr 1990;117:482–489. plantation. J Heart Lung Transplant 1996;15: primary prophylaxis of variceal bleeding. 42 Cotting J, lentze MJ, Reichen J: Effects of 536–538. Ligation versus Propranolol for the primary ursodeoxycholic acid treatment on nutrition 55 Madden AM, Morgan MY: Patterns of energy prophylaxis of variceal bleeding cirrhosis. and liver function in patients with cystic fibro- intake in patients with cirrhosis and healthy Hepatology 2004;40:65–72. sis and longstanding cholestasis. Gut 1990;31: volunteers. Br J Nutr 1999;82:41–48. 71 Garcia-Tsao G: Portal hypertension. Curr 918–921. 56 Sokol RJ, Durie PR: Recommendations for Opin Gastroenterol 2003;19:250–258. 43 Colombo C, Crosignani A, Assaisso M, management of liver and biliary tract disease 72 Shawcross D, Jalan R: Dispelling myths in the Battezzati PM, Podda M, Giunta A, Zimmer- in cystic fibrosis. Cystic Fibrosis Foundation treatment of hepatic encephalopathy. Lancet Nechemias L, Setchell KD: Ursodeoxycholic Hepatobiliary Disease Consensus Group. 2005;365:431–433. acid therapy in cystic fibrosis-associated liver J Pediatr Gastroenterol Nutr 1999;28(suppl 1): 73 Westwood AT, Millar AJ, Ireland JD, Swart A: disease: A dose-response study. Hepatology S1–S13. Splenectomy in cystic fibrosis patients. Arch 1992;16:924–930. 57 Jalan R, Hayes PC: UK guidelines on the man- Dis Child 2004;89:1078. 44 Van de Meeberg PC, Houwen RH, agement of variceal haemorrhage in cirrhotic 74 Zach MS, Thalhammer GH, Eber E: Partial Sinaasappel M, Heijerman HG, Bijleveld CM, patients. British Society of gastroenterology. splenectomy in CF patients with hyper- Vanberge-Henegouwen GP: Low-dose venous GUT 2000;46 S3–4:III1-III15. splenism. Arch Dis Child 2003;88:649. 260 Westaby
75 Gilljam M, Chaparro C, Tullis E, Chan C, and management. Curr Surg 2004;61: D. Westaby
Keshavjee S, Hutcheon M: GI complications 290–293. Chelsea and Westminster Hospital
after lung transplantation in patients with 78 Maisonneuve P, FitzSimmons SC, Neglia JP, 369 Fulham Road
cystic fibrosis. Chest 2003;123:37–41. Campbell PW 3rd, Lowenfels AB: Cancer risk London SW10 9NH (UK)
76 Angelico M, Gandin C, Canuzzi P, Bertasi S, of nontransplanted and transplanted cystic Tel. ⫹44 208 846 1076
Cantafora A, De Santis A, Quattrucci S, fibrosis patients: Year study. J Natl Cancer Inst Fax ⫹44 208 237 5007
Antonelli M: Gallstones in cystic fibrosis: A 2003;95:381–387. E-Mail westaby.david@chelwest.nhs.uk
critical reappraisal. Hepatology 1991;14: 79 McKeon D, Day A, Parmar J, Alexander G,
768–775. Bilton D: Hepatocellular carcinoma in associ-
77 Lahmann BE, Adrales G, Schwartz RW: ation with cirrhosis in a patient with fibrosis.
Choledocholithiasis-principles of diagnosis J Cyst Fibros 2004;3:193–195.
Cystic Fibrosis: Liver Disease 261You can also read