Daylight saving time and myocardial infarction: should we be worried? A review of the evidence - European Review for ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Review for Medical and Pharmacological Sciences 2018; 22: 750-755
Daylight saving time and myocardial infarction:
should we be worried? A review of the evidence
R. MANFREDINI1,4, F. FABBIAN1,4, A. DE GIORGI1,4, B. ZUCCHI2,4,
R. CAPPADONA2,4, F. SIGNANI3,4, N. KATSIKI5, D.P. MIKHAILIDIS6
1
Department of Medical Sciences, University of Ferrara, Ferrara, Italy
2
Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara,
Italy
3
Department of Public Health, Azienda Sanitaria Locale of Ferrara, Ferrara, Italy
4
Center for Studies on Gender Medicine, University of Ferrara, Ferrara, Italy
5
Second Department of Propaedeutic Internal Medicine, Medical School, Aristotle University of
Thessaloniki, Thessaloniki, Greece
6
Department of Clinical Biochemistry, University College of London Medical School, London, UK
Abstract. – Transitions into and out of Day- Introduction
light Saving Time (DST) may disrupt circadi-
an rhythms and lead to sleep disturbance and The purpose of Daylight Saving Time (DST),
deprivation. A first report observed an associa-
which is applied in many countries (including the
tion between DST and acute myocardial infarc-
tion (AMI), especially after the spring shift and United States and some countries in Europe), is to
in women. We tried to identify and evaluate the prolong the sunlight proportion of the day. Since
possible association between DST and AMI, us- sunlight influences the sleep/wake physiological
ing the MEDLINE, EMBASE and Google Schol- rhythms and most of the circadian processes,
ar electronic database (years 2009-2016), with DST may induce a disruption; also, adaptation to
regards to the searching terms ‘daylight sav- DST requires a certain amount of time1. Similar
ing time’, ‘daylight saving time’ plus ‘gender’, to jet lag, a temporary misalignment between the
and ‘daylight saving time’ plus ‘acute myocar-
dial infarction’. In total, 72, 10, and 6 studies
endogenous circadian clock and the destination
were found, respectively. Overall, 6 studies, in- time, where eastward flights (phase advance) take
cluding a total of 87,994 cases, resulted to sat- longer to re-entrain the circadian clock compared
isfy the searching request, and were included with westward flights (phase delay)1, spring DST
in the present analysis. All studies confirmed shift (phase advance) may also disrupt circadian
a higher occurrence of AMI in the spring shift, rhythms more than autumn DST (phase delay).
ranging from 4 to 29%, whereas only 1 study Transitions into and out of DST may lead to
showed a higher occurrence of AMI in the au- sleep disturbance and sleep deprivation, fatigue,
tumn shift. By the way, in 5 studies providing
separate analysis, the results by sex were not headache, loss of attention and alertness, as well
univocal. In fact, as for the spring shift, 2 stud- as reduced motivation. However, despite these
ies did not show differences between men and negative effects, a series of studies showed that
women, 2 reported a higher frequency in men, DST transition does not have significant negative
and 1 in women. Regarding the autumn shift, impact on workplace injuries, occupational acci-
only 1 study reported a higher occurrence of dents2,3, and traffic road accidents4.
AMI in women. These results support the pres- Some years ago, Janszky and Ljung5 first re-
ence of an association between DST and a
modest increase of AMI occurrence, especially
ported an association between acute myocardial
for the spring shift, and with no definite gender infarction (AMI) and DST, characterized by a
specific differences. higher incidence of AMI (incidence ratio [IR]
for the first week 1.051, 95% confidence interval
Key Words: [CI], 1.032-1.071) and 0.985, 95% CI, 0.969-1.002,
Daylight saving time, Acute myocardial infarction, after the spring and autumn shift, respectively).
Circadian rhythms, Gender, Chronotype, Sleep depri-
vation.
The effect of DST on the incidence of AMI al-
so showed gender differences, being more pro-
750 Corresponding Author: Roberto Manfredini, MD; e-mail: roberto.manfredini@unife.itDaylight saving time and myocardial infarction
nounced in women in the spring shift, and more coronary intervention were recorded on Monday
pronounced in men in the autumn shift5. The aim after the spring shift of DST. In addition, there
of the present review was to discuss the associa- was a decrease in the incidence of AMI on the
tion between DST and AMI occurrence based on Tuesday after the autumn DST shift. This study
the up-to-date available literature. did not provide data on the numerical distribu-
tion or analysis of men/women9. Kirchberger et
Acute Myocardial Infarction and al10, after adjustment for potential confounders,
Daylight Saving Time Shifts reported an increased AMI risk after the spring
We aimed to evaluate the possible associa- shift, in particular for the first 3 days, especially
tion between DST and AMI, using the MED- for men, but not for women. Finally, Sipila et al11
LINE, EMBASE and Google Scholar electronic found an increased incidence of AMI on Wednes-
database (years 2009-2016), with regards to the day (spring shift) and Thursday (autumn shift),
searching terms ‘daylight saving time’, ‘daylight but the overall incidence in AMI during the entire
saving time’ plus ‘gender’, and ‘daylight saving week after each DST transition was not different
time’ plus ‘acute myocardial infarction’. Respec- from control weeks. Furthermore, no gender dif-
tively, 72, 10, and 6, were found. The 6 papers ferences were found by subgroups analysis. Only
dealing with DST and AMI (Table I)6-11 were Culic7 reported a significant increase of AMI
manually checked for the presence of separate during both spring and autumn post-transitional
reports and/or analyses of subgroups by gender. weeks, with more pronounced effects in subjects
Of these studies, 4 were conducted in Europe admitted during first workdays of those weeks
(Sweden6, Croatia7, Germany10, and Finland11), and and, in contrast to the other findings, with a high-
2 in the United States 8,9. er risk in autumn than in spring ([IR]: 1.44 vs.
There was a total of 87,994 AMI cases, and in 1.29, and 95% CI, 1.09-1.49 and 1.19-1.69, respec-
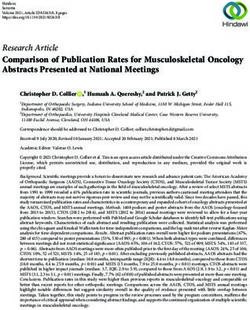
5 of 6 studies women and men were included. All tively). Patients with AMI during the spring shift
the 6 studies confirmed a higher (4-29%) occur- were more likely to be men, and those with AMI
rence of AMI in the spring shift, whereas only 1 during the autumn shift were more likely to be
study showed a higher occurrence of AMI in the women. At multivariate analysis, male gender in-
autumn shift7 (Figure 1). As for the 5 studies with dependently contributed to the prediction of AMI
analysis by gender, in the spring shift 2 studies during the first 4 workdays after the spring shift,
did not find differences between men and wom- and female gender during the same period of the
en8,11, 2 reported a higher frequency in men7,10, and autumnal shift7. Three studies provided separate
1 in women7. Regarding the autumn shift, only analysis of possible risk factors regarding spring
1 study reported a higher occurrence of AMI in and autumn shift6,7,10, and results of significant
women7. associations found are reported in Table II.
Although these studies differ each other, they
substantially support an association between DST Sleep, Personal Circadian Preference,
and the risk of AMI, reporting a higher risk after and Gender
spring DST transition. Jansky et al5 provided The spring shift of DST, due to a circadian
substantial confirmation of their previous find- phase-advance, is associated with modest sleep
ings, even with a limited increase in risk (0.3% to deprivation and is a plausible cause for any in-
7.5%)6. A small risk (overall [IR]: 1.044, 95% CI, creased risk of AMI. Previous studies involving
1.006-1.083, expected = 2687.5, observed = 2806) accelerometer-based measurements showed that
was confirmed, especially for women compared transition to DST may compromise the process
with men ([IR]: 1.07 vs. 1.02)6. A modest increase of sleep by both depriving sleep and reducing
in the risk of AMI ([IR]: 1.12, 95% CI, 1.00-1.36), sleep efficiency of the deprived sleep12. Individ-
but only in the week after the spring shift, was ual circadian physical functions identify persons
also confirmed by Jiddou et al8. Such increase in with early (morning) and late (evening) chrono-
risk was characterized especially by non-ST ele- types. Nearly 4 decades ago Horne and Ostberg13
vation infarction, whereas no differences in risk presented a self-assessment Morningness-Eve-
and type of infarction were reported after the au- ningness questionnaire (MEQ), consisting of 19
tumnal shift. This study did not provide data on items with a definite score each, identifying 5
sub-analysis by gender, possibly due to its small categories: definitely evening type (59-69), mod-
size8. Sandhu et al9 reported that significantly erately evening type (31-41), neither type (42-58),
increased rates of AMI requiring percutaneous moderately morning type (59-69), and definitely
751752
Table I. Review of the available studies on the association between Daylight Saving Time and acute myocardial infarction.
DST (overall) DST (subgroups by gender)
Country, Cases (n°)
Authors Years M/W (n°) Spring Autumn Spring Autumn
Janszky et al6
Sweden 3236 First week: First week: First week: First week:
1995-2007 2035/1201 1.04 [1.00-1.08] 0.99 [0.97-1.03] M: 1.02 [0.98-1.07] M: 1.00 [0.96-1.04]
W: 1.07 [1.01-1.13] W: 0.99 [0.94-1.04]
Culic7 Croatia 2412 1.29 [1.09-1.49] 1.44 [1.19-1.69] Multivariate: male sex Multivariate: female sex
1990-1996 1666/746 Highest: Tuesday Highest: Monday 2.84 [1.09-7.35] p = 0.03 2.08 [1.02-4.24] p = 0.04
Jiddou et al 8
USA 328 1.12 [1.00-1.36] NSTEMI: 0.99 [0.85-1.16] STEMI/
2006-2012 206/122 increase p = 0.022 NSTEMI: p = 0.56) No differences by gender No differences by gender
Highest: Sunday Highest: Saturday
1.71 [1.09-2.02] p < 0.05.
Sandhu et al9 USA 42060 Monday Tuesday No analysis by gender No analysis by gender
2010-2013 not given 1.24 [1.05-1.46] p = 0.011 0.79 [0.62-0.99] p = 0.044
Kirchberger et al10
Germany 25499 First 3 days 1.10 [0.97-1.25] First 3 days 0.98 [0.86-1.12] M: first 3 days 1.16 [1.00-1.34] M: first 3 days 1.01 [0.85-1.18]
1985-2010 18524/6975 Monday 1.21 [0.92-1.50] Friday 1.24 [1.04-1.46] 1 week 1.11 [0.99-1.23] 1 week 1.04 [0.92-1.17]
1 week 1.08 [0.92-1.50] 1 week 1.03 [0.93-1.13] W: first 3 days 0.96 [0.74-1.24] W: first 3 days 0.91 [0.71-1.18]
1 week1.00 [0.83-1.21] 1 week 0.99 [0.81-1.20]
Sipila et al11 Finland 14459 Highest: Wednesday Highest: Thursday No differences by gender No differences by gender
2001-2009 9301/5158 1.16 [1.01-1.34] 0.85 [0.74-0.97]
Abbreviations: M = men; W = women; DST = Daylight Saving Time; STEMI = ST elevation myocardial infarction; NSTEMI = non-ST elevation myocardial infarction.
R. Manfredini, F. Fabbian, A. De Giorgi, B. Zucchi, R. Cappadona, et al.Daylight saving time and myocardial infarction
immediate nor without consequence14. In fact, in-
creased sleep fragmentation and sleep latency
present a cumulative effect of sleep loss, at least
across the following week, and perhaps longer14.
Moreover, individuals with evening chronotype
show either sleep-related issues, e.g., later bed-
time and wake-up, decreased sleep quality and
quantity, as well as more pronounced metabolic
risk , e.g., reduced physical activity, unhealthy di-
etary patterns and other habits15. Finally, it is like-
ly that even modest sleep deprivation and circa-
dian misalignment may influence cardiovascular
health, since even partial night sleep deprivation
has been associated with increases in sympathetic
Figure 1. Graphic representation of the weighted mean tone and catecholamine levels16. However, none
ratio between number of events during spring shift (white) of the 6 available studies provided data on sleep
and autumn (black) shift. The diameter of every circle is (duration, quality), circadian habits, or person-
proportional to the number of subjects analyzed in each
study.
al chronotype. Three studies provided separate
analysis of possible associations with AMI, DST
and baseline characteristics, possible triggers,
risk factors, and medications used6,7,10. It does not
morning type (70-86) 13. It has been reported1 that seem that these factors play an important role,
individuals with late chronotype may have more since significant associations were found in single
problems in adjusting to the spring shift of DST. studies only for some of these, e.g., employment,
Even if the start of the spring shift of DST is physical activity, previous AMI, total cholesterol,
thought to lead to the relatively inconsequential and some cardiovascular medications. By the
loss of 1 h of sleep on the night of the transition, way, careful attention has to be given to female
there is evidence that adjustment to DST is neither gender, since it seems to be exposed to some
Table II. Associations with baseline characteristics, possible triggers, risk factors, and medications used (significant results
only) in the different studies.
Janszky et al6 Spring
Expected vs. observed Cholesterol: ≥ 5.2 vs. < 5.2 mmol/L**
Incidence Ratios (IR) 0.960 (0.880-1.044)
1.099 (1.022-1.180)
Autumn
Cholesterol: ≥ 5.2 vs. < 5.2 mmol/L** Calcium channel blockers: Y vs. N** Statins: Y vs. N**
0.919 (0.855-0.988) 0.901 (0.834-0.973) 0.917 (0.854-0.984)
1.045 (0.981-1.112) 1.018 (0.984-1.053) 1.019 (0.984-1.055)
Culic7 Spring
Odds Ratios (OR) Calcium channel blockers ** Physical activity**
0.16 (1.09-7.35) 0.18 (0.04-0.77)
Autumn
Beta-blockers** Physical activity** Employment**
0.10 (0.01-0.75) p = 0.03** 0.24 (0.07-0.80) 2.76 (1.34-5.68)
Kirchberger et al10 Spring
Risk Ratios (RR) ACE-inhibitors (3 days): Y vs. N* ACE-inhibitors (1 week): Y vs. N*
1.489 (1.151-1.927) 1.297 (1.063-1.582)
1.036 (0.865-1.241) 1.059 (0.928-1.208)
Autumn
Recurrent AMI (3 days)* Recurrent AMI (1 week)*
1.318 (1.029-1.691) 1.270 (1.048-1.539)
Abbreviations: ACE = angiotensin converting enzyme; AMI = acute myocardial infarction; N = no; Y = yes. Levels of
significance: *p < 0.5; **p ≤ 0.05.
753R. Manfredini, F. Fabbian, A. De Giorgi, B. Zucchi, R. Cappadona, et al.
sex-dependent aspects of cardiovascular risk fac- References
tors17-18 and to a higher frequency of hospital mul-
tiple readmissions.19 Finally, 3 out of the 5 studies 1) K anterman T, Juda M, Merrow M, Roennenberg T.
with indication of the day of highest frequency of The human circadian clock’s seasonal adjust-
ment is disrupted by daylight saving time. Curr Bi-
AMI onset, reported a higher incidence on Mon- ol 2007; 17: 1996-2000.
day or the first days of the week7,9,10. It is known 2) Morassei S, Smith PM. Switching to daylight saving
that Monday has been identified as a critical day time and work injuries in Ontario, Canada: 1993-
for onset of acute coronary events, either AMI 2007. Occup Environ Med 2010; 67: 878-880.
and Takotsubo cardiomyopathy20-24, probably be- 3) L ahti T, Sysi -A ho J, Haukka J, Partonen T. Work-re-
cause of a series of unfavorable factors, such as lated accidents and daylight saving time in Fin-
stress of commencing weekly activities, higher land. Occup Med 2011; 61: 26-28.
blood pressure, and unfavorable metabolic pan- 4) L ahti T, Nysten E, Haukka J, Partonen T. Daylight
el25-27. A circadian misalignment, even if slight, saving time transitions and road traffic accidents.
J Environ Public Health 2010; 2010: 657167.
could favor circadian disruption and cardiovas-
cular consequences28, and add another extra-risk 5) Janszky I, L jung R. Shift to and from daylight sav-
ing time and incidence of myocardial infarction. N
piece to the puzzle of Monday chronorisk. Engl J Med 2008; 359: 1966-1968.
6) Janszky I, Ahnye S, L jung R, Mukamal KJ, Gautam S,
Wallentin L, Stenestrand U. Daylight saving time
Conclusions shifts and incidence of acute myocardial infarction
– Swedish Register of Information and Knowledge
The available studies seem to support the About Swedish Heart Intensive Care Admissions
presence of an association between DST and a (RIKS-HIA). Sleep Med 2012; 13: 237-242.
modest increase of AMI occurrence only for the 7) Culic V. Daylight saving time transitions and acute
myocardial infarction. Chronobiol Int 2013; 30:
spring shift. Furthermore, in contrast to earlier 662-668.
findings5, a higher risk of AMI in women is not
8) Jiddou MR, Pica M, Boura J, Franklyn BA. Incidence
confirmed. It is interesting that 5 out of 6 studies of myocardial infarction with shifts to and from
(83%) collected and analyzed data for both wom- daylight savings time. Am J Cardiol 2013; 111:
en and men, and this certain represents a point of 631-635.
strength when trying to draw conclusions, since it 9) Sandhu A, Seth M, Gurm HS. Daylight savings time
has been recently shown that only less than 44% and myocardial infarction. Open Heart 2014; 1:
of chronobiological studies can exhibit separate e000019.
analysis by gender29. On one hand, since a pos- 10) K irchberger I, Wolf K, Heier M, Kuch B, Von Scheidt
sible disruption of biological rhythms and sleep W, Peters A, Meisinger C. Are daylight saving time
transitions associated with changes in myocardi-
deprivation may represent potential risk factors al infarction incidence? Results from the German
for AMI, an easy and inexpensive assessment MONICA/KORA Myocardial Infarction Registry.
of individual circadian preference (morning or BMC Public Health 2015; 15: 778.
evening chronotype) as well as detailed infor- 11) Sipila JO, R autava P, Kyto V. Association of daylight
mation on sleep duration and quality should be saving time transitions with incidence and in-hos-
encouraged, also at a population level. If indeed pital mortality of myocardial infarction in Finland.
Ann Med 2016; 48: 10-16.
a DST effect on AMI is confirmed, then certain
actions can be implemented. This may include 12) L ahti TA, L eppamaki S, Lonnqvist J, Partonen T. Tran-
sition to daylight saving time reduces sleep dura-
its abolition, information to the public regarding tion plus sleep efficiency of the deprived sleep.
sleep pattern, and provision for increased hospital Neurosci Lett 2006; 406: 174-177.
admission for AMI in the subsequent days. 13) Horne JA, Ostberg O. A self-assessment question-
naire to determine morningness-eveningness in
human circadian rhythms. Int J Chronobiol 1976;
4: 97-110.
Funding Support 14) Harrison Y. The impact of daylight saving time on
This work has been supported, in part, by a research grant sleep and related behaviours. Sleep Med Rev
from the University of Ferrara, Fondo di Ricerca di Ateneo 2013; 17: 285-292.
– FAR – (year 2016, prof. Roberto Manfredini).
15) Fabbian F, Zucchi B, De Giorgi A, Tiseo R, Boari B,
Salmi R, C appadona R, Gianesini G, Bassi E, Signani F,
R aparelli V, Basili S, M anfredini R. Chronotype, gen-
Conflict of Interest der and general health. Chronobiol Int 2016; 33:
The Authors declare that they have no conflict of interests. 863-882.
754Daylight saving time and myocardial infarction
16) Nagai M, Hoshide S, K ario K. Sleep duration as a weekly patterns of hospital admissions for non-
risk factor for cardiovascular disease – a review fatal and fatal myocardial infarction. Am J Emerg
of the recent literature. Curr Cardiol Rev 2010; 6: Med 2009; 27: 1097-1103.
54-61. 24) Manfredini R, Citro R, Previtali M, Vriz O, Ciampi Q,
17) Chen DW, Jin Y, Zhao RM, Long LJ, Han CL, Rio - Pascotto M, Tagliamonte E, Provenza G, Manfredini
vanen A, K nuuti J, Jalkanen S, Wang JC. Age-, and F, Bossone E; Takotsubo Italian Network Investigators.
sex- and glucose-dependent correlation of plas- Monday preference in onset of Takotsubo cardio-
ma soluble vascular adhesion protein-1 concen- myopathy. Am J Emerg Med 2010; 28: 715-719.
tration with cardiovascular risk factors and sub- 25) K imura G, Inoue N, Mizumo H, Izumi M, Nagatoya K,
clinical atherosclerosis. Eur Rev Med Pharmacol Ohtahara A, Munakata M, and Workplace Hyperten -
Sci 2016; 20: 1544-1548. sio Co -Operative Study by 29 Rosai Hospitals belong -
18) K atsiki N, Mikhailidis DP. Emerging vascular risk ing to the Japan Organization of Occupational Health
factors in women: any differences from men? Curr and S afety. Increased double product morning
Med Chem 2015; 22: 3565-3579. during work. Hypertens Res 2017; 40: 671-674.
19) De Giorgi A, Boari B, Tiseo R, Lopez-Soto PJ, Signani 26) Murakami S, Otsuko K, Kubo Y, Shinagawa M, Ya-
F, Gallerani M, M anfredini R, Fabbian F. Hospital manaka T, Ohkawa S, K itaura Y. Repeated ambula-
redmissions to internal medicine departments: a tory monitoring reveals a Monday morning surge
higher risk for females? Eur Rev Med Pharmacol in blood pressure in a community-dwelling pop-
Sci 2016; 20: 4557-4564. ulation. Am J Hypertens 2004; 17(12 Pt 1): 1179-
20) Willich SN, Lowel H, L ewis M, Hormann A, A rntz 1183.
HR, K eil U. Weekly variation of acute myocardial 27) Urdal P, A nderssen SA, Holme I, Hjermann I, Mundal
infarction: increased Monday risk in the working HH, Haaland A, Torjesen P. Monday and non-Mon-
population. Circulation 1994; 90: 87-93. day concentrations of lifestyle-related blood com-
21) Gnecchi -Ruscone T, Piccaluga E, Guzzetti S, Contini ponents in the Oslo diet and exercise study. J In-
M, Montano N, Nicolis E. Mornings and Monday: tern Med 1998; 244: 507-513.
critical periods for the onset of acute myocardial 28) Young ME, Bray MS. Potential role for peripheral
infarction. Eur Heart J 1994; 15: 882-887. circadian clock dyssinchrony in the pathogenesis
22) Spielberg C, Falkenham D, Willich SH, Wegscheider of cardiovascular dysfunction. Sleep Med 2007;
K, Voller H. Circadian, day of week and season- 8: 656-667.
al variability in myocardial infarction: comparison 29) M anfredini R, Salmi R, C appadona R, Signani F, Basili
between working and retired patients. Am Heart S, K atsiki N. Sex and circadian periodicity of car-
J 1996; 132: 579-584. diovascular diseases. Are women sufficiently rep-
23) M anfredini R, M anfredini F, Boari B, Bergami E, M ari resented in chronobiological studies? Heart Fail
E, G amberini S, Salmi R, G allerani M. Seasonal and Clin 2017; 13: 719-738.
755You can also read