Dynamics of Genome Alterations in Crohn's Disease-Associated Colorectal Carcinogenesis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Biology of Human Tumors Clinical
Cancer
Research
Dynamics of Genome Alterations in Crohn's
Disease–Associated Colorectal Carcinogenesis
Daniela Hirsch1,2, Darawalee Wangsa2, Yuelin J. Zhu3, Yue Hu2, Daniel C. Edelman3,
Paul S. Meltzer3, Kerstin Heselmeyer-Haddad2, Claudia Ott4, Peter Kienle5,
Christian Galata5, Karoline Horisberger5, Thomas Ried2, and Timo Gaiser1
Abstract
Purpose: Patients with inflammatory bowel diseases, that exception: the gain of 5p was significantly more prevalent in
is, ulcerative colitis and Crohn's disease (CD), face an CD-CRCs. CD-CRCs had a distinct mutation signature: TP53
increased risk of developing colorectal cancer (CRC). (76% in CD-CRCs vs. 33% in sporadic mucinous CRCs),
Evidence, mainly from ulcerative colitis, suggests that TP53 KRAS (24% vs. 50%), APC (17% vs. 75%), and SMAD3 (3%
mutations represent an initial step in the progression from vs. 29%). TP53 mutations and SCNAs were early and fre-
inflamed colonic epithelium to CRC. However, the pathways quent events in CD progression, while APC, KRAS, and
involved in the evolution of CRC in patients with CD are SMAD2/4 mutations occurred later. In four patients with
poorly characterized. CD-CRC, at least one mutation and/or SCNAs were already
Experimental Design: Here, we analyzed 73 tissue sam- present in non-dysplastic colonic mucosa, indicating occult
ples from 28 patients with CD-CRC, including precursor tumor evolution.
lesions, by targeted next-generation sequencing of 563 can- Conclusions: Molecular profiling of CD-CRCs and precur-
cer-related genes and array-based comparative genomic sor lesions revealed an inflammation-associated landscape
hybridization. The results were compared with 24 sporadic of genome alterations: 5p gains and TP53 mutations occurred
CRCs with similar histomorphology (i.e., mucinous adeno- early in tumor development. Detection of these aberrations
carcinomas), and to The Cancer Genome Atlas data (TCGA). in precursor lesions may help predicting disease progression
Results: CD-CRCs showed somatic copy-number altera- and distinguishes CD-associated from sporadic colorectal
tions (SCNAs) similar to sporadic CRCs with one notable neoplasia. Clin Cancer Res; 1–15. 2018 AACR.
Introduction mation (2). CD-CRCs are predominantly located in the distal
colorectum (40%–50%), followed by the cecum/ascending
Crohn's disease (CD), a condition when associated with
colon (20%–30%), and can also occur in anorectal fistulae
chronic inflammation of the large intestine, considerably
(3, 4). Compared with sporadic CRCs, CD-CRCs develop at an
increases the risk for the development of colorectal cancer
earlier age, are usually diagnosed at more advanced stages and
(CRC), comparable with ulcerative colitis (UC; ref. 1). In both
are therefore associated with a poorer prognosis (5). The
CD and UC the risk for developing CRC depends on disease
histomorphology of CD-CRCs often resembles a mucinous
duration, and on the extent and severity of colorectal inflam-
and/or signet ring cell phenotype, which is associated with
poor prognosis in sporadic CRC (3, 6). Many patients with CD
1
are diagnosed with multifocal CRCs (10%) and frequently
Institute of Pathology, Medical Faculty Mannheim, University Medical Center show synchronous dysplastic lesions (30%–50%), which may
Mannheim, Heidelberg University, Mannheim, Germany. 2Cancer Genomics
Section, Genetics Branch, Center for Cancer Research, NCI, NIH, Bethesda,
be the consequence of extended chronic inflammation causing
Maryland. 3Molecular Genetics Section, Genetics Branch, Center for Cancer the so-called field cancerization (4, 7).
Research, NCI, NIH, Bethesda, Maryland. 4Department of Internal Medicine I, Inflammation-induced CRCs arise in a stepwise fashion from
University Medical Center Regensburg, Regensburg, Germany. 5Department of dysplastic precursor lesions, comparable with the development
Surgery, Medical Faculty Mannheim, University Medical Center Mannheim, of sporadic CRCs from adenomas (8). The development of
Heidelberg University, Mannheim, Germany. sporadic CRCs is caused by the sequential accumulation of
Note: Supplementary data for this article are available at Clinical Cancer cancer gene mutations and specific chromosomal copy-number
Research Online (http://clincancerres.aacrjournals.org/). changes (9, 10). For instance, inactivating mutations of the
K. Horisberger, T. Ried, and T. Gaiser contributed equally to this article. tumor suppressor gene APC and gains of chromosome 7 occur
Corresponding Author: Timo Gaiser, Institute of Pathology, Medical Faculty before the development of invasive disease, and are maintained
Mannheim, University Medical Center Mannheim, Heidelberg University, during tumorigenesis, while mutations of TP53 and copy-
Theodor-Kutzer-Ufer 1-3, Mannheim 68167, Germany. Phone: þ49-621-383- number increases of chromosome arm 20q manifest later in
2876; E-mail: timo.gaiser@umm.de; Thomas Ried, Center for Cancer Research, the progression of sporadic CRC (9, 11, 12). However, the gene-
National Cancer Institute, Building 50, Room 1408, Bethesda, MD 20892-8010. tic events that define CD-CRCs, in particular the dynamics of
Phone: 240-760-6383; Fax: 240-541-4441; E-mail: riedt@mail.nih.gov
their development from histologically undetectable precursor
doi: 10.1158/1078-0432.CCR-18-0630 lesions to invasive disease, remain largely elusive. Most studies
2018 American Association for Cancer Research. on inflammation-related colorectal carcinogenesis focused on
www.aacrjournals.org OF1
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.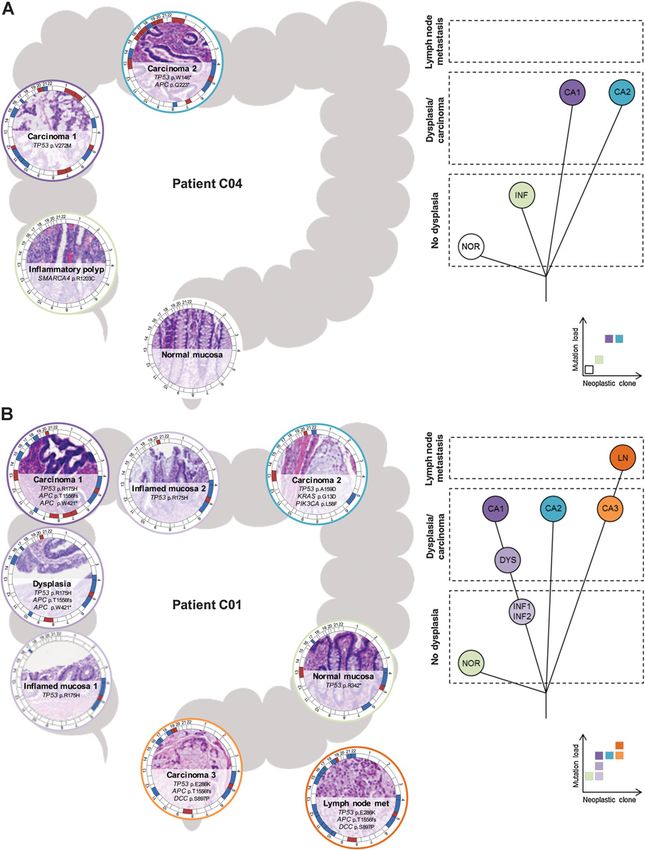
Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Hirsch et al.
top). CD–related etiology of a CRC was assumed (i) if the
Translational Relevance patient had long-standing CD with colonic involvement at the
The distinction between Crohn's disease (CD)-associated time of CRC diagnosis, (ii) if inflammation in the colon
and sporadic colorectal neoplasia is crucial for treatment involved the large bowel segment, in which the CRC was
decisions but extremely difficult based on endoscopy and located, and (iii) in resection specimens: if inflammation
histology alone. Our findings indicate a possible approach and/or chronic inflammatory changes in adjacent mucosa were
to distinguish CD–associated dysplasia from sporadic visible. In addition, 24 sporadic CRCs (histologically mucinous
adenoma based on TP53 mutations and gains of chromo- adenocarcinomas with and without signet ring cells) and cor-
some arm 5p as molecular biomarkers. In addition, the responding normal mucosa were collected, diagnosed between
detection of these aberrations in non-dysplastic precursor 2004 and 2015 (Supplementary Fig. S1, bottom). All sporadic
lesions may help predicting progression to CRC in patients mucinous CRCs were mismatch repair proficient. In addition
with CD. to the initial diagnosis, all samples were re-evaluated by two
pathologists (T. Gaiser and D. Hirsch). Tumor staging was
performed according to the current American Joint Committee
on Cancer/Union for International Cancer Control staging sys-
UC-CRCs or "colitis-associated cancer" (CAC) subsuming UC- tem. All experiments were conducted in accordance with the
CRCs and CD-CRCs without differentiating. Two recent studies Declaration of Helsinki and approved by the institutional review
using next-generation sequencing suggest differences in the boards (2016-819R-MA, OHSRP#13229/MTA#41436) that
mutational landscape not only between sporadic CRCs and waived the need for informed consent for this retrospective and
CACs, but also between CD-CRCs and UC-CRCs (13, 14). anonymized analysis of archival samples.
While TP53 mutations occurred at a slightly higher frequency
in CACs than in sporadic CRCs, APC and KRAS mutations were Histopathologic criteria
less common in CACs compared with sporadic CRCs (13–15). Histopathologic classification was performed according to the
Yaeger and colleagues reported that IDH1 mutations were World Health Organization by two pathologists (T. Gaiser and
significantly more frequent in CD-CRCs compared with both D. Hirsch; ref. 17). Mucinous colorectal adenocarcinoma diag-
UC-CRCs and sporadic CRCs (14). Neither of these studies nosis in the sporadic control group was confirmed if the tumors
investigated genome-wide copy-number changes, nor the were composed of >50% extracellular mucin. Tumors were also
sequence of mutational events during CD–related tumorigen- evaluated for the presence of signet ring cells. In CD-CRCs, we
esis. Molecular data regarding precursor lesions of CD-CRCs, reviewed for the presence or absence of extracellular mucin
including both inflamed and dysplastic epithelium, are sparse. (mucinous component) and/or signet ring cells (signet ring cell
By targeted sequencing of TP53, CDKN2A, and KRAS in indi- component). All intestinal tissue samples were screened for
vidual crypts, Galandiuk and colleagues showed frequent and inflammation, regenerative, that is, inflammatory, changes, and
occasionally very extensive field cancerization in the chroni- dysplasia according to the histopathologic criteria defined by
cally inflamed bowel of five patients with CD (16). the Inflammatory Bowel Disease-Dysplasia Morphology Study
In this study, we aimed (i) to characterize the landscape Group (18).
of somatic gene mutations and chromosomal copy-number
alterations of CD-CRCs compared with histomorphologically DNA isolation
similar sporadic mucinous CRCs, (ii) to elucidate the genetic DNA was isolated from FFPE tissue after histopathologic
pathways of tumor development in CD, and (iii) to explore the determination of tumor areas on H&E sections, avoiding
dynamics of the development of genome alterations in CD– foci of inflammation as well as foci of high mucin and low
associated colorectal neoplasia by analyzing multiple CD– cellular content, as published previously (12). DNA concentra-
related lesions at different stages of development from indi- tion was measured by fluorometric quantitation (Qubit 3.0
vidual patients. To this end, we analyzed 73 samples from 28 Fluorometer, Life Technologies, Thermo Fisher Scientific)
patients with CD-CRC, including carcinomas and lymph node using the Qubit dsDNA HS (High Sensitivity) Assay Kit (Life
metastases, dysplastic lesions, inflamed mucosa, and histolog- Technologies). DNA integrity was evaluated on the basis of
ically normal colonic mucosa, by targeted next-generation Bioanalyzer traces (2100 Bioanalyzer Instrument, Agilent
sequencing of 563 cancer-related genes and array-based com- Technologies) using the High Sensitivity DNA Kit (Agilent).
parative genomic hybridization (aCGH). As a control collec-
tive, we investigated 24 sporadic mucinous CRCs and matched Microsatellite PCR
normal colonic mucosa, and compared our results to CRC data Tumor DNA and corresponding normal DNA were subjected
from The Cancer Genome Atlas (TCGA). to microsatellite PCR using a panel of five mononucleotide
markers (BAT25, BAT26, NR-21, NR-24, and MONO-27;
cf. MSI Analysis System, Promega), and a panel of two mono-
Materials and Methods nucleotide (BAT25 and BAT26) and three dinucleotide markers
Patients and tissue samples (D5S346, D2S123, and D17S250; so-called Bethesda panel;
We collected 73 formalin-fixed, paraffin-embedded (FFPE) ref. 19). Briefly, 10-ng DNA was used to amplify the micro-
tissue samples from 28 patients with CD-CRC diagnosed satellite loci in multiplex PCR reactions. PCR products were
between 2003 and 2016 from the archives of the Institutes of separated by capillary electrophoresis using an ABI 3130
Pathology in Mannheim and Regensburg, including primary Genetic Analyzer (Applied Biosystems). A tumor was classified
CD-CRCs, lymph node metastases, dysplastic lesions, inflamed as high-level microsatellite instable (MSI-H) when two or more
mucosa, and normal colonic mucosa (Supplementary Fig. S1, markers of the Bethesda panel and/or of the Promega panel
OF2 Clin Cancer Res; 2018 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.
Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Genetics of Colorectal Cancer Development in Crohn's Disease
showed an allelic size variation (i.e., a band shift compared ESP6500 (NHLBI Exome Sequencing Project; http://evs.gs.
with corresponding normal DNA), as low-level microsatellite washington.edu/EVS/), and COSMIC database (Catalogue
instable (MSI-L) when one marker of either panel showed an of Somatic Mutations in Cancer; http://cancer.sanger.ac.uk/
allelic size variation, and as microsatellite stable (MSS) when cosmic; ref. 28). The following filtering criteria were used for
no marker showed an allelic size variation. germline variation calls: (i) passed variant caller filters; (ii) read
depth 10 reads with fraction of alternative reads of 0.25;
Array-based comparative genomic hybridization (iii) MAPQ score of >55; (iv) Exome Aggregation Consortium
aCGH was performed as previously described using ULS label- (ExAC) filter (ExAC AF) 0.001; (v) annotation impact "high"
ing (Agilent) and SurePrint G3 CGH 4 180K microarrays or "moderate"; and (vi) candidate variants were examined in
(Agilent; ref. 20). Data were visualized and analyzed using HGMD (Human Gene Mutation Database; http://www.hgmd.
Nexus Copy Number software version 8.0 (BioDiscovery, cf.ac.uk/ac/index.php; ref. 27). The following filtering criteria
Inc.). Arm-level somatic copy-number alterations (SCNAs) were were used for somatic variation calls: (i) passed variant caller
defined as single alteration or an aggregate of alterations encom- filters; (ii) fraction of alternative reads in the matched normal is
passing half or more (50%) of a chromosome arm (21). Array- 0.01; (iii) read depth in the tumor 10 reads with fraction of
based CGH data have been deposited in Gene Expression alternative reads 0.1 (0.05 for samples C01CA2, C13CA,
Omnibus (GEO) database (data accession number: GSE113015). C15CA, C16CA, C16LR, C25CA, C27CA, M10CA, and M24CA
because tumor cell content was very low due to extensive
Fluorescence in situ hybridization extracellular mucin); (iv) MAPQ score of >49 (for Strelka only);
A bacterial artificial chromosome contig centering on the (v) ExAC filter (ExAC AF) 0.001; and (vi) annotation impact
5p14.3 region (CDH12) was assembled in UCSC Genome "high" or "moderate". Visual inspection of SNVs and indels was
Browser (http://genome.ucsc.edu), and the two overlapping done using Integrative Genomics Viewer (IGV, Broad Institute,
bacterial artificial chromosome clones were labeled with Cambridge, MA; refs. 29, 30). A supplementary excel file is
DY-505-dUTP (Dyomics) using nick translation. The centro- provided containing the list of mutations used for all analyses
mere probe (CEP 10) was obtained from Abbott Molecular in this study. Those mutations comprise (i) mutations called by
(Vysis CEP10 SpectrumOrange, catalog No. 06J36–090). Pre- both MuTect and Strelka algorithm, (ii) mutations in genes
treatment, denaturation, hybridization, and detection were known to be significantly mutated in non-hypermutated CRC
done using the ZytoLight FISH-Tissue Implementation Kit according to TCGA data (15), that is, APC, TP53, KRAS,
(catalog No. Z-2028–20, ZytoVision GmbH) according to the PIK3CA, FBXW7, SMAD4, NRAS, TCF7L2, SMAD2, CTNNB1,
manufacturer's instructions with slight modifications. Slides and ACVR1B, which were called by either MuTect or Strelka and
were analyzed using an Olympus BX41 fluorescence micro- validated by an alternative method, and (iii) mutations called
scope (Olympus Deutschland GmbH) connected to an F-View by either MuTect or Strelka that were present in more than one
II CCD-Camera (Soft Imaging System GmbH). Between 40 and neoplastic lesion of an individual patient. In addition, as
100 non-overlapping nuclei were counted per sample. We used histologically normal mucosa does not necessarily represent
a ratio (number of target locus signals/number of centromere germline, we inversely analyzed normal mucosa samples for
signals) of 1.2 as threshold for copy-number gain of the mutations that were present in normal mucosa but absent in
target locus as published previously (22). the tumor. These mutations could either be germline muta-
tions, sequencing artifacts or real mutations in normal mucosa.
Targeted next-generation sequencing Germline mutations seem unlikely since one would expect
The targeted sequence capture approach, named OncoVar, germline mutations to be present in both tumor and normal
was designed to span coding exons of 563 cancer-related genes mucosa. To ensure that we do not call sequencing artifacts,
(see Supplementary Table S1 for gene list). Briefly, library mutations in normal mucosa were only reported if (i) they
construction was done with the KAPA Hyper Prep Kits for could be verified by an alternative method and (ii) were listed
Illumina (https://www.kapabiosystems.com), and the resulting in COSMIC and predicted to be pathogenic. Copy-number
paired-end libraries were sequenced on NextSeq 500 systems analysis from targeted sequencing data was done with the
(Illumina). The mean read depth for targeted regions (mean CNVkit from Eric Talevich (31). Sequencing data have been
coverage) was 185. Data processing and variant calling pro- deposited in the Sequence Read Archive (SRA) database (data
cedure mainly followed the Best Practices workflow recom- accession number: SRP140665).
mended by the Broad Institute (http://www.broadinstitute.
org/gatk/guide/best-practices). Briefly, the raw sequencing TCGA data retrieval and processing
reads were mapped to human genome build 19 by Burrows- Clinicopathologic data of TCGA colorectal adenocarcino-
Wheeler Aligner (23), followed by local realignment using the ma cohort were downloaded from the NCI's Genomic Data
GATK suit from the Broad Institute. Duplicated reads were Commons (GDC) Data Portal (https://portal.gdc.cancer.gov/)
marked by Picard tools (http://picard.sourceforge.net). Somat- and cBioPortal for Cancer Genomics (http://www.cbioportal.
ic variant calling was performed on sequencing reads of org/; refs. 15, 32, 33). Data of the 276 patients included
matched tumor–normal samples by the Strelka somatic were processed as follows: (i) samples without sequencing data
variant caller (version 1.0.15; ref. 24), and by MuTect (version were removed (n ¼ 52); (ii) samples classified as MSI-H (n ¼ 28),
2; ref. 25). Germline variant calling was done with the MSI-L (n ¼ 36) or with not evaluable microsatellite status (n ¼ 1)
UnifiedGenotyper from the Broad Institute. SnpEff (26) were removed; (iii) remaining hypermutated samples were
was used to annotate and predict the effects of variants with removed (n ¼ 5); (iv) remaining samples without copy-number
multiple annotation databases, including dbNSFP (27), dbSNP data were removed (n ¼ 7); and (v) histopathologic designation
147 (NCBI; https://www.ncbi.nlm.nih.gov/projects/SNP/), as provided by TCGA was verified for all samples by inspection of
www.aacrjournals.org Clin Cancer Res; 2018 OF3
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.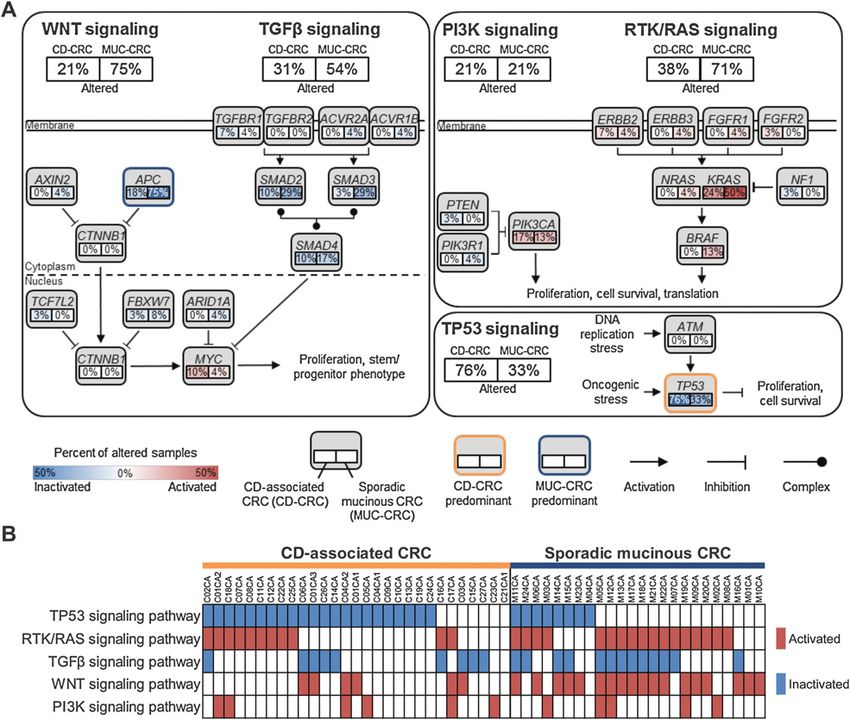
Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Hirsch et al.
the deposited pathology reports and tissue images, and samples MSH6 (ready-to-use; clone EP49, catalog No. IR086, Dako),
with unclear or inconclusive histology (intestinal type vs. mucin- PMS2 (1:50; clone EP51, catalog No. M3647, Dako) and TP53
ous) were removed (n ¼ 3). This approach resulted in a total of (1:50; clone DO-7, catalog No. M7001, Dako). Heat-induced
144 microsatellite stable, non-hypermutated CRC samples with antigen retrieval was performed in Target Retrieval Solution,
available sequencing and copy-number data, of which 15 showed pH 9.0 (Tris/EDTA, 1:10; catalog No. S2367, Dako) in a water
a mucinous histology, and 129 were of intestinal type. Those 144 bath at 95 C for 20 minutes. Detection was done using the
samples were used for comparison with our data. EnVision Detection System, Peroxidase/DAB, Rabbit/Mouse
(catalog No. K5007, Dako) according to the manufacturer's
Curated pathway analysis instructions with slight modifications. All stainings were vali-
Analogous to TCGA's study of CRC, we performed a focused dated by internal and/or external positive controls as well as
analysis of pathways known to be frequently altered in CRC, negative control specimens. IHC stainings were evaluated by
namely the WNT, TGFb, PI3K, RTK-RAS, and TP53 signaling two pathologists (D. Hirsch and T. Gaiser). Tumor samples
pathways (15). For all pathway analyses, we used the set of lacking nuclear staining for MLH1, MSH2, MSH6, and/or PMS2
microsatellite stable/non-hypermutated CD-CRC samples (n ¼ were considered microsatellite instable while tumor samples
29) and sporadic mucinous CRC samples (n ¼ 24). Samples with retained expression of MLH1, MSH2, MSH6, and PMS2 in
were stratified by etiology of CRC (inflammation associated vs. the tumor cells were considered microsatellite stable. TP53
sporadic). The approach relies on the general abstraction of staining could be classified into four staining patterns accord-
gene alterations per sample, which were assigned to manually ing to nuclear staining intensity and distribution of positive
curated pathways based on TCGA's study of CRC (15), on cells as published by Sato and colleagues (35): (i) sporadic:
studies by Robles and colleagues (13) and Yaeger and collea- only a few of weakly positive cells were sporadically dispersed
gues (14), and on KEGG PATHWAY database. Pathways were in a tubule, (ii) scattered: a small number of weakly positive
composed of the following genes: WNT (APC, ARID1A, AXIN2, cells were focused in a tubule, (iii) nested: moderate to strongly
CTNNB1, FBXW7, and TCF7L2), TGFb (ACVR1B, ACVR2A, positive cells were aggregated in restricted areas of tubule, and
SMAD2, SMAD3, SMAD4, TGFBR1, and TGFBR2), PI3K (AKT1, (iv) diffuse: strongly positive cells existed in most areas of
AKT2, AKT3, PIK3CA, PIK3R1, PTEN, TSC1, and TSC2), RTK/ tubules, and (v) negative: tubule did not contain a single TP53
RAS (BRAF, EGFR, ERBB2, ERBB3, FGFR1, FGFR2, KRAS, MET, positive nucleus. Alternatively, TP53 immunoreactivity could
NF1, and NRAS), and TP53 (ATM and TP53). A pathway be classified into three basic patterns according to nuclear
was considered altered in a given sample, if at least one gene staining intensity and distribution of positive cells as published
in the pathway was altered. A particular gene in a specific by Noffsinger and colleagues (36): (i) isolated immunoreactive
sample was considered altered if it was either altered (i) by cells in the crypt bases, (ii) strongly positive cells confined to
mutation (non-synonymous, somatic mutation in a protein- the basal half of the glands, and (iii) diffusely staining cells.
coding region) or (ii) by high-level copy-number amplification Microscopy images were acquired with a digital microscope and
(aCGH, log2 ratio >1.0). The ERBB2 and MYC amplifications scanner M8 (PreciPoint GmbH).
(ERBB2: C11CA; MYC: C04CA1, C08CA, C26CA, and M10CA)
detected by aCGH were verified by FISH using ZytoLight
Statistical analysis
SPEC ERBB2/CEN 17 Dual Color Probe (catalog No. Z-2015,
Statistical analysis was performed using GraphPad Prism
ZytoLight) and ZytoLight SPEC MYC/CEN 8 Dual Color Probe
software version 7.03 (GraphPad Software; www.graphpad.
(catalog No. Z-2092, ZytoLight). A gene was assumed to be a
com). Differences in clinicopathologic variables were estimated
likely oncogene if it was primarily altered by missense muta-
by unpaired t test (age), Fisher's exact test (sex), or x2 test (stage
tions or high-level copy-number amplification, and to be a
and location). For all statistical tests involving molecular data,
likely tumor suppressor gene if it was primarily affected by
only microsatellite stable, non-hypermutated CRCs were con-
truncating mutations.
sidered. Differences in SCNAs between CD-CRC and sporadic
Phylogenetic analysis mucinous CRC were estimated using Mann–Whitney test (num-
Phylogenetic trees representing the evolutionary relationship ber of SCNAs, fraction of genome altered by SCNAs) or Fisher's
between the tissue samples sequenced from each patient were exact test with correction for multiple comparisons via false
inferred by comparing lists of mutations in each lesion as described discovery rate (FDR; arm-level SCNA frequencies). Differences
by Izumchenko and colleagues (34). Briefly, a lesion that contained in gene mutation frequencies between CD-CRC and sporadic
all mutations present in another lesion was considered its ancestor. mucinous CRC were estimated using Fisher's exact test; no
If there was no such lesion, putative precursors were inferred from multiplicity adjustment was done here because significant dif-
the set of mutations common to multiple lesions. Lesions with no ferences in mutation rates were restricted to those genes with
genetic alterations were considered parallel branches, although an the highest mutation frequencies in sporadic mucinous CRC
alternative phylogenetic tree could have been created if these (APC, TP53, and SMAD3) rather than distributing uniformly in
lesions were considered ancestors of lesions with mutations. All the whole gene list, indicating their disease-related nature.
phylogenetic trees were drawn with a common stem (trunk), which
represents the normal, that is, diploid, genome. Results
Immunohistochemistry Clinicopathologic characteristics of CD-CRCs
Immunohistochemistry (IHC) was performed using the fol- Our cohort comprised 28 patients with CD who developed
lowing primary antibodies: MLH1 (1:25; clone ES05, catalog CRC (Table 1; Supplementary Table S2). Patients with CD were
No. M3640, Dako, Agilent Pathology Solutions, Agilent), diagnosed with CRC at a relatively young age (median 50 years)
MSH2 (ready-to-use; clone FE11, catalog No. IR085, Dako), and had a long history of CD (median 24 years). The majority of
OF4 Clin Cancer Res; 2018 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.
Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Genetics of Colorectal Cancer Development in Crohn's Disease
Table 1. Clinicopathologic characteristics of cases of Crohn's disease–associated CRC and sporadic mucinous CRC
CD–associated CRC Sporadic mucinous CRC
Variable n ¼ 28 patients n ¼ 24 patients
Age at CRC diagnosis, years
Mean SD 50 11 65 13
Median (range) 50 (28–76) 65.5 (33–87)
Duration of CD at CRC diagnosisa
Mean SD 23 9 N/A
Median (range) 24 (5–40) N/A
Sex
Male 16 16
Female 12 8
AJCC stage at diagnosis
I 5 4
II 8 4
III 7 9
IV 5 7
Data not available 3 0
Site of primary carcinomab
Right hemicolon 11 12
Left hemicolon 4 7
Rectum 17 5
Synchronous colorectal carcinoma(s)
Present 3 0
Absent 25 24
Carcinoma associated to (anorectal) fistula
Yes 9 0
No 23 24
Histology
Mucinous with signet ring cells 9 7
Mucinous without signet ring cells 11 17
Intestinal type 12 0
Microsatellite status
Microsatellite stable 30 24
Microsatellite instable 2 0
Abbreviations: CD, Crohn's disease; N/A, not applicable.
a
On the basis of n ¼ 23 patients because for n ¼ 5 patients no exact data on duration of CD were available.
b
Right hemicolon was defined as cecum, ascending, and transverse colon; left hemicolon as descending and sigmoid colon.
CD-CRCs (53%) were located in the rectum, followed by the right test; Fig. 1C). Array-CGH derived patterns of SCNAs in CD-
hemicolon (34%; Supplementary Fig. S2A). Mucinous and/or CRC were similar to sporadic mucinous CRC and to previously
signet ring cell histology was observed in two-thirds of the published data on sporadic CRC, including gains of chromo-
CD-CRCs (Fig. 1A; Supplementary Figs. S2B–S2D and S3). Two somes and chromosome arms 7, 8q, 13q, and 20q, and losses of
CD-CRCs were high-level microsatellite instable (MSI-H), and 5q, 8p, 17p, and 18q (10, 37). However, we observed a
one CD-CRC was microsatellite stable but showed a POLE muta- significant difference: gain of chromosome arm 5p occurred
tion resulting in hypermutation (Supplementary Figs. S4 and S5). in 20 of 29 CD-CRCs (69%) compared with five of 24 (21%)
The reference group of sporadic mucinous CRCs differed signifi- sporadic mucinous CRCs (FDR adjusted P ¼ 0.03; Fisher's exact
cantly from CD-CRCs in terms of age at CRC diagnosis (P ¼ 0.0001, test; Fig. 1D). In addition, a loss of 5p was never observed in
unpaired t test) and CRC location (P ¼ 0.04; x2 test), reflecting CD-CRCs, in contrast to 2 of 24 (8.3%) sporadic mucinous
the different etiology of CRC (Table 1; Supplementary Table S3). CRCs. This is in line with TCGA data on intestinal type (n ¼
The two CRC groups of different etiology were matched in terms 129) and mucinous (n ¼ 15) CRCs that rarely showed a 5p
of sex (P ¼ 0.57; Fisher's exact test) and tumor stage at diagnosis copy-number gain (20 of 129, 16% and 1 of 15, 7%, respec-
(P ¼ 0.31; x2 test). tively) or loss (10 of 129, 8% and 0 of 15, 0%, respectively;
Supplementary Fig. S6). The gain of 5p in CD-CRCs was
Landscape of genomic imbalances in CD-CRCs versus sporadic confirmed by interphase FISH on tumor sections (Fig. 1E;
mucinous CRCs Supplementary Table S4), and by copy-number profiles derived
To determine genome alterations that characterize CD-CRCs, from targeted sequencing data (Supplementary Fig. S7).
we performed aCGH and sequence analysis of a panel of 563
cancer-related genes (Supplementary Table S1 for gene list). Landscape of somatic mutations in CD-CRCs versus sporadic
As control groups, we used histomorphologically similar spo- mucinous CRCs
radic mucinous adenocarcinomas, and the TCGA CRC dataset For sequencing data analysis, the applied Strelka and MuTect
(15). The number of SCNAs per tumor tended to be higher in variant calling algorithms resulted in a total of 814 variant calls
CD-CRCs compared with sporadic mucinous CRCs (P ¼ 0.07; with a core fraction of 84% of concordant calls (Supplementary
Mann–Whitney test; Fig. 1B), while the fraction of the genome Fig. S8). The highest mutation counts were observed in the
subject to SCNAs was similar (P ¼ 0.88; Mann–Whitney POLE-mutated CD-CRC (C21CA2) followed by MSI-H tumors
www.aacrjournals.org Clin Cancer Res; 2018 OF5
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Hirsch et al.
Figure 1.
Histology and copy-number alterations in Crohn's disease–associated colorectal carcinomas (CD-CRC) and sporadic mucinous colorectal carcinomas
(MUC-CRCs). A, CD-CRCs frequently show areas with extracellular (mucinous) and/or intracellular (signet ring cell) mucin accumulation. B, Number of
somatic copy-number alterations tends to be higher in CD-CRC than in MUC-CRC (P ¼ 0.07). C, Fraction of copy-number–altered genome does
not differ significantly between CD-CRC and MUC-CRC (P ¼ 0.88). D, Cumulative copy-number frequencies for CD-CRC and MUC-CRC cohorts.
Numbers below the graph (x-axis) denote chromosomes, frequency (y-axis) denotes the proportion of microsatellite stable, non-hypermutated samples with
a gain or a loss at the respective chromosomal position. E, Representative fluorescence in situ hybridization images, confirming the frequent gain of
chromosome arm 5p in CD-CRC.
(C20 and C28; Supplementary Fig. S9A). Those samples with predominantly in the DNA binding domain of the protein
the highest mutation counts had the lowest amount of SCNAs (Supplementary Fig. S10). Mutations in KRAS, the second
(Supplementary Fig. S9B and S9C). The base substitution most commonly mutated gene in both CRC entities, occurred
patterns in CD-CRCs and sporadic mucinous CRCs were very exclusively as missense mutations and involved the known
similar (Supplementary Fig. S9D) and typical for colonic tissue mutation hotspots, independent of CRC etiology (Supplemen-
(38). Somatic mutations in CD-CRCs involved genes known tary Fig. S11). In contrast to TP53 and KRAS mutations, APC
to be significantly altered in CRC; however, mutation frequen- mutations in both CD-CRC and sporadic mucinous CRC were
cies were different compared with sporadic mucinous CRC truncating mutations. While the distribution of APC mutations
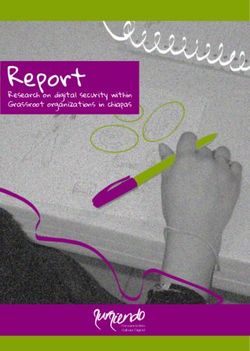
(Fig. 2A): TP53 (76% in CD-CRCs vs. 33% in sporadic mucin- in sporadic mucinous CRCs reflected the distribution expected
ous CRCs), KRAS (24% vs. 50%), APC (17% vs. 75%), and from TCGA data on sporadic CRC and involved high-frequency
SMAD3 (3% vs. 29%). While TP53 missense mutations showed mutations according to the COSMIC database, the few APC
a strongly increased nuclear positivity for TP53 compared to the mutations detected in CD-CRCs were primarily located at
wild-type staining pattern, a TP53 truncating mutation was positions infrequently mutated in sporadic CRC, which was
associated with a complete absence of staining (Fig. 2B). reflected by the reported low frequency of these mutations in
Both in CD-CRCs and sporadic mucinous CRCs, the majority COSMIC (Supplementary Fig. S12). In summary, CD-CRCs
of TP53 mutations occurred as missense mutations, located demonstrated major mutational differences compared to
OF6 Clin Cancer Res; 2018 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Genetics of Colorectal Cancer Development in Crohn's Disease
Figure 2.
Mutational landscape of CD–associated colorectal carcinomas (CRCs). A, "Oncoprint" showing genes mutated in >10% in either of the analyzed carcinoma
groups, genes reported as significantly mutated in CRC according to TCGA data, and genes previously reported as significantly mutated in colitis-associated
cancer by Robles and colleagues (13) or Yaeger and colleagues (14). Each row represents a clinicopathologic feature or gene, each column denotes an
individual carcinoma sample. Mutation frequencies are based only on microsatellite stable, non-hypermutated cases. B, Immunohistochemical
staining of TP53 for determining TP53 mutation status. Abnormal overexpression, that is, strongly intense staining in tumor cell nuclei (C01CA3, C04CA1,
and C12CA), or abnormal complete absence of expression within tumor cell nuclei (C04CA2) indicates TP53 mutation, while normal or wild-type
pattern (C17CA) is characterized by variable staining intensity. Scale bars, 100 mm.
sporadic CRCs including TCGA CRC data (Table 2). Of note is Altered pathways in CD-CRC versus sporadic mucinous CRC
the high frequency of TP53 mutations in inflammation-asso- To better understand the consequences of mutations and how
ciated CRCs compared with sporadic intestinal type CRCs and pathways were altered in CD-CRCs compared with sporadic
in particular compared with sporadic mucinous CRCs. mucinous CRC, we integrated mutation and copy-number data
www.aacrjournals.org Clin Cancer Res; 2018 OF7
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Hirsch et al.
Table 2. Comparison of mutation frequencies in Crohn's disease–associated colorectal carcinomas (CD-CRCs) in the current report with the frequencies
reported by Robles and colleagues (13) and by Yaeger and colleagues (14), and comparison with frequencies in TCGA data (15) of CRCs of mucinous and
intestinal-type histology
Abbreviations: NR, mutation frequency of the respective gene not reported; NI, respective gene not included in sequencing panel (FoundationOne Assay/MSK-
IMPACT Assay).
a
All microsatellite stable (MSS).
b
Microsatellite/hypermutation status not determined.
c
Includes two small intestinal carcinomas.
to analyze alterations in WNT, TGF-b, PI3K, RTK-RAS, and TP53 synchronous lesions from separate sites, both synchronous car-
signaling pathways (Fig. 3; Supplementary Figs. S13 and S14). cinomas and synchronous precursor lesions/carcinomas, were
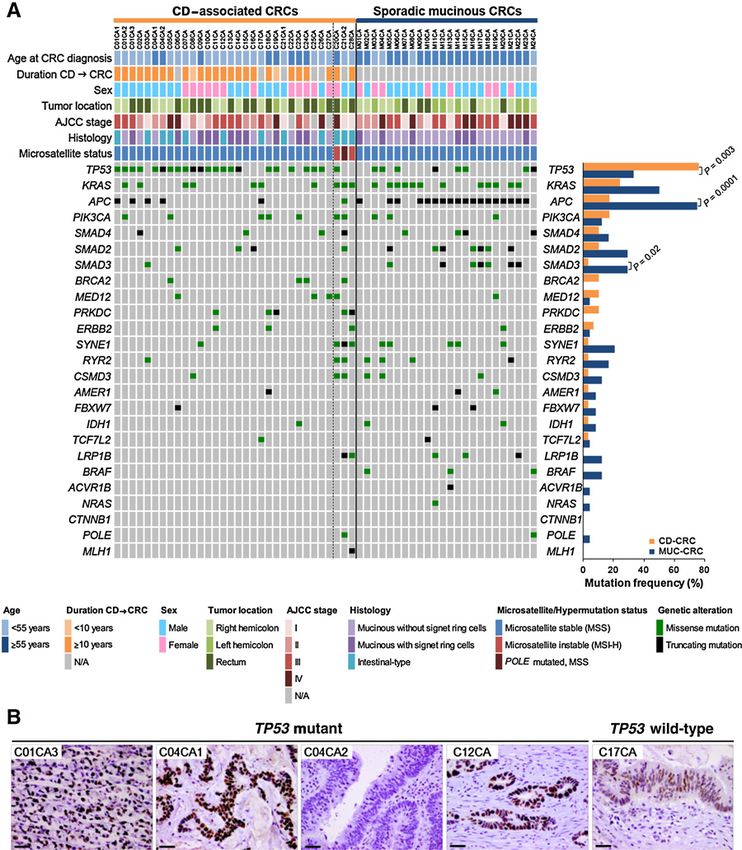
While genetic alterations in the TP53 signaling pathway were distinct. For instance, in patient C04 both carcinomas showed
predominant in CD-CRCs, WNT, TGFb and, although to a lesser copy-number increases of 5p and mutations of TP53, yet different
degree, RTK/RAS signaling was more often affected in sporadic ones, while inflamed mucosa harbored three mutations (FGF23,
mucinous CRC. PLAG1, and SMARCA4) but no SCNAs, and no genome altera-
tions were present in normal mucosa (Fig. 4A). Similarly, three
Analysis of CD–associated precursor lesions and matched carcinomas and histologically normal colonic mucosa from
primary CD-CRCs: tumor evolution and sequence of patient C01, all spatially separated, were affected by distinct TP53
genetic events mutations. Only the inflamed mucosa samples and the dysplasia
Our collection of samples included 11 patients (patients C01, adjacent to carcinoma 1 shared their TP53 mutation with carci-
C02, C04, C05, C06, C07, C11, C12, C18, C21, and C26), from noma 1 (Fig. 4B). The gain of 5p was present in all lesions from
which we could analyze multiple, synchronous lesions at different patient C01, except carcinoma 2. Of note, carcinomas 1 and 3
stages of tumor development accompanying the CD-CRC (Sup- from patient C01 shared an identical APC mutation (p.T1556fs),
plementary Fig. S1 for an overview of samples for analysis per while the respective TP53 mutations (p.R175H in carcinoma 1
patient). In general, the mutation load increased during disease and p.E286K in carcinoma 3), among other mutations, were
progression, and so did the number of SCNAs and the fraction of distinct. The TP53 p.R175H mutation, in contrast to the APC
the genome affected by SCNAs (Supplementary Fig. S15). Across p.T1556fs mutation, could also be detected in the inflamed
all synchronous lesions from the above-mentioned patients mucosa samples adjacent to carcinoma 1, indicating that the
(except patient C21, who was excluded due to POLE mutation TP53 p.R175H mutation had occurred before the APC p.T1556fs
in one of his carcinomas), the gain of 5p was the most frequent mutation. However, the TP53 p.R175H mutation, despite equiv-
SCNA present in three of 11 non-dysplastic colonic mucosa alent or higher mutant allele fractions, could not be detected in
samples, two of three dysplastic lesions, 11 of 13 carcinomas, carcinoma 3, which instead harbored a distinct TP53 p.E286K
and two of two lymph node metastases. TP53 was the most mutation. On the basis of these observations, we assumed that
frequently mutated gene occurring in four of 14 non-dysplastic carcinoma 1 and carcinoma 3 evolved independently, though in
colonic mucosa samples, two of three dysplastic lesions, 13 of 13 general the presence of an identical mutation in a tumor sup-
carcinomas, and two of two lymph node metastases (Supplemen- pressor gene in two independent lesions is considered very
tary Fig. S16 for an overview of all mutations in patients with CD- unlikely. Patient C12 had one carcinoma and one dysplastic
CRC with multiple lesions). Interestingly, TP53 mutations in lesion, which both harbored a 5p gain and a TP53 mutation, yet
OF8 Clin Cancer Res; 2018 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Genetics of Colorectal Cancer Development in Crohn's Disease
Figure 3.
Distribution and frequency of genetic alterations leading to deregulation of signaling pathways in Crohn's disease–associated colorectal carcinomas
(CD-CRC) and sporadic mucinous colorectal carcinomas (MUC-CRC). Only microsatellite stable, non-hypermutated tumors were included in the analysis.
A, Pathway analysis map. Alteration frequencies are expressed as a percentage of CD-CRC and of MUC-CRC cases. Red denotes activated genes and
blue denotes inactivated genes with the color intensity corresponding to the percentage of cases altered. B, Pathway alteration pattern. A pathway was
considered altered, if at least one gene in the respective pathway harbored a genetic alteration.
mutations were different (Supplementary Fig. S17). In patient each had a TP53-mutated carcinoma with a 5p gain, while no
C26, the carcinoma had a TP53 mutation and a gain of 5p, aberrations were observed in normal or inflamed mucosa
while the dysplastic lesion was TP53 wild-type but had muta- (Supplementary Figs. S21 and S22). Patient C07 revealed no
tions in APC and KRAS, and no 5p gain (Supplementary genetic aberrations in the inflamed mucosa sample, but a TP53
Fig. S18). Patient C18 had TP53 mutations, both in the carci- mutation and SCNAs, however without a 5p gain, in the
noma and in histologically normal colonic mucosa; however, carcinoma (Supplementary Fig. S23). In patient C06, mutation
they were distinct from each other (Supplementary Fig. S19). A load and SCNAs increased from the CRC to its corresponding
gain of 5p could be detected in the carcinoma but not in lymph node metastasis, though both harbored similar changes,
histologically normal colonic mucosa despite the presence of including identical TP53 mutations and the gain of 5p (Sup-
SCNAs. The carcinoma of patient C05 showed a TP53 mutation, plementary Fig. S24).
and a 5p gain, while interestingly, the inflamed mucosa, his- To further delineate the sequence of genetic events under-
tologically without signs of dysplasia, showed five mutations, lying tumor development in CD, we analyzed mutant allele
including an FBXW7 mutation, but neither a TP53 mutation fractions. Potential founder mutations (and/or mutations
nor SCNAs (Supplementary Fig. S20). Patients C02 and C11 providing a great selective advantage) would be expected at
www.aacrjournals.org Clin Cancer Res; 2018 OF9
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Hirsch et al.
Figure 4.
Tumor heterogeneity: spatial and phylogenetic relationship of lesions. Left, the anatomic location of all analyzed samples from patients C04 (A) and
C01 (B) is depicted along the colon frame. Selected somatic mutations and genome-wide copy-number alterations are displayed with the respective
histology. The outer circle indicates genome-wide chromosomal gains (red) and losses (blue) with their chromosomal location (1–22). Right, corresponding
phylogenetic trees of neoplasia development. The different colors in the circles indicate different neoplastic clones, that is, different founder mutations,
and correspond to the color of the outermost circle on the left part. Color intensity correlates with general mutation load.
OF10 Clin Cancer Res; 2018 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Genetics of Colorectal Cancer Development in Crohn's Disease
fractions of 0.28 0.13 (mean tumor cell content divided by 2 progression (Fig. 5A; refs. 9, 10). In CD, TP53 mutation and 5p
2 SD; Supplementary Table S5) for CRCs (n ¼ 53), and gain occurred early and were frequent, while APC and KRAS
0.29 0.06 (mean epithelial cell content divided by 2 2 mutations occurred later and were rare.
SD; Supplementary Table S6) for precursor lesions (n ¼ 12),
while higher allele fractions indicate an additional loss of Detection of mutant clones at non-dysplastic sites distinct
heterozygosity, and lower allele fractions indicate subclonal from carcinoma: evidence for occult tumor evolution in
mutations (39). Applying these criteria, clonal and thus poten- patients with CD
tial founder mutations in CD-CRCs mainly occurred in TP53, The fact that we observed genome alterations in normal and
sometimes accompanied by an allelic loss, while in sporadic inflamed colonic mucosa without histologic evidence for dys-
mucinous CRCs clonal mutations were distributed among plasia led to further investigations. In 19 of 28 patients with
APC, KRAS, and TP53 (Supplementary Fig. S25A). Interesting- CD-CRC, we analyzed samples of non-dysplastic mucosa com-
ly, in precursor lesions TP53 mutations were virtually all prising histologically normal colonic mucosa (n ¼ 16) and
clonal, in few samples accompanied by additional allelic loss, inflamed mucosa (n ¼ 7; Supplementary Fig. S1). None of the
while mutations in other genes were mostly subclonal (Sup- normal and inflamed colonic mucosa samples showed evi-
plementary Fig. S25B). Of note, the majority of these subclonal dence for MSI (Supplementary Table S7). By aCGH, we
mutations occurred in genes that did not show alterations in detected SCNAs in two normal colonic mucosa samples
CD-CRCs, indicating that these mutant clones do not neces- (C01NOR and C18NOR), and two inflamed mucosa samples
sarily have the potential to progress and may disappear over (C01INF1 and C01INF2; Fig. 4B; Supplementary Fig. S19).
time. Sequencing revealed mutations in TP53 in four of the normal
On the basis of our analyses, we could reconstruct the putative and inflamed mucosa samples (C01INF1, C01INF2, C01NOR,
sequence of genetic events of CD–related colorectal carcinogen- and C18NOR), and mutations in genes other than TP53 in two
esis, which is different from sporadic adenoma to carcinoma other inflamed mucosa samples (C04INF and C05INF; Fig. 4;
Figure 5.
Genetic progression of CD–associated
CRCs. A, Genetic events in the
progression of CD over time. TP53
mutation and copy-number gain of
chromosome arm 5p occur early and
occasionally already in non-dysplastic
(normal/inflamed) mucosa. The gain
of 5p is specific to CD–associated
tumorigenesis; APC and KRAS
mutations define the transition to
dysplasia; SMAD2/4 gene mutations
were exclusively observed in
carcinomas. Chromosomal copy-
number changes are already present in
normal, inflamed, and dysplastic
colonic mucosa; the degree of
aneuploidy and the mutation burden
increase during disease progression.
B, Our data suggest two distinct
genetic mechanisms for CRC
progression in patients with CD: (i)
clonal sweeps, that is, a clone with a
specific mutation expands to cover
large colonic segments, from which
further clones with additional
mutations can emerge, and (ii) clonal
mosaicism, that is, multiple clones with
distinct (founder) mutations arise
independently at different locations
of the colorectum.
www.aacrjournals.org Clin Cancer Res; 2018 OF11
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Hirsch et al.
Supplementary Figs. S19 and S20). Thus, in total, four of 19 ports the critical role of TP53 signaling in CD–associated tumor-
(21%) patients with CD-CRC harbored at least one mutation igenesis. Inactivation of TP53 signaling was a nearly ubiquitous
and/or SCNAs in normal or inflamed, that is, non-dysplastic, event in CD-CRC in our cohort, while, in contrast to sporadic
colonic mucosa (six of 23 samples), pointing to an occult CRC, WNT pathway activation by mutation was rare. However,
tumor evolution in patients with CD. Interestingly, all normal this does not exclude WNT pathway activation through epigenetic
and inflamed mucosa samples with the presence of SCNAs had or microenvironmental influences.
a TP53 mutation, while normal and inflamed colonic mucosa In general, the mutational spectrum for CD-CRC confirms
with wild-type TP53 status showed no SCNAs (Supplementary findings from previous studies (13, 14). However, by studying
Table S8). TP53 mutation status could be visualized by IHC, the so far largest collective of CD-CRCs and precursor lesions,
showing a characteristic "nested" or "diffuse" staining pattern distinct features emerged. While Robles and colleagues found
that can be confined to the basal half of the crypts, as originally similar or slightly lower mutations rates within CD-CRCs com-
described in TP53-mutated, non-dysplastic mucosa from pared with our study by whole exome sequencing, Yaeger and
patients with UC (Supplementary Fig. S26–29; refs. 35, 36). colleagues detected a higher TP53 (94% vs. 76%) and IDH1
(28% vs. 3%) mutation rate within CD-CRCs using a targeted
Development and progression of CRC in patients with CD sequencing approach covering some 300 genes (13, 14). Overall,
through clonal sweeps and clonal mosaicism our mutation frequencies match the average of the two above-
The distribution of mutations across multiple samples along mentioned studies. However, we could not confirm the high
the colorectum at different stages of tumor development from 11 IDH1 mutation rate in CD-CRC reported by Yaeger and colleagues
individual patients suggests two distinct mechanisms for CRC (14). In line with previous studies and in contrast to sporadic
development and progression in patients with CD: (i) clonal CRC, BRAF mutations were absent from CD-CRCs (overall muta-
sweeps, that is, a clone with a specific mutation expands to cover tion rate 19% in sporadic CRC; 3% in non-hypermutated CRC
large colonic segments, from which further clones with additional and 46% in hypermutated CRC; 37% in mucinous CRC and
mutations can emerge; and (ii) clonal mosaicism, that is, multiple 6% in nonmucinous CRC; refs. 13, 14, 43, 44).
clones with distinct (founder) mutations arise independently at In our cohort of CD-CRCs, we detected MSI at a similar
different locations of the colorectum (Fig. 5B; ref. 40). There was a frequency (2 of 32, 6.3%) as Lennerz and colleagues (2 of 33,
predilection for TP53 mutations, and, interestingly, all synchro- 6.1%; ref. 43). This frequency is slightly lower compared with
nous CRCs from individual patients showed distinct TP53 muta- sporadic CRC and to that reported by Svrcek and colleagues (7 of
tions, as did spatially unrelated precursor lesions. 50, 14%; ref. 45). This slight difference might be a reflection of
small sample numbers in both studies. In contrast to UC where
MSI usually occurs early (46), we did not detect MSI in CD–related
Discussion precursor lesions. Consistently, Svrcek and colleagues did not
Our study of CD-CRCs and corresponding precursor detect MSI in any of the 14 dysplastic CD samples included in their
lesions analyzed by targeted NGS and aCGH revealed a signi- study (45).
ficant difference in the pattern of mutations and SCNAs As summarized by Ullman and Itzkowitz, the development of
between CD-CRC and sporadic CRC. According to data from inflammation-related carcinoma appears to progress through a
TCGA, APC mutations are the major event in sporadic non- sequence consisting of inflamed mucosa, dysplasia, carcinoma, in
hypermutated CRC (observed in 81% of cases), followed by contrast to the classical progression of a discrete focus of neoplasia
TP53 (60%) and KRAS mutations (43%; ref. 15). In contrast, we from a polypoid adenoma to an invasive carcinoma in sporadic
found in CD-CRC a much lower frequency of APC mutations CRC (8). However, patients with CD can also develop sporadic
(17%) and a higher rate of TP53 mutations (76%). The genetic adenomas but endoscopic and histologic distinction of an inflam-
differences suggest distinct pathways of carcinogenesis. TP53 mation-/CD–associated lesion and a sporadic adenoma arising in
mutations likely play an initiating role in CRC associated with an inflamed colon segment is extremely difficult. The distinction
chronic inflammation of the large intestine, whereas in spo- is critical: while a sporadic lesion offers the therapeutic option for
radic CRC, they are more important for the progression from a safe local removal followed by surveillance, in case of an
late adenoma to invasive carcinoma (41). The high frequency inflammation-/CD–associated dysplastic lesion and possible
of TP53 mutations in non-dysplastic and dysplastic colonic field cancerization, proctocolectomy should be considered as
mucosa of patients with UC was already reported, and for treatment (47). As shown recently, the detection of aneuploidy
diagnostic purposes, TP53 status can be determined by IHC could be useful in identifying patients with UC and CD with an
as a surrogate for the detection of TP53 mutations (35, 36). This increased progression risk toward CRC (48). Similarly, the pres-
is far less well studied in CD and CD-CRC. One study of a ence of SCNAs in gastric intestinal metaplasia has recently been
cohort of 14 patients with CD revealed that IHC TP53 positivity identified as a molecular determinant of progression to dysplasia
was associated with dysplasia and could predict progression or gastric cancer (49).
to CRC in some cases (42). In contrast to sporadic CRC, we Our findings confirm aneuploidy as an early event in CD
detected TP53 mutations in both dysplasia and non-dysplastic progression; however, we identified a specific significant differ-
mucosa from patients with CD-CRC. As a side note, IHC for ence in the pattern of SCNAs, namely the gain of chromosome
TP53 was able to confirm mutational status and could therefore arm 5p, in CD-CRCs compared with sporadic tumors. The copy-
be helpful in the evaluation of colonic biopsies from patients number increase of 5p is particularly interesting because it was not
with CD with respect to their progression risk. only frequently present in CD-CRC, but also a common finding in
We observed distinct TP53 mutations in different, spatially precursor lesions including yet non-dysplastic colonic mucosa. In
unrelated lesions in four patients in our cohort, a genetic phe- contrast, sporadic colorectal adenomas very rarely show a gain of
nomenon termed "clonal mosaicism." This finding further sup- 5p. In our own previously published cohort of hyperplastic
OF12 Clin Cancer Res; 2018 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on January 16, 2021. © 2018 American Association for
Cancer Research.Published OnlineFirst July 2, 2018; DOI: 10.1158/1078-0432.CCR-18-0630
Genetics of Colorectal Cancer Development in Crohn's Disease
polyps, tubulovillous adenomas and serrated polyps (n ¼ 84), we Disclosure of Potential Conflicts of Interest
did not detect any 5p gain (50). Adenomatous regions of malig- No potential conflicts of interest were disclosed.
nant polyps did not harbor a 5p gain either (n ¼ 13; ref. 12).
Richter and colleagues found extra copies of 5p only in non- Authors' Contributions
polypoid dysplastic lesions (2 of 23, 9%), while polypoid neo- Conception and design: D. Hirsch, D.C. Edelman, P. Kienle, C. Galata,
plasia never showed this gain (0 of 28, 0%; ref. 51). Interestingly, K. Horisberger, T. Ried, T. Gaiser
Development of methodology: D. Hirsch, D.C. Edelman, C. Galata
they observed gains of the entire chromosome 5, while in our CD–
Acquisition of data (provided animals, acquired and managed patients,
associated lesions the gain was restricted to the short arm of the provided facilities, etc.): D. Hirsch, D. Wangsa, D.C. Edelman, P.S. Meltzer,
chromosome, sometimes extending to the 5q pericentromeric C. Ott, P. Kienle, K. Horisberger
region, and sometimes accompanied by a loss of 5q indicating Analysis and interpretation of data (e.g., statistical analysis, biostatistics,
isochromosome formation. Our findings are consistent with CGH computational analysis): D. Hirsch, D. Wangsa, Y.J. Zhu, Y. Hu, P.S. Meltzer,
data from 13 UC-CRCs, which revealed in about 50% of samples a K. Heselmeyer-Haddad, P. Kienle, T. Ried, T. Gaiser
Writing, review, and/or revision of the manuscript: D. Hirsch, D. Wangsa,
gain of 5p, and in about 25% a concomitant loss of 5q (52). This is
Y.J. Zhu, Y. Hu, D.C. Edelman, P.S. Meltzer, K. Heselmeyer-Haddad, C. Ott,
particularly intriguing because in that cohort 5p was also an early P. Kienle, C. Galata, K. Horisberger, T. Ried, T. Gaiser
event that could already be observed in ulcerative colitis–associ- Administrative, technical, or material support (i.e., reporting or organiz-
ated dysplastic lesions. Interestingly, while early sporadic colo- ing data, constructing databases): D. Hirsch, D. Wangsa, D.C. Edelman,
rectal lesions are often characterized by gains of chromosome 7 P.S. Meltzer, K. Heselmeyer-Haddad, C. Ott, P. Kienle, C. Galata, K. Horisberger,
(10, 11), 5p gains appear to be the distinctive feature of inflam- T. Ried, T. Gaiser
Study supervision: D. Hirsch, P. Kienle, T. Ried, T. Gaiser
mation-associated, and in particular, CD–associated intestinal
neoplasia.
Gains of 5p have previously been implicated in progression of Acknowledgments
The authors would like to thank David Petersen (Molecular Genetics
lung and cervical cancer, but it appeared difficult to relate this Section, Genetics Branch, CCR, NCI, and NIH) for help with library pre-
SCNA to a specific candidate gene (53, 54). Nevertheless, the TERT paration, Bao Tran (Sequencing Facility, CCR, NCI-Frederick, NIH) for
gene (5p15.33) encodes one of the main functional subunits of performing sequencing, Yonca Ceribas, Alexandra Eichhorn and Romina
the telomerase enzyme and high TERT expression was shown to Laegel (Institute of Pathology, University Medical Center Mannheim) for
be associated with progression and unfavorable outcome of CRC technical assistance, Ferdinand Hofstaedter and Matthias Evert (Institute of
Pathology, University of Regensburg) for administrative/material support,
(55, 56). Another study demonstrated that increased expression
Buddy Chen for help with figures and IT-related support, and Reinhard
of TERT can promote antiapoptotic response through inactivation Ebner for critical comments on the manuscript. This study was supported
of TP53 via induction of basic fibroblast growth factor (57). in part by the Intramural Research Program of the NIH, NCI, and by a grant
Furthermore, CDH12 (5p14.3) was reported to enhance prolif- from the Manfred Stolte-Foundation (to D. Hirsch and T. Gaiser). D. Hirsch
eration and tumorigenicity of CRC cells and to increase progres- received an intramural research scholarship from the Medical Faculty
sion by promoting epithelial–mesenchymal transition (58, 59). Mannheim, Heidelberg University.
In conclusion, our study of CD–related colorectal lesions
The costs of publication of this article were defrayed in part by the
indicates a new biomarker, that is, the gain of 5p, which, in
payment of page charges. This article must therefore be hereby marked
combination with TP53 IHC or TP53 mutation analysis, could advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate
assist in the assessment of CD precursor lesions that might this fact.
progress to CRC. This intriguing finding should be pursued in
further clinical validation studies, in particular in the context of Received February 23, 2018; revised April 23, 2018; accepted June 25, 2018;
occult tumor evolution in patients with CD. published first July 2, 2018.
References
1. Gillen CD, Walmsley RS, Prior P, Andrews HA, Allan RN. Ulcerative 8. Ullman TA, Itzkowitz SH. Intestinal inflammation and cancer.
colitis and Crohn's disease: a comparison of the colorectal cancer risk in Gastroenterology 2011;140:1807–16.
extensive colitis. Gut 1994;35:1590–2. 9. Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell
2. Beaugerie L, Itzkowitz SH. Cancers complicating inflammatory bowel 1990;61:759–67.
disease. N Engl J Med 2015;372:1441–52. 10. Ried T, Knutzen R, Steinbeck R, Blegen H, Schrock E, Heselmeyer K, et al.
3. Choi PM, Zelig MP. Similarity of colorectal cancer in Crohn's disease Comparative genomic hybridization reveals a specific pattern of chromo-
and ulcerative colitis: implications for carcinogenesis and prevention. somal gains and losses during the genesis of colorectal tumors. Genes
Gut 1994;35:950–4. Chromosomes Cancer 1996;15:234–45.
4. Ribeiro MB, Greenstein AJ, Sachar DB, Barth J, Balasubramanian S, Harpaz 11. Bardi G, Pandis N, Fenger C, Heim S. Trisomy 7 as the sole cytogenetic
N, et al. Colorectal adenocarcinoma in Crohn's disease. Ann Surg 1996; aberration in the epithelial component of a colonic adenoma. Cancer
223:186–93. Genet Cytogenet 1995;82:82–4.
5. Averboukh F, Ziv Y, Kariv Y, Zmora O, Dotan I, Klausner JM, et al. 12. Hirsch D, Camps J, Varma S, Kemmerling R, Stapleton M, Ried T, et al. A
Colorectal carcinoma in inflammatory bowel disease: a comparison new whole genome amplification method for studying clonal evolution
between Crohn's and ulcerative colitis. Colorectal Dis 2011;13: patterns in malignant colorectal polyps. Genes Chromosomes Cancer
1230–5. 2012;51:490–500.
6. Tan Y, Fu J, Li X, Yang J, Jiang M, Ding K, et al. A minor (You can also read