Epilepsy for the General Internist
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Epilepsy for the General Internist
William O. Tatum DO, FAAN, FACNS
Professor of Neurology
Mayo College of Medicine
Senior Consultant, Mayo Clinic Florida
Director, Epilepsy Center and Monitoring Unit
Jacksonville, Florida USA
14th Annual Internal Medicine Conference
March 26, 2017
©2016 MFMER | slide-1
Confluence of Interest
Professional Affiliations
• American Clinical Neurophysiology Society
• EFA and ILAE
• American Board of Clinical Neurophysiology
Financial Disclosure
• Demos Publishers Inc., Springer Publishers
• Epilepsy & Behavior Case Report journal: Editor-in-Chief
• Grant support
– Mayo Clinic
– Brain Sentinel®
• Consultant: SK Life Science
©2016 MFMER | slide-2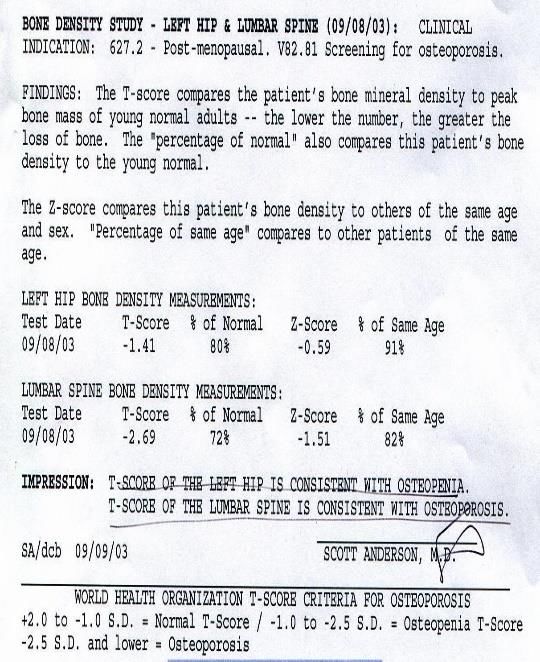
An 18 y/o female with migraine
experienced her first “grand mal”
seizure after partying the night
before. In the ED, she was loaded
with IV PHT and begun on PHT 200
mg PO BID (15 ug/dl). An increase
in morning “jerks” occurred.
Following a normal MRI and VIDEO
abnormal EEG with GSW, she was
begun on VPA ER and titrated to
1000 mg PO q HS. She had no
further seizures but she was dizzy,
had blurry vision & an unsteady gait.
Does she have epilepsy? ©2016 MFMER | slide-3
The First Seizure
• Recurrence greatest in 1st 2 years (21-45%).
• Response to the 1st ASD predicts control.1
• + risk factors double the likelihood &
treatment with ASDs halves it.2
• Prior brain insult (level A)
• Epileptiform EEG (level A)
• Abnormal MRI/nocturnal Sz (level B)
• ASD treatment renders 65-85% seizure free3
1. Brodie MJ et al. Neurology 2012;78:1548–1554.
• SE occur in 7-31% (level B).2 2. Krumholz A et al. Neurology 2015;84:1705–1713.
3. Hakami T, et al. Neurology 2013;81(10):920-7.
Her EEG demonstrated epileptiform discharges
©2016 MFMER | slide-4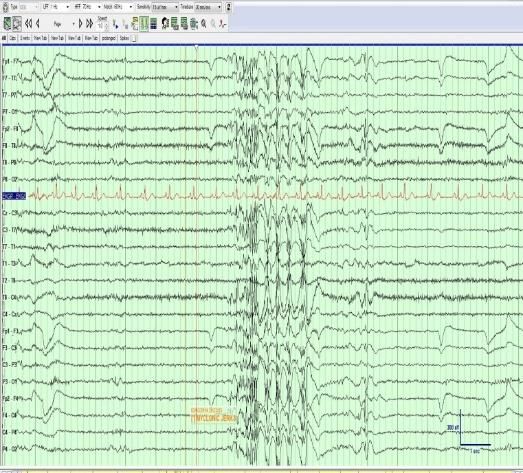
Epilepsy
• Definition: Epilepsy exists after a single unprovoked seizure
when the risk of a recurrence is >60%.1
• Nearly 3 million people in U.S.
• One epileptic seizure/life-time occurs in 1/10 people.
• 70% of adults with new-onset epilepsy have focal seizures.2
• The cause is unknown in 62%. In the rest, stroke 9%, trauma
9%, alcohol 6%, neurodegenerative 4%, static encephalopathy
3.5%, brain tumor 3%, and infection in 2%.
• PCP in the US see 83% of new-onset cases;
40% with epilepsy.3
1. Fisher R et al. Epilepsia 2014;55(4):475-82.
2. French JA, Pedley TA. N Engl J Med 2008;359:166-76.
3. Smith MC, Buelow J. Epilepsy. Dis Mon 1996;42(11):729-827.
• .
Yes, she does have epilepsy
©2016 MFMER | slide-5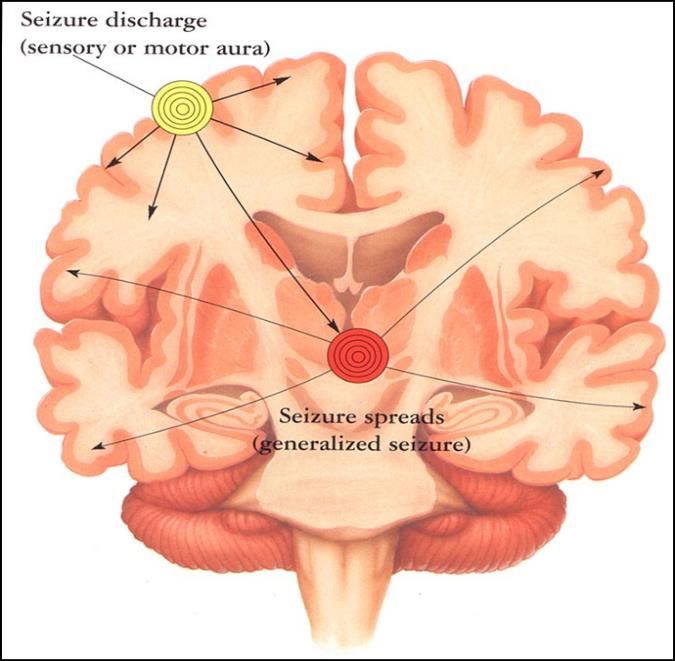
Seizures are a Symptom
• An age-related predisposition exists that reflects cause.
• Brain malformations and infection during childhood
• Trauma and brain tumor in mid-life
• Stroke and dementia in later life
Annegers JF. The Epidemiology of Epilepsy. In: Wyllie E, ed. The treatment of epilepsy: principles & practice. Philadelphia: LWW. 2001:165-72.
©2016 MFMER | slide-6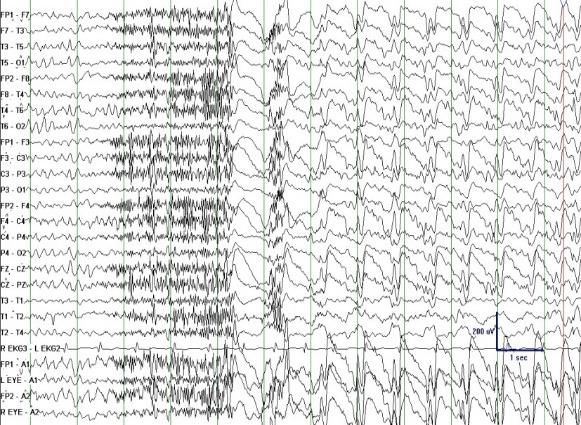
The Impact of Epilepsy
• Mental & physical QoL worse.
• Memory and cognitive impairment worse.
• Neurotoxicity due to ASDs and seizures.
• Co-morbidities are more common (DM,
smoking, obesity, stroke, and depression
greater).
• Injury, unemployment, household and lifetime
income reduced, and health care over-
utilization is more common.
©2016 MFMER | slide-7
Driving • State-specific driving laws exist. • Epilepsy increases the risk of MVAs (up to 7x).1 • Fatalities rare (

Pharmacologic Management
• Classification is the foundation for ASD selection;
focal or generalized?
• When unclear or unknown…
• Broad spectrum ASDs
• VPA, LTG, TPM, LEV, ZNS
• Treatment should be a hierarchy
• Efficacy, safety, tolerability
• ASD monotherapy if possible
Scheffer I et al. Epilepsia 2017:8 MAR 2017 | DOI: 10.1111/epi.13709
With myoclonus & GTC seizures she needs a broad spectrum ASD.
©2016 MFMER | slide-9
Genetic Generalized Epilepsy
• Absence, myoclonic, (clonic)-tonic-clonic
• Genetic influence
• Common in children
• Normal neuroimaging and intelligence
• Treatment responsive
• ETH for CAE1,3
• VPA1,3 (JAE, JME, GTC)
• LEV, LTG, TPM, ZNS
1.Nadkarni S et al. Neurology 2005;64(suppl3):S2-S11.
2.Nicolson A et al. JNNP 2004;75:75-79.
3.Karceski S et al. Epilepsy & Behavior 2005;7:S1-S64.
Our patient has Juvenile Myoclonic Epilepsy
©2016 MFMER | slide-10Focal Epilepsy
• Most common type in adults
• > 60% of epilepsies
• Temporal lobe epilepsy is most common
• Focal seizures with and without impaired
consciousness, focal evolving to convulsion
• Due to focal CNS “lesion”
• EEG may clarify seizure classification.
• Treatment
• *Initial: CBZ, LTG, OXC
• Alternate: LEV
*Karceski S et al. Epilepsy & Behavior 2005;7:S1-S64.
Up to 50% of JME manifest lateralized features.
©2016 MFMER | slide-11Encephalopathic Epilepsy
• Clinical features
• Mixed seizure types & cognitive impairment
• EEG abnormalities
• West’s Syndrome
• Epileptic spasms
• Lennox-Gastaut syndrome
• Tonic-atonic
• Atypical absence
• Refractory to treatment; recurrent injury
• Broad spectrum ASDs
• Surgical procedures
Winesett SP, Tatum WO. In: Wyllie’s Treatment of Epilepsy Principles and Practice. 6th edition: Wolters Kluwer. Philadelphia, PA 2015.
©2016 MFMER | slide-12Treatment
• Antiseizure Drugs1
• Seizure freedom
• No side-effects
• Epilepsy Surgery2
• Neurostimulation3
• Ketogenic Diet4
1.Kwan P, Brodie MJ. Neurology 2003;60(Suppl 4):S2-S12.
2.Wiebe S et al. NEJM 2001;345:311-318.
3.Cascino GD. Epilepsia 2008;49(Suppl 9):79-84.
4.Sirven J et al. Epilepsia 1999;40:1721-1726.
©2016 MFMER | slide-13Anti-Seizure Drugs
• None alter the course of the disease process (“AEDs”).
• All current ASDs provide symptomatic treatment.
• Effective in focal seizures 2/3rds of the time in generalized
seizures 80-85% of the time.
• The response to ASD treatment has been stable over time.
• All ASDs potentially have adverse events and none treat the
non-seizure symptoms (e.g. neurocognitive, psychosocial).
• No ASDs are truly prophylactic for prevention of epilepsy (due
to trauma, stroke, brain tumor etc.).
Mohanraj R, Brodie MJ. Eur J Neurol 2006;13:277–282.
Kwan P, Schachter SC, Brodie MJ. N Engl J Med 2011;369:919–926.
©2016 MFMER | slide-14Consider Treatment after a First Seizure
• If it really wasn’t the first seizure and other
seizure types were present (our patient).
• Prolonged seizure or status epilepticus
• A neurological deficit or abnormality on
examination
• + immediate family history
• Abnormality on CT/MRI or on the EEG
• High risk jobs or patient/family opinion
©2016 MFMER | slide-15Consider the Individual
• Seizure type and
epilepsy syndrome
• Age
• Gender
• Pregnancy potential
• Comorbidities
• Co-medications
• Lifestyle
Scheffer I, Epilepsy Currents 2011.
Chung, JAMA 2014 .
©2016 MFMER | slide-16The Elderly
• >60 is fastest growing segment of
population.
• Most have focal seizures.
• 3.3% in nursing homes on ASD1.
• More concurrent medical disorders2.
• Stroke, hepatic, renal disease
• Osteopenia/osteoporosis
• PHT is the most common ASD but
LEV, LTG, GBP are a better choice3.
1Garrad et al. Ann Neurol 2003;54:75-85.
2Ramsay RE, Rowan AJ, Pryor FM. Neurology 2004;9(suppl 5):S24-9.
3Rowan AJ et al. Neurology 2005;64:1868-1873.
©2016 MFMER | slide-17Women of Childbearing Potential
• Childbearing potential 9-51 years old
• Contraception
• Pregnancy
• Vitamin supplementation
• Precautions
Harden CL, Hopp J, Ting TY, et al. Practice parameter update: management issues for women with epilepsy:
focus on pregnancy (an evidence-based review): obstetrical complications and change in seizure frequency:
report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee
of the American Academy of Neurology and American Epilepsy Society. Neurology 2009;73:126-132.
Tomson et al. Epilepsia. 2015;56(7):1006-1019.
Folate 1-2 mg daily was recommended. ©2016 MFMER | slide-18What about ASDs and Pregnancy?
• Globally 15 million WWE are of child-bearing age.
• Uncontrolled GTC Sz can have devastating
consequences (> 5 associated with lower IQ).
• 10-fold increase of SUDEP in pregnancy.
• VPA impairs cognitive development
• 6 years post-partum
• Lower IQ (~ 10 IQ points)
• Dose-dependence > 800 mg/day
Baker GA et al. IQ after in utero exposure to AEDs: a controlled cohort study. Neurology 2015;84:382-390.
Meador KJ et al. NEAD Sutdy Group. A prospective observational study. Lancet Neurol 2013;12:244-252. N American Pregnancy
Adab N et al. The long term outcome of children born to mothers with epilepsy. JNNP 2004;75:1575-1583. Registry Fall 2014
Alternatives to VPA were recommended. ©2016 MFMER | slide-19Consider Co-morbidities
• Mental Health issues
• Select: LTG, VPA, OXC, PGB
• Avoid: PB, TPM, LEV, ZNS, PER
• Pain
• Select: GBP, PGB, TPM, CBZ
• Eating disorder: avoid drugs that impact weight
• Weight gain: VPA, GBP, PGB, CBZ, OXC, PER, EZO
• Weight loss: TPM, ZNS, FBM
• Hyponatremia (elderly, on diuretics)
• Avoid: CBZ, OXC, ESLI (CBZ derivatives)
• Cardiovascular risks (e.g. high cholesterol)
• Avoid: CBZ, PHT (P450 enzyme inducers)
©2016 MFMER | slide-20Eslicarbazepine acetate (Aptiom)
$650 for a 30-day supply of 400 mg brand name
Antiseizure Drugs Divalproex sodium (Depakote ER)
$165 for a 30-day supply of 500 mg brand name
$107 for 30-day supply of 500 mg generic
• The mainstay of epilepsy management Phenytoin (Dilantin)
$28 for a 30-day supply of 100 mg brand name
in >90% of patients. 1 $18 for 30-day supply of 100 mg generic
Perampanel (Fycompa)
$712 for a 30-day supply of 4 mg brand name
• Choices are based on seizure type and Levetiracetam (Keppra)
$435 for a 60-day supply of 500 mg brand name
epilepsy syndrome2 $158 for 60-day supply of 500 mg generic
Lamotrigine (Lamictal)
• Focal Epilepsy: Essentially all ASDs $310 for a 30-day supply of 100 mg brand name
$115 for 30-day supply of 100 mg generic
• Generalized Epilepsy: VPA, LTG, Pregabalin (Lyrica)
$153 for a 30-day supply of 75 mg brand name
TPM, LEV, ? LCS, ETH (absence) Gabapentin (Neurontin)
$109 for a 30-day supply of 300 mg brand name
$25.33 for 90-day supply of 300 mg generic
• Advantages of newer ASDs include Carbamazepine (Tegretol)
$117 for a 60-day supply of 200 mg brand name
tolerability and advantages of $19 for 60-day supply of 200 mg generic
conventional ASDs is cost.3 Topiramate (Topamax)
$506 for a 30-day supply of 100 mg brand name
1.Marson A et al. The Lancet 2007;369:1000-1026. $147 for 30-day supply of 100 mg generic
2.Tatum WO. Current Treatment Neurology 2013. Oxcarbazepine (Trileptal)
3.French JA, et al. Neurology. 2003;60:1631-1637. $193 for a 30-day supply of 300 mg brand name
$90 for 30-day supply of 300 mg generic
Zonisamide (Zonegran)
Levetiracetam is a great option in JME. $458 for a 60-day supply of 100 mg brand name
$120 for 60-day supply of 100 mg generic
©2016 MFMER | slide-21ASD Interactions
• Some ASDs (e.g. PHT, VPA) are highly protein bound and
interact increasing free unbound drug concentrations.
• Some ASDs (i.e. PHT) induce the P450 enzyme system
and increase the metabolism of lipid soluble drug
clearance. Therefore, dose increases of other drugs may
be required.
• e.g. contraception and anticoagulation compromised.
• Some ASDs (i.e. VPA) inhibit hepatic enzymes and reduce
metabolism of other ASDs/drugs and cause toxicity
requiring dose reductions.
• Some ASDs do both (e.g. TPM, ZNS)-variable effects.
Levetiracetam has no drug-drug interactions
©2016 MFMER | slide-22Consider Safety
• Steven-Johnson Syndrome: most of the ASDs
• Aplastic Anemia: carbamazepine, oxcarbazepine, felbamate
• Organ Failure (e.g. hepatic): valproate, felbamate
• Depression: phenobarbital, perampanel, leviteracetam,
zonisamide
topiramate, lacosamide
• Nephrolithiasis: topiramate, zonisamide
• Visual loss: vigabatrin, ezogabine
• Weight Loss: felbamate, topiramate, zonisamide
• Weight Gain: gabapentin, pregabalin, valproate,
carbamazepine, perampanel, vigabatrin
• Teratogenesis: all ASDs
©2016 MFMER | slide-23Sudden Unexpected Death in Epilepsy
• SUDEP is 24 times > the population
involving 1.1-3.8/1000 person years.
• Young people 20-40 years
• Males: females 7:4 VIDEO
• Substance abuse
• Epilepsy > 10 years
• GTC seizures
• Unattended/prone position
• MR/Symptomatic epilepsy (1/100)
http://www.epilepsyscotland.org.uk
©2016 MFMER | slide-24Drug-resistance: A Treatment Approach
Newly 1st 2nd 3rd Mono or
Diagnosed Monotherapy Monotherapy Polytherapy
No Video-EEG
Seizure freedom Monitoring
No Side effects Drug
ASDs (Polytherapy) Resistant
Neurostimulation Epilepsy
Seizure reduction
Ketogenic Diet Surgery
Minimize ASD side effect
(children)
Optimize quality of life
In: Wheless JW, Willmore LJ, Brumback RA, eds. Advanced Therapy in Epilepsy. Hamilton, Ontario:
BC Decker, Inc. 2008.
©2016 MFMER | slide-25Quality Indicators in Epilepsy
1. Seizure frequency & intervention noted each encounter.
2. Etiology, seizure type/syndrome noted each encounter.
3. Ask about side-effects to ASDs each visit.
4. Personalize safety issues/education yearly.
5. Screen for psychiatric health each visit.
6. Counsel women of childbearing yearly.
7. Refer drug-resistant patients to a CEC after 2 years.
Fountain NB et al. Quality Improvement in Neurology: Epilepsy Update Quality Measurement Set.
Neurology 2015;84(14):1483-1487.
©2016 MFMER | slide-26Conclusions
• The treatment approach to epilepsy requires a definitive
diagnosis and classification of seizure/epilepsy type.
• Management is individualized and a shift toward the new
ASDs has been based upon Pks and tolerability.
• Drug-resistance is a problem and VEM and non-medical
therapies should be considered a standard of care.
• The future promises better diagnosis and treatment for
patients with epilepsy though the PCP plays a primary role
for access to care.
©2016 MFMER | slide-27THE END
tatum.william@mayo.edu
©2016 MFMER | slide-28You can also read