Hematogenous osteomyelitis - A changing disease - Cleveland Clinic Journal of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hematogenous osteomyelitis
A changing disease
Martin C. McHenry, M.D. Despite the availability of potent antimicro-
bial drugs, improved diagnostic techniques, and
Department of Infectious Diseases
effective surgical procedures, hematogenous osteo-
Ralph J. Alfidi, M.D. myelitis continues to provide difficulties in diag-
nosis, complex problems in management, serious
Department of Radiology morbidity and even mortality. In recent years,
changes have occurred in the clinical setting,
Alan H. Wilde, M.D. presenting manifestations and the types of causa-
Department of Orthopaedic Surgery tive microorganisms. 1 - 2 Microorganisms that
rarely caused infection in the past have emerged
William A. Hawk, M.D. as significant bone pathogens. New clinical syn-
dromes, unusual locations of bone infection, and
Department of Pathology
additional pathogenetic mechanisms have been
documented. Although chronic osteomyelitis has
long been known to be a difficult lesion to pro-
duce in laboratory animals, recent experimental
models of chronic osteomyelitis that mimic hu-
man disease have been devised. 3-7 New informa-
tion is available concerning defects in host resist-
ance which may predispose to some forms of
osteomyelitis. Furthermore, knowledge of some of
the microbial factors related to virulence of cer-
tain bone pathogens is increasing. T h e purpose of
this report is to review briefly, in view of current
developments, selected aspects of the problem of
hematogenous osteomyelitis.
General considerations
Given the appropriate predisposing factors, os-
teomyelitis may develop in any bone of the body.
In the human skeleton, at least 206 bones develop
125
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.126 Cleveland Clinic Quarterly Vol. 42, No. 1
which vary in location, size, shape, bone, while much of the arch has the
structure, and function. In general, configuration of a flat bone. 8
bones are composed of a cortex of Although bone is the most solid of
compact (lamellar) bone and a me- the organs of the body, it is permeated
dulla of spongy or cancellous bone. with a system of channels that may
With respect to general architecture, provide a reservoir for pathogenic
Jaffe 8 has grouped bones into four microorganisms—lacunae, canaliculae,
categories: (1) tubular (long and Haversian or Volkmann's canals, and
short), (2) short (cuboidal), (3) flat, the medullary cavity.9"11
and (4) irregular. T h e tubular bones
include the humerus, radius, ulna, fe- Pathogenesis
mur, tibia, fibula (the long tubular Microorganisms may reach bone
bones), metacarpals, metatarsals and by one of three mechanisms: (1) direct
phalanges (short tubular bones). T h e inoculation secondary to trauma or
shaft of a tubular bone consists of a surgery, (2) contiguous spread from an
cortex of compact osseous tissue sur- adjacent soft-tissue infection, or (3)
rounding loosely meshed cancellous hematogenous spread from a distant
tissue of the bone marrow cavity; in focus of infection. We will confine our
the midportion of the shaft (di- remarks to the latter mechanism.
aphysis), the cortex is thickest and Collins 9 and Kahn and Pritzker 10
there is the least amount of cancellous have emphasized some special charac-
osseous tissue. T h e short (cuboidal) teristics of bone relevant to pyogenic
bones comprise the carpals, tarsals, bacterial infection. These include a
sesamoids, and certain anomalous relatively small volume of tissue space
bones. T h e bulk of the short bones is surrounded by a rigid wall favoring
composed of spongy osseous tissue, and the accumulation of exudate under
where they are not covered by articular increased tension; an anatomical ar-
cartilage they are enclosed only by a rangement of blood vessels that favors
thin cortical shell. T h e flat bones com- massive bone necrosis in association
prise the ribs, sternum, scapulae, and with increased tissue pressure; an in-
many of the bones of the skull. These adequate mechanism for resorption of
bones are thin in part or throughout, necrotic bone, which can lead to in-
are composed primarily of cortical complete healing and recurrent in-
bone, and contain relatively little fection; and the capacity for reactive
spongy bone. T h e irregular bones in- ossification which may take place
clude the innominate (ilium, ischium, readily in fibroblastic granulation tis-
pubis), the vertebrae, and some of the sue of walls of abscesses.
bones of the skull. These bones are
classified as irregular because they do Acute hematogenous osteomyelitis
not qualify for inclusion in the first Table 1 lists the site of bone in-
three categories. Some of the irregular volvement in 1,865 patients with acute
bones may have the characteristics of hematogenous osteomyelitis gathered
more than one of those in the first from several reports of studies con-
three categories. For example, the body ducted in the preantimicrobial, 12-14
of a vertebra resembles that of a short and in the antimicrobial era. 14-22 T h e
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 127
Table 1. Site of bone involvement in acute hematogenous osteomyelitis based on
review of studies conducted at various time periods12-22
Bones i n v o l v e d
Femur 207 ( 2 4 . 4 % ) 29 (29.3%) 323 ( 3 5 . 5 % )
Tibia 214 ( 2 5 . 3 % ) 28 (28.2%) 293 ( 3 2 . 2 % )
Humerus 76 ( 8 . 9 % ) 20 (20.2%) 95 ( 1 0 . 4 % )
Foot 61 ( 7 . 2 % ) 17 (17.1%) 52 ( 5 . 7 % )
Galcaneous 29 4 24
O t h e r tarsals 19 3 7
Metatarsals 13 6 6
Phalanges
Unspecified
Skull 59 (7%) 6 (6%) 3 (0.3%)
Mandible 18 2
Frontal 13 4
Maxilla 12
Temporal 5
Cranium 4 1
Nasal 2
Sphenoid 2
Malar 1
Basiooccipital 1
Parietooccipital 1
Occipital 1
Parietal 1
Pelvis 58 (6.9%) 11 ( 1 1 . 1 % ) 38 (4.2%)
Ilium 7 16
Ischium 2 8
Pubis 2 7
Unspecified 58 7
Fibula 51 (6%) 10 ( 1 0 . 1 % ) 61 (6.7%)
Radius 29 (3.4%) 5 (5%) 29 (3.2%)
Ulna 19 (2.2%) 9 (9.1%) 22 (2.4%)
Clavicle 11 (1.3%) 5 (5%) 8 (0.9%)
Rib 11 (1.3%) 6 (6.1%) 7 (0.8%)
Patella 6 4
Scapula 6 3 1
Metacarpal 6
Carpal 3
Sternum 1 2
Phalanx-hand 5 (5%) 1
Phalanges unspecified 31 (3.7%)
U n s p e c i f i e d bones 10 (1.1%)
Multiple bony involvement 45 (5.3%) 24 (24%) 45 (4.9%)
1
O f t h e 99 p a t i e n t s , in 57, o s t e o m y e l i t i s w a s d i a g n o s e d before 1939.
data are arbitrarily arranged into bial and antimicrobial era. Table 2
three time periods because one of the lists other data from these studies.
studies 14 overlapped the preantimicro- Acute hematogenous osteomyelitis is
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.128 Cleveland Clinic Quarterly Vol. 42, No. 1
Table 2. Selected features of acute hematogenous osteomyelitis based on review of
studies conducted at various time periods 12-22
T i m e of studies 1919-1937 1924-1954 1948-1968
N u m b e r of p a t i e n t s 846 99* 911
A g e of p a t i e n t s < 2 1 yr (75%) < 1 5 yr (100%) < 2 1 yr ( 8 1 - 1 0 0 % ) f
Male/female Î 584/262 58/41 503/253
Pathogens§
Staphylococcus aureus 4 1 8 / 5 6 0 (75%) 6 2 / 8 6 (72%) 5 6 7 / 6 7 2 (84%)
Streptococcus pyogenes 75/560 (13.4%) 18/86 ( 2 0 . 9 % ) 28/672 (4.2%)
Gram-negative bacilli 7/560 (1.3%) 3/86 (3.4%) 16/672 (2.4%)
Mortality 12%-25.4% 21.2% 1%
S o m e c o m p l i c a t i o n s (survivors)
R e l a p s e or c h r o n i c o s t e o m y e l i t i s 23%-46% 28.2% 20%
A d j a c e n t pyoarthrosis 18.7% 1% 5.7%
P a t h o l o g i c fracture 0.4% ?2% 1%
Amyloidosis 0.4%
* O f the 99 p a t i e n t s , in 57, o s t e o m y e l i t i s w a s d i a g n o s e d b e f o r e 1939.
t A g e s n o t r e p o r t e d in o n e study of 110 p a t i e n t s .
| S e x n o t r e p o r t e d in t w o s t u d i e s (155 p a t i e n t s ) .
§ B a s e d u p o n t h e n u m b e r of cases in w h i c h t h e i n f e c t i n g o r g a n i s m w a s d e t e r m i n e d .
caused most frequently by Staphylococ- phagocytes which may also favor de-
cus aureus or by Group A streptococci. velopment of infection in that re-
It occurs most frequently in long tu- gion. 26
bular bones, but no bone is exempt. Initially, the acute inflammatory
T h e majority of cases of acute hema- process behaves as a cellulitis of the
togenous osteomyelitis occur in chil- bone marrow; it may be amenable to
dren before the age of puberty; the appropriate antimicrobial chemother-
initial lesion is usually located in the apy and resolve with minimal or no
metaphyseal sinusoidal veins of the destruction of bone. When the infec-
red bone marrow of long bones. 9 ' 13' tion is uncontrolled, there is necrosis
23-25 T h e term metaphysis was first of marrow, osteocytes, and trabecular
used by Kocher to denote the broad bone. Abscesses form, and tiny seques-
cancellous end of the bone shaft which tra of necrotic trabeculae remain in a
is adjacent to the epiphyseal growth pool of purulent exudate. 9
plate. 26 Branches of the nutrient ar- Accumulation of exudate under
tery end in the metaphysis as narrow pressure results in spread of the infec-
capillaries, which turn back on them- tion in the medullary cavity and into
selves in acute loops at the growth the cortex through the Haversian and
plate, and enter a system of large Volkmann's canals. In infants less than
sinusoidal veins leading to the sinu- 1 year of age, nutrient metaphyseal
soids of the bone marrow. 23 ' 25 At this capillaries may still perforate the epi-
point, blood flow slows,25 presumably physeal growth plate; the infection
allowing bacterial emboli to settle and may spread to affect the epiphysis and
initiate the inflammatory process. T h e the adjacent joint. In children more
sinusoids of the metaphyseal bone mar- than 1 year of age, the epiphyseal cir-
row are said to have a paucity of culation is separated from the vascular
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 129
system of the metaphysis by an avas- direct involvement of the joint may de-
cular barrier, the epiphyseal growth velop from extension of the meta-
plate. 2 5 ' 2 6 T h e epiphyseal growth physeal infection through the peri-
plate acts as a barrier to spread of in- osteum without passage through the
fection, preventing epiphysitis and in- epiphyseal cartilage. 27
fection of the adjacent joint. 2 5 T h e Pyoarthrosis of an adjacent joint is
infection spreads laterally through the a relatively frequent complication of
cortical canals; this causes ischemia acute hematogenous osteomyelitis even
and focal necrosis of cortical bone in the antimicrobial era ( T a b l e 2). It
nourished by blood vessels in the Hav- most frequently involves the hip,
ersian a n d Volkmann canals. Subperi- shoulder, or knee; but other joints may
osteal infection follows escape of the be involved.
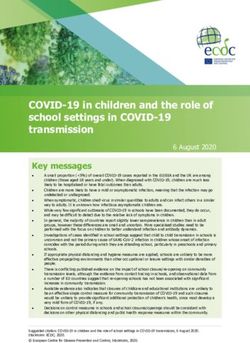
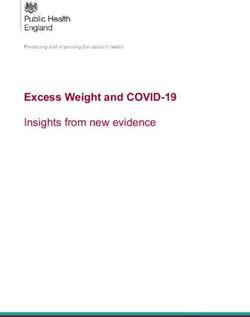
exudate t h r o u g h the cortex in the re- Figure 1 is a roentgenogram of the
gion of the metaphysis, probably be-
cause the cortical bone of the metaph-
ysis is t h i n n e r than that of the diaph-
ysis. 27 I n children, the periosteum
is loosely attached to bone and may
become elevated by subperiosteal ab-
scesses. This, in turn, may cause dis-
r u p t i o n of periosteal blood vessels that
supply the underlying cortical bone
and infarction of large portions of the
cortex, resulting in the formation of
very large bony sequestra. Eventually
these sequestra become separated from
viable bone and are surrounded by
p u r u l e n t exudate. If the patient sur-
vives, fibrous tissue a n d new bone
may be produced in the medullary
cavity a n d subperiosteal new bone (in-
volucrum) will be formed. 1 0
Bacteria invade the bony substance
of nearly all sequestra and remain
there as long as the sequestra per-
sist. 28 Sequestra serve as a potential
source for reinfection because they
have n o blood supply, a n d neither anti-
microbial drugs nor antibodies pene-
trate well into them. 1 0 ' 29
W h e n exudate perforates through Fig. I. R o e n t g e n o g r a m of t h e left f e m u r a n d
the periosteum, subcutaneous ab- t i b i a - f i b u l a of a 5-week-old i n f a n t , r e v e a l i n g
scesses a n d chronic draining sinuses de- soft tissue swelling a b o u t t h e knee, a r a d i o l u -
cent defect in t h e m e t a p h y s e a l region of t h e
velop. In joints such as the hip or
distal f e m u r , a n d periosteal elevation a n d new
shoulder, where the joint capsule sur- b o n e f o r m a t i o n on t h e l a t e r a l aspect of t h e
rounds a portion of the metaphysis, f e m u r a n d m e d i a l aspect of t h e tibia.
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.130 Cleveland Clinic Quarterly Vol. 42, No. 1
left femur and tibia-fibula of a 5-week- periosteal space. T h e periosteum may
old infant taken on the day of admis- rupture early with the formation of
sion for acute hematogenous osteomy- soft tissue abscesses. This rapid de-
elitis. This infant had evidence of os- compression prevents the vascular phe-
teomyelitis of the femur and tibia as nomena which are responsible for
well as infection of the knee joint. A bony infarction and sequestra forma-
hemolytic streptococcus was isolated tion in older infants and children.
from the knee joint. This patient il- Qureshi and Puri 3 5 reported the oc-
lustrated many of the unique features currence of hematogenous osteomye-
of neonatal hematogenous osteomye- litis in two infants after umbilical
litis. 27 , 30-32 Pyoarthrosis and multiple catheterization for exchange transfu-
bone involvement are more common sion and were unable to find similar
in hematogenous osteomyelitis in ne- cases reported in the literature. On
onates than in older infants and chil- the other hand, umbilical infection
dren. 25, 27 ' 30 Although the long tubu- has appeared to be an important pre-
lar bones are most frequently involved disposing factor to neonatal osteomy-
in neonates, 33 there is an increased in- elitis in some series,34 but not in oth-
cidence of involvement of membra- ers.30 Respiratory and cutaneous in-
nous bones such as the maxilla. 31 ' 32 fections have also been found to be
Systemic manifestations frequently are important predisposing factors in
minimal or absent despite multiple many cases. In some series, group A
bony involvement. T h e most common streptococci have been the most
presenting problem is swelling and frequent causative organisms, 27 ' 34
pain or loss of movement of an ex- whereas in others staphylococci pre-
tremity. If the epiphysis and joints dominate. 30 ' 32 ' 33
are not involved in the neonate and I n the preantimicrobial era, acute
bacteremia is controlled, prognosis for hematogenous osteomyelitis was un-
recovery without sequellae is unusu- common in adults. 24 When it occur-
ally good. Sequestra, chronic infection, red, it usually involved the vertebrae,
and draining sinuses rarely develop af- presumably because they are one of
ter hematogenous neonatal osteomye- the most active sites of hematopoiesis
litis. 27 ' 31 Although there is consider- in adults. 36 Acute hematogenous os-
able roentgenographic evidence of per- teomyelitis of long bones in adults ap-
iosteal reaction, infarction of the bony pears to be extremely rare, 38 ' 37 prob-
cortex does not occur. 25 ' 34 ably because the marrow cavities of
Certain anatomic factors appear to the limbs in adults are filled with ad-
contribute to the different nature of ipose tissue, with the exception of tiny
the disease in neonates. 27 T h e cancel- foci of red marrow in the extreme
lous spaces of the metaphysis are proximal portions of the humeri and
larger, the bone is of a more spongy femora. Zadek 37 and Wiley and Tru-
texture, the cortex is thinner, and the eta 36 reported a total of 22 cases of
periosteum is more loosely attached to acute hematogenous osteomyelitis in
bone of neonates than in older infants long bones of adults. Recently King
and children. 25 ' 27 This allows the in- and Mayo 38 described the findings in
fection to pass more easily from the six additional cases. T h e lesion usu-
medulla to the cortex and to the sub- ally begins around the nutrient artery
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 131
in the diaphysis of long bone. 38 T h e
pathologic changes are principally
periosteal and central. 37 W h e n the
infection is uncontrolled, the sup-
purative process spreads primarily
through marrow cavity. Because the
periosteum is more firmly adherent to
the adult bone, subperiosteal abscess
formation occurs less frequently than
in children; the large cortical seques-
tra of osteomyelitis in children do not
develop in the long bones of adults.
W h e n the infection progresses to the
end of the long bone of adults, neigh-
boring joints may become involved.
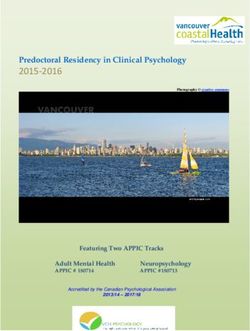
Figure 2 shows the excretory uro-
gram of a diabetic woman with a soli-
tary, mildly hydronephrotic kidney and
a functioning ureterosigmoidostomy. A
Charnley-Mueller prosthesis had been
inserted in the right hip because of
disabling osteoarthritis. Several days Fig. 2. Intravenous urogram revealing a soli-
postoperatively, a rectal tube was re- tary, mildly hydronephrotic kidney and a
functioning ureterosigmoidostomy; a Charn-
quired and severe rectal bleeding de-
ley-Mueller prosthesis is present in the right
veloped. T h i s was followed by bactere- hip.
mia due to Klebsiella type 32,
probably arising from infection of the Klebsiella. In each of the cases, the
urinary tract. T h i s in turn, was com- femur was involved. T h e association
plicated by Klebsiella type 32 infection of this type of hematogenous osteomy-
of the hip and femur, which pro- elitis with urologic procedures or pel-
gressed to involve the entire femur vic operations was emphasized. 39 Re-
and the right knee joint (despite ap- cently, Irvine et al 40 and Hall 4 1 have
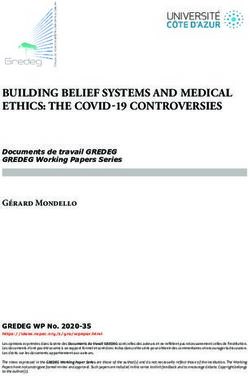
propriate therapy). Figure 3 shows the noted an association between geni-
lateral roentgenogram of the femur tourinary tract infections and deep in-
taken 24 days after the onset of bac- fections after total hip or knee re-
teremia and before pyoarthrosis of the placements. All of the serious infec-
knee was evident clinically. T h e r e was tions reported by those physicians
gas in the tissues of the thigh and evi- were caused by enteric gram-negative
dence of extensive osteomyelitis of the bacilli.
femur.
Since 1944, the incidence of acute
In 1966, Smith 3 9 reported a case of hematogenous osteomyelitis of chil-
acute hematogenous Klebsiella osteo- dren has been descreasing. 1 In some
myelitis of the femur in an adult; his medical centers, the relative propor-
search of the literature produced only tion of cases caused by S. aureus has
nine other reported cases of acute hem- diminished; 1 however, the staphylo-
atogenous osteomyelitis caused by cocci that cause disease have become
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.132 Cleveland Clinic Quarterly Vol. 42, No. 1
acute hematogenous osteomyelitis of
children has changed since the advent
of antibiotics. 1 , 2 ' 3 8 - 4 5 - 4 7 More severe
forms of the disease were observed in
the preantimicrobial era when the
mortality rate was as high as 25% ( T a -
ble 2). Severe shaking chills, fever, a n d
bone pain were characteristic; death
usually could be attributed to septi-
cemia and, in about two thirds of the
patients, occurred within 2 weeks of
the onset of the illness. 13 After 1944,
the mortality fell to 1% or less. Fur-
thermore, the f u l m i n a t i n g type of in-
fection is now rarely seen a n d the in-
cidence of acute systemic illness with
the disease has diminished. 1 ' 2 • 3 S - 4 5 - 4 7
T h e onset of the illness is more fre-
quently gradual and insidious, bone
lesions remain localized a n d may be
mistaken for benign or malignant tu-
mors or other conditions.
Before the introduction and use of
antimicrobial drugs, hematogenous os-
teomyelitis of the spine was considered
an u n c o m m o n condition. 1 3 I n the last
3 decades, the incidence appears to
have increased. 1 Hematogenous spinal
osteomyelitis is a disease primarily of
Fig. 3. L a t e r a l r o e n t g e n o g r a p h i c view of t h e adults; the majority of cases occur after
r i g h t f e m u r f r o m t h e s a m e p a t i e n t as in Figure
the third decade of life, when the
2, t a k e n 24 days a f t e r the onset of Klebsiella
type 32 b a c t e r e m i a . T h e r e is gas in soft tissues.
spine is completely formed. 4 8 Accord-
T h e b o n y cortex is t h i n n e d a n d e r o d e d a n d ing to Kulowski, 4 8 the predilection for
t h e r e a r e focal areas of periosteal r e a c t i o n . hematogenous osteomyelitis to involve
vertebrae of adults (in contrast to os-
increasingly resistant to antibiotics. 4 2 teomyelitic involvement of long tubu-
Gram-negative bacilli have been cited lar bones in children) may be at-
more frequently as being bone path- tributed in part to lack of true epiphy-
ogens. 1 - 43 In a recent study from Aus- seal growth of vertebrae, persistence of
tralia, 4 4 gram-negative bacilli ac- rich, cellular, red bone marrow, a n d
counted for 8% of cases of acute a sluggish voluminous blood supply.
hematogenous osteomyelitis, which is T h e latter condition might favor lo-
considerably higher than that re- calization of bacteria in the vertebral
corded in previous years ( T a b l e 2). body.
T h e r e are also indications that the Table 3 lists some of the pertinent
type of clinical illness associated with features of hematogenous osteomyelitis
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 133
Table 3. Nontuberculous hematogenous osteomyelitis of the spine of adults: selected
features based on review of reported cases36, 49-67
N u m b e r of p a t i e n t s 86
A g e r a n g e , yr 26-79 ( m e a n 5 8 . 6 yr, ± 1 1 . 3 S D )
Men/women 56/30
A n t e c e d e n t urinary tract or jjelvic i n f e c - 38 44.2%
tion
Pathogen*
Staphylococcus aureus 28/55 50.9%
Gram-negative bacilli 17/55 30.9%
Streptococci 4/55 7.3%
Mortality from infection 5/86 5.8%
Complications
Paralysis 7/86 8.1%
Temporary 5
Permanent 2
P a r a v e r t e b r a l abscess 6/86 6.9%
E p i d u r a l abscess or g r a n u l o m a 5/86 5.8%
R e t r o p h a r y n g e a l abscess 2/86 2.3%
Endocarditis 2/86 2.3%
Vertebra involved
Cervical 8
Thoracic 35
Thoracolumbar 2
Lumbar 35
Lumbosacral 7
> 1 interspace 9
* B a s e d u p o n t h e n u m b e r of cases in w h i c h a p a t h o g e n w a s isolated f r o m t h e i n v o l v e d b o n e or
b l o o d or b o t h .
of the spine in 86 adult cases gathered portant predisposing factors in more
from several reports in the litera- than 40% of the cases. Organisms
ture. 36 - 49-57 Data from other reports 1 ' may reach the spine directly through
48,58-ao w e r e not included because it the nutrient branches of the posterior
was not always possible to separate spinal artery during bacteremia 36 or
adult from childhood cases, to differ- by retrograde spread through the para-
entiate between cases caused by hema- vertebral venous plexus of Batson. Ac-
togenous spread from those produced cording to Wiley and Trueta, 3 6 the
by other mechanisms, or to tabulate all earliest lesion is in the body of the
the bones involved. vertebrae close to the anterior longi-
S. aureus, various enteric gram-nega- tudinal ligament. T h e lesion spreads
tive bacilli, and streptococci are most across the periphery of the interverte-
frequently responsible for hematoge- bral disc in a system of freely anasto-
nous spinal osteomyelitis in the adult mosing venous channels to involve the
(Table 3). Infections of the urinary body of the adjacent vertebrae. More
tract or pelvis, particularly those de- than one vertebral body is involved as
veloping after a surgical or instru- a rule, at least in the later stages of
mental procedure, appear to be im- the disease. Extension to the contigu-
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.134 Cleveland Clinic Quarterly Vol. 42, No. 1
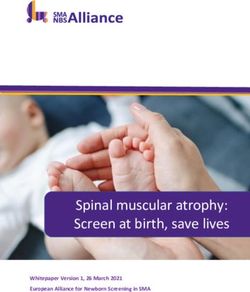
ous disc and vertebral body is abetted bacilli, and fungi. This can be accom-
by the absence of a circumferential plished either by percutaneous (Craig
cartilaginous plate and the lack of needle) biopsy under fluoroscopic con-
definite protective subchondral layer trol or by open surgical biopsy when
of compact bone. 48 Rapid progression this seems indicated. It is extremely
of the infection in the spongy verte- important to remember to obtain cul-
bral bone and in the intervertebral tures for acid-fast bacilli because it
disc may cause significant destruction may be difficult or impossible to dif-
of these structures. ferentiate tuberculous from pyogenic
T h e lumbar vertebrae are involved infection of the spine (Fig. 4 A, B).
most commonly by hematogenous os- Positive blood cultures usually es-
teomyelitis, followed in order of fre- tablish the cause of hematogenous ver-
quency by the thoracic and cervical tebral osteomyelitis, but rarely they
vertebrae. Extension of infection an- may be misleading. For example, dur-
teriorly to the spine occurred com- ing our study of gram-negative bacte-
monly in the preantibiotic era. 48 De- remia, 72 we treated a patient with re-
pending upon the location, anterior current urinary tract infection and
extension of infection may cause a Proteus mirabilis bacteremia at the
retropharyngeal abscess, mediastinitis time when signs, symptoms, and roent-
with pleural or pericardial involve- genographic changes of vertebral oste-
ment, subphrenic and retroperitoneal omyelitis and disc-space infection
abscess, or a psoas abscess. T h e tend- were evolving. Culture of the affected
ency of these abscesses to gravitate vertebral interspace yielded Mycobac-
or migrate is well known. terium tuberculosis rather than P. mi-
T h e infection may also extend pos- rabilis. Thus, whenever possible, cul-
teriorly and invade the spinal canal ture of the involved bone or interspace
causing an extradural abscess or gran- should be obtained.
uloma; this may lead to compression More recently, new pathogenic
of the spinal cord and paralysis. When mechanisms for acute hematogenous
the infection perforates the dura, men- osteomyelitis in adults have been de-
ingitis results. There were no exam- scribed. Since 1971, 59 cases of acute
ples of meningitis in the 86 cases in- hematogenous osteomyelitis have been
cluded in Table 3, but meningitis de- reported in adults who are addicted
veloped in four patients in Kulow- to or abuse drugs by taking them in-
ski's 48 series and in one patient in the travenously. 61-69 Pertinent clinical and
series of Waldvogel et al. 1 One of the microbiologic data from those 59 pa-
goals of antimicrobial chemotherapy tients are summarized in Table 4.
for vertebral osteomyelitis is to try to Most of the patients were heroin ad-
prevent extension of the process and dicts who took the drug intravenously.
associated complications. Each of the patients complained of
Because vertebral osteomyelitis may pain, but most were remarkably free
be produced by a wide variety of or- of systemic illness. Vertebrae and
ganisms, we routinely recommend ob- pelvic bones were most frequently
taining material from the involved affected, but a wide variety of other
bone or interspace for smears and cul- bones and joints were involved in some
tures for aerobes, anaerobes, acid-fast patients. Diagnosis frequently was
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 135
delayed a n d initially mistaken for
other conditions. Pseudomonas aerugi-
nosa a n d other gram-negative bacilli
were the pathogens in the majority of
cases. Of the 59 patients, only two had
endocarditis and there were no deaths
reported.
Leonard et al 7 0 reported the devel-
opment of acute hematogenous osteo-
myelitis in five patients receiving in-
termittent hemodialysis for chronic
renal failure. Of the five patients, in
four, repeated intravenous cannula in-
fections occurred and Staphylococcus
epidermidis and S. aureus were cul-
tured from the blood on different oc-
casions. T h e fifth patient h a d a sub-
cutaneous arteriovenous fistula a n d
the source of osteomyelitis was not de-
fined. Staphylococci were the most
common etiologic organisms, b u t P.
aeruginosa was the pathogen in one
patient. T h e thoracic spine and ribs
were the bones most commonly in-
volved, b u t the tibia, toes, and clavicle
were affected in some patients. O n e
patient had bacterial endocarditis. T h e
overall mortality was 60%.
In 1974, we treated a patient with
Fig. 4A, B. P o s t e r o a n t e r i o r a n d lateral r o e n t -
chronic renal failure (who was being
g e n o g r a m s of t h e t h o r a c o l u m b a r region
maintained on intermittent hemo- s h o w i n g evidence of d e s t r u c t i o n of large p o r -
dialysis) for an infected subcutaneous tions of t h e bodies of t h e first a n d second l u m -
arteriovenous fistula and bacteremia bar v e r t e b r a e a n d collapse of t h e i n t e r v e r t e -
caused by S. aureus. Bacteremia was b r a l disk space. Mycobacterium tuberculosis
was c u l t u r e d f r o m specimens o b t a i n e d by aspi-
eradicated promptly and appropriate
r a t i o n biopsy of the affected area. T h e p a t i e n t
antimicrobial therapy was adminis- recovered a f t e r a l o n g course of a n t i t u b e r c u -
tered for a n extended period of time. lous t h e r a p y .
Figures 5 to 7 are roentgenograms of
the thoracic spine taken 50, 63, and 83 tic levels of vancomycin had been
days after the day of staphylococcal present in the blood for several weeks.
bacteremia. Needle biopsy and aspira- Because of the patient's cachectic state
tion of the interspace between the 11th and hopeless prognosis, surgery to re-
and 12th thoracic vertebrae was per- lieve the spinal cord compression was
formed on the 74th day after the day not u n d e r t a k e n a n d hemodialysis was
of bacteremia; the culture yielded 5. discontinued at the request of his fam-
aureus, despite the fact that therapeu- ily. T h e patient died from his under-
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.136 Cleveland Clinic Quarterly Vol. 42, No. 1
Table 4. Selected features of acute hematogenous osteomyelitis in drug addicts or
abusers based on review of reported cases (1971-1974) 61 " 69 *
N u m b e r of p a t i e n t s 59
Age 18-50 yr ( m e a n 33 yr ± 8 . 9 S D )
Sex M a n / w o m a n = 50/9
Pathogen (s)f
Pseudomonas aeruginosa 47
Pseudomonas aeruginosa a n d o t h e r p a t h o g e n ( s ) | 3
K l e b s i e l l a ( 3 ) — E n t e r o b a c t e r (1) 4
Pseudomonas sp 2
Candida stellatoidea 1
Candida guillermondi 1
Staphylococcus aureus 1
Bone and joints involved
Vertebra 40
Cervical 7
Thoracic 2
Lumbar 22
Lumbosacral 8
Nonspecified 1
Sacroiliac
Symphysis pubis
Radial styloid
Sternoclavicular
Ischium
Humerus
Rib(s)
Hip
Femur
Clavicle
Scapula
Knee
Shoulder
Acromioclavicular
Costochondrals
Pain 59/59
S y s t e m i c illness 5/59§
Endocarditis 2/59
Mortality reported 0
* H e r o i n a d d i c t s (57) or abusers (2); p e n t a z o c i n e a n d m e t h a l p h e n i d a t e h y d r o c h l o r i d e (1); all
p a t i e n t s took drugs i n t r a v e n o u s l y .
t D i a g n o s i s w a s e s t a b l i s h e d by c u l t u r e of the b o n y lesion, i n t e r s p a c e , or joint in 57 p a t i e n t s
a n d b y b l o o d c u l t u r e a l o n e in 2 patients.
t K l e b s i e l l a (1), Staphylococcus aureus (1), Enterobacter cloacae and Streptococcus fecalis (1).
§ F e v e r , chills, a n d o t h e r s y m p t o m s or signs of a c u t e i n f e c t i o n w e r e a b s e n t in m o s t cases.
lying renal disease. At autopsy, there Baker et al 7 1 reported the develop-
was n o evidence of endocarditis. Fig- ment of acute hematogenous osteomy-
ure 8 is a photomicrograph of a his- elitis in three adults with severe neu-
tologic section of the skeletal infection tropenia and were unable to find re-
obtained at autopsy. ports of similar cases in the literature.
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 137
tients with Salmonella septicemia. 73 ' 74
T h e risk for hematogenous Salmo-
nella osteomyelitis in patients with
sickle cell disease a n d related hemo-
globinopathies is several h u n d r e d
times that seen in the normal popula-
tion. 7 4 - 7 8 T h i s complication occurs
primarily in infants a n d young chil-
Fig. 6. L a t e r a l r o e n t g e n o g r a m of t h e involved
thoracic region t a k e n 63 days a f t e r t h e d a y of
b a c t e r e m i a . T h i s shows f u r t h e r progression of
t h e disease w i t h o b l i t e r a t i o n of t h e i n t e r s p a c e .
Figs. 5A, B. P o s t e r o a n t e r i o r a n d lateral to-
m o g r a m s s h o w i n g decrease in vertical h e i g h t
of t h e 11th t h o r a c i c v e r t e b r a , n a r r o w i n g of
t h e s u b j a c e n t v e r t e b r a l interspace, a n d loss of
t h e n o r m a l a r c h i t e c t u r e of t h e v e r t e b r a l e n d
plates of t h e 11th a n d 12th thoracic v e r t e b r a e .
( T o m o g r a m s t a k e n 50 days a f t e r t h e d a y of
staphylococcal b a c t e r e m i a ) .
Recently, d u r i n g a study of gram-neg-
ative bacteremia, 7 2 members of our
group treated an adult patient with
neutropenic leukemia for hematoge-
nous pyoarthrosis of the hip and oste- Fig. 7. T h o r a c i c m y e l o g r a m w i t h p a t i e n t in
omyelitis of the femur due t o £ . coli. the h e a d - d o w n position s h o w i n g m a r k e d ex-
t r a d u r a l constriction b e h i n d t h e T 1 1 - T 1 2
H e m a t o g e n o u s osteomyelitis in sickle disk space. (Myelogram was d o n e 83 days a f t e r
cell disease a n d related anemias t h e d a y of staphylococcal b a c t e r e m i a . Staphy-
lococcus aureus was isolated f r o m t h e involved
Salmonella osteomyelitis is uncom- s p i n a l i n t e r s p a c e o n t h e 74th day a f t e r t h e on-
mon, occurring in less than 1 % of pa- set of bacteremia.)
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.138 Cleveland Clinic Quarterly Vol. 42, No. 1
Fig. 8. T h i s p h o t o m i c r o g r a p h was p r e p a r e d f r o m t h e T l l - 1 2 lesion d e m o n s t r a t e d in Fig-
ure 7. T h e process a p p e a r s to be in a subsidiary p h a s e a n d f o r m e d largely of g r a n u l a t i o n tissue
c o n t a i n i n g f r a g m e n t s of necrotic b o n e a n d m o d e s t n u m b e r s of i n f l a m m a t o r y cells. At a u t o p s y ,
t h e r e was c o n s i d e r a b l e d e s t r u c t i o n of interspace tissues w i t h e n c r o a c h m e n t o n t h e s p i n a l c o r d
by t h e process (hematoxylin-eosin, XlO).
dren, but cases in adults have been re- cell crisis. Eventually the diagnosis
ported. 7 8 may become apparent, particularly in
T h e infection begins in the medulla those patients who have persistent
of the diaphysis of long and short tu- fever, continued leukocytosis, and
bular bones. 7 6 ' 7 7 Multiple bony in- roentgenographic changes that are far
volvement is common. T h e phalanges more severe than those secondary to
of the hands a n d feet may become in- bone marrow thromboses in sickle cell
volved 7 8 producing an illness resem- disease. 7 4 , 7 7 According to Engh et al, 77
bling the "hancl-foot" syndrome of the most f r e q u e n t distinguishing
sickle cell disease. 78 T h e clinical and roentgenographic findings are longi-
roentgenographic features of Salmo- tudinal intracortical diaphyseal fissur-
nella osteomyelitis may be very diffi- ing, overabundant involucrum forma-
cult or impossible to differentiate from tion, and involvement of multiple and
those of a sickle cell crisis, especially often symmetrical diaphyseal sites.
in the earliest stages of the illness; T h e linear structures in the cortical
therefore, blood cultures should be ob- diaphysis have been termed "cortical
tained from all patients with sickle Assuring," b u t probably represent a
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 139
layer of purulent exudate beneath the Staphylococci and other gram-positive
involucrum and between it and the cocci have caused hematogenous oste-
dead bone. 74 omyelitis less frequently in patients
T h e pathogenesis of hematogenous with sickle cell disease than in other
Salmonella osteomyelitis is a complex children, 74 and the reasons for this are
phenomenon and may be related to not clear.
several factors. Salmonella organisms Studies of antibacterial host factors
are widely present in the environ- in patients with sickle cell disease
ment, 80 providing ample opportunity failed to reveal immunoglobulin defi-
for exposure and colonization of the ciencies, and the response to Salmo-
intestinal tract with or without pro- nella vaccine in those patients was the
ducing overt illness. Some strains of same as that in normal controls. 89 Par-
Salmonella have the capacity per se to adoxically, although pneumococcal os-
cross the intestinal mucosal barrier teomyelitis is quite rare in patients
and gain access to the systemic circu- with sickle cell anemia, 90 a wide vari-
lation. 81 ' 82 However, injuries to the ety of abnormalities have been deter-
intestinal mucosa from localized mined which may help to explain the
thrombosis in sickle-hemoglobinopa- significantly increased incidence of se-
thies and impairment of the hepatic rious pneumococcal infections in pa-
reticuloendothelial system may facili- tients with sickle cell anemia. These
tate invasion of the bloodstream by include functional asplenia, 91 im-
those organisms. 73 Hemolytic crises of paired antibody response to intrave-
sickle cell disease and related hemo- nous immunization, 92 a defect in se-
globinopathies may decrease the abil- rum opsonizing activity against the
ity of macrophages of the spleen and pneumococcus, 93 and an abnormality
other sites to phagocytize circulating in the alternate pathway of comple-
bacteria because of engorgement of ment activation. 94 T h e apparent rar-
reticuloendothial cells with hemolyzed ity of pneumococcal osteomyelitis in
erythrocytes. 83 Bone marrow throm- patients with sickle cell disease may
boses and infarction that occur in be due to the frequent, rapidly lethal
sickle cell crises may favor localization nature of pneumococcal infections in
of circulating bacteria in bone. In- patients with this hemoglobinopa-
creased concentrations of bilirubin or thy. 90
other breakdown products of erythro-
cytes in the bone marrow may provide Osteomyelitis in chronic granuloma-
an environment favorable to Salmo- tous disease of childhood
nella organisms. 77 - 84
Of 28 patients with chronic gran-
Shigella and certain strains of E. ulomatous disease of childhood re-
coli may also invade the intestinal ported by Wolfson et al, 95 eight pa-
mucosal barrier 8 1 and occasionally tients had evidence of osteomyelitis
cause bacteremia. 8 5 ' 8 6 In patients with involving 19 bones. Some of these le-
sickle cell disease, hematogenous oste- sions may have been the result of hem-
omyelitis has been produced by E. atogenous spread of infection and oth-
coli,85 Shigella sonnet,86 Serratia mar- ers from contiguous spread of an ad-
cescens,81 and Arizona hinshawii.88 jacent focus of soft tissue infection;
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.140 Cleveland Clinic Quarterly Vol. 42, No. 1
the authors did not specify. Members of the onset of the illness. 16 When the
of the family Enterobacteriaceae, S. patient presents with a typical history
aureus, and Aspergillus fumigatus were of chills, fever, pain in one site in a
the offending organisms. These orga- limb, and localized tenderness to pal-
nisms produce catalase, are phagocy- pation, a provisional diagnosis can be
tized normally by the patient's poly- made and therapy started after ap-
morphonuclear leukocytes, but they propriate pretreatment cultures are
survive and persist within the abnor- obtained. Detection of localized ten-
mal phagocytes. Osteomyelitis in the derness is the most significant early
patients with chronic granulomatous clinical finding and indicates that the
disease was manifested by granuloma- periosteum has been involved. 14 When
tous inflammation and did not present therapy is started more than 3 days af-
with pain, fever, or local signs of in- ter the onset of the illness, persistence
flammation. T h e most frequent sites of infection, sequestra formation, and
of involvement were the metatarsals, chronic osteomyelitis is much more
tarsals, and metacarpals; but the tibia, likely. It is somewhat discouraging to
fibula, humerus, femur, ribs, and tho- note that approximately 20% of pa-
racic vertebrae were involved in some tients with acute hematogenous osteo-
patients. Roentgenographic changes myelitis in the antibiotic era have
in some small bones (increased breadth relapses or progress to chronic osteo-
and lack of acute destruction) simu- myelitis (Table 2). T h e roentgeno-
lated tuberculous dactylitis. In other graphic changes of chronic osteomye-
small bones, there was marked destruc- litis are shown in Figures 9 to 12. Al-
tion and widening concomitantly. Ab- though the changes were observed on
scesses and sequestra rarely occurred. the roentgenograms of a patient in
Long-term antimicrobial therapy with- whom osteomyelitis developed after
out surgical intervention usually was internal fixation of a comminuted frac-
all that was required for cure. Of the ture, the changes are illustrative of se-
eight patients, a surgical procedure vere chronic osteomyelitis: sequestra-
was required for cure in two. tion in a radiolucent cavity, periosteal
elevation with extensive subperiosteal
Diagnostic considerations new bone formation.
One of the major problems in es- Patients who have hematogenous os-
tablishing an early diagnosis of acute teomyelitis in certain locations may
hematogenous osteomyelitis is that present unusual diagnostic difficulties.
roentgenographic examination is nor- For example, patients with osteomye-
mal in the early stages of the disease. litis of the pelvis may be misdiagnosed
Bone changes may be demonstrated as having acute appendicitis on the
earlier in acute osteomyelitis by right, paracolic abscess on the left,
means of radioisotope scanning than pyelonephritis, arthritis of the hip,
by conventional roentgenography, 6 3 ' 6 5 pelvic tumor, sciatica, or other con-
and should be used when indicated. ditions. 96 Some patients with hema-
Available data indicate that persist- togenous osteomyelitis of the ilium
ence of infection, sequestra formation, have had a normal appendix removed
and chronic osteomyelitis rarely de- because of a mistake in diagnosis. 97
velop when appropriate antimicrobial Hematogenous osteomyelitis of the
therapy is initiated within 3 days metatarsal sesamoids may masquerade
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 141
osseous infection are essential for op-
timal therapy. In patients with chronic
d r a i n i n g sinuses, care must be taken
to avoid contamination of specimens
with members of the normal body
flora. After cleansing the surrounding
skin with isopropyl alcohol, material
should be obtained for culture by aspi-
ration or with a swab u n d e r aseptic
technique. Whenever possible, necro-
tic or infected tissue from the depth of
the w o u n d should be obtained. O f t e n
this can be best accomplished at the
time of surgery. T h e material should
be placed in a suitable container and
transported to the laboratory with an
j| - » j H
- /4 mm •
II
Fig. 9. R o e n t g e n o g r a m of t h e left f e m u r , Oc-
t o b e r 27, 1969, s h o w i n g m a r k e d periosteal re-
action, f o u r r a d i o o p a q u e sequestra a n d a ra-
d i o l u c e n t a r e a of cortical d e s t r u c t i o n l a t e r a l
to t h e largest of t h e sequestra.
u n d e r the guise of cellulitis, trauma, or
gout. 9 8 Hematogenous sternal osteo-
myelitis may present as a mass lesion
with the differential diagnosis includ-
ing perforating aneurysm, tuberculo-
sis, carcinoma, and mediastinal ab-
scess.99 Osteomyelitis of a rib may be
mistaken for bone tumor, particularly
Ewing's sarcoma. 1 0 0
Microbiologic considerations
Since hematogenous osteomyelitis
Fig. 10. S i n o g r a m of t h e left f e m u r on Octo-
may be produced by a wide variety of ber 27, 1969. T h e c o n t r a s t m a t e r i a l o u t l i n e s
pathogens, adequate pretreatment cul- the lateral and central sequestrum and par-
tures of blood a n d accessible sites of tially o u t l i n e s t h e large m e d i a l s e q u e s t r u m .
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.142 Cleveland Clinic Quarterly Vol. 42, No. 1
chronic osteomyelitis, L-form vari-
ants 1 0 7 or protoplasts 1 0 8 have been re-
covered from lesions using special hy-
pertonic media.
In recent years, anaerobic bacteria
have received increased attention as
being causes of bone infection. 1 0 1 - 1 0 3
It is of interest in this regard, that be-
fore 1920, T a y l o r and Davies 28 regu-
larly cultured anaerobic bacteria from
sequestra of patients with chronic os-
teomyelitis secondary to trauma. An-
aerobic bacteria frequently participate
in mixed infections with other orga-
nisms and usually occur in cases of os-
Fig. 11. S i n o g r a m o n N o v e m b e r 4, 1969, a f t e r
s e q u e s t r e c t o m y , s h o w i n g c o n t r a s t m a t e r i a l in
t h e surgical space.
informative requisition without delay.
Special techniques are required for
isolation of anaerobes 1 0 1 and other
fastidious organisms. Gram-stained
smears of exudates, abscesses, or in-
fected tissues should always be ob-
tained simultaneously with the cul-
tures. T h e y may be extremely helpful
in evaluating the results of cultures. 1 0 2
W h e n routine aerobic cultures of
bone are sterile in cases of osteomye-
litis, anaerobic bacteria, 101 - 103 acid-
fast bacilli, 104 - 105 actinomyces, fungi,
Fig. 12. R o e n t g e n o g r a m of t h e f e m u r t a k e n
or other unusual pathogens 1 0 6 should
in t h e h e a l i n g phases of t h e c h r o n i c osteomye-
be considered. In cases of recurrent or litis.
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 143
certainty in this case whether Bacte-
roides osteomyelitis resulted directly
from trauma or from hematogenous
spread from a focus of infection in the
abdomen.
Fig. 13. R o e n t g e n o g r a m of r i g h t f e m u r a n d
u p p e r t i b i a - f i b u l a , s h o w i n g c o m p o u n d frac-
t u r e of distal f e m u r a n d gas in soft tissues.
T h e r o e n t g e n o g r a m was t a k e n b e f o r e t h e on-
set of Bacteroides fragilis b a c t e r e m i a w h i c h
lasted 24 days.
teomyelitis resulting from trauma or
spread of contiguous soft tissue infec-
tion. 101 - 103
However, cases of hematogenous os-
teomyelitis d u e to anaerobic bacteria
have been reported. Figures 13 to 15
are roentgenograms of the femur from
a patient with osteomyelitis due to
Bacteroides fragilis. T h i s patient had
abdominal a n d skeletal trauma, ab-
dominal infection, and B. fragilis bac-
Fig. 14. R o e n t g e n o g r a m t a k e n later in clinical
teremia that persisted for 24 days de-
course shows area of cortical d e s t r u c t i o n a n d
spite parenteral clindamycin therapy. periosteal reaction in t h e d i a p h y s i s of f e m u r
It was not possible to determine with laterally a n d medially.
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.144 Cleveland Clinic Quarterly Vol. 42, No. 1
the infected joint space yielded the
same organisms.
Hematogenous osteomyelitis has re-
sulted rarely from smallpox 1 1 2 and
BCG vaccination. 113 - 114 Hematoge-
nous skeletal tuberculosis does not oc-
cur as frequently as in the past, but
still causes significant diagnostic and
therapeutic problems. 104
Microbial determinants
T h e properties of microorganisms
which determine their ability to cause
disease of bone are not well defined.
Some of the properties of gram-nega-
tive bacilli relevant to their pathoge-
nicity have been reviewed elsewhere 115 '
116
and will not be repeated here. W e
will confine ourselves to some brief
remarks about the Staphylococcus,
since it is still the organism most com-
monly responsible for hematogenous
osteomyelitis.
Recent studies indicate that a muco-
peptide of the cell wall of virulent
Fig. 15. R o e n t g e n o g r a m of t h e f e m u r on J u n e
4, 1974, s h o w i n g f u r t h e r evidence of osteomye-
litis.
W i t h the increased use of prolonged
intravenous therapy and immunosup-
pressive drugs, unusual organisms such
as fungi 1 0 9 ' 110 or atypical acid-fast
bacilli 111 may cause hematogenous os-
teomyelitis. Figure 16 is the roent-
genogram of a patient with hematoge-
nous osteomyelitis of the phalanx.
T h i s patient was receiving therapy for Fig. 16. R o e n t g e n o g r a m s of t h e r i g h t m i d d l e
Hodgkin's disease when pulmonary in- finger of a p a t i e n t w i t h H o d g k i n ' s disease.
filtrates and pain and swelling of the T h e y show soft tissue swelling, periosteal re-
finger developed. Material aspirated a c t i o n , a n d erosion of t h e b o n y cortex of t h e
m i d d l e p h a l a n x w i t h n a r r o w i n g of t h e j o i n t
directly from the lung yielded Myco-
space. M a t e r i a l a s p i r a t e d f r o m t h e i n f e c t e d
bacterium kansasii and Cryptococcus j o i n t space yielded Mycobacterium kansasii
neoformans. Material aspirated from a n d Cryptococcus neoformans.
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 145
strains of S. aureus inhibits chemotaxis predominantly to phage groups I and
of polymorphonuclear leukocytes, sup- II; most were lipase-positive and all
presses inflammatory edema formation, produced protein A. They suggested
and enables the bacteria to produce that a possible host-parasite interac-
more severe lesions presumably as a tion takes place in the bone marrow in
result of their unbridled multiplica- which lipids and staphylococcal lipases
tion in the early stages of established may play a role analogous to that sug-
infection. 117 Another constituent of gested for furunculosis.
the cell wall of S. aureus, protein A,
reacts with the Fc fragment of normal Therapeutic considerations
and immune IgG immunoglobulin. 118 Patients with acute hematogenous
T h e main opsonic site of the immu- osteomyelitis should be on bed rest
noglobulin G is located on the Fc with immobilization of the affected
region. 1 1 9 ' 1 2 0 Evidence suggests that part. Appropriate antimicrobial ther-
protein A of staphylococci inhibits apy alone may be sufficient to cure
phagocytosis by competing with poly- this infection if treatment is started
morphonuclear leukocytes for the Fc within 72 hours after the onset of the
sites.119 Thus, it is possible that pro- disease.15 Whenever possible, a Gram-
tein A may enhance survival of stained smear of an aspirate from the
staphylococci in tissues and may be affected area should be used as a guide
another virulence factor, along with to initial therapy. When this is not
leukocidins, hemolysins, coagulase, possible, initial therapy must be based
and penicillinase. 119 It also has been upon an educated guess as to what is
shown that a considerable number of the most likely etiologic organism.
staphylococci isolated from human Knowledge of the age of the patient,
sources are capable of producing cap- the location of the infection, the pres-
sules which may enhance their viru- ence of underlying predisposing dis-
lence. 120 It is known that extracellular eases and circumstances involved in
staphylococcal toxins may cause capil- development of the infection may per-
lary vasospasm with thrombosis, 121 mit an educated guess as to the etio-
which might contribute to the develop- logic organism. For example, in an
ment of the acute lesion in staphylo- otherwise healthy child with a history
of a recent furuncle and a presumptive
coccal osteomyelitis.
clinical diagnosis of acute hematoge-
An attribute of osteomyelitis caused
nous osteomyelitis of the distal femur,
by S. aureus is its tendency to recur,
parenteral antistaphylococcal therapy
often at some time remote from the
with therapeutic doses of a penicil-
initial episode. 11 ' 13 Cases are on rec-
linase-resistant penicillin should be
ord in which recurrences occurred af-
administered after appropriate pre-
ter quiescent periods of 40 to 70
treatment cultures are obtained (pro-
years. 11 ' 13 T h e ability of staphylococci
vided there is no history of penicillin
to persist in bone remains unex-
allergy). Definitive antimicrobial
plained. Recently, Hedstrom and chemotherapy depends upon the
Kronvall 122 showed that strains of identity of the pathogen, its in vitro
staphylococci responsible for chronic susceptibility and the patient's ability
hematogenous osteomyelitis belonged
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.146 Cleveland Clinic Quarterly Vol. 42, No. 1
Table 5. Currently preferred antimicrobial drugs for initial presumptive therapy of
acute hematogenous osteomyelitis*
Suspected etiologic organism Currently preferred drugs f
Staphylococcus aureus 1) O x a c i l l i n , m e t h i c i l l i n , or n a f c i l l i n
2) A c e p h a l o s p o r i n
3) V a n c o m y c i n
4) Clindamycin
Streptococcus pyogenes 1) Penicillin G
2) A cephalosporin
3) Erythromycin
4) Clindamycin
Salmonellae 1) Chloramphenicol
2) Ampicillin
3) Trimethoprim-sulfamethoxazole
Pseudomonas aeruginosa 1) Carbenicillint and gentamicin§
E. coli, K l e b s i e l l a - E n t e r o b a c t e r , Proteus, Ser- 1) Gentamicin
ratia
Bacteroides 1) C l i n d a m y c i n
2) C h l o r a m p h e n i c o l
* D e f i n i t i v e a n t i m i c r o b i a l therapy is d e t e r m i n e d s u b s e q u e n t l y f r o m the results of in v i t r o suscep-
tibility tests a n d the p a t i e n t ' s response to t r e a t m e n t . I n i t i a l therapy of a c u t e h e m a t o g e n o u s
o s t e o m y e l i t i s is a d m i n i s t e r e d b y the p a r e n t e r a l r o u t e .
f N u m e r a l 1 represents t h e d r u g ( s ) of first c h o i c e , n u m e r a l s after 1 represent a l t e r n a t i v e drugs
that m a y be used when circumstances indicate.
Î S h o u l d n o t b e u s e d in p e n i c i l l i n - a l l e r g i c p a t i e n t s .
§ T o b r a m y c i n , a m i k a c i n , or sisomicin are i n v e s t i g a t i o n a l a m i n o g l y c o s i d e antibiotics t h a t m a y b e
effective a g a i n s t g e n t a m i c i n - r e s i s t a n t strains of Pseudomonas aeruginosa.
to tolerate the drug. Table 5 lists some technique in the operating room, an
of the preferred antimicrobial drugs incision of the skin is made over the
for initial presumptive therapy of area of maximum tenderness. T h e
acute hematogenous osteomyelitis for periosteum is incised in order to drain
various suspected pathogens. We be- the subperiosteal abscess. In some in-
lieve that antimicrobial therapy stances, it may be necessary to drill
should be administered for at least 4 one or more small holes in the bony
to 6 weeks in cases of uncomplicated cortex to decompress the medullary
acute hematogenous osteomyelitis. cavity, allowing an abscess to drain
When the patient with acute hema- and prevent infarction of the bony
togenous osteomyelitis does not re- cortex. We now prefer to close the
spond to treatment within 48 to 72 operative wound to prevent secondary
hours (lysis of fever, decreased pain, infection. Suction drainage tubes are
increased appetite and sense of well- utilized for a short period of time.
being, sterile blood cultures), surgery When hematogenous osteomyelitis
becomes mandatory. When the roent- in the neck of the femur is strongly
genogram and bone scan reveal no suspected, arthrotomy for decompres-
diagnostic changes, the surgeon has to sion and for culture is mandatory. T h e
rely on his judgment as to the probable neck of the femur lies within the syno-
location of the lesion. Under aseptic vial capsule of the hip joint. A sub-
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.Spring 1975 Hematogenous osteomyelitis 147
periosteal abscess in that region may is of little consequence. However, oc-
r u p t u r e into the joint causing septic casionally it may give rise to serious
arthritis. This can be complicated by gram-negative bacillary infection. Fig-
necrosis of the head of the femur and ures 17 and 18 are roentgenograms of
dislocation of the hip—a disaster for the hip region of a patient who re-
a young child. quired suction-irrigation after removal
T h e therapy of chronic hematoge- of an infected total hip prosthesis
nous osteomyelitis is a complex sub- (staphylococcal pyoarthrosis). The
ject and will be considered only postoperative hip wound became con-
briefly. Bed rest, immobilization of the taminated with gram-negative bacilli,
affected part, and administration of leading to recurrent episodes of gram-
specific antimicrobial chemotherapeu- negative bacteremia. Fortunately, with
tic agents are extremely important. appropriate surgical and medical man-
However, because of the nature of the agement, the patient survived. It is our
lesion itself, surgical procedures are policy to utilize the suction-irrigation
mandatory in order to accomplish the apparatus for less than 10 days when-
following: excise sinus tracts down to ever possible, and to obtain cultures of
the involved bone, culture and biopsy the effluent solutions at frequent in-
the infected bone, remove all seques- tervals.
tra, drain abscesses, and debride all in- Recently, Hedstrom 1 2 7 showed that
fected granulation tissue and bone if prolonged antibiotic treatment of
feasible. T h e surgeon attempts to re- chronic staphylococcal osteomyelitis
move all ischemic bone and soft tissue for at least 6 months, significantly
leaving a well-vascularized wound lowered the frequency of recurrences
bed. 123-125 Other more complicated during the first year after the end of
measures such as insertion of autoge- treatment than did shorter courses of
nous bone grafts and application of
split thickness skin grafts may be re-
quired in some patients.
Under ideal conditions, postopera-
tive treatment of patients with chronic
osteomyelitis with the closed suction-
irrigation technique serves to elimi-
nate dead space by allowing healthy
granulation tissue to obliterate the
cavity occasioned by the infection
and the surgical procedure. 1 2 6 This
has been responsible for improved re-
sults of surgical therapy of chronic os-
teomyelitis. 124 ' 126 However, optimal
use of the suction-irrigation apparatus
requires meticulous nursing care to
maintain continuous flow and to
avoid contamination of the system.
Even with the best technique, con- Fig. 17. F i l m t a k e n f o l l o w i n g r e m o v a l of in-
fected C h a r n l e y - M u e l l e r prosthesis, s h o w i n g
tamination may occur, but usually it
s u c t i o n - i r r i g a t i o n t u b e a n d gas in soft tissues.
Downloaded from www.ccjm.org on October 9, 2021. For personal use only. All other uses
require permission.You can also read