PodiatryToday - AMERICAN COLLEGE OF FOOT AND ANKLE Highlights from the 2018 Scientific Conference of the - Podiatry Today
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Periodicals Supplement to June 2018
PodiatryToday
Highlights from the 2018
Scientific Conference of the
AMERICAN
COLLEGE OF
FOOT AND ANKLE
SURGEONS
| Pre-Fellowship Instructional Course
We bring efficiency to your hospital, without compromise to your patient.
Novastep proudly salutes the following group of distinguished young surgeons and pays
tribute to the prestigious Fellowship programs they are soon to enter. We also celebrate
their completion of the industry’s only Pre-Fellowship Instructional Course, offered exclusively
by Novastep. We wish them continued success, inspiration and achievement during their
Fellowship engagements and throughout their careers.
Ugo Adigweme, DPM Emily Anzmann, DPM Dustin Constant, DPM
Orthopedic Center of Florida Broadlawns Medical Center Coordinated Health
Fort Myers, FL Des Moines, IA Bethlehem, PA
Jordan Ernst, DPM Ajay Ghai, DPM Colin Graney, DPM
Paley Orthopedic Ankle & Foot Care Centers Florida Orthopedic
and Spine Institute Youngstown, OH Foot & Ankle Center
West Palm Beach, FL Sarasota, FL
Matt Johnson, DPM Chris Juels, DPM Michael Kelly, DPM
UT Southwestern The CORE Institute Pediatric & Adult Foot & Ankle
Dallas, TX Phoenix, AZ Surgical Fellowship
Atlanta, GA
Sara E. Lewis, DPM Timothy P. McConn, DPM Timothy Miller, DPM
Southeast Permanente Weil Foot and Ankle Institute Foot & Ankle
Atlanta, GA Chicago, IL Specialists of Ohio
Mentor, OH
Amber Morra, DPM Joseph Park, DPM Daniel Peterson, DPM
University Hospitals Southeast Permanente North Jersey Reconstructive
Chardon, OH Atlanta, GA Foot & Ankle Fellowship
Lyndhurst, NJ
Andrew Pierre, DPM Nathan Shane, DPM Eric So, DPM Mark Wavrunek, DPM
Foot & Ankle Specialists Weil Foot and Ankle Institute The CORE American Health Network
of Central Ohio Chicago, IL Institute Indianapolis, IN
Newark, OH Phoenix, AZ
Lowell Weil, Jr., Christopher Hyer,
DPM, FACFAS DPM, FACFAS
CEO, Weil Foot & Ankle Institute Director, OFAC Fellowship
Co-Chairman, Pre-Fellowship Co-Chairman, Pre-Fellowship
Instructional Course Instructional Course
Hammertoe Implants | Nitinol Compression Clips | Screw Systems | Plating Systems
External Fixation Systems | Biologics | Single-Use Instrument Kits | Medical Education Programs
To learn more please call 877.287.0795 or visit
TM
Trademarks and Registered marks of Novastep, Inc. 2018 Novastep Inc. All Rights Reserved
TABLE OF
CONTENTS
4
TACKLING TREATMENT
CONTROVERSIES
IN THE FOREFOOT
In a discussion of forefoot conditions,
these ACFAS speakers debated effective
treatments for Grade 2 and 3 hallux rigidus,
hallux valgus and instability under the second
metatarsophalangeal joint.
8 18
EVALUATING AND A CLOSER LOOK AT
TREATING STAGES OF TREATMENT OPTIONS
POSTERIOR TIBIAL FOR HALLUX RIGIDUS
TENDON DYSFUNCTION Can arthrodesis, cheilectomy and amnion
Exploring current concepts in treating tissue have an impact for hallux rigidus?
posterior tibial tendon dysfunction, several These ACFAS speakers explored the
panelists detailed protocols for Stages II research and shared insights from their
and IV flatfoot, and discussed pertinent experience on treatments to relieve
considerations in choosing between double pain and improve function in the first
arthrodesis and triple arthrodesis. metatarsophalangeal joint.
12 24
ESSENTIAL INSIGHTS
ON MANAGING ACHILLES CURRENT PRINCIPLES
TENDON RUPTURES AND INSIGHTS ON HALLUX
Given the challenges of treating Achilles VALGUS PROCEDURES
tendon ruptures and the potential for In a session on the range of options
re-rupture, these panelists at ACFAS shared for bunion surgery, panelists at ACFAS
their thoughts as well as the literature discussed frontal plane rotation, debated
findings on chronic Achilles ruptures, minimally invasive versus open surgery and
insertional tendinopathy and how to reviewed literature findings on the utility of
prevent complications. the Lapidus and Akin procedures.
Post-ACFAS Supplement
Tackling Treatment Controversies
In The Forefoot
In a discussion of forefoot conditions, these ACFAS speakers debated effective treatments for Grade 2 and 3 hallux
rigidus, hallux valgus and instability under the second metatarsophalangeal joint.
By Brian McCurdy, Managing Editor
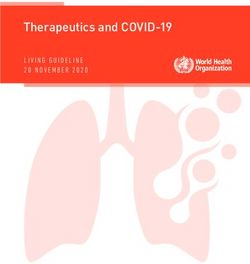
C heilectomy is highly success-
ful in early stage hallux rigidus,
notes Kyle Fiala, DPM, FACFAS.
He says the technique is simple, effective
and has minimal complications.
In a review of 38 patients, Erdil and
coworkers noted that although arthrode-
sis is reliable, implant arthroplasty can be
an effective alternative for patients with
advanced hallux rigidus.8 Dr. Rubin says
In a study of 110 patients, Dr. Fiala O’Doherty compared arthrodesis with a
notes Coughlin and Shurnas successful- Keller arthroplasty, finding that arthrod-
Photo courtesy of Doug Richie, DPM
ly used cheilectomy for patients with esis had no advantages and six of 50 toes
Grades 1 and 2 hallux rigidus as well as that had arthrodesis needed revision.9
selected Grade 3 patients.1 The authors In contrast, Jordan Grossman, DPM,
recommend arthrodesis for patients with FACFAS, argues that history shows that
Grade 4 or Grade 3 hallux rigidus with first MPJ replacements do not work in
less than 50 percent of the metatarsal the long term. Relevant issues for Dr.
head cartilage remaining at the time of Grossman in procedure selection include
surgery. Nicolosi and coworkers con- pain relief, functional results, patient sat-
cluded that cheilectomy is a successful isfaction, complications, revision surgery
alternative to first metatarsophalangeal and cost.
joint (MPJ) arthrodesis in the long term, This foot has Grade 2 hallux rigidus. Comparing hemiarthroplasty to ar-
citing good results during a mean fol- Cheilectomy is highly successful in early throdesis, Raikin and colleagues found
low-up of seven years.2 stage hallux rigidus, notes Kyle Fiala, DPM, that arthrodesis was more predictable
Although cheilectomy has support in FACFAS. He says the technique is simple, at relieving the pain of severe first MPJ
the literature and a low complication effective and has minimal complications. osteoarthritis at a mean follow-up of 79
rate, Matthew Williams, DPM, FACFAS, months.10 Dr. Grossman notes no pa-
says the procedure does not change the notes Laurence Rubin, DPM, FACFAS. tients with arthrodesis needed revision
structure of the foot or alter the deform- In a study of 79 patients with Grade 3 and arthrodesis patients had a higher sat-
ing forces of hallux rigidus. hallux rigidus, Papagelopoulos and col- isfaction rate than those who had hemi-
Citing complications, Dr. Williams leagues cited 82 percent implant survival arthroplasty.
notes Roukis recommended only per- at 10 years for patients age 57 or younger In regard to patient satisfaction, Do-
forming isolated periarticular first meta- in comparison to 90 percent in patients negan and Blume studied first MPJ fu-
tarsal osteotomies for hallux rigidus with 57 and older.5 Lawrence and Thuen also sion with the use of dual-crossed screws
caution or not performing the procedure noted that implant arthroplasty is more in 228 patients.11 Dr. Grossman says 91
at all.3 Dr. Williams adds that Cullen and effective in older patients with less de- percent of patients would have the sur-
colleagues, in a study of 423 procedures, mand, citing high patient satisfaction in gery again and 88 percent reported hav-
noted that cheilectomy had a higher re- a study of 70 first MPJ implants in 54 ing little or no pain.
visional surgery rate over a five-year fol- patients with hallux rigidus.6 Gibson and Thomson, in a study of 63
low-up than decompression osteotomy.4 In a review of 3,049 first MPJ im- patients with unilateral or bilateral first
plant arthroplasties, Cook and coworkers MPJ arthritis, noted those who had ar-
Debating First MPJ Arthrodesis found an 85.7 percent post-op satisfac- throdesis had fewer complications and
Versus Implant Arthroplasty tion rate with first MPJ implants, a num- better function than those who had ar-
For Grade 3 Hallux Rigidus ber the authors adjusted to 94.5 percent throplasty, according to Dr. Grossman.12
Age can be an important factor influ- when considering only the highest qual- When it comes to revision rates, Stone
encing the survival of first MPJ implants, ity studies.7 and colleagues contacted 52 patients
4
RY
RGE
L T O
CAL DULE A
S U
6 6 37A.com
.
602fo@i2b
E -US
SCH
. OW In
84AI4
L S
U N
EM
In2Bones
A G LO BA L E X T R E M I T Y CO M PA N Y
UNIQUE, SEE-THROUGH PLATING
Colink View ®
X-rayand
MTP Transparent Hubavailable
Lapidus plates
Dynamic, Mechanical Compression
Generated by Transverse Lag Screw
Across Fusion Site
• X-ray Transparent PEEK Hub to View Fusion Site
• Low Profile • Anatomic Design • Type II Anodized
• Plates and Screws OR Ready, Delivered Nested in Sterile Tubes
To See Our Full Line Visit Our Site at www.i2b-USA.com
CoLink, In2Bones and the In2Bones logo are registered trademarks of In2Bones and its subsidiaries. | In2Bones USA Memphis, TN, 38119 USA • In2Bones SAS, 69130 Ecully, FRANCE • © 2018
In2Bones USA, Memphis, TN - All rights reserved • PATENT PENDING FAS0518-A, 0418
Post-ACFAS Supplement
from the Gibson and Thomson study for
a 15-year follow-up.12,13 Dr. Grossman
says one patient with arthrodesis required
revision in comparison to nine revisions
in the arthroplasty group.
Brodsky and coworkers found all 23
hallux rigidus patients who had arthrod-
esis achieved radiographic union and
clinical improvement in walking and ac-
tivity, notes Dr. Grossman.14
Dr. Grossman cites poor Grade C ev-
idence in favor of arthroplasty to treat
hallux rigidus effectively and notes fair
Grade B evidence in favor of arthrodesis.
Photo courtesy of Doug Richie, DPM
Should You Perform A First
Metatarsal Osteotomy
Or A Lapidus Bunionectomy
For Hallux Valgus?
Noting there are over 130 options to
treat hallux valgus, Shane Hollawell,
DPM, FACFAS, says one can often use
proximal and distal osteotomies, or a
combination of proximal and distal oste-
otomies, in lieu of a Lapidus procedure.
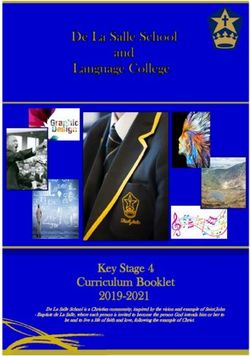
Ravenell and coworkers examined This radiograph shows a foot with Grade 3 hallux rigidus. Coughlin and Shurnas
radiographs from 61 patients who had recommend performing arthrodesis for patients with Grade 4 or Grade 3 hallux
received a Lapidus procedure, Austin rigidus with less than 50 percent of the metatarsal head cartilage remaining at
bunionectomy or first MPJ fusion.15 All the time of surgery.
patients reviewed had first intermeta-
tarsal angles greater than 15 degrees and
hallux abductus angles greater than 25 more of an influence on load sharing or digitorum longus transfer as it can
degrees. Noting no significant difference distribution than a chevron osteotomy.18 both stabilize the second MPJ and
in the amounts of correction for any of Lagaay and coworkers cited a reop- address the underlying pathology.21
the three procedures, the authors sug- eration rate of 2.92 percent for recur- In their study of 68 patients who re-
gested that one could use an Austin bun- ring hallux valgus following a modified ceived treatment for plantar plate tears,
ionectomy or first MPJ fusion to correct Lapidus arthrodesis and a 0.29 per- Nery and coworkers utilized the follow-
the large intermetatarsal and hallux ab- cent reoperation rate for hallux varus.19 ing grading system:
ductus angles that many surgeons treat The authors noted that revision rates • patients with grade 0 and grade I tears had
with a Lapidus procedure. were similar for the Lapidus bunio- thermal shrinkage with radiofrequency;
Dr. Hollawell cites a retrospective study nectomy, closing base wedge osteot- • patients with grade II and III tears had
of 38 patients by Stienstra and colleagues omy and chevron-Austin osteotomy. direct plantar plate reinsertion; and
noting that surgeons can perform distal Early weightbearing is another advan- • patients with grade IV tears had flex-
chevron osteotomies to correct metatarsus tage of the Lapidus procedure with King or-to-extensor tendon transfer.22
primus varus of more than 15 degrees.16 and colleagues citing post-op weight- The authors noted those in groups I, III
In contrast, Sandeep Patel, DPM, bearing at a mean of 34 days with 133 of and IV had less stable MPJs after surgery
FACFAS, cites the efficacy of the Lapidus 136 patients achieving union.20 and less toe purchase and ground touch.
arthrodesis for hallux valgus. Donegan and Caminear found that if
Dr. Patel says Avino and colleagues Treatment Insights the plantar plate is attenuated or does not
found that the Lapidus bunionectomy On Sub-Second MPJ Instability have residual tissue, one can use imbri-
had an influence on the medial longitu- When treating instability under the cation with the flexor digitorum longus
dinal arch in 35 patients.17 The Lapidus second MPJ, Thomas Chang, DPM, sheath.23 Dr. Chang also cites a study not-
procedure also has positive effects on FACFAS, says plantar plate repair is ef- ing that combining plantar plate repair and
plantar forefoot pressures. Dr. Patel cites a fective. He notes one study that con- hammertoe repair with a flexor digitorum
68-patient study by King and colleagues, cluded primary repair of the plantar longus tendon transfer can address chronic
who found the Lapidus procedure has plate provides an alternative to flex- sagittal plane instability of the lesser MPJs.24
6
Podiatry Today | June 2018
The literature supports flexor tendon joint arthrodesis using dual crossed screw fixa-
tion. J Foot Ankle Surg. 2017;56(2):291-297.
transfer for second MPJ instability, argues
12. Gibson JN, Thomson CE. Arthrodesis or total
Photo courtesy of Neal Blitz, DPM
Lawrence Ford, DPM, FACFAS. As he replacement arthroplasty for hallux rigidus:
says, plantar plate insufficiency leads to a randomized controlled trial. Foot Ankle Int.
a loss of the reverse windlass mechanism 2005;26(9):680-90.
so there is no passive toe purchase and 13. Stone OD, Ray R, Thomson CE, Gibson JN.
Long-term follow-up of arthrodesis vs total
the flexor tendon transfer technique uses
joint arthroplasty for hallux rigidus. Foot Ankle
dynamic transfer to address the reverse Int. 2017; 38(4):375–80.
windlass mechanism. 14. Brodsky JW, Baum BS, Pollo FE, Mehta H.
Dr. Ford notes surgeons can combine Prospective gait analysis in patients with first
a flexor tendon transfer with a proximal metatarsophalangeal joint arthrodesis for hallux
rigidus. Foot Ankle Int. 2007; 28(2):162–5.
interphalangeal joint fusion for a rigid
15. Ravenell RA, Camasta CA, Powell DR. The
hammertoe. He says one can use a Gir- Here is a post-op view after a Lapidus unreliability of the intermetatarsal angle in
dlestone-Taylor procedure for flexible, bunionectomy. Sandeep Patel, DPM, choosing a hallux abducto valgus surgical proce-
mild deformity. Complications of the FACFAS, says Avino and colleagues found dure. J Foot Ankle Surg. 2011;50(3):287-92.
flexor tendon transfer include stiffness that the Lapidus bunionectomy had an 16. Stienstra JJ, Lee JA, Nakadate DT. Large dis-
influence on the medial longitudinal arch placement distal chevron osteotomy for the cor-
and sausage toe, according to Dr. Ford.
in 35 patients. rection of hallux valgus deformity. J Foot Ankle
Surg. 2002;41(4):213-20.
When Patients Have Metatarsus 17. Avino A, Patel S, Hamilton GA, Ford LA. The
Adductus And Hallux Valgus References effect of the Lapidus arthrodesis on the medial
Clinically, patients with metatarsus ad- 1. Coughlin MJ, Shurnas PS. Hallux rigidus. Grad- longitudinal arch: a radiographic review. J Foot
ing and long-term results of operative treatment. Ankle Surg. 2008;47(6):510-4.
ductus present with a C-shaped footprint,
J Bone Joint Surg Am. 2003;85-A(11):2072-88. 18. King CM, Hamilton GA, Ford LA. Effects of
hallux valgus or varus and a skewed foot, 2. Nicolosi N, Hehemann C, Connors J, Boike the Lapidus arthrodesis and chevron bunionec-
notes Jason Naldo, DPM, FACFAS. He A. Long-term follow-up of the cheilecto- tomy on plantar forefoot pressures. J Foot Ankle
says there are significantly higher peak my for degenerative joint disease of the first Surg. 2014;53(4):415-9.
plantar pressures in patients with metatar- metatarsophalangeal joint. J Foot Ankle Surg. 19. Lagaay PM, Hamilton GA, Ford LA, et al. Rates
2015;54(6):1010-20. of revision surgery using Chevron-Austin
sus adductus than in patients without the
3. Roukis TS. Clinical outcomes after isolated osteotomy, Lapidus arthrodesis, and closing base
deformity. Dr. Naldo says patients with periarticular osteotomies of the first metatarsal wedge osteotomy for correction of hallux valgus
hallux valgus can have metatarsus adduc- for hallux rigidus: a systematic review. J Foot deformity. J Foot Ankle Surg. 2008;47(4):267-72.
tus, adding that forefoot adduction can Ankle Surg. 2010;49(6):553-60. 20. King CM, Richey J, Patel S, Collman DR.
lead to compensation in the hindfoot. 4. Cullen B, Stern AL, Weinraub G. Rate of Modified Lapidus arthrodesis with crossed screw
revision after cheilectomy versus decompression fixation: early weightbearing in 136 patients. J
For metatarsus adductus, Troy Boffeli,
osteotomy in early-stage hallux rigidus. J Foot Foot Ankle Surg. 2015;54(1):69-75.
DPM, FACFAS, notes procedure selection Ankle Surg. 2017;56(3):586-588. 21. Ford LA, Collins KB, Christensen JC. Stabiliza-
criteria include the severity of the defor- 5. Papagelopoulos PJ, Kitaoka HB, Ilstrup DM. tion of the subluxed second metatarsophalangeal
mity, multiple joint arthritis, bone spur Survivorship analysis of implant arthroplasty for joint: flexor tendon transfer versus primary
with neuritis and lesser toe deformity. He the first metatarsophalangeal joint. Clin Orthop repair of the plantar plate. J Foot Ankle Surg.
Relat Res. 1994;(302):164-72. 1998;37(3):217-22.
notes an underlying metatarsus adductus
6. Lawrence BR, Thuen E. A retrospective review 22. Nery C, Coughlin MJ, Baumfeld D, et al.
can have an effect on hallux valgus surgery. of the primus first MTP joint double-stemmed Prospective evaluation of protocol for surgical
The complexity of metatarsus adduc- silicone implant. Foot Ankle Spec. 2013;6(2):94- treatment of lesser MTP joint plantar plate tears.
tus can make the assessment of hallux 100. Foot Ankle Int. 2014;35(9):876-85.
valgus difficult, according to Dr. Naldo. 7. Cook E, Cook J, Rosenblum B, et al. Meta-anal- 23. Donegan RJ, Caminear D. Anatomic repair
ysis of first metatarsophalangeal joint implant ar- of plantar plate with flexor tendon sheath
Citing a retrospective study by Aiyer and
throplasty. J Foot Ankle Surg. 2009;48(2):180-90. reinforcement: case series. Foot Ankle Spec.
colleagues of 587 patients with metatar- 8. Erdil M, Elmadag NM, Polat G, et al. Compar- 2016;9(5):438-43.
sus adductus, Drs. Boffeli and Naldo not- ison of arthrodesis, resurfacing hemiarthroplasty, 24. Bouché RT, Heit EJ. Combined plantar plate
ed the authors found a 30 percent rate of and total joint replacement in the treatment and hammertoe repair with flexor digitorum
radiographic recurrence of hallux valgus of advanced hallux rigidus. J Foot Ankle Surg. longus tendon transfer for chronic, severe sagit-
2013;52(5):588-93. tal plane instability of the lesser metatarsopha-
after bunion surgery.25 The authors note
9. O’Doherty DP, Lowrie IG, Magnussen PA, langeal joints: preliminary observations. J Foot
that metatarsus adductus raises the risk Gregg PJ. The management of the painful first Ankle Surg. 2008;47(2):125-37.
of hallux valgus deformity recurrence. metatarsophalangeal joint in the older patient. 25. Aiyer A, Shub J, Shariff R, et al. Radiographic
However, Dr. Boffeli cites a study by Arthrodesis or Keller’s arthroplasty? J Bone Joint recurrence of deformity after hallux valgus sur-
Shibuya and coworkers noting that af- Surg Br. 1990;72(5):839-42. gery in patients with metatarsus adductus. Foot
10. Raikin SM, Ahmad J, Pour AE, Abidi N. Com- Ankle Int. 2016;37(2):165-71.
ter adjusting for covariates, there was no
parison of arthrodesis and metallic hemiarthro- 26. Shibuya N, Jupiter DC, Plemmons BS, et
connection between underlying metatar- plasty of the hallux metatarsophalangeal joint. J al. Correction of hallux valgus deformity in
sus adductus and the outcome of bunion Bone Joint Surg Am. 2007;89(9):1979-85. association with underlying metatarsus adductus
surgery.26 n 11. Donegan RJ, Blume PA. Functional results and deformity. Foot Ankle Spec. 2017;10(6):538-542.
patient satisfaction of first metatarsophalangeal
7
Post-ACFAS Supplement
Evaluating And Treating Stages
Of Posterior Tibial Tendon Dysfunction
Exploring current concepts in treating posterior tibial tendon dysfunction, several panelists detailed protocols for Stages II
and IV flatfoot, and discussed pertinent considerations in choosing between double arthrodesis and triple arthrodesis.
By Brian McCurdy, Managing Editor
W hen classifying posterior
tibial tendon dysfunction,
Lawrence Ford, DPM, FAC-
FAS, cites the system devised by Johnson
and Strom and added to by Myerson.1,2
As he notes, Stage I involves inflamma-
tion of the tendon but no deformity. Dr.
Ford says Stage II is controversial because
these patients have varying levels of de-
Photo courtesy of Jason Miller, DPM
formation and symptoms with a vari-
ety of options for reconstruction. Stage Jason Miller, DPM, FACFAS, cites several studies noting a high accuracy for magnetic
III involves a rigid flatfoot deformity resonance imaging (MRI). Here is a longitudinal MRI of distal posterior tibial tendon
while Stage IV suggests incompetence with rupture and retraction of the tendon (EOT denotes end of tendon). To the left
of the deep deltoid ligament resulting of the tendon is some fluid/hemorrhage in the collapsed tendon sheath.
in ankle valgus, according to Dr. Ford.
In a patient with a normal gait, Dr. Ford What is the imaging gold standard for and less expensive alternative to MRI for
notes there is inverted heel contact and evaluating abnormalities in the patient detecting posterior tibial tendon tears.15,16
lateral forefoot loading, followed by first suffering from soft tissue insufficiency as- In a study of 22 ankles in 18 patients with
ray loading, which provides a rigid lever sociated with posterior tibial tenon dys- posterior tibial tendon dysfunction, Nal-
for propulsion. He says posterior tibial function and unstable pes planovalgus? lamshetty and colleagues demonstrated
tendon dysfunction is associated with pes Jason Miller, DPM, FACFAS, cites several that imaging with ultrasound was concor-
planovalgus deformity with compromise studies that note a high accuracy for mag- dant with MRI in a majority of patients.17
of the incompetent medial soft tissue re- netic resonance imaging (MRI). As he
straints. He says the gastrocnemius-soleus points out, numerous authors have doc- A Guide To Surgical Decision
complex is a deforming force. umented the benefits of MRI for pre-op Making For Stage II Flatfoot
An age old debate is whether to fix the planning for ankle tendon reconstructive Stage IIA (early) flatfoot hallmarks in-
lateral or medial column or both, notes surgery as well as as quantifying the true clude medial symptoms, mild deformi-
Dr. Ford. In the lateral column, he notes etiology and extent of rupture.3–8 ty, equinus and a low talonavicular-first
lengthening is powerful in all three planes However, Dr. Miller also cites several metatarsal angle, notes Christopher
but there can be issues if the patient has recent studies investigating the efficacy Reeves, DPM, FACFAS. He says charac-
a raised calcaneal pitch or metatarsus ad- of ultrasonography as an alternative diag- teristics of patients with Stage IIB (late)
ductus. He notes that addressing the me- nostic tool for pathology of the posteri- flatfoot include lateral and postural symp-
dial column makes sense if there is insta- or tibial tendon.9–14 As Dr. Miller notes, toms, subfibular pain, progressive defor-
bility of the medial column, hallux valgus the superficial location of the posterior mity, equinus, and a moderate to high
or other first ray deficiencies. Dr. Ford tibial tendon makes it well suited for talonavicular-first metatarsal angle.
notes the medial column is underrated imaging by high-resolution ultrasound. There is no one best way to fix Stage
in flatfoot mechanisms. As he says, if the He says the development of linear ar- II posterior tibial tendon dysfunction
medial column is unstable, hypermobile, ray high-frequency transducers can help and the profession must eliminate “dog-
elevated, short or essentially not acting as produce high-resolution images that can matism,” asserts Dr. Reeves. He suggests
a buttress to prevent further overprona- display inner tendon structure. Dr. Miller undertaking a well-rounded, critical as-
tion, then the foot will collapse. says ultrasound offers a more convenient sessment of each patient as well as pre-
8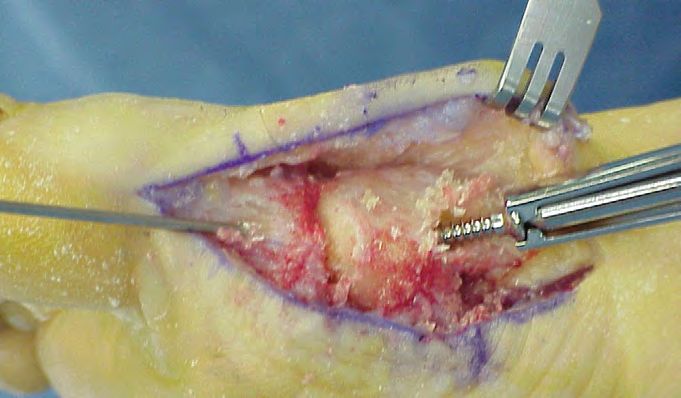
Podiatry Today | June 2018
Photo courtesy of Jason Miller, DPM
Here one can see axial (image A) and longitudinal (image B) sonographic images of the
right posterior tibial tendon at the level of distal tibia, demonstrating a linear hypoechoic
partial tear (arrows). Image C is an axial fast spin-echo, fat-suppressed T2-weighted MRI
(6000/72) of the right posterior tibial tendon showing partial disruption of the fibers of
the tendon near its insertion, which is indicated by foci of fluid signal intensity (arrow).
operatively assessing the potential pitfalls options in the face of arthrosis include ament with grafts harvested from the an-
of surgery. As he notes, joint-sparing os- Evans osteotomies, subtalar joint fusion, terior tibial tendon.20 Jeng and colleagues
teotomy is the “workhorse” for Stage II medial soft tissue reconstruction and gas- noted success with minimally invasive
flatfoot. One can combine an osteotomy troc recession. deltoid ligament reconstruction together
with selective arthrodesis and soft tissue Is body mass index (BMI) a factor in de- with a triple arthrodesis.21
reconstruction for deformity correction cision making for flatfoot? Dr. Reeves cites
and pain relief, notes Dr. Reeves. a study of 633 patients who had forefoot Considering The Medial Double
Dr. Reeves’ treatment algorithm for surgery, noting that obesity did not lead to Versus The Triple Arthrodesis
Stage II posterior tibial tendon dysfunc- more frequent post-op complications.18 The triple arthrodesis is indicated for
tion in younger patients includes Evans flatfoot patients with pain, instability and
osteotomies, medial calcaneal displace- Key Insights On Treating progressive deformity, notes Allen Jacobs,
ment osteotomies, medial soft tissue re- Stage IV Posterior Tibial DPM, FACFAS. However, he points
construction and gastrocnemius recession Tendon Dysfunction out the triple arthrodesis can lead to
with or without a Cotton osteotomy. Patients with Stage IV posterior tibial wound healing complications and calca-
Comorbidities are likely to dictate surgi- tendon dysfunction will present with an- neocuboid joint reduction and nonunion
cal options and he says these include di- kle and foot pain, poor gait and no heel can be problematic. He also says the pro-
abetes, neuropathy, age, and preoperative raise, according to Benjamin Clair, DPM, cedure requires a long operative time, has
arthrosis. He notes hindfoot fusion is an FACFAS. Radiographs will indicate an prolonged healing time and there can be
option for patients with comorbidities, increased talar tilt and he suggests always adjacent joint arthritis, a stiff gait and an-
large angular deformities or neuropathy. taking weightbearing views of the foot and gle valgus. Dr. Jacobs notes that some pa-
A gastrocnemius recession aids in the ankle. Non-operative treatments for Stage tients can progress to ankle arthrosis.
reduction of flatfoot deformity, notes Dr. IV include ankle foot orthotics (AFOs) to In a study of 32 patients with poste-
Reeves. He says a medial displacement control talar tilt while Dr. Clair notes sur- rior tibial tendon dysfunction, Galli and
calcaneal osteotomy corrects hindfoot gical options include ankle fusion, tibio- colleagues noted that a medial double
valgus and removes the deforming force talocalcaneal fusion or a pantalar fusion. arthrodesis increased the volume of the
of the Achilles. He notes one can achieve Dr. Clair notes those with Stage IV-A calcaneocuboid joint by 62 percent.22
pain relief through techniques including should have joint sparing treatment with Dr. Jacobs cites data by Catanzariti and
posterior tibial tendon debridement/exci- the goal of preserving ankle motion. He Adeleke, who prefer a double arthrode-
sion and flexor digitorum longus transfer. emphasizes realigning the forefoot first, sis of the talonavicular joint and subtalar
Patients with arthrosis in the face of noting that one should also identify ankle joint using a single medial approach for
a flexible and reducible deformity pre- varus and valgus instability. severe transverse plane deformity.23 The
operatively are at risk for loss of correc- As far as deltoid ligament reconstruc- authors note they use this procedure as an
tion with only an osteotomy, advises Dr. tion goes, Dr. Clair cites several studies alternative to triple arthrodesis in patients
Reeves. If arthrosis is present preopera- involving grafts and triple arthrodeses. who are at high risk for complications.
tively, he suggests considering a comput- Deland and colleagues noted the use of Lee found that the medial approach to
ed tomography (CT) scan to assess sever- a tendon graft through bone tunnels can the double arthrodesis for a foot with se-
ity. He says one should consider lateral help reconstruct the deltoid ligament and vere, longstanding valgus facilitates sim-
column lengthening with selective fusion rectify a valgus talar tilt.19 In a cadaver- ilar correction to the triple arthrodesis,
and medial soft tissue reconstruction for ic study, Haddad and coworkers noted obviating the necessity of calcaneocuboid
patients with pre-op arthrosis. Treatment success in reconstructing the deltoid lig- grafting.24 The author adds that the dou-
9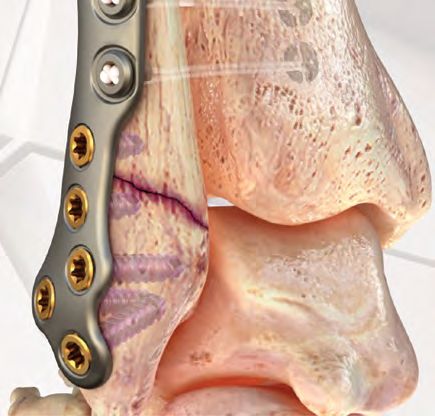
Post-ACFAS Supplement
nographic examination of the posterior tibial
tendon. Foot Ankle Int. 1997; 18(1):34–38.
12. Rockett MS, Waitches G, Sudakoff G, Brage M.
Use of ultrasonography versus magnetic reso-
nance imaging for tendon abnormalities around
the ankle. Foot Ankle Int. 1998; 19(9):604–612.
13. Shetty M, Fessell DP, Femino JE, et al. So-
nography of ankle tendon impingement with
surgical correlation. AJR Am J Roentgenol. 2002;
179(4):949–953.
Photo courtesy of Jason Miller, DPM
14. Chen YJ, Liang SC. Diagnostic efficacy of ul-
trasonography in stage I posterior tibial tendon
dysfunction: sonographic-surgical correlation.
Ultrasound Med. 1997; 16(6):417–423.
15. Therman H, Hoffmann R, Zwipp H, Tscherne
H. The use of ultrasonography in the foot and
ankle. Foot Ankle. 1992; 13(7):386–390.
16. Bureau NJ, Roederer G. Sonography of Achilles
tendon xanthomas in patients with heterozygous
familial hypercholesterolemia. AJR Am J Roent-
genol. 1998; 171(3):745–749.
17. Nallamshetty L, Nazarian LN, Schweitzer ME,
et al. Evaluation of posterior tibial pathology:
In this longitudinal view of the posterior tibial nerve in the tarsal tunnel, one can see hypoechoic comparison of sonography and MR imaging.
infiltrative scar tissue superficial to the nerve and obscuring the margins of the nerve. Skeletal Radiol. 2005;34(7):375-80.
18. Stewart MS, Bettin CC, Ramsey MT, et al. Ef-
fect of obesity on outcomes of forefoot surgery.
References
Foot Ankle Int. 2016; 37(5):483–7.
ble arthrodesis leads to fewer wound 1. Johnson KA, Strom DE. Tibialis posterior
19. Deland JT, de Asla RJ, Segal A. Recon-
complications, has higher union rates and tendon dysfunction. Clin Orthop Relat Res.
struction of the chronically failed deltoid
1989;239:196–206.
shorter surgical and recovery times. 2. Myerson MS. Adult acquired flatfoot deformity:
ligament: a new technique. Foot Ankle Int.
In a study of 32 severe pes planoval- 2004;25(11):795-9.
treatment of dysfunction of the posterior tibial
20. Haddad SL, Dedhia S, Ren Y, et al. Deltoid
gus deformities in 30 patients, Knupp and tendon. Instr Course Lect. 1997;46:393-405.
ligament reconstruction: a novel technique
coworkers evaluated the use of a double 3. Conti SF, Michelson J, Jahss M. Clinical
with biomechanical analysis. Foot Ankle Int.
arthrodesis using a medial approach for significance of magnetic resonance imaging
2010;31(7):639-51.
in preoperative planning for reconstruction of
hindfoot malalignment.25 The authors posterior tibial tendon rupture. Foot Ankle. 1992;
21. Jeng CL, Bluman EM, Myerson MS. Mini-
noted all feet had fusion in a mean of 13 mally invasive deltoid ligament reconstruction
13(4):208–214.
for stage IV flatfoot deformity. Foot Ankle Int.
weeks and added that the isolated medi- 4. Kerr R, Forrester DM, Kingston S. Magnetic
2011;32(1):21-30.
al approach led to fewer wound healing resonance imaging of foot and ankle trauma.
22. Galli MM, Protzman NM, Brigido SA. Ar-
problems in comparison with the lateral Orthop Clin North Am. 1990; 21(3):591–601.
throdiastasis of the lateral column with medial
5. Khoury NJ, El-Khoury GY, Saltzman CL,
approach. Brandser EA. MR imaging of posterior tibial
fusion: a retrospective examination of medial
Anand and colleagues studied 18 pa- double and Lapidus arthrodeses. J Foot Ankle
tendon dysfunction. AJR Am J Roentgenol. 1996;
Surg. 2015;54(3):412-6.
tients with posterior tibialis dysfunction 167(3):675–682.
23. Catanzariti AR, Adeleke AT. Double arthrod-
who had a double arthrodesis of subtalar 6. Schweitzer ME, Caccese R, Karasick D, et al.
esis through a medial approach for end-stage
and talonavicular joints via a single-in- Posterior tibial tendon tears: utility of secondary
adult-acquired flatfoot. Clin Podiatr Med Surg.
signs for MR imaging diagnosis. Radiology. 1993;
cision medial approach.26 Although the 188(3):655–659.
2014;31(3):435-44.
authors noted an 89 percent union rate, 24. Lee MS. Medial approach to the severe valgus
7. Khoury NJ, El-Khoury GY, Saltzman CL,
foot. Clin Podiatr Med Surg. 2007;24(4):735-44, ix.
they did not recommend their approach Kathol MH. Peroneus longus and brevis tendon
25. Knupp M, Schuh R, Stufkens SA, et al. Subtalar
as an alternative to a triple arthrodesis. tears: MR imaging evaluation. Radiology. 1996;
and talonavicular arthrodesis through a single
DeVries and Scharer compared triple 200(3):833–841.
medial approach for the correction of severe
8. Rosenberg ZS, Cheung Y, Jahss MH, et al.
arthrodesis with double talonavicular and Rupture of posterior tibial tendon: CT and MR
planovalgus deformity. J Bone Joint Surg Br.
subtalar arthrodesis, sparing the calca- 2009;91(5):612-5.
imaging with surgical correlation. Radiology.
26. Anand P, Nunley JA, DeOrio JK. Single-inci-
neocuboid joint.27 The authors found that 1988; 169(1):229–235. sion medial approach for double arthrodesis of
one can correct hindfoot deformity with 9. Waitches GM, Rockett M, Brage M, Sudakoff hindfoot in posterior tibialis tendon dysfunction.
hindfoot arthrodesis whether surgeons G. Ultrasonographic-surgical correlation of Foot Ankle Int. 2013;34(3):338-44.
include the calcaneocuboid joint or not. ankle tendon tears. J Ultrasound Med. 1998; 27. DeVries JG, Scharer B. Hindfoot deformity
17(4):249–256. corrected with double versus triple arthrodesis:
Dr. Jacobs notes Shi and Weinraub de- 10. Miller SD,Van Holsbeeck M, Boruta PM, et radiographic comparison. J Foot Ankle Surg.
scribed arthroscopic joint preparation as al. Ultrasound in the diagnosis of posterior 2015;54(3):424-7.
an effective alternative for hindfoot cor- tibial tendon pathology. Foot Ankle Int. 1996; 28. Shi E, Weinraub GM. Arthroscopic medial
rection in six patients.28 n 17(9):555–558. approach for modified double arthrodesis of
11. Hsu TC, Wang CL, Wang TG, et al. Ultraso- the foot. J Foot Ankle Surg. 2017;56(1):167-170.
10THE OFFICIAL MEETING
FOR MEMBERS OF
SYMPOSIUM ON ADVANCED WOUND CARE
THE
ASSOCIATION
November 2 – 4, 2018
FOR THE
ADVANCEMENT
OF WOUND
CARE
CAESARS PALACE | LAS VEGAS
EVERYTHING
PODIATRISTS
NEED TO KNOW ABOUT
WOUND CARE
Join us in Las Vegas, Nevada for the
Symposium on Advanced Wound Care Fall (SAWC Fall),
a leading interdisciplinary conference dedicated
to the advancement of wound care and healing.
Relevant Sessions for Podiatrists
AMP: The Multidisciplinary
Biofilm Busters: What They Are,
Approach to Limb Salvage How They Work, and How to Use Them
Debridement: Fact or Fiction
Update on Diabetes Management, 2018
Diagnosing and Treating Diabetic
And many more!
Foot Infections
New Skin Grafting Techniques
22+ 4 1,300+ 100+
CME/CE/CECHs TRACKS ATTENDEES EXHIBITORS
Register Today
SAWCFALL.COM
800 . 854. 8869
INTENDED LEARNERS Physicians NACCME designates this live activity for a max- Dietitians North American Center for Continuing REQUIRE-
This conference is designed for physicians, podiatrists, imum of 22.75 AMA PRA Category 1 Credits™. Physicians Medical Education, LLC (NACCME) is a Continuing MENTS FOR
nurses, physical therapists, researchers, and dietitians should claim only the credit commensurate with the extent CREDIT
Professional Education (CPE) Accredited Provid-
involved in wound healing or wound care issues. SAWC of their participation in the activity. er with the Commission on Dietetic Registration (CDR). To be eligible for documenta-
Fall provides attendees who study and treat wounds CDR credentialed practitioners will receive 4.0 continuing tion of credit for each session
4.0 AMA PRA Category 1 Credits™ for the pre-conference.
with state-of-the-art reviews of clinical problems and professional education units for the pre-conference, 15.5 attended, participants must
15.75 AMA PRA Category 1 Credits™ for the main conference. participate in the full activity
research information. continuing professional education units for the main
3.0 AMA PRA Category 1 Credits™ for the post-conference. conference, and 3.0 continuing professional education and complete the online general
CONFERENCE LEARNING OBJECTIVES
units for the post-conference for completion of this ac- survey and online evaluation
Nurses This continuing nursing education activ-
Assess current and emerging wound assessment and form for each session by
ity awards 4.0 contact hours for the pre-confer- tivity/material.
healing techniques December 4, 2018. Once these
ence, 15.75 contact hours for the main conference, CDR-Accredited Provider #HM001
Employ an interdisciplinary approach to wound pre- forms are completed online,
and 3.0 contact hours for the post-conference.
vention and treatment Level 3 Synthesis participants may immediately
Provider approved by the California Board of Registered
Physical Therapists North American Center for Continuing print documentation of credit.
Summarize current “gold standard,” evidence-based Nursing, Provider #13255 for 4.0 contact hours for the
guidelines for prevention and management of pres- pre-conference, 15.75 contact hours for the main con- Medical Education, LLC (NACCME) will be applying for Copyright ©2018 by North Amer-
sure ulcers ference, and 3.0 contact hours for the post-conference. pre-approved accreditation in California, Florida, Louisiana, ican Center for Continuing Medical
Maryland, New Jersey, Nevada, Ohio, and Texas, which Education, LLC. All rights reserved.
Investigate critical elements associated with proper Podiatrists North American Center for Continuing Medical
require pre-approval. If you practice in any other state, ADA STATEMENT
management of complex wound types, including Education, LLC (NACCME) is approved by the Council on
please consult its PT Board.
atypical wounds. Podiatric Medical Education as a provider of continuing North American Center for Con-
education in podiatric medicine. NACCME has approved For questions regarding this educational activity, please tinuing Medical Education complies
Identify the changes in the healthcare system and
this activity for a maximum of 22.75 continuing educa- call 609-371-1137. with the legal requirements of the
reimbursement that will impact wound care providers
tion contact hours. HARDWARE/SOFTWARE Americans with Disabilities Act and
across the continuum
4.0 continuing education contact hours for the pre-con- the rules and regulations thereof. If
Review the prevention, early detection, treatment, REQUIREMENTS
ference, 15.75 continuing education contact hours for the any participant in this educational
and rehabilitation of people with peripheral arterial All educational activities are accessible via a PC (Windows
main conference, and 3.0 continuing education contact activity is in need of accommodations,
and venous disease 2000/XP/Vista/7) or Mac (Mac OS 10.x or later) computer
hours for the post-conference. please call 609-371-1137.
with current versions of the following browsers: Internet
ACCREDITATION Explorer, Mozilla Firefox, Google Chrome, or Safari. Windows *Information contained herein is subject to
In support of improving patient care, North Media Player or compatible alternative, sound card, and change without notice.
American Center for Continuing Medical speakers are required for streamed audio. The latest version No commercial interest provided commercial
Education, LLC (NACCME) is jointly accredit- of the Adobe Flash Player is suggested for video programs. support for this continuing education activity.
ed by the Accreditation Council for Continuing Medical A PDF reader is required for print publications. Please
Education (ACCME), the Accreditation Council for Phar- direct technical questions to webmaster@naccme.com.
macy Education (ACPE), and the American Nurses Cre-
dentialing Center (ANCC) to provide continuing education
for the healthcare team.Post-ACFAS Supplement
Essential Insights On Managing
Achilles Tendon Ruptures
Given the challenges of treating Achilles tendon ruptures and the potential for re-rupture, these panelists at ACFAS
shared their thoughts as well as the literature findings on chronic Achilles ruptures, insertional tendinopathy and how to
prevent complications.
By Brian McCurdy, Managing Editor
W hen do you perform surgery
for Achilles tendon ruptures?
Amber Shane, DPM, FAC-
FAS, notes that the literature supports sur-
gical management for active older patients
noted that operative treatment leads to
better outcomes for patients with chronic
ruptures.1,2
Dr. Reeves says there are several surgical
options for chronic Achilles ruptures, in-
and those with chronic ruptures. She says cluding V-Y tendon plasty, a fascial turn-
Photo courtesy of William DeCarbo, DPM
one should reserve non-operative treat- down flap, allograft transplantation and
ment for inactive patients, those in poor flexor hallucis longus transfer.
health, those with poor skin and patients Guclu and colleagues cited good results
with systemic diseases. for the V-Y plasty in 17 patients with no
Ryan Rigby, DPM, FACFAS, says in- re-ruptures and a mean follow-up of 16
trinsic etiologies for intratendinous years.3 Patients had average Achilles de-
changes in the Achilles include tendon fects of 6 cm. Studying patients with de-
vascularity, gastrocnemius dysfunction, fects of more than 10 cm, Ponnapula and
age, sex and weight. He notes extrinsic colleagues described an inverted V tech-
etiologies include a change in training nique with a 180-degree twist to create a
patterns, poor technique and previous in- fascial strut, according to Dr. Reeves.4
jury. Ultimately, Dr. Rigby says excessive The V-Y advancement flap is Dr.
loading on the Achilles leads to tendinop- When it comes to surgical options for
Reeves’ preferred approach, especially for
athy and an imbalance between muscle Achilles tendinopathy, William DeCarbo, younger patients and those who have acute
power and elasticity. DPM, FACFAS, cites debridement of on chronic Achilles ruptures. He notes the
Dr. Rigby notes Achilles tendinopathy the posterior calcaneus/Achilles/bursa, technique is straightforward and surgeons
is due to a failed healing response, namely gastrocnemius recession, calcaneoplasty can easily combine it with flexor hallu-
a haphazard proliferation of tenocytes, de- or calcaneal osteotomy. cis longus transfers. Dr. Reeves adds that
generation in tendon cells and disruption a soleus attachment provides vascularity.
of collagen fibers. tion (ROM) and receive physical therapy. In regard to the flexor hallucis longus
Preoperatively, Dr. Rigby will discuss transfer, Dr. Reeves notes the tendon’s
with the patient intrinsic and extrin- Key Pearls For Treating Chronic close proximity to the Achilles is ad-
sic factors that may have led to rupture Achilles Ruptures vantageous and the surgical approach is
or chronic pathology, and ensure proper Patients with chronic Achilles ruptures relatively simple. He says the axis of the
surgical planning. Intraoperatively, he em- will complain of plantarflexion weakness contracture closely resembles that of the
phasizes a minimally invasive technique, in the ankle, a palpable mass in the ten- Achilles, the flexor hallucis longus fires
preserving the paratenon, offsetting the don, a palpable gap and an inability to rise in phase with the gastroc-soleus complex
paratenon incision from the skin incision, up on the toes, according to Christopher and the transfer has minimal biomechani-
addressing equinus contracture in the Reeves, DPM, FACFAS. In patients with cal effects.5 Dr. Reeves says flexor hallucis
chronic setting, respecting the soft tissues, chronic Achilles ruptures, he notes there longus harvest sites include the posterior
avoiding non-absorbable sutures when is a large fixed gap with secondary con- tibial tendon, sustentaculum tali, the mid-
possible, and avoiding suture strangula- traction and fibrosis. Dr. Reeves acknowl- foot and the hallux. He selects his harvest
tion of tendon tissue. Postoperatively, he edges primary anastomosis is inadequate site based on the size of the defect and the
says patients achieve early range of mo- for these patients. He says researchers have amount of distal tendon.
12Podiatry Today | June 2018
Citing a study of 20 patients with
chronic Achilles tendinopathy receiving
flexor hallucis longus transfers, David Cal-
darella, DPM, FACFAS, says the authors
found that 90 percent of patients scored
70 or above on the American Orthopedic
Foot and Ankle Society (AOFAS) scale
with no post-op re-ruptures.6 Schon and
colleagues, in a study of 46 patients with
insertional or mid-substance Achilles ten-
dinosis, found improvements in function
and pain with surgical debridement and a
flexor hallucis longus transfer.7 Photo courtesy of William DeCarbo, DPM
When performing a flexor hallucis lon-
gus transfer, Dr. Caldarella notes an in-
phase transfer is ideal. He says this approach
offers several advantages, including per-
forming the procedure locally, the intrin-
sic vascular supply of the area and the area
being within the axis of contractile force.
For the post-op course, Dr. Reeves
keeps patients non-weightbearing in a
plantarflexed splint for the first two and a
half weeks while patients can bear weight
in a neutral boot by weeks five to eight. Reattachment options for the Achilles include bone anchors, screws and trans-
He says patients walk in shoes between osseous sutures (shown here).
eight and 16 weeks post-op.
What You Should Know About stimulation, extracorporeal shockwave nosis.14 In addition, Dr. DeCarbo says De
Insertional Achilles Tendinopathy therapy (ESWT), and surgical release. He Vos and colleagues found no difference in
Insertional Achilles tendinopathy ac- notes corticosteroid injections are an op- pain improvement between patients using
counts for 20 to 25 percent of all Achilles tion but are very controversial. PRP and a placebo.13
disorders, according to William DeCarbo, In a review, Wiegerinck and colleagues When it comes to surgical options, Dr.
DPM, FACFAS.8 He cites possible causes noted that eccentric exercises for in- DeCarbo cites debridement of the poste-
for insertional Achilles tendinopathy in- sertional Achilles tendinopathy are not rior calcaneus/Achilles/bursa, gastrocne-
cluding inflammatory arthropathies, dia- as good as they are for non-insertional mius recession, calcaneoplasty or calcaneal
betes, corticosteroid use, age and repetitive pathology.10 In their study of eccentric osteotomy.15 He notes procedures that
loading. He notes differential diagnoses stretching, Verrall and coworkers found would use open repair include debriding
include Haglund’s deformity and posteri- the therapy less effective for insertion- a degenerated tendon, decompressing the
or heel spurs. al Achilles pathology in comparison to bursa, resecting bony pathology, reattach-
As far as pathomechanics go, Dr. De- mid-portion Achilles tendinopathy.11 ing the Achilles insertion and augmenting
Carbo says the anterior tendon is more Wiegerinck and colleagues found scle- repair with a graft/transfer.
involved than the posterior tendon, the rosing polidocanol and hyperosmolar dex- Surgeons can debride between 50 to 70
posterior tendon experiences higher trose to be effective, but urged physicians percent of the Achilles,according to Dr.De-
strain during dorsiflexion and there is to exercise caution with these injections.10 Carbo.16–18 He notes Paavola and cowork-
fibrocartilaginous endochondral ossifi- The same authors found ESWT to be ef- ers found an overall debridement compli-
cation.9 However, he notes fibrocartilagi- fective for insertional Achilles tendinopa- cation rate of 11 percent in 432 patients.19
nous ossification develops on the anteri- thy, notes Dr. DeCarbo. Dr. DeCarbo says Jerosch and cowork-
or aspect of the tendon. Dr. DeCarbo cites two studies finding ers found good or excellent results with
Dr. DeCarbo cites several treatment op- that PRP injections had less than favor- calcaneoplasty for 81 patients with Ha-
tions for insertional Achilles tendinopathy, able results in those with non-insertion- glund’s syndrome at an average follow-up
including stretching, offloading, non-ste- al Achilles tendinopathy.12,13 Sadoghi and of 35 months.15
roidal anti-inflammatory drugs (NSAIDs), coworkers found PRP to be benefi- In a review of six studies focusing on
orthotics or foot ankle orthotics (AFOs), cial for healing strength in patients with 211 Achilles tendons in 200 patients,Wie-
platelet-rich plasma (PRP)/bone marrow acute ruptures but says the therapy had gerinck and colleagues studied resection
aspirate, ultrasound-guided debridement/ no benefit for those with Achilles tendi- of the calcaneus, the retrocalcaneal bursa
13Post-ACFAS Supplement
and calcifications.10 Overall, they noted adaptive gait patterns.
good patient satisfaction and improved
Visual Analogue Scale scores for all the How To Handle Postoperative
techniques with no one technique being Achilles Complications
superior to the others. What complications commonly arise fol-
Surgeons can reattach the Achilles with lowing Achilles rupture surgery? While
bone anchors, screws or transosseous su- the Achilles tendon is easy to access and
tures, according to Dr. DeCarbo. Refer- has no non-vascular bundles nearby, the
ring to a study assessing a central incision patient may have tendon dehiscence, scar
technique to facilitate surgical treatment tissue, repair failure and slow healing, ac-
Photo courtesy of William DeCarbo, DPM
of insertional Achilles tendinopathy, Dr. cording Dr. Rigby. The Achilles midsec-
DeCarbo says Nunley and colleagues tion is more hypovascular than the rest of
noted 96 percent patient satisfaction at a the tendon, which he says poses the highest
mean follow-up of four years.16 risk of rupture and other complications.
A study by DeCarbo and Hyer de- Eric Barp, DPM, FACFAS, cites skin
scribed transferring the flexor hallucis necrosis, dehiscence, adhesions, sural
longus tendon to the calcaneus.20 The nerve injury, tendon lengthening issues,
authors note this technique entails a pos- complex regional pain syndrome, deep
terior incision and fixation with an inter- vein thrombosis (DVT)/pulmonary em-
ference screw. Hunt and colleagues found bolism, re-rupture, infection and painful
patients who had a flexor hallucis longus scars as possible complications of surgery
tendon transfer had better ankle plantar- for Achilles tendon ruptures.
flexion strength in comparison with those Dr. DeCarbo cites possible causes for A review by Wong and colleagues
who had Achilles debridement alone insertional Achilles tendinopathy including found the incidence of skin healing com-
with no difference in pain and function inflammatory arthropathies, diabetes, plications in Achilles rupture patients to
between the two groups.21 However, Dr. corticosteroid use, age and repetitive be the highest, 14.6 percent, in a total of
DeCarbo notes the authors suggested re- loading. He notes differential diagnoses 3,718 patients receiving open repair and
include Haglund’s deformity (shown above)
serving flexor hallucis longus transfer for in immobilized patients.30 Dr. Barp says
and posterior heel spurs.
revisional Achilles surgery. the authors noted general complications
Tallerico and colleagues performed were lower in those who had open repair
a retrospective study on gastrocnemius noted poor visualization of the sural nerve and early mobilization.
recession for insertional Achilles tendi- and a risk of iatrogenic nerve injury.25 Patients can be at risk for Achilles
nopathy in 11 patients.22 Dr. DeCarbo Pinney and coworkers found that pa- re-rupture after surgery, according to Dr.
says the authors found patients had relief tients with gastrocnemius contracture Shane. In a study of 762 patients, she notes
from pain and a quick recovery at an av- who had an isolated gastrocnemius release Deng and colleagues found surgically
erage follow-up of one year. He notes that increased their ankle dorsiflexion by an treated patients experienced a 3.7 percent
studies by Duthon, Laborde and their re- average 18.1 degrees with a postoperative rate of re-rupture in comparison to 9.8
spective colleagues found similar positive ankle dorsiflexion equivalent to preopera- percent of those who received non-surgi-
results for gastrocnemius recession with tive ankle dorsiflexion.26 cal treatment.31
Laborde recommending the procedure as In a study focusing on 35 patients with Studying 210 patients who had eight
the initial treatment.23,24 flatfoot, Rong and colleagues noted the weeks of non-operative care for Achilles
Baumann procedure can correct the tendon ruptures, Reito and colleagues
Managing Equinus In Achilles tightness of the gastrocnemius or the gas- found 7.1 percent of patients had a
Rupture Patients trocnemius-soleus complex.27 re-rupture while 10 percent had “all-
When performing the Silfverskiold test to Chimera and coworkers found patients cause failure” of treatment.32 Dr. Shane
evaluate equinus, Michael Gentile, DPM, with isolated gastrocnemius contracture says the authors noted age alone was not
FACFAS, suggests using consistent land- had improved dorsiflexion range of mo- an indicator for operative treatment as it
marks, ensuring the subtalar joint is in tion, function and plantarflexion strength was not a predictor of early failure.
neutral and the midtarsal joint is locked. following gastrocnemius recession.28 As Dr. Barp notes, risk factors for wound
He says one should measure equinus twice In another study by Chimera and col- complications following Achilles surgery
and confirm the position intraoperatively. leagues, surgical intervention for patients include tobacco and steroid use. He cites a
In a cavader study, Tashjian and col- with isolated gastrocnemius contracture study noting wound complications in 10
leagues found surgeons can attain a did not create any negative gait adapta- percent of 219 Achilles surgery patients.33
complete gastrocnemius aponeurosis tions.29 However, the authors noted that In a study of 371 patients who were im-
transection with a modified endoscopic patients may benefit from gait retraining mobilized after an Achilles rupture, Lassen
gastrocnemius recession, but the authors following recession due to post-op mal- and coworkers found deep vein throm-
14Superior Strength* and Profile for
Uncompromised Performance
ORTHOLOC 2 ™
with 3Di Technology
CROSSCHECK™
Plating System
Ankle Fracture
Small Bone LP System
Plating System
Strength* Profile Speed
Type II Ti Alloy Provides Increased Low Profile Plates Designed to Implants and Instruments Designed to
Material Fatigue Strength Reduce Soft Tissue Irritation Reduce Steps and Improve Efficiency
Superior to Color Anodized Ti
Alloy & Stainless Steel.
* Data on file.
All products not available in all markets.
™ and ® denote Trademarks and Registered marks of Wright Medical Group N.V. or its affiliates.
©2018 Wright Medical Group N.V. or its affiliates. All Rights Reserved. 016489AYou can also read