Quality Account 2018/19 - Page 1 of 76 - Bristol Community Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Quality Account 2018/19
Page 1 of 76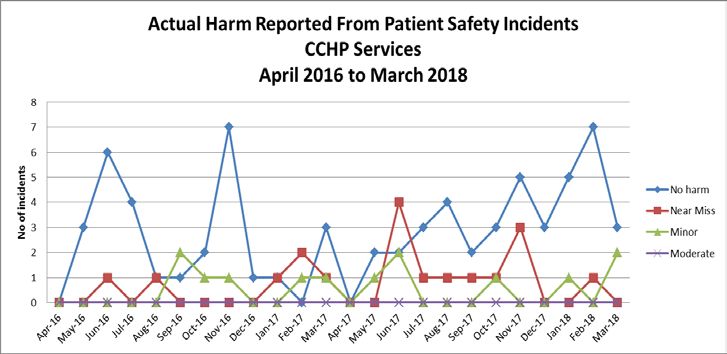
Contents
Introduction .............................................................................................................. 4
What is the Quality Account? .................................................................................. 4
Foreword ................................................................................................................. 4
Who we are ............................................................................................................. 5
Our activity in 2017/18, in numbers ......................................................................... 6
About our partnerships ............................................................................................ 6
Our approach to quality ........................................................................................... 6
Thank you ............................................................................................................... 8
Looking back ............................................................................................................ 9
Our quality priorities over the last 12 months .......................................................... 9
Priority 1: Healthy Together clinic ........................................................................... 9
Priority 2: Patient activation measure .................................................................... 11
Priority 3: Making every contact count .................................................................. 12
Priority 4: Patient leadership programme – Healthcare Change Makers .............. 13
Priority 5: Human factors training .......................................................................... 15
Priority 6: Multi-agency safeguarding hub ............................................................. 17
Other aspects of assurance .................................................................................. 18
Safeguarding ‘Think Family’ .................................................................................. 18
Staff experience .................................................................................................... 18
Learning and development.................................................................................... 19
Patient safety ........................................................................................................ 19
Pressure ulcer prevention ..................................................................................... 20
Infection prevention and control ............................................................................ 20
Clinical supervision ............................................................................................... 21
Our performance against key national indicators .................................................. 21
Review of CQUIN goals: 2018/19 ......................................................................... 22
Areas of consistently good or improved performance ........................................... 23
Our awards and achievements ............................................................................. 24
Innovation ............................................................................................................... 26
Wound care service In-Reach model .................................................................... 26
Community Navigators Bristol ............................................................................... 27
Diabetic Eye Screening Programme ..................................................................... 27
HealthBar .............................................................................................................. 29
Page 2 of 76
Learning disability and domestic violence and abuse ........................................... 30
Patient and public empowerment ......................................................................... 32
Working with our service users ............................................................................. 32
Listening to our service users ............................................................................... 32
Learning and improving ........................................................................................ 34
Involving and engaging ......................................................................................... 36
Looking forward: Quality account priorities 2018/19 .......................................... 39
Overview ............................................................................................................... 39
Person-centred care ............................................................................................. 39
Developing our research capability and expertise................................................. 40
Pressure ulcers and the malnutrition universal screening tool .............................. 42
Safeguarding adults: Making safeguarding personal ............................................ 43
Learning and action: patient experience and patient stories ................................. 45
Catheter pathway and passport ............................................................................ 46
Service improvement ............................................................................................ 48
Quality and effectiveness ...................................................................................... 50
Data quality ........................................................................................................... 50
Audits .................................................................................................................... 51
Clinical effectiveness ............................................................................................ 54
Clinical research ................................................................................................... 55
Care Quality Commission ..................................................................................... 56
Continuous learning and improvement ................................................................. 58
What other organisations say about us ................................................................. 58
Statement of assurance: Patient and staff feedback ............................................. 59
Appendix ................................................................................................................. 59
Safeguarding: ‘Think Family’ ................................................................................. 59
Staff experience .................................................................................................... 61
Learning and development.................................................................................... 64
Information governance toolkit - attainment levels ................................................ 65
Patient safety ........................................................................................................ 66
Optimising medicines management ...................................................................... 71
Pressure ulcer prevention ..................................................................................... 73
Infection prevention and control ............................................................................ 75
Page 3 of 76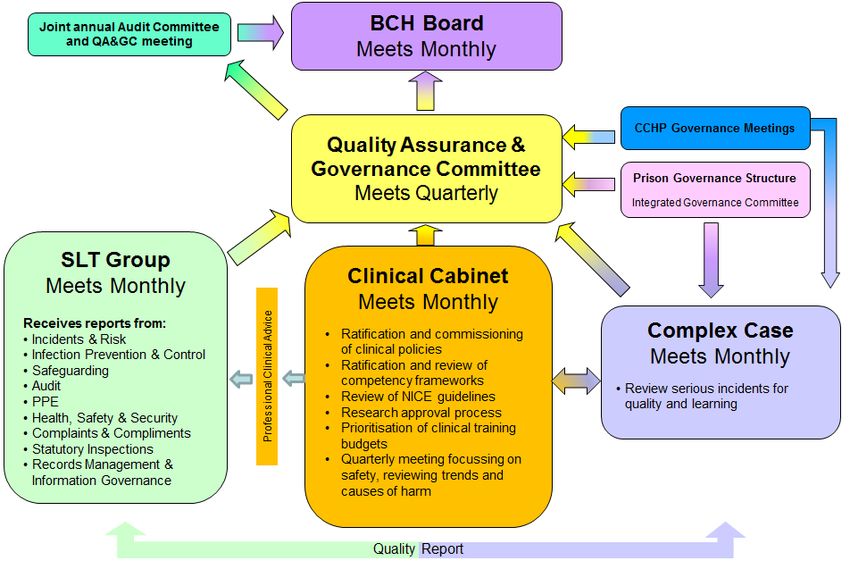
Introduction
What is the Quality Account?
The Quality Account is an annual document that the Department of Health requires
from providers of healthcare that reports on quality of care under three key elements
- patient safety, patient experience and clinical effectiveness.
In this Quality Account, we outline our quality improvement initiatives for the year
ahead, and reflect on those from the past year and aim to help our readers
understand the areas we have advanced, as well as those areas that we have
identified where quality or safety can be further improved. All the information has
been drawn together and shared with a variety of stakeholders and their feedback
incorporated in the published version.
This Quality Account is written for our patients, children, young people, families and
carers, as well as our commissioners (BNSSG CCG and NHS England) and other
healthcare providers and Trusts that work alongside us. We understand that some of
the abbreviations and clinical terms used in healthcare can be difficult to understand,
so to make this information as accessible as possible, there are explanations
throughout the document.
Foreword
Welcome to our 2018/2019 Quality Account. It is a comprehensive and honest
summary of our work over the past year - it highlights areas where we have excelled
and also those we want to improve. It also outlines our priorities for next year.
As the biggest provider of local community health services, we hope you will see
evidence of ways we help families thrive in their own homes and empower them to
make the most of the community on their doorstep. You will also see how we support
our local hospitals, GPs and social care organisations by proactive interventions in
the community, getting patients home from hospital sooner and preventing
admissions in the first place.
None of this is possible without working closely with local partners and challenging
ourselves to think creatively about better ways of doing things.
For example, our Diabetic Eye Screening team is working closely with local GP
practices and other healthcare providers to target hard-to-reach communities in
Bristol. They’re now screening significantly more people with diabetes than ever
before.
We’ve been partnering with social care teams to devise a new tool to help carers
identify the early warning signs of pressure ulcers, which currently cost the NHS
Page 4 of 76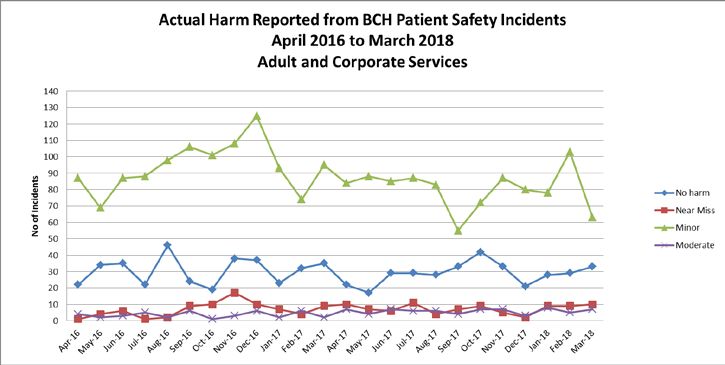
more than £3.8 million every day to treat and cause avoidable suffering to patients.
We’re sharing expertise within teams too: specialist wound care nurses are now
spending time in our community nursing teams as wound care ‘buddies’. Earlier
specialist intervention means quicker healing.
We are also setting our sights on becoming local leaders in research in community
healthcare so we are at the forefront of new treatments and technology. So we have
become the first ever community organisation to join the Clinical Research Network
Site Initiative, which will give us expertise and support to take the lead.
Another priority will be continuing our work on service improvements to make sure
that our teams have more time to care for our patients. We’ve already reorganised
our community nursing teams to enhance the patient experience and continuity of
care.
This is just a taste - you can read all about what we’ve been doing over the past year
along with plans for the future in this Quality Account. At a time when the health
sector is under well-publicised pressure, we’re committed to keeping our focus on
what’s most important: working with patients, the public and our staff for a better
quality of life for everyone and high-quality, safe care.
Julia Clarke, Chief Executive
Steve Hughes, Chair of the Board
Who we are
Bristol Community Health provides NHS health services to adults, children, young
people and families in the community, at home and in local prisons. Our 1,700 staff
provide a wide range of community services ranging from community nursing teams
and end of life care to offender healthcare, school nursing, health visiting, diabetes
support, physiotherapy and occupational therapy.
• We are a not-for-profit social enterprise owned by our staff
• All surpluses that we make are reinvested back into our services for the good
of our local community
• Our dedicated and compassionate teams have a reputation for high-quality,
person-centred care
• We were given an overall rating of ‘Good’ for all our community services by
the Care Quality Commission in 2017
• Our turnover is expected to be £77 million (between April 2018 and March
2019) which comes mainly from contracts with NHS England, Bristol, North
Somerset and South Gloucestershire Clinical Commissioning Group (BNSSG
CCG).
Page 5 of 76
Our activity in 2017/18, in numbers
• 97% of our patients seen in patients’ homes or in community settings would
recommend our services to friends or family, should they need similar care or
treatment. In urgent care settings, 93% of patients would recommend us.
• Made over half a million patient contacts
• Prevented 4,644 hospital admissions
• Worked with over 50 local partners and over 400 GPs
About our partnerships
Community Children’s Health Partnership (CCHP)
Community Children’s Health Partnership (CCHP) provides all of the community
child health and child and adolescent mental health services for Bristol and South
Gloucestershire. The partnership includes Bristol Community Health, Sirona care &
health CIC, Avon and Wiltshire Mental Health Partnership NHS Trust, University
Hospital Bristol NHS Foundation Trust, Barnardo's and Off the Record.
http://cchp.nhs.uk/cchp/what-cchp
InspireBetterHealth
InspireBetterHealth provides a complete offender healthcare service, including
physical health care, mental health care, health promotion and professional training
and development. The partnership brings together the expertise of leading
healthcare organisations including: Bristol Community Health CIC, Avon and
Wiltshire Mental Health Partnership NHS Trust, Hanham Health, GP Care, Time for
Teeth, Homecare Opticians, Day Lewis Pharmacy, Sirona care & health CIC.
Our approach to quality
The three key strands of our quality model reflect the Department of Health
approach. They are patient safety, patient experience and clinical effectiveness. Our
quality model aims to ensure that staff deliver the fundamental elements of good
care – compassion, dignity, respect and safety – first time and every time and to
everyone whom we serve. We want staff to make every contact count, aspire to the
highest quality of care, and focus on achieving the best outcomes for our patients
through best practice and innovation.
Our clinical governance structure (see diagram 1) aims to ensure that we continually
improve quality within our services.
Page 6 of 76Diagram 1. Bristol Community Health’s clinical governance structure
Clinical governance is reinforced through a structure of focused working groups that
monitor the outcomes from our work streams for:
• Patient and public empowerment - which includes complaints and
compliments
• Patient safety and risk management – which includes complex case reviews
• Information governance
• Prison governance groups
• Clinical audit, effectiveness, research and innovation
• Safeguarding adults and children
• Medicines management and our non-medical prescribing groups
• Supervision and competency of clinical staff
• Infection prevention and control
Each is monitored through review of data including audits and incidents and
comparing our performance against national and local standards. This is overseen
by the Quality Assurance and Governance Committee which reports directly to our
Board (see diagram 1), who receive a monthly report on all areas of quality. We aim
to group clinical outcomes to provide evidence that assures our services are:
Page 7 of 76• Safe
• Effective
• Caring
• Responsive
• Well-led
As an independent sector provider of NHS funded services our main mechanisms for
accountability, quality and assurance include:
• Corporate and individual accountability
• Contractual relationship with the Clinical Commissioning Group and NHS
England
• Regulatory relationships with the Care Quality Commission, the Health and
Safety Executive and the Community Interest Companies Regulator
• Scrutiny by local Healthwatch and Bristol City Council People Scrutiny
Committee
Thank you
We would like to thank the patients, carers and voluntary sector organisations that
have helped us shape this Quality Account. Thanks to your input, our future Quality
Account priorities have your needs and concerns at their centre. Have a look through
this document to see exactly where your thoughts and views have made an impact.
Throughout this Quality Account, the term ‘you’ refers to the people we serve. Every
change we have made has been made with the intention of improving the lives of
people in our communities.
This is a public document and is available in a variety of media, formats and on our
website.
To access the document in another format, call 0117 440 9000 or email
briscomhealth.comms@nhs.net
Page 8 of 76Looking back
Our quality priorities over the last 12 months
In this section you will find information relating to our quality priorities of 2017/18.
The numbering of these priorities is for ease of navigation rather than an indication of
priority.
Clinical effectiveness
Priority 1 – Healthy Together clinic *Patient choice priority*
Priority 2 - Patient activation measure (PAM)
Priority 3 - ‘Making every contact count’ (MECC)
Patient experience
Priority 4 - Patient leadership programme: Healthcare Change Makers
Patient safety
Priority 5 - Human factors training
Priority 6 - Multi-agency safeguarding hub (MASH)
Priority 1: Healthy Together clinic
The Healthy Together clinic (formerly known as the integrated community clinic) is a
new model of healthcare provision. It aims to provide intervention and treatment for
leg ulcers - as well as an opportunity for social interaction - among patients in South
Bristol. Consultation with patients attending the clinic led to the renaming of the clinic
in October 2017 as the Healthy Together clinic.
The Healthy Together clinic demonstrates an important development in partnership
working between the South Bristol Primary Care Collaborative (SBPCC) and Bristol
Ageing Better (BAB).
What we said we’d do
We said we would set up the Healthy Together clinic to deliver our common aims of:
• Developing new ways of working together.
• Providing services tailored to promoting independence and improving
social value locally.
• Delivering accessible, joined-up healthcare for patients in South Bristol.
• Promoting faster and longer-lasting wound healing by delivering clinical
interventions in a social setting that supports and encourages people to
feel more in control of their condition.
Page 9 of 76• Providing consistent treatment by clinical staff working in a new and
integrated way.
What we did
We based our model and clinical interventions on best practice, including:
• Securing a non-clinical, accessible community venue at the Withywood
Centre to promote social inclusion.
• Employing a specialist tissue viability nurse, ensuring patients received the
highest standard of treatment.
• Delivering the gold-standard of leg ulcer management and compression
bandaging to promote faster healing.
• Jointly staffing the clinic with Bristol Community Health community nurses,
GP practice treatment room nurses and healthcare assistants to promote
integrated working and consistent practice across the local area.
• Working with AgeUK Bristol, to deliver social support for patients, recruit
volunteers and arrange transport for patients where needed.
• Hosting speakers and information sessions organised by AgeUK to
promote healthy living and wellbeing.
• We received 67 referrals, of which 12 were inappropriate or did not
continue attendance. Of the remaining 55 patients, 35 have healed and
the remaining 20 continue to attend.
What has changed and how?
The clinic is delivering important clinical and social outcomes for patients including:
• 55% of patients have been discharged as healed within three months of
first attendance at the clinic. 1
• Less than 2% of patients who attended the clinic have had a recurrence of
their leg ulcer. 2
• Two patients have returned to the clinic as volunteers.
• Patients report that they feel more positive about their treatment when they
see other patients progress.
• Some patients who were previously attending treatment rooms for multiple
visits per week now only require one visit to the clinic due to a change in
treatment regime.
• The majority of patients report that they enjoy the social aspect of the clinic
and some patients stay on at the centre to have lunch following their
treatment.
1
Based on four months of recording clinical outcomes between Sep 17 and Jan 18
2
Based on 10 months of clinic attendance
Page 10 of 76• All nurses and healthcare assistants report an improvement in their clinical
knowledge and practice as a direct result of working in the integrated
setting supported by the specialist nurse.
What have we learnt?
• We need to manage our patient intervention time.
• Some patients have more readily accepted having their care delivered at
the clinic rather than the treatment room.
• Some patients do not feel comfortable having their treatment delivered in a
communal setting.
• Some GP practices involved in the clinics have a higher proportion of
patients who require lower leg wound care than the others.
• Most community-nursed patients need specialist transport arrangements
and can’t leave their home without support. While the clinic environment is
fully accessible, the risk of falls for physically frail patients is high and
therefore the clinic environment is potentially unsafe.
• Referral to the clinic has been on a first-come, first-served basis and not
necessarily clinical need.
• Our social interventions need to be relevant, useful and patient led.
How we will continue the work
Our model will require proportionate staffing levels to patient numbers per practice.
Both the SBPCC and AgeUK Bristol support the continuation of the Healthy Together
clinic. However, funding is coming to an end. We are working together to seek new
ways to fund the clinic to ensure that patients in South Bristol continue to benefit and
our partnership with the voluntary sector continues to thrive.
There is significant interest in replicating the Healthy Together clinic model in other
areas of Bristol and therefore this learning has been essential to ensure the future
roll-out of a tested and improved model.
Priority 2: Patient activation measure
The patient activation measure (PAM) is a tool that enables healthcare professionals
to understand a patient’s level of knowledge, skills and confidence in managing their
own health and care. Activation is particularly important to people living with long-
term conditions who are frequent and long-term users of health services because
evidence shows that higher activation is associated with higher quality of life and
better healthcare outcomes.
Page 11 of 76What has changed and how?
The use of PAM is enabling staff to better triage patients for intervention based on
their level of activation and interest. It has improved communication with patients
about their needs, wishes and goals to promote the management of their condition
and has improved collaboration and shared decision making. We now offer patients
the right information appropriate to their level of activation at the right time to support
access to the most appropriate services for them. 100% of staff in the teams
implementing PAM have received training on how to complete PAM surveys are
holding care and support planning discussions with patients and to date PAM has
been completed in appropriate patients with long term conditions in Respiratory
(75%) and Macmillan Cancer Rehab support (85%) teams. Pathways of care in each
of the teams have been reviewed to enable the embedding of person-centred care
approaches and to support appropriate patients to develop personalised care and
support plans.
What have we learnt?
Assessing a patient’s activation enables us to appropriately triage the patient and
allocate resources required to ensure their needs are met. The completion of a post-
intervention PAM survey supports our review of the effectiveness of the intervention
as well as improvement in patient motivation.
How we will continue the work
We will continue to implement PAM in other appropriate teams serving patients with
long-term conditions, for example the Specialist Community Neurology service. We
will continue to measure patient activation levels and tailor our support to improve
their activation and empower patients to be in control of their own health and care.
This will become part of a new priority for person-centred care (see p.41).
We will keep holding care and support planning conversations with patients identified
as having low activation levels along with their carers to support them to become
more activated.
The training will be rolled out to teams who will take up PAM implementation in
2018/19.
Priority 3: Making every contact count
Making every contact count (MECC) is an approach to behaviour change that is
about staff having ‘healthy conversations’ with patients. It includes asking open
questions to help them make positive lifestyle changes, specifically to:
• Stop smoking
• Drink alcohol only within the recommended limits
Page 12 of 76• Eat more healthily
• Be physically active
• Maintain a healthy weight
• Improve mental health and well being
By having healthy conversations, we can help patients find their own solutions and
encourage them to set their own goals using a specific, measurable, attainable,
relevant, and time-based (SMART) template.
What has changed and how?
In December 2017, Bristol Community Health was awarded an £8,000 grant from
HEE to support the roll out of MECC. We have held meetings with key MECC leads
from other organisations within BNSSG awarded the same grant. Bristol Community
Health also received 3 places on the recent MECC train the trainer programme held
in Bristol to boost its pool of trainers.
We have made available the e-learning course to complement the face to face
training and facilitated introductory MECC training sessions with some staff teams
including a community nursing team, Diabetes and Nutrition Service, Heart Failure
and Respiratory.
What have we learnt?
Holding the MECC sessions alongside two other self-management training
sessions (Shared Decision Making and Patient Activation) really cements the value
of a patient centred approach to our clinicians
How we will continue the work
We have started to draft the Bristol Community Health strategic implementation and
training plan and it will be ready for review by 18th May 2018.
MECC, in combination with PAM, is now being developed as a new priority for
person-centred care. Please see p.41 for further information.
Priority 4: Patient leadership programme – Healthcare Change
Makers
What we said we’d do
Bristol Community Health, North Bristol NHS Trust and University Hospitals Bristol
NHS Foundation Trust jointly invested in a patient and community leadership
programme in 2016.
Page 13 of 76The intended outcome for the programme is to create a new collaborative
relationship between the healthcare system and its communities, in line with the
NHS Five Year Forward View.
The patient leadership training that took place between October 2016 and February
2017 was designed to equip members of the public with the knowledge, confidence
and skills to build relationships with and influence healthcare decision-makers, senior
managers and clinicians to support integration and new ways of working.
We said we would develop and grow the role of patient leadership over the year by
creating space and dialogue between the Healthcare Change Makers and the
decision-makers in the local health system.
What we did
Following the patient and community leadership training programme, the Healthcare
Change Makers came together with the Patient and Public Involvement leads from
across the partner organisations to create the Healthcare Change Maker forum
which started in March 2017 and met bi-monthly over the course of the year.
The forum has become a supportive space for the Healthcare Change Makers that
encourages them to learn from one another, share ideas and discuss projects they
have been involved with. It’s also encouraged them to consider approaches to
influence the planning and delivery of local health services.
Over the course of the year, the forum afforded the space for collaboration and
dialogue between the Healthcare Change Makers and the decision-makers in the
local health system. Examples of involvement work over the year have included:
• The Healthier Together 3 respiratory care pathway
• The Healthier Together diabetes care pathway
• The overarching Healthier Together care model
• Engagement on the out of hospital/integrated primary and community care
work stream of Healthier Together.
During the year, the workforce and public engagement approach for Healthier
Together was being developed and the Healthcare Change Makers were part of the
overall engagement plan. Discussions have started on how the patient leadership
model could be grown across BNSSG to facilitate the influence of patient voice in
shaping the Healthier Together plans.
What has changed and how?
3
Healthier Together is the name for the Bristol, North Somerset and South Gloucestershire
Sustainability and Transformation Partnership (STP).
Page 14 of 76We commissioned the University of West of England Leadership and Change Centre
to evaluate the impact of the patient leadership programme. The interim evaluation
report was published in January 2018 and has highlighted:
• Stakeholders, including decision makers in the local health system and the
Healthcare Change Makers, valued the innovative nature and design of
the programme. There was broad agreement that the concept was strong
and worth pursuing further.
• More could be done to facilitate the coming together of Healthcare Change
Makers throughout the programme and in between the forums to support
building productive relationships, team working and a sense of identity.
• Further work is required to focus on increasing the Healthcare Change
Maker’s knowledge on the wider healthcare system in order to cultivate a
better understanding of how services and providers work together and
specifically further involvement of healthcare staff to facilitate this.
Overall, there have been some demonstrable examples of how the Healthcare
Change Makers have influenced specific areas of work, for example the diabetic foot
care pathway and the overarching care model for the STP.
How we will continue the work
This early success and momentum needs to be built on to encourage a greater
public voice in decision-making at a time when the health system is facing
considerable challenge, both financially and in increasing demand for services. The
final evaluation report is due in September 2018 and we hope this will influence the
engagement approach of both individual providers as well as the Healthier Together
plans going forwards.
Priority 5: Human factors training
It is acknowledged within the Duty of Candour legislation that medical treatment and
care is not risk-free. Errors will happen and nearly all of these will be due to failures
in organisational systems or genuine human errors. Minimising the risk of errors and
providing person-centred, harm-free care is a key priority for Bristol Community
Health and to help achieve this we introduced human factors and simulation training.
Human Factors Training encourages staff to think about the failings a human can
make, particularly in communication.
What we did
We provided staff with human factors training including SBAR (Situation,
Background, Assessment and Recommendation). This structure for communication
standardises and simplifies information passing between health professionals and
there is evidence that this reduces errors that could affect patient care.
Page 15 of 76We successfully applied for funding from Health Education England (HEE) so that a
bespoke Community Simulation Training course could be developed.
We introduced the global trigger tool (GTT) case note review in prison settings. GTT
is a model where a sample of case notes is reviewed to identify any gaps in care.
What has changed and how?
We are now seeing the SBAR tool being used in clinical records, at handovers and
within the incident reporting system. It is becoming more commonly used as part of
the language to transfer patient information within the healthcare community.
All prison healthcare settings have completed their baseline audit of the global
trigger tool and found there was no latent harm identified in the records. Most of the
prison sites now include global trigger tool in their audit cycle and the process is
becoming embedded into service assessment.
The simulation training (an opportunity to practise these techniques in a simulated
situation) took place between 14-16 March 2018 and involved 16 members of staff
from the prison and adult community services. The training used scenarios that
reflect the business challenges that Bristol Community Health personnel face.
How we will continue the work
This is very new training for Bristol Community Health, one that involves new ways of
thinking and which had not been previously applied to the community setting. This
learning will be continued by working to set up a Bristol Community Health SIM
(simulation) network during 2018/19 and to embed the learning through involvement
with the Learning and Development team. Some of the feedback received since the
training includes:
“It is very powerful and allows individuals to understand not
just the clinical task but a situational awareness of their role
and responsibilities.”
“The course gave us skills on using non-judgemental
feedback which will be explored to find how individuals feel
within a scenario.”
We will continue to evaluate the effectiveness of this approach.
Page 16 of 76Priority 6: Multi-agency safeguarding hub
What we said we’d do
The multi-agency safeguarding hub (MASH) in Bristol brings together a small team
of expert professionals, from services such as the local authority, police and health
providers. Our aim was to:
• Provide the representation for the combined health service providers
working in Bristol in the newly formed Bristol MASH.
• Deliver the safeguarding children training requirement to services in Bristol
Community Health, the Community Children’s Health Partnership (CCHP)
and InspireBetterHealth.
What we did
The MASH went live on 7 August 2017. There were some initial IT problems due to
the complex nature of the MASH working across several agencies, including external
agencies. These issues were resolved by early October 2017.
Referral into the MASH is an internal process within the local authority children’s
services. From October to December 2017, of the 5,757 contacts received by the
local authority ‘front door’ (first response), 153 (3%) were sent to the MASH for
review.
• Over a third (38%) of the 153 contacts sent to MASH required no further
action.
• 44% were sent to either a social work unit or the pathway decision team (team
within the local authority children’s services).
• 5% were referred to early help services.
• 11% were passed onto other single agencies including police (1%), health
(9%) and other (1%).
How we will continue the work
The MASH is now fully established in Bristol and we will continue to work with our
multi-agency colleagues to ensure that all of those children and families who are
reviewed by MASH and who require further actions receive a suitably targeted
service.
Page 17 of 76Other aspects of assurance
Within this section you will find information on other areas of quality improvement.
• Safeguarding ‘Think family’
• Staff experience
• Learning and development
• Patient safety – incident reporting
• Pressure ulcer prevention
• Infection prevention and control
• Clinical supervision
• Our performance against national priorities
• Review of our CQUIN goals: 2017/18
• Areas of consistently good or improved performance
• Our awards and achievements
You can find more detailed information on safeguarding, incident reporting, staff
experience, learning and development, pressure ulcer prevention and infection
prevention and control in the appendix (p. 62).
Safeguarding ‘Think Family’
Ensuring all our staff are supported to prevent, recognise, report and help address
abuse continued to be an important priority for us in 2017/18. We want our staff to be
able to recognise and respond to whatever form exploitation or abuse takes and
whoever it affects. When our staff visit or see people in clinics, they are in an ideal
position to identify the wider risks affecting families, carers, people who are part of
neighbourhood and care communities and to see how this impacts everyone
involved.
One of our main initiatives has been to introduce training at induction level that
combines both safeguarding adults and children.
Reporting processes have been brought together so we are presenting a much more
memorable set of instructions about who can advise staff and how they report.
Read more in the appendix on p.62.
Staff experience
During 2017/18, we continued to prioritise improving the experience of our staff, to
ensure the continued delivery of high-quality patient care. Our annual staff survey
found that from the 69% of staff that responded, 78% would recommend Bristol
Community Health to friends and family if they needed care or treatment.
Page 18 of 76As well as gathering information through the staff survey, a series of team ‘talkbacks’
were held by senior management and board members and various staff events were
held to encourage staff to be involved in shaping the future of our organisation.
Read more in the appendix on p.64.
Learning and development
We continue to invest in the development of our staff and offer a wide range of
learning and development opportunities to ensure that they are able to deliver the
best possible care and support to our patients and their carers and ensure our staff
can maximise their career opportunities.
All our services continue to exceed the 90% compliance target of their statutory and
mandatory training.
Staff have told us that they struggle to find time in their day to attend face-to-face
training. We have therefore started to develop our own online training that staff can
do remotely. We have also created study days where staff can complete a whole
portfolio of training in one day to minimise travel time and mileage costs.
Read more in the appendix on p.67.
Patient safety
Ensuring and improving safety for patients, children, young people and families is
central to our culture in Bristol Community Health. We have developed an open and
transparent culture where staff are good at reporting any concerns about quality via
our incident reporting system. We know that this is working well as we have high
levels of incident reports but low levels of harm – the sign of a healthy learning
culture. This is present across the three separate business units, adults and
corporate services, prison services (InspireBetterHealth) and children’s services
(Community Children’s Health Partnership) to help us to learn and improve. We
involve the people we serve in investigations whenever possible and have carried
out focus groups to look at some complex areas like the development of pressure
ulcers and how to prevent them.
The patient safety team have a strategy that describes how we will achieve
continuous improvement and this includes embedding SBAR (situation background
assessment and recommendation) training and simulation training.
Read more in the appendix on p.69.
Page 19 of 76Medicines management continues to be a key area of safety as there are many
challenges to delivering services in people’s homes and other settings like prison.
Work has focused on;
• Antibiotic stewardship to ensure that antibiotics are only prescribed when
appropriate
• The introduction of community drug authorisation and administration
charts to reduce missed medication doses following hospital discharge
• Improved training on safe medicines handling to minimise the risk of
harmful medicine related incidents
Read more in the appendix on p.74.
Pressure ulcer prevention
Proactive pressure injury prevention has been a high priority and in 2017/18 we
started working on a new pressure ulcer prevention strategy which aims to ensure all
our patients:
• Are assessed quickly for their risk of developing pressure injuries
• Are provided with equipment and care plans
• Understand their risk and what they can do to protect their skin themselves.
The wound care team has continued to support community clinicians in identifying
learning opportunities to improve patient care and wound management and have
invested in new equipment.
In response to patient feedback, a webpage for patients and the public regarding the
prevention of pressure ulcers has been developed. This encourages patients to be
involved in the management of their own conditions and develops the knowledge
and skills of carers:https://briscomhealth.org.uk/videos/how-to-prevent-pressure-
injuries/
Read more in the appendix on p.76.
Infection prevention and control
During 2017/18, the infection, prevention and control team has implemented their
strategy to engage and inform staff, infection prevention and control link
practitioners, patients, and the public to prevent infection.
At the end of this year, 92% of our clinical and 100% of our non-clinical staff were
up-to-date on their infection prevention and control training, against a target of 90%.
In 2017/18 we investigated 91 healthcare-associated infections. No significant trends
Page 20 of 76were identified, but we did identify learning from some cases and have made
changes to practice as a result such as the introduction of the catheter passport.
We have also created a dance video to engage staff and the public and remind them
about the key steps of hand hygiene: https://goo.gl/TMV6z6
Read more in the appendix on p.78.
Clinical supervision
Clinical supervision is essential for staff to improve their clinical practice and identify
any learning needs they might have. In 2017/18 89% of clinical staff were compliant
with Bristol Community Health clinical supervision policy. This is 4% higher than the
previous year. Our programme to enhance staff competence and confidence in
clinical supervision was achieved through the introductory and advanced level
courses.
• 54 staff members (mostly in senior roles) accessed the advanced level
training and are subsequently providing local and hands-on support to junior
and less experienced colleagues within various teams across the
organisation.
• Four clinicians have been trained and joined the pool of facilitators to support
delivery of the clinical supervision training and others have expressed an
interest.
We continued the facilitation and roll-out of action learning sets to various grades of
staff including one specifically held with team and service managers and sets to
support the development of advanced practice.
Our performance against key national indicators
There are a number of national indicators that are used to assess quality. The table
below shows Bristol Community Health’s performance against key national
indicators.
Indicator 2016-2017 2017-2018
Serious incidents requiring investigation 39 68
Never events 1 0
Incidence of falls 53 37
Incidence of pressure ulcers 872 873
Medication incidents 457 490
All patient safety incidents 2,089 1,946
Infection control pre-48 hour MRSA bacteraemia 1 2
Infection prevention and control clostridium 0 0
difficile infections leading to death or colectomy
Page 21 of 76This table demonstrates that most areas of potential harm have remained static or
reduced. Those incidents requiring investigation have risen however most of these
relate to patients developing pressure injuries and on investigation most have been
found to not be preventable, e.g. skin breakdown in palliative patients so BCH staff
had delivered all possible care.
Review of CQUIN goals: 2018/19
The commissioning for quality and innovation framework (CQUIN) is an incentive
scheme between providers and their commissioners aimed at fostering innovation
and improving quality in service delivery. In 2017/18, 2.5% of Bristol Community
Health’s contracts were linked directly to the achievement of CQUIN targets.
In 2017 CQUINs became nationally directed programmes of work that last two years.
Here we report on what these CQUINs are for 2017-2019 and what we have
achieved in this first year (2017/18).
CQUIN Our year-end position 2017/18
Improving staff health and wellbeing: We asked all staff about their wellbeing
asking staff about their wellbeing generally and any work-related stress or
generally and any work related stress or MSK problems and had over 1,000
musculo-skeletal (MSK) problems responses. We unfortunately did not
meet the targets for the number of
specified responses for the CQUIN
requirements. We have identified some
key areas for improvement and will be
working closely with staff to improve
these figures over the coming months.
Improving staff health and wellbeing: 69% of frontline staff across adults,
improving the uptake of the flu prisons and children’s services had the
vaccination among frontline staff flu vaccination. We report only against
adults services for the CQUIN, where we
achieved 77%, exceeding our target of
65%.
Supporting safe discharge: We achieved a 10% increase in the
demonstrating an increase in the number number of patients admitted via non-
of patients admitted via non-elective elective route discharged on Pathway 1.
route discharged on Pathway 1 (to their This far exceeded our target of 2.5%.
normal place of residence).
Preventing ill health caused by smoking Across the year, 97% of eligible patients
and alcohol use: screening all patients in were screened for smoking and 98% for
our intermediate care centres in the alcohol use. Since the CQUIN has
south and east for smoking and alcohol embedded, 100% of patients have been
use; providing brief advice, stop smoking offered subsequent interventions,
medications and referrals to specialist including advice, support and medication
support services, where appropriate. where appropriate. We have met or
exceeded all targets throughout the year.
Improving the assessment of wounds: 73% of the patients sampled in quarter 4
Page 22 of 76administering a full wound assessment received a full wound assessment. This
for all wounds that do not heal within four exceeded our target of 25%.
weeks.
Personalised care and support planning, We exceeded our target of 85% of staff
enabling patients to gain greater control trained in personalised care and support
over their health and wellbeing: planning and we also exceeded the 50%
developing skills, knowledge and target of the identified patient cohort
confidence. having received a baseline patient
activation measure.
4
To work with Healthier Together and be There were no quantitative targets set for
proactive in partnership working to the CQUIN related to Healthier Together
deliver the outcomes of the Rehabilitation but we have fulfilled three of the four
Delivery Board and the Integrated Care milestone requirements set throughout
Bureau Board. the year and await confirmation that we
have achieved the fourth.
Areas of consistently good or improved performance
Many of our key adults services have continued to see a growing demand
throughout 2017/18 and an increased number of referrals as a result. This has
added pressure within our teams but our clinicians have responded positively and
ensured the continued delivery of high-quality, safe services to patients whilst
achieving or exceeding targets.
“My experience was excellent. All my questions were
answered and in great detail. It was a very friendly and
pleasant experience - I feel so much better.” Patient,
Community Respiratory service, pulmonary rehabilitation
The following services stand out as having managed increased demand whilst
maintaining exceptionally high standards of care:
• Haven (service for refugees)
• Tuberculosis
• Chronic obstructive pulmonary disease (COPD)
• Admission avoidance and early supported discharge
• Bladder and bowel service
• Diabetic eye screening programme
Our services deliver value and quality through patients’ access to clinical care. We
set a 95% target for patients to be seen within 18 weeks and the following services
are examples of where we have achieved and exceeded the target at year end.
• Dermatology (100%)
• Heart Failure (99.6%)
4
Healthier Together is the name for the Bristol, North Somerset and South Gloucestershire
Sustainability and Transformation Partnership (STP).
Page 23 of 76• Learning Difficulties (95.8%)
• Podiatry (95%)
Over 90% of our patients seen by the enhanced palliative care home support service
were supported to die in their preferred place, thereby setting a high standard for the
quality measure of maintaining patient choice. This is an increase from 80% in
2016/17.
Over 90% of new assessments for continuing healthcare and funded nursing care
(FNC) by the Health Assessment and Review team were made within 28 days.
The performance data that has been collected from the children’s and offender
health services throughout 2017/18 has continued to improve. This has meant we
have been able to accurately benchmark our services and see improvements across
all areas of children’s and offender health services in the last two quarters.
We have met all performance targets for the National Child Measurement
Programme for the academic year 2016/17.
Our awards and achievements
Award nomination for Southmead community nursing team
The Southmead Community Nursing team were nominated in March 2018 for Mentor
of the Year at the University of the West of England. Despite a busy caseload and
being the largest community nursing team, these staff have been recognised for
always prioritising students and ensuring they have a positive experience.
Nurse invited to Buckingham Palace in recognition of frontline service
In March 2018, David Pugh, one of our nurses and a team leader, was invited by the
Queen to attend a reception at Buckingham Palace. The event was to celebrate
frontline nursing in the UK. David was representing Bristol Community Health and
also attending as a Queen’s Nurse, a title given by the Queen’s Nursing Institute to
those who have demonstrated a high-level of commitment to patient care and
nursing practice. David met HRH the Prince of Wales at the event.
New book on coordination published by paediatric occupational therapist
Rachel White has written a new book for parents and professionals called ‘Helping
Children to Improve Their Gross Motor Skills: The Stepping Stones Curriculum’. This
step-by-step programme enables children and young people with motor coordination
difficulties to master basic skills and develop their sporting ability. Activity worksheets
Page 24 of 76provide instruction on how to complete incremental exercises building up to the
achievement of a specific activity, such as climbing, riding a bike and playing
football. The book is published by Jessica Kingsley Publishers.
Many other staff have published articles on their specialist areas and spoken at
national conferences.
Page 25 of 76Innovation
Wound care service In-Reach model
“Cannot think of any way to improve your tender care!”
Patient, Wound Care service
Leg ulcers, wounds, pressure ulcers and their prevention represent a large part of
the community nurse’s workload. Education and training is provided on all these
aspects by the wound care specialist nurses. However it is recognised that to really
embed knowledge and become confident in this field, there is a need for ongoing
support and training. Early comprehensive assessment and appropriate treatment
plans lead to increased healing rates, improved patient outcomes and levels of
satisfaction for the staff and patients.
What we did
A new InReach model of working was developed where specialist nurses from the
wound care service started working regularly with the community nursing teams,
teaching and developing the nurses in proactive pressure ulcer prevention and the
use of SSKIN (a wound assessment tool that involves: looking at the Surface the
patient is on; Skin inspection; Keeping the patient moving; reviewing Incontinence
and moisture issues; and looking at Nutrition and hydration).
Outcomes
• There has been an overall 80% reduction in patients waiting for Doppler
(scans) assessment across the teams. This means patients are receiving
compression therapy earlier which in turn increases healing rates.
• There has been raised awareness for proactive ulcer prevention observed
by our specialist nurses working in all the teams.
• There has been an improved use of the electronic SSKIN template so
ensuring better consistent documentation. Through audit we have
demonstrated a rise in documentation of at-risk patients from 66% in
November 2015 to 100% in November 2017.
• Patients are receiving early intervention of specialist advice at the point of
contact rather than waiting for a referral to be submitted and processed.
• There is regular opportunity for teaching teams through joint assessments
so they are up to date with tissue viability issues. Community nurses report
how much this benefits their knowledge.
Feedback from staff in community teams has been positive and specialist nurses
have been welcomed into the teams. Staff have reported that they have found it very
useful having this contact with the tissue viability service. It has made specialist
advice more easily accessible and increased their confidence.
Page 26 of 76Community Navigators Bristol
What we did
In September 2017 we launched our new Community Navigator service, which is a
signposting and support service for people aged over 50 in Bristol. Its primary aim is
to reduce social isolation and loneliness in our over 50s population. The service is
delivered through a mixture of telephone and face-to-face support by a team of
Community Navigators, which includes both paid and volunteer staff. Navigators get
to know people and then conduct personalised research of activities, services and
groups that will be of interest to the individual. Navigators also help people overcome
barriers such as accessing transport or concerns about safety. If people need a little
extra support to access a new group or activity for the first time, the navigator can go
along to help improve confidence and self-esteem.
Outcomes
By the end of March 2018, we had received over 160 referrals from a wide range of
sources – including self-referrals, GPs, social workers, health staff and the police.
We have already visited over 60 people in their homes and provided telephone
advice and support to many more.
As well as our paid staff, we have recruited and trained 11 volunteer navigators who
visit and provide support to older people in Bristol.
We are developing plans to help us reach and support some of our isolated minority
communities and we are working alongside city-wide strategic groups for social
prescribing type services. We want to ensure that we create a robust and effective
service which will become an important part of the health and social care landscape
in Bristol and enable it to be commissioned beyond the end of the pilot in 2020.
Diabetic Eye Screening Programme
“It was a very good experience with only a short wait before I
was called, which was on time. The screener escorted me to
the correct room and explained the procedure. I cannot think
of anything that could make the experience any better. He was
pleasant and very professional.” Patient, Diabetic Eye
Screening Programme
What we did
The Diabetic Eye Screening Programme (DESP) team measures the number of
people with diabetes from each GP practice who attend for a yearly eye screening
appointment. The 2015/16 data showed that there were a number of practices where
Page 27 of 76You can also read