IL TRATTAMENTO FARMACOLOGICO DELLA DISMOTILITA' INTESTINALE NEL PAZIENTE CON SCI - GABRIELE BAZZOCCHI, M.D., PHD, A.G.A.F. MONTECATONE ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Gabriele Bazzocchi, M.D., PhD, A.G.A.F.
Neuro-Gastroenterology and G.I. Rehabilitation Unit
Montecatone Rehabilitation Institute
Imola (Italy)
Milano, 25 Novembre 2019
IL TRATTAMENTO
FARMACOLOGICO
DELLA DISMOTILITA’
INTESTINALE NEL
PAZIENTE CON SCI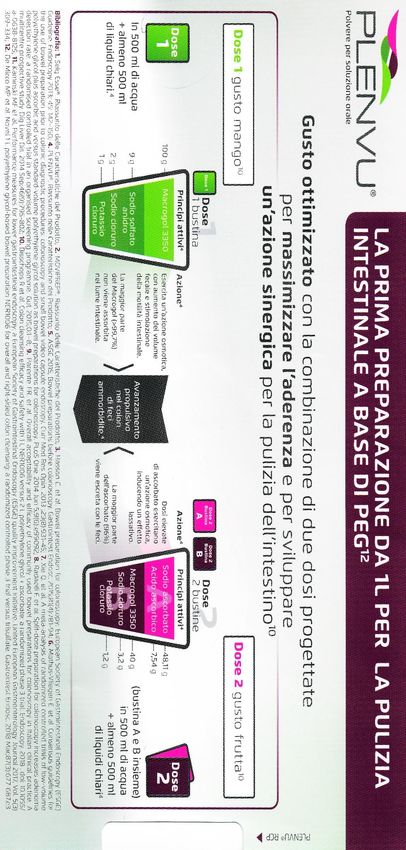
Intestinal evacuation is direct consequence of the
propagating contractions (HAPC) action
Repeated HAPC associated with an urge to defecate and the defecation
Bazzocchi G et al. Gastroenterology 1991; Herbst F et al. GUT 1997; 41: 381-389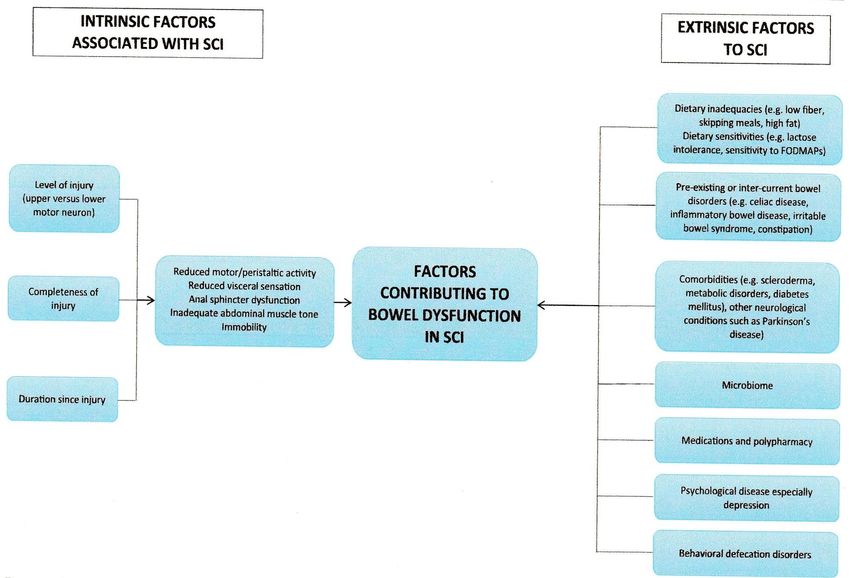
Propagating High Amplitude
Contractions (HAPC) induce the
principal ab-oral transport of the
intraluminal colonic contents
Rapid
scintigraphic scans
(1-min interval)
showing transport
from the right colon
into the rectum during
HAPC
min +67 +68 +69
Bazzocchi G et al. Gastroenterology 1991
Colorectal transport during defecation in subjects with supraconal spinal cord injury
Rasmussen MM et al. Spinal Cord 2013; 51: 683- 7
Normal subject
Before defecation After defecation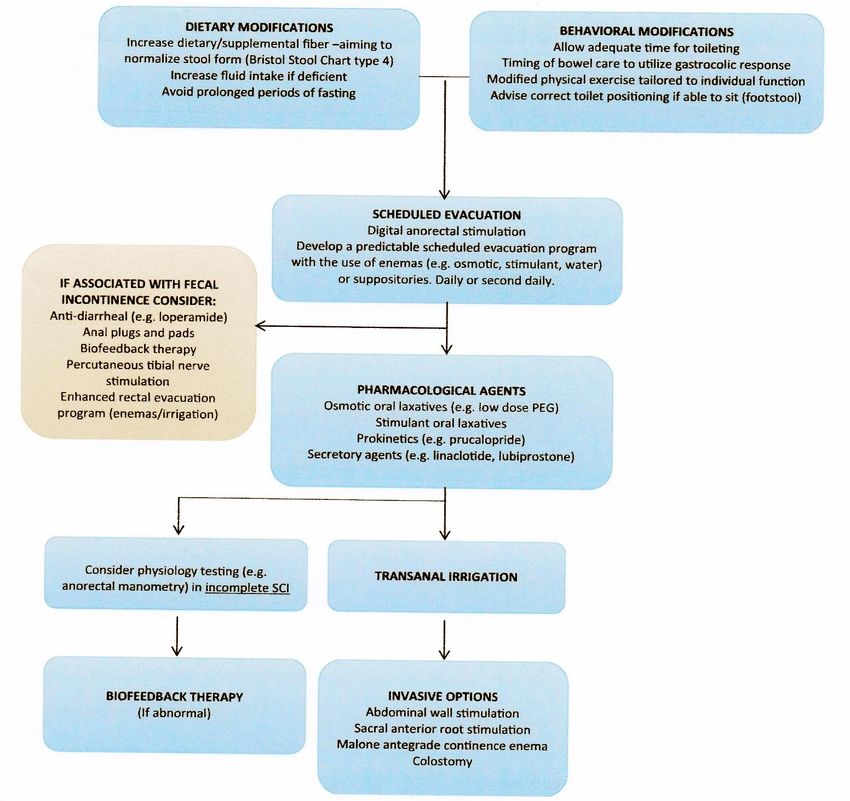
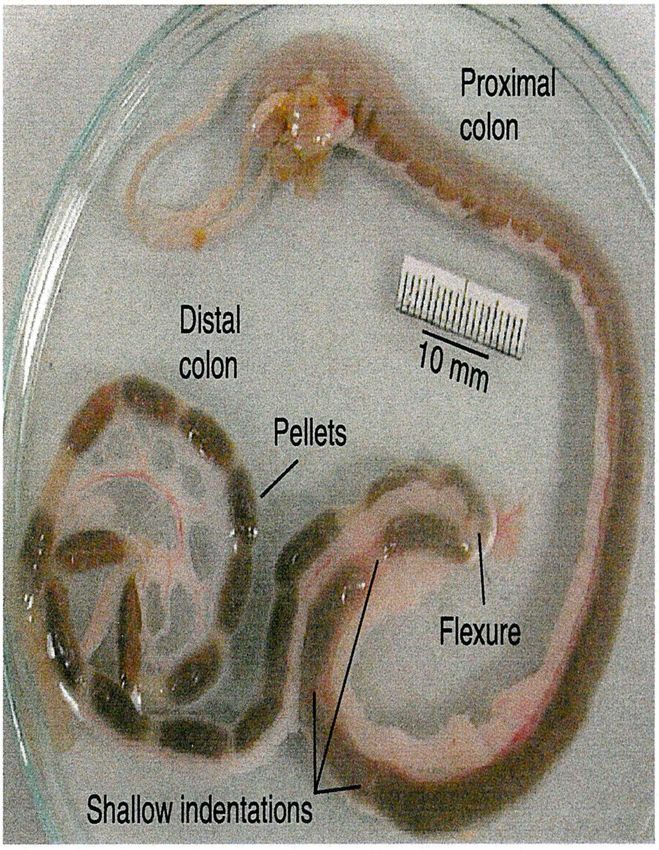
The Guinea-pig proximal colon, colonic flexure, and distal colon, removed from freshly killed animal and showing the normal appearance of fecal contents Costa M et al. Neurogastroenterol Motil 2015
THE ENTERIC NERVOUS SYSTEM: THE SECOND BRAIN
~ 50 transmitters / modulators / messengers
(i.e. amines, neuropeptides, gases, etc…)
~ 20 subclasses of functionally distinct neurons
(i.e. IPANS, interneurons, motorneurons, etc…)
various integrated reflex pathways
(i.e. Peristalsis, MMC, secretomotor reflexes, etc…)
neuroplasticity
(i.e. maintenance and repair)
De Giorgio R., et al., TiPS, 2007; 28:473-81
submucous
plexus as a third and distinct division of the
myenteric Autonomic Nervous System along with
5x 108 neurons (humans) plexus the sympathetic and parasympathetic
divisions
Camilleri M et al. Nature Reviews 2017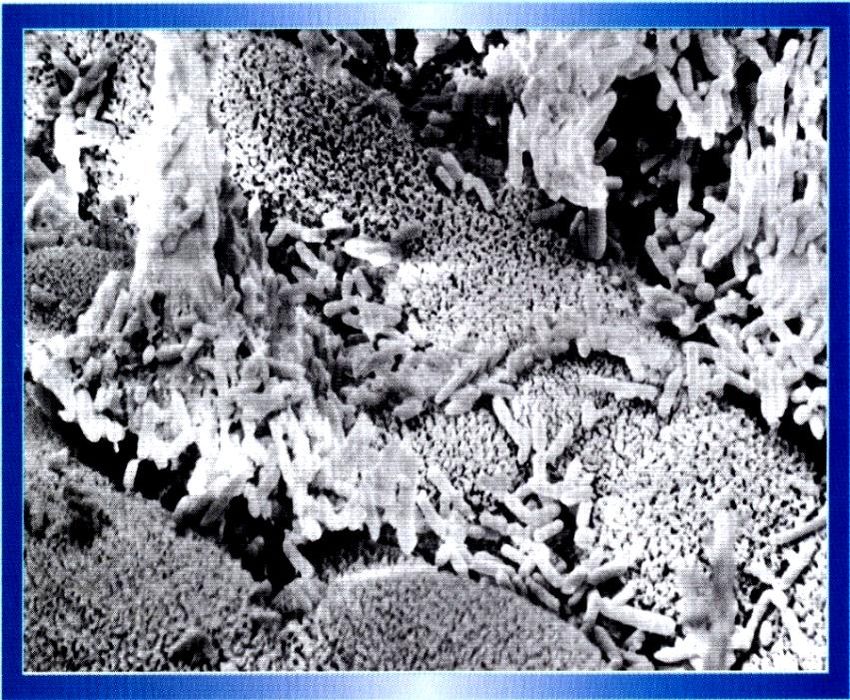
MECHANISMS UNDERLYING COLONIC MOTOR PATTERNS
Spencer NJ et al. J Physiol 2016; 594: 4099-4116
Mechanosensory enteric neurons
have essential mechanosensitive
nerve endings in the circular
muscle.
Distension or stretch of the colon
activates these sensory neurons to
initiate polarized neural pathways
that result in oral contraction and
anal relaxation.
These pathways do not require the
mucosa but can be modulated by
sensory nerve endings that project
into the mucosa.
The polarized enteric circuits form
the bases of a neuromechanical
loop which ensures that polarized
enteric neural circuitry can
efficiently propel content with a
wide range of physical properties.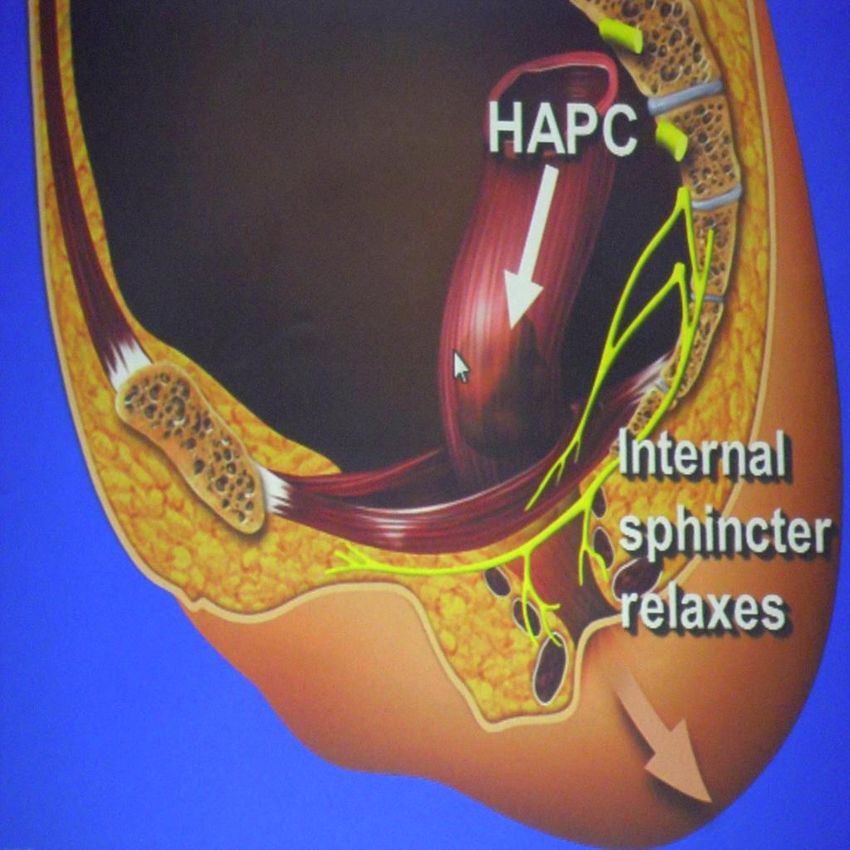
NEUROMECHANICAL FACTORS INVOLVED IN
THE
FORMATION AND PROPULSION OF FECAL
PELLETS IN THE GUINEA-PIG.
PROPULSION IS NOT A SIMPLE
Costa M et al. Neurogastroenterol Motil 2015 REFLEX BUT RATHER A MORE
COMPLEX PROCESS INVOLVING AN
ADAPTABLE NEUROMECHANICAL
LOOP
……..BOLUS SIZE AND
CONSISTENCY AFFECTS
PROPULSION SPEED…
Distension of the descending colon induces increase in rectal tone in
pts with SCI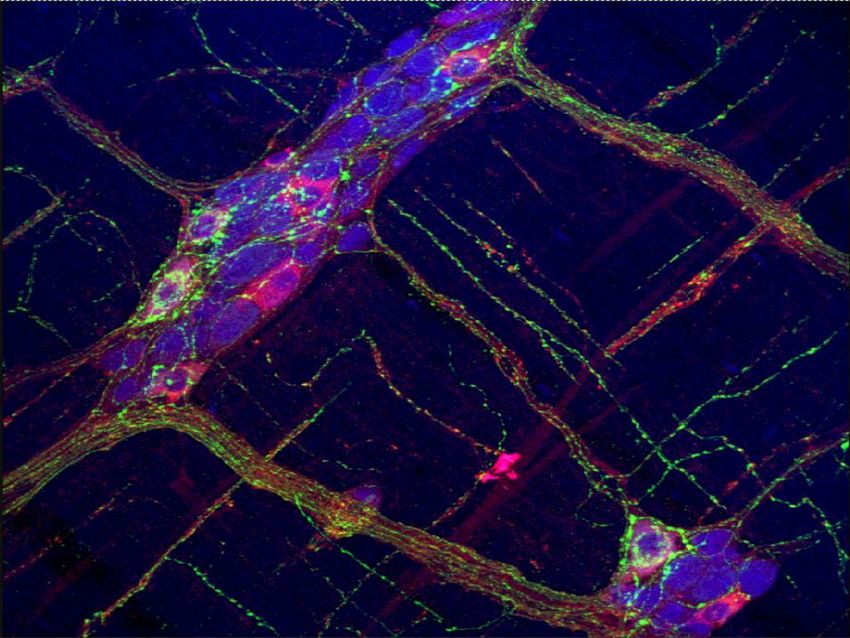
Factors associated with successful decrease and discontinuation of
Antegrade Continence Enemas (ACE) in children with defecation disorders:
a study evaluating the effect of ACE on colonic motility
Colon motility tracing demonstrating
improvement of HAPCs:
(A): Normalization of HAPCs from partial to
full propagation
(B): Normalization of HAPCs from absent to full propagation
Liem O et al. Neurogastroenterol Motil 2010COLONIC MOTILITY DURING RECTOCLYSIS
irrigationPATIENTS
16 SCI pts, 10 tetraplegic,
ASIA A post-traumatic lesion
50 cms
40 cms
20 cms Intraluminal pressure recording points
10 cms
30 cms
Internal Anal Sphincter
30 min later manometric probe was placed into the
colonic lumen, a Trans Anal Irrigation procedure using
Peristeen® device was performed according to the
following protocol:
Bazzocchi G et al. Pelviperineology 2012; 31: 85-92LEFT COLON MANOMETRY during TRANS ANAL IRRIGATION
50 cm
40 cm
30 cm
20 cm
10 cm
SAI
Catheter balloon
Irrigation
initiation water
Bazzocchi G et al. Pelviperineology 2012; 31: 85-92Abdominal x-ray film in a Abdominal x-ray film in the
pts with SCI after 6 days previous patient (CF) after
where 10 radioopaque only one
markers were taken daily. TRANS ANAL IRRIGATION
session
Patient (CF) had only 1
by means of Peristeen
bowel movement during
study weekTransanal irrigation
Before irrigation After irrigation
Anterior view of the 111In-labeled bowel content before washout (A) and after (B):
the colon is empty anal to the left colic flexure
Christensen P et al. Dis Colon Rectum 2003: 46:68-76 Laboratory animals are tetrapedal
They do not stop normal activity to defecate
They do not adopt a defecatory posture
Humans normally retain feces and defecate only
intermittently
Differences in the structure and functional
characteristics of the pelvic floor of humans compared
with tetrapods reflect its important role in continence
imposed by an upright postureConstipation
Pelvic Floor Musculature
At rest Straining to defecate
Symphysis
pubis
Coccyx
Anorectal
angle Anorectal
Puborectalis angle
Rectum
External
anal
sphincter Descent of
pelvic floorThe nerve pathways for voluntary control
of defecation and fecal continence
GUT innervation by ANS ce
BN: Barrington’s nucleus;
LCG: Lateral Cell Group;
IML: InterMedioLateral column;
ENS: Enteric Nervous System;
Pelv gang: pelvic ganglia; 2 ord: second order neurons;
ON: Onuf’s nucleusNORMAL COLONIC MOTILITY NORMAL ANORECTAL
SENSATION
NORMAL DEFECATION
NORMAL RECTAL
EXPULSION FORCENORMAL ANORECTAL
NORMAL COLONIC MOTILITY SENSATION
NORMAL DEFECATION
COORDINATED
NORMAL RECTAL
ABDOMINAL- PELVIC
EXPULSION FORCE
and PERINEAL
NEUROMUSCOLAR
FUNCTION TO
EVACUATENORMAL COLONIC MOTILITY NORMAL ANORECTAL
SENSATION
NORMAL DEFECATION
COORDINATED
NORMAL RECTAL
ABDOMINAL- PELVIC
EXPULSION FORCE
and PERINEAL
NEUROMUSCOLAR
FUNCTION TO
EVACUATE NORMAL
Colonic intraluminal
content:GUT MICROBIOTA: THE MOST
DENSE AND COMPLEX
BACTERIAL ECOSYSTEM ON
THE PLANET EARTH
Bengmark S. Gut 1998
Sender R et al. PLoS Biol 2916
BACTERIA ARE THE MAJOR COMPONENT
200 billions/g → OF FORMED STOOL
contributing of 0.5-1.0 kg
of the average adult’s body weightCONSTIPATION CAN BE THE
CONSEQUENCE OF
DISTURBANCE OF THE
MICROBIOTA BALANCE
Quigley EMM. The enteric microbiota in the
pathogenesis and management of
constipation. Best Practice &Research
Clinical Gastroenterology 2011
Rhee SH et al. Principles and clinical
implications of the
Brain-Gut-Enteric Microbiota Axis.
Nature Reviews Gastroenterology &
Hepatology 2009
Quigley EMM et al. Constipation and the
microbioma: lumen versus mucosa.
Gastroenterology 2016; 150: 300-303
“AN EMPY COLON HAS
NO MOTOR ACTIVITY”
Costa M et al.
Am J Physiol Gastrointest Liver Physiol 2013IN PTS WITH SLOW TRANSIT CONSTIPATION HAPC OCCURRENCE IS
SIGNIFICANTLY REDUCED AFTER MEAL (M) AND DURING AWAKENING (A)
Bazzocchi G et al. Gastroenterology 1991; 98: 686-93
Bassotti G et al. World J Gastroenterol 2005; 11: 2691-6.Neurogastroentero Motil 2011
There were no HAPC observed in the SCI group during pre-sleep, sleep, and post-sleep phases. All non-SCI subjects experienced subjective symptoms (e.g. sensation of flatus) and two had bowel movements in close proximity to having HAPC in the post-sleep phase.
Abdominal X-RAY in ♀ with p.t. paraplegia
Scintigraphic study showing defecation produces a complete emptying of the
left colon in normal subjects, but not in SCI
Before defecation After defecation
Normal
(Score = 81 (53-140)
SCI
(Score = 27 (0-44)
Rasmussen MM et al. Spinal Cord 2013; 51: 683- 7COLONIC TRANSIT STUDY WITH RADIOPAQUE MARKERS
IN A PATIENT WITH P.T. PARAPLEGIA
Patient reported daily bowel
movements during the 7 day study
period.
N° of markers ingested = 60
N° of markers in the large bowel on
the 7th day = 53
Total Transit Time = 127.2 hours
(n.v.COLONIC TRANSIT in SCI:
differentiate transport for
fluid and hard stool through
the large bowel
Radiopaque markers are
not inserted in the
formed/hard stoolsPathophysiology of Bowel Dysfunction in Spinal Cord Injury
There are intrinsic factors associated with the injury itself which disrupt normal motor and sensory
functions within the g.i. tract. Additional external factors may influence bowel disorders.
Qi Z et al. Bowel management in Spinal Cord Injury. Curr Gastroenterol Rep 2018BOWEL DYSFUNCTION in SCI
- GENERAL DECREASE IN MOTOR DELAYED COLONIC
ACTIVITY IN THE COLONIC TRACTS TRANSIT TIME
(LACK OF HAPC?)
- VISCERAL SENSORY LOSS
- ABDOMINAL MUSCLE
INCOMPLETE
INSUFFICIENCY EVACUATION
ANORECTAL
- DEFECT IN THE STRIATED
OUTLET
MUSCLE CONTROL
- RECTO-ANAL INHIBITORY DYSFUNCTION
REFLEX IS MAINTAINED
FORMATION OF POST-
EVACUATION FECAL
NOT SCHEDULED
RESIDUES AND THEIR
(UNWANTED)
ACCUMULATION
DEFECATION
FECAL
INCONTINENCE/
SOILING FECAL IMPACTION
IN THE LARGE
BOWELManagement of neurogenic bowel dysfunction manifesting as constipation and fecal incontinence
Qi Z et al. Bowel management in Spinal Cord Injury. Curr Gastroenterol Rep 2018Management of neurogenic bowel dysfunction manifesting as constipation and fecal incontinence
Antispasmodics
Antimeteorics
Prebiotics
Probiotics
Synbiotics
AntibioticsManagement of neurogenic bowel dysfunction manifesting as constipation and fecal incontinence
loperamide?
anal plugs?
Cholestyramine
Antispasmodics
Antimeteorics
Prebiotics
Probiotics
Synbiotics
AntibioticsFECAL RETENTION / COPROSTASIS / CONSTIPATION
Colonic hypo-dysmotility
DISORDERS of PERISTALSIS
Decrease of HAPC
Diseases of the Enteric Nervous System Disorders of retrograde
propulsion
Changes in regulation by external signals Alterations in regional
wall tone
Reduced fecal volume and changes in stool
consistencyFECAL RETENTION / COPROSTASIS / CONSTIPATION
Colonic hypo-dysmotility
MEDICAL and REHABILITATION APPROACH
- Poliethylene glycol (macrogol)
- Stimulant laxatives: sodium picosulphate, bisacodyl, sennosides
- Prokinetic drugs: prucalopride, linaclotide, neostigmine, trimebutine
- Water consumption (!??)
- Dietary (hydrosoluble) fiber supplementation
- Prebiotics
- Probiotics, symbiotics
- Lactulose, lactilole
- Digital rectal stimulation
- Abdominal massage
- Mechanical distention of the colonic wall: COLONIC IRRIGATION
SURGERY ?Physical factors in the stimulation
of colonic peristalsis
Hardcastle JD, Mann CV. Gut 1970; 11: 41-46Bisacodyl and High-Amplitude-Propagating Colonic Contractions
in Children
Hamid SA, Di Lorenzo C, Reddy SN, Alex F, Hyman P . J Pediatr Gastroenterol Nutr 1998POLYETHYLENE GLYCOL solution
MACROGOL 3350/electrolyte improves constipation in
Parkinson’s disease and multiple system atrophy
Eichhorn TE, Oertel WH. Mov Disord 2001; 16: 1176-7
Long term efficacy, safety, and tolerabilitity of low daily doses of
isosmotic polyethylene glycol electrolyte balanced solution
(PMF-100) in the treatment of functional chronic constipation.
Corazziari E, Badiali D, Bazzocchi G et al. Gut 2000; 46:522-6.
Polyethylene glycol solution in subgroups of chronic
constipation patients: experience in obstructed defecation.
Bazzocchi G. Ital J Gastroenterol Hepatol 1999; 31: S257-9PRODOTTI a base di PEG
NOME (AIC) FORMULAZIONE INDICAZIONE
MOVICOL 20 buste (1 in 125 ml) Stipsi cronica idiopatica
PEG 3350 (13,125 g) + E (NaCl, e secondaria; fecaloma
(Norgine)
KCl, Ca2Na)
MOVICOL Stipsi cronica idiopatica
SENZA AROMA 20 buste (1 in 125 ml) e secondaria; fecaloma
(Norgine) PEG 3350 (13,125 g) + E
MOVICOL
Flacone da 500 ml Stipsi cronica idiopatica
CONCENTRATO
PEG 3350 (13,125 g) + E e secondaria
(Norgine)
MOVICOL
SOLUZIONE 20 buste da 25 ml Stipsi cronica idiopatica
ORALE e secondaria; fecaloma
PEG 3350 (13,125 g) + E
(Norgine)
MOVICOL 20 buste (1 in 62,5 ml) Stipsi cronica nei
BAMBINI PEG 3350 (6.9 g) + E bambini da 2 a 11 anni.
Fecaloma nei bambini
(Norgine) sopra i 5 anni.
MOVICOL Stipsi cronica nei
20 buste (1 in 62,5 ml) bambini da 2 a 11 anni.
BAMBINI
PEG 3350 (6.9 g) + E Fecaloma nei bambini
SENZA AROMA
sopra i 5 anni.
(Norgine)PRODOTTI a base di PEG
NOME (AIC) FORMULAZIONE INDICAZIONE
SELG 250 16 buste (1 in 250 ml) Trattamento della
stitichezza
(Alfa Wassermann)
PEG 4000 (14,8 g) Bambini di peso superiore
+ E + solfato di sodio ai 20Kg
ISOCOLAN 8 buste (1 in 250 ml) Trattamento della
stitichezza
(Zambon)
PEG 4000 (17,4)
+ E + solfato di sodio
COLIREI 16 buste (1 in 250 ml) Pulizia dell’intestino prima
di indagini diagnostiche o
Abc (in concessione interventi chirurgici sul
a Sofar) PEG 4000 (14,8 g)
colon-retto. Trattamento
+ E + solfato di sodio saltuario della stipsi
funzionale.
PERGIDAL 20 buste (1 in 125 ml) Trattamento della
stitichezza
(Valeas)
PEG 4000 (7,3 g)
+ E + solfato di sodioPRODOTTI a base di PEG
NOME (AIC) FORMULAZIONE INDICAZIONE
PAXABEL 20 BUSTE Trattamento
sintomatico della
(Ipsen) stipsi nell’adulto e nel
PEG 4000 (10 g) (1 in 125 ml)
bambino (6 mesi – 8
anni)
PEG 4000 (4 g) (1 in 50 ml)
LAXIPEG Polvere barattolo 200g Trattamento di breve
durata della
(Zambon) stitichezza
20 buste 9,7 g
occasionale
PEG 4000
REGOLINT Polvere barattolo 200 grammi Trattamento della
stitichezza nel
(Baldacci) bambino
20 buste da 9,7 grammi
Trattamento di breve
durata della
PEG 4000 stitichezza
occasionale
CASENLAX 20 buste 10g Trattamento
sintomatico della
(Recordati) stipsi
PEG 4000ULTIMEa NOVITA’
PRODOTTI base di PEG
NOME (AIC) FORMULAZIONE INDICAZIONE
ONLIGOL 20 BUSTE 10g Stitichezza cronica o
intestino occasionalmente
(Alfawassermann) irregolare
Flacone polvere 400g
Dispositivo Medico PEG 4000
SANIPEG 300g barattolo Trattamento sintomatico
20buste 4g della stipsi
Sanitas
20 buste 10
Dispositivo Medico PEG (non specificato)
CLIN 4000 Barattolo 200g Stitichezza cronica o
30buste 10g intestino occasionalmente
Akkadeas irregolare
PEG 4000
Dispositivo Medico
MACROGOL 20 buste 13,8g Stitichezza cronica;
GENERICI fecaloma
PEG 3350 + E
Mylan (Goganza)/
Sandoz/
Carlo Erba….A safe and effective multi-day colonoscopy bowel preparation for
individuals with spinal cor injuries
Song SH et al. J Spinal Cord Med 2018
Day 1:
- Start clear liquid diet at dinner
- Magnesium citrate 480 ml after dinner
Day2:
- Continue clear liquid diet
- PEG 3350 and electrolyte colonic lavage solution (PEG-ELS) 4L over 2 hours in the
morning
Day 3:
- Continue clear liquid diet until midnight, then nothing per os
- PEG-ELS over 2 hours in the morning
Day 4: - Is rectal/colostomy output clear?
YES NO
READY FOR COLONOSCOPY
PEG-ELS 2L PRIOR COLONOSCOPY Colonic intraluminal contents have a sub- stantial effect on colonic transit In female controls bowel cleansing shortened rectosimoid transit Women with constipation had faster transit in the cleansed state, however, the distribution of markers was not altered: DELAYS in TRANSIT TIME were still present in the same colonic tract
PROKINETICS DRUGS Neostigmine Prucalopride Linaclotide Cisapride Domperidone Trimebutine Levolsulpiride Erythromycin Misoprostol
Neostigmine reduced the time to first flatus, time to start of bowel movement, time to end of bowel movement, and time for total bowel care as compared to placebo INTRASTIGMINA f. 1 ml, 0.5 mg TID
PRUCALOPRIDE 2 mg significantly reduced total colonic transit time in patients with supraconal SCI This reduction in transit time was also associated with an increase in the weekly frequency RESOLOR 2 mg cpr, 1 cpr 5 hours before scheduled evacuation
Effect of 5 days linaclotide on transit and bowel
function in females with constipation-
predominant Irritable Bowel Syndrome.
Andresen V. et al. Gastroenterology 2007; 133: 761-8
CONSTELLA 290 mg, caps, 30 min before breakfast or lunchPROKINETICS DRUGS Neostigmine Prucalopride Linaclotide Cisapride Domperidone Trimebutine Levolsulpiride Erythromycin Misoprostol
- Intravenous administration of 100 mg trimebutine was followed,
Poynard T. et al. TRIMEBUTINE and IBS
META-ANALYSIS OF SMOOTH MUSCLE RELAXANTS IN THE
TREATMENT OF IBS
-1888 pts, 23 randomized clinical trials
- global assessment, pain, abdominal distension, constipation improved
significantly with cimetropium, mebeverine, otilonium, pinaverium and trimebutine
APT 2001; 15: 355-61
Rahman MZ et al.
COMPARATIVE EFFICACY AND SAFETY OF TRIMEBUTINE
VERSUS MEBEVERINE IN THE TREATMENT OF IRRITABLE
BOWEL SYNDROME
-IBS-QOL was assessed in 122 pts with IBS before and after 6 weeks of treatment
with trimebutine 100 mg b.i.d. or mebeverine 135 mg b.i.d.
- QOL score decreased from 103 to 82 in trimebutine and from 106 to 95 in
mebeverine group: improvement in both groups was statistically significant, as the
difference between the two groups.
Mymensingh Med J 2014; 23: 105-13LEVOSULPIRIDE IN IBS
Lanfranchi GA, Bazzocchi G, Marzio L et al.
INHIBITION OF POSTPRANDIAL COLONIC MOTILITY BY SULPIRIDE IN
PATIENTS WITH IRRITABLE COLON
- administration of sulpiride 100 mg i.m. significantly reduced the postprandial increase in colonic motor
activity
- dopaminergic receptors may be involved in the colonic motor response to food
Eur J Clin Pharmacol 1983; 769: 772LEVOSULPIRIDE IN IBS - Levosulpiride 25 mg t.i.d. for 10 days accelerate colonic transit time more than placebo in 20 pts with Functional Constipation or IBS
- Levosulpiride was better than domperidone in improving 6 out
of 10 recorded symptoms, and was better than metoclopramide
in improving 6 out of 10 selected symptoms
anorexia
nausea
vomiting
upper abdominal pain
postprandial bloating
abdominal fullness
early satiety
belching
heartburn
regurgitation
LEVOSULPIRIDE 25 mg 30 min before mealsAdvantages of Azithromycin Over Erythromycin in Improving the
Gastric Emptying Half-Time in Adult Patients With Gastroparesis
Jean M Larson et al.
J NEUROGASTROENTEROL MOTIL 2010; 16: 407-413
Erythromycin 250 mg f, 1 f i.v. TID
ERITROCINA 200 mg cpr masticabili
ERITROCINA 10% granulato sosp oraleCYTOTEC 200 µg, 2 cpr TID
QUESTRAN 4 gr polvere x sosp orale, 1 busta ad ogni pasto
Management of neurogenic bowel dysfunction manifesting as constipation and fecal incontinence
loperamide?
anal plugs?
Cholestyramine
Antispasmodics
Antimeteorics
Prebiotics
Probiotics
Synbiotics
AntibioticsPrimary endpoints: - bowel evacuations with normal stool consistency - Intestinal Transit Time Secondary endpoints: - Symptoms according to Rome III Diagnostic Criteria - Agachan-Wexner score - Changes in gut microbiota composition
abdominal bloating
No effect on pain, gas, urgency
flatulence
colonic transit
Mean BSFS scores and
CSBMs/week increased in
FCGUT DYSBIOSIS IMPAIRS RECOVERY AFTER SPINAL CORD INJURY
In mice with experimental SCI,
the pre-existence of intestinal
dysbiosis caused larger lesions
to form after injury.
Kigerl KA et al. J Experim Med 2016;
213: 2603-20
Probiotics (VSL#3) confer neuroprotection and improve locomotor recovery after SCI
In an effort to develop a clinically feasible therapeutic protocol, SCI mice received VSL#3 probiotics starting immediately
after injury and then again daily until 35 dpi. In VSL#3-treated SCI mice, locomotor recovery was significantly improved
relative to vehicle-treated SCI mice. VSL#3 increased the frequency of plantar stepping and fore limb–hind limb
coordination with concomitant improvements in paw position and trunk. VSL#3 also reduced lesion volume and
axon/myelin pathology at the injury epicenter. Smaller lesion volumes in the VSL#3-treated mice correlated with
improved behavioral recovery.Alpha diversity (i.e. biodiversity) of the GUT MICROBIOTA from 100 pts with
SCI and 100 healthy subjects matched for age and sex.
A stool sample was collected during the first week after admission to 10 Spinal Units scattered all
over the Italian territory
p=0.001 ***Diversity of the GUT MICROBIOTA structure
Diversity of the GUT MICROBIOTA between pts showing greater severity of
STRUCTURE between pts with AIS score A the SCI (cervical or thoracic lesional level
or B vs pts with AIS score C or D with AIS score A or B) vs pts with minor
severity (AIS score C or D or lumbar level)
p=0.029*
p=0.036 *Fecal microbiota transplantation in spinal cord injury. Brechmann T et al. WJG 2015 Amount of fresh feces prepared for infusion or infused fecal suspension: from 30 to 250 g of fresh stool in 30 to 700 mL. Number of FMT regimens: from single treatments to 14
TAKE HOME MESSAGE Gli studi che valutano efficacy/safety di farmaci potenzialmente utili nel trattamento dei disturbi intestinali dopo mielolesione sono ancora troppo pochi L’evidenza di un overlap tra la disfunzione intestinale nella persona con patologie del SNC e quella della popolazione con disturbi «funzionali» autorizza all’impiego di numerosi farmaci per ben specificati obiettivi terapeutici Per le specificità, in termini di complessità dei problemi e tempi, del trattamento medico/riabilitativo di cui necessita una persona con SCI, i Prontuari Ospedalieri di cui siamo dotati non sono adeguati La cura della disfunzione intestinale dopo SCI mostra di essere cruciale ai fini della morbidità e QoL di questi pazienti
You can also read