Innovative Clinical Programs Targeting the Tumor Microenvironment to Improve Therapeutic Outcomes in Underserved Solid Tumors - July 2020 ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Innovative Clinical Programs Targeting the Tumor Microenvironment to Improve Therapeutic Outcomes in Underserved Solid Tumors July 2020
Forward-looking Statements
The information and opinions contained in this presentation and any other information discussed at this presentation are provided as at the
date of this presentation and are therefore of a preliminary nature, have not been independently verified and may be subject to updating,
revision, amendment or change without notice and in some cases has not been audited or reviewed by the Company’s auditors. This
presentation is selective in nature and does not purport to contain all information that may be required to evaluate the Company and/or its
securities. Neither the Company nor any other person is under any obligation to update or keep current the information contained in this
presentation or to correct any inaccuracies in any such information which may become apparent or to provide you with any additional
information. No reliance may or should be placed for any purpose whatsoever on the information contained in this presentation, or any other
information discussed verbally, or on its completeness, accuracy or fairness. None of the Company, its investment banking representatives,
or any of their respective directors, officers, employees, direct or indirect shareholders, agents, affiliates, advisors or any other person
accept any responsibility whatsoever for the contents of this presentation, and no representation or warranty, express or implied, is made by
any such person in relation to the contents of this presentation.
Certain information in this presentation is based on management estimates. Such estimates have been made in good faith and represent
the current beliefs of applicable members of management. Those management members believe that such estimates are founded on
reasonable grounds. However, by their nature, estimates may not be correct or complete. Accordingly, no representation or warranty
(express or implied) is given that such estimates are correct or complete. Where this presentation quotes any information or statistics from
any external source, it should not be interpreted that the Company has adopted or endorsed such information or statistics as being
accurate. This presentation contains forward-looking statements. These statements reflect the Company’s current knowledge and its
expectations and projections about future events and may be identified by the context of such statements or words such as “anticipate,”
“believe”, “estimate”, “expect”, “intend”, “plan”, “project”, “target”, “may”, “will”, “would”, “could”, “might” or “should” or similar terminology. By
their nature, forward-looking statements are subject to a number of risks and uncertainties, many of which are beyond the Company’s
control that could cause the Company’s actual results and performance to differ materially from any expected future results or performance
expressed or implied by any forward-looking statements. The Company undertakes no obligation publicly to release the results of any
revisions to any forward-looking statements in this presentation that may occur due to any change in its expectations or to reflect events or
circumstances after the date of this presentation.
2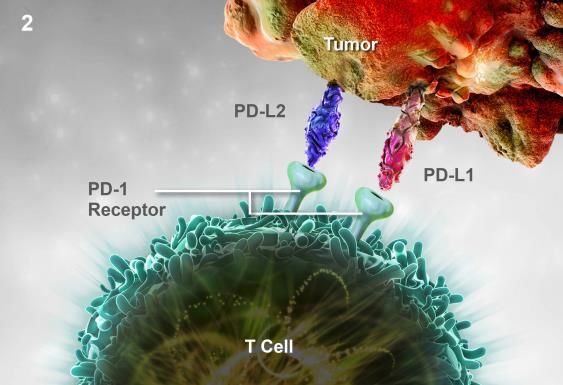
NOXXON Overview
NOXXON is a biotechnology company focused on improving
cancer treatments
Cancer drug candidates NOX-A12 & NOX-E36 target the
tumor microenvironment (TME)
NOX-A12 + Immunotherapy combination in metastatic colorectal and
pancreatic cancer patients
NOX-A12 + Radiotherapy in 1st line brain cancer patients (glioblastoma)
NOX-E36 shows monotherapy activity in preclinical solid tumor models
Strong IP position with patent families covering NOX-A12 & NOX-E36
Committed team with clinical, regulatory and business development experience
3
Pipeline Assets Leverage Existing Anti-Cancer Therapies
to Optimize their Therapeutic Efficacy
NOX-A12
Indication Combination Preclinical Phase 1 Phase 2 Phase 3
Scientific
Collaborator Phase 1/2 trial completed
Solid tumors
Immunotherapy Top-line update published April 2020
Pancreatic / Colorectal • Phase 2 at planning stage
Orphan
Solid tumors Ablation Phase 1/2 trial initiated in Sept. 2019
Status
Brain cancer / Glioblastoma / radiation • 1st cohort top-line data Oct-2020
US & EU
• 2nd & 3rd cohort top-line data end-Q1-2021 & mid-2021
Top-10 Undisclosed
Ongoing preclinical evaluation
Pharma Market >€1b
NOX-E36
Indication Combination Preclinical Phase 1 Phase 2 Phase 3
Solid tumors Immunotherapy & Phase 1 & 2a trials completed in
Pancreatic / Liver chemotherapy non-oncology indications
Trial to be completed by Noxxon Trial to be completed with a partner
All timelines subject to financing and patient recruitment
4
Team with Strong Commitment
Dr. Aram Mangasarian Dr. Jarl Ulf Jungnelius Dr. Don deBethizy
CEO Senior Medical Advisor Board Member, Finance/M&A Lead
▪ 20 years biotech experience in EU, ▪ Oncologist with 25+ years clinical and ▪ Chairman of Albumedix, Board member of
transformed NOXXON into a lean research experience in large pharma and arGEN-X NV, Newron Pharma SPA,
oncology-focused company listed on academic organizations Proterris
Euronext Growth ▪ CEO at Isofol Medical ▪ Formerly CEO of Santaris Pharma
▪ Headed Business Development at Novexel ▪ Leadership positions at Celgene, Pfizer, (sale to Roche), Chairman of Rigontec
- €150m licensing deal with Forest Labs on Takeda and Eli Lilly & Company (sale to Merck & Co./MSD), Chairman
avibactam; company bought by ▪ Significant role in the approval of multiple Contera Pharma ApS, Serendex A/S
AstraZeneca for $505m successful oncology drugs including ▪ Co-founder and former CEO of Targacept
▪ Ran Business Development at ExonHit Abraxane®, Gemzar®, Alimta® and
Therapeutics; closed $30m discovery and Revlimid®
development alliance with Allergan
▪ Bertram Köhler ▪ Dr. Maurizio PetitBon ▪ Dr. Don deBethizy ▪ Dr. Oscar Izeboud
Formerly
Supervisory
Board
5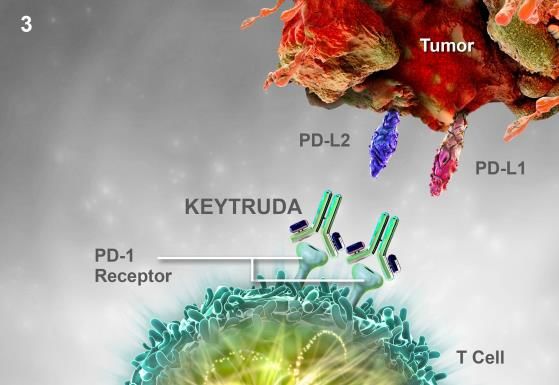
NOX-A12 + Radiotherapy

NOX-A12: Attacking Brain Cancer by Blocking Key Survival
Mechanisms Following Radiotherapy
SUPERIOR PHARMACOLOGY CD11b monocytes
Direct targeting of CXCL12
provides more complete VASCULOGENESIS
inhibition of axis than CXCR4 Main driver of new vessel CXCR4 receptor
or CXCR7 antagonists formation after radiotherapy
CXCR7 receptor
Radiotherapy NOX-A12
Endothelial Cells
Tumor Attraction to
CXCL12 CXCL12
chemokine
Hypoxia
HIF-1
HIF-1 Triggers the two
main pathways to re-grow VEGF
blood vessels:
Vasculogenesis &
Angiogenesis.
ANGIOGENESIS
RADIOTHERAPY kills many tumor Limited / no ability to trigger
cells and destroys blood vessels in new vessel formation
irradiated zone leading to lack of following radiotherapy
oxygen (hypoxia) in the tumor
Inhibition of the CXCL12/CXCR4/CXCR7 axis can block tumor vasculogenesis
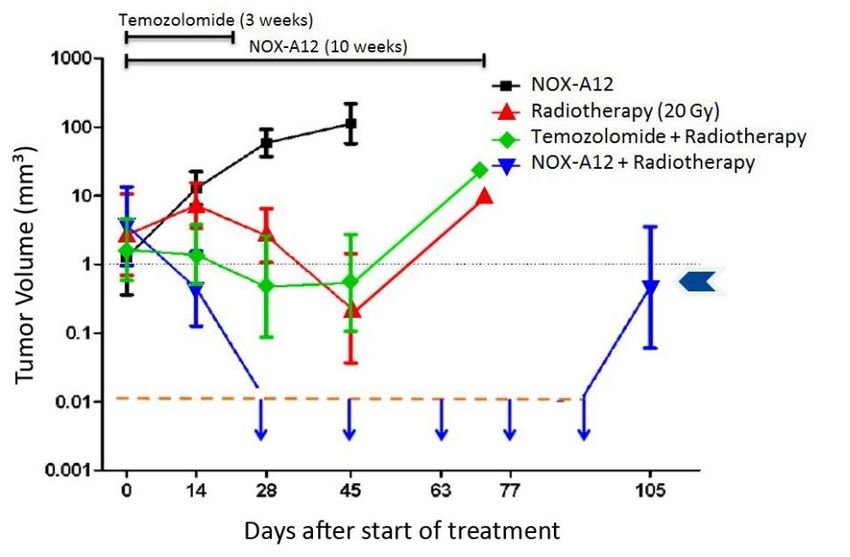
7 Source: Adapted from Liu 2014, Neuro-Oncology 16:21NOX-A12 + Radiotherapy Significantly Increases Survival and
Demonstrates Complete Regression of Brain Tumors
Autochthonous brain tumor model in rats Effects of treatments
Radiotherapy
at day 0
Pregnant rats:
ENU on gestational
age day 17 - 18
Tumor
recurrence
detected only
in 1/3rd of
animals
Key features of the model
100% Complete Response
▪ Spontaneous tumor development in immuno- MRI Detection limit
competent host
▪ Diversity of tumor cell sensitivity comparable
to human situation
▪ Refractory to standard therapies
Combining NOX-A12 with radiotherapy resulted in 100% complete response (66% durable)
in a spontaneous rat model of brain cancer
8 Source: Liu 2014, Neuro-Oncology 16:21Phase 1/2 Trial of NOX-A12 + Radiotherapy: 1st Line Treatment
in Chemotherapy Resistant, Unresectable Brain Cancer Patients
Overview Study Population
▪ Newly diagnosed brain cancer glioblastoma
▪ Include only patients where standard of care chemotherapy temozolomide will not be active, and is thus not given
▪ Only patients with tumor remaining after surgery which allows imaging to assess efficacy (blocking of blood vessel regrowth)
▪ For this patient population Progression-Free Survival (PFS) is 6 months and Overall Survival (OS) 10 months1
Trial Design Objectives & Endpoints
▪ Patients treated in 1st line of therapy ▪ Primary: Safety of NOX-A12 in combination with
radiotherapy, definition of recommended Phase 2 dose
▪ Three doses to be tested: 200, 400 & 600mg / week
▪ Efficacy of NOX-A12 in combination with radiotherapy:
▪ Cohorts of 3 patients per dose, escalation of dose upon tumor vascularization, PFS-6, mPFS, mOS
acceptable safety
▪ Pharmacokinetics and pharmacodynamics of NOX-A12
Planned Timeline2 during and after administration
▪ Cohort 2 first patient dosed 30 June 2020 Regulatory Status
2020 2021
▪ Orphan drug status obtained for NOX-A12 + radiotherapy in
US & EU
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
▪ Trial approved by competent regulatory authority in
PFS-6 Cohort 1 2 3
Germany and currently ongoing
9
1. Kreth 2013, Annals of Oncology 24:3117
2. Timeline subject to financing & recruitment rateNOX-A12 + Immunotherapy
Phase 1/2 Trial of NOX-A12 + Immunotherapy in 20 Patients with
Metastatic Colorectal (11) & Pancreatic Tumors (9)
Baseline tumor biopsy 2nd tumor biopsy
Part 1 Part 2
NOX-A12 Induction NOX-A12 + Keytruda®
1 2
Patients from Part 1
Tumor biopsy before and after then transitioned to
NOX-A12 treatment combination treatment
for 2 weeks of NOX-A12 with checkpoint
inhibitor
Primary endpoint: Endpoint:
Changes in the tumor Assess safety and efficacy
microenvironment induced by of combination
NOX-A12: immune cells &
cytokine/chemokine profile
Clinical Trial a Scientific Collaboration with:
11Merck’s PD-1 Inhibitor KEYTRUDA® (Pembrolizumab)
KEYTRUDA® helps to restore T-cell response and immune response to kill tumor cells
Normal immune response Tumor evasion and T-cell deactivation T-cell reactivation with Keytruda®
When functioning properly, T cells are Tumors can evade the immune system Keytruda® blocks the PD-1 pathway which
activated and can attack tumor cells through the PD-1 pathway by inactivating helps restore the immune response
the T cells
Keytruda® is approved in the US for:
1. Non-small cell lung cancer 8. Gastric cancer
2. Melanoma 9. Cervical cancer
3. Head and neck squamous cell cancer 10. Primary mediastinal B-cell lymphoma
4. Urothelial bladder cancer 11. Hepatocellular carcinoma
5. Kidney cancer 12. Merkel cell carcinoma
6. Microsatellite instability-high cancer 13. Esophageal squamous cell carcinoma
7. Hodgkin lymphoma
KEYTRUDA® sales in 2019: USD 11.1bn
12
Source: www.keytruda.com, Merck/MSD Fourth Quarter 2019 Financial ResultsUnexpectedly High Number of Patients with Long Survival for this
Heavily Pre-Treated Population
SD | 01-020 (PaC) 3
SD | 01-010 (CRC) 5 Number of prior therapies
SD | 01-015 (PaC) 3
01-018 (CRC) 9
01-003 (PaC) 1
01-009 (CRC) 6
01-006 (CRC) 2
01-024 (CRC) 3
01-017 (CRC) 4 Monotherapy
01-013 (PaC) 4
Combination Therapy
01-019 (PaC) 4
01-012 (PaC) 1 Clinical Progress
01-014 (CRC) 7 PD (iRECIST)
SD | 01-001 (CRC) 3
Follow-up: Survival
01-008 (CRC) 4
SD | 01-007 (CRC) 4 Deceased
01-004 (PaC) 5 Lost to follow up
01-002 (PaC) 3
Premature discontinuation
01-011 (CRC) 7
01-016 (PaC) 3
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100
Weeks of treatment / Follow-up
▪ Almost half of patients survived on the study for over 6 months, approx. a quarter for 12 months
▪ Colorectal cancer patients receiving 6th line of therapy on average
▪ Pancreatic cancer patients receiving 4th line of therapy on average
13 Source: Halama et al, Phase 1/2 Study with CXCL12 Inhibitor NOX-A12 and Pembrolizumab in Patients with Microsatellite-Stable, Metastatic Colorectal or Pancreatic Cancer.
ESMO Congress 2019 Poster 613PNOX-A12 + Immunotherapy: Mode of Action (MoA)
▪ CXCL12 excludes effector immune cells from entering the tumor and attracts bone-
marrow derived immune-suppressive / pro-cancer cells to region of tumor
Anti-Cancer Tumor Immuno-suppressive /
Immune Response Pro-cancer
Helper T Cell
Killer T Cell
Natural Killer
Cell
CXCR4 receptor CXCL12 Chemokine
CXCR7 receptor
14
Sources: Feig 2013, PNAS 110:20212; Fearon 2014, Cancer Immunol Res 2:187; Liu 2014, Neuro-Oncology 16:21, NOXXON dataNOX-A12 + Immunotherapy: Mode of Action (MoA)
▪ NOX-A12 reduces CXCL12 “wall” around solid tumors, allowing Killer T cells to
enter, eliminates attraction of immune-suppressive / pro-cancer cells
Anti-Cancer Tumor Immuno-suppressive /
Immune Response Pro-cancer
Helper T Cell
Killer T Cell
Natural Killer
Cell
CXCR4 receptor CXCL12 Chemokine
CXCR7 receptor NOX-A12
15
Sources: Feig 2013, PNAS 110:20212; Fearon 2014, Cancer Immunol Res 2:187; Liu 2014, Neuro-Oncology 16:21, NOXXON dataNOX-A12 + Immunotherapy: Mode of Action (MoA)
▪ NOX-A12 reduces CXCL12 “wall” around solid tumors, allowing Killer T cells to
enter, eliminates attraction of immune-suppressive / pro-cancer cells
Anti-Cancer Tumor Immuno-suppressive /
Immune Response Pro-cancer
Helper T Cell
Killer T Cell
Natural Killer
Cell
CXCR4 receptor CXCL12 Chemokine
CXCR7 receptor NOX-A12
16
Sources: Feig 2013, PNAS 110:20212; Fearon 2014, Cancer Immunol Res 2:187; Liu 2014, Neuro-Oncology 16:21, NOXXON dataNOX-A12 Penetrates Tumor Tissue and Triggers Th1-Type
Anti-Tumor Immune Response
> 3-fold increase
Patient 10 was the only
patient with favorable
baseline T-cells numbers
at tumor invasive margin
17 Source: Halama et al, Phase 1/2 Study with CXCL12 Inhibitor NOX-A12 and Pembrolizumab in Patients with Microsatellite-Stable, Metastatic Colorectal or
Pancreatic Cancer. ESMO Congress 2019 Poster 613POverall Survival Longer Than Expected for this Heavily
Pre-Treated Population
Expected survival
100 Overall Survival
90
OS at 6 months 42%
80
OS at 12 months 22%
Colorectal cancer
Percent survival
70 patients receiving
on average their
60 6th line of therapy
50
Pancreatic cancer
40 patients receiving
on average their 4th
30 line of therapy
20
Responses to 10
immunotherapy can
take 3-6 months to 0
observe and many 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
advanced patients
don’t have that time Time (months)
18 Source: Halama et al, Phase 1/2 Study with CXCL12 Inhibitor NOX-A12 and Pembrolizumab in Patients with Microsatellite-Stable, Metastatic Colorectal or
Pancreatic Cancer. ESMO Congress 2019 Poster 613PNOXXON Investment Highlights ▪ Strong evidence that NOX-A12 may improve survival in solid tumors with high unmet medical need by targeting CXCL12 ▪ NOX-A12 + immunotherapy: mature overall survival data combined with safety profile of combination with checkpoint antibody in metastatic, microsatellite-stable colorectal and pancreatic cancer → catalyst for a co-development deal ▪ NOX-A12 + radiotherapy: trial in 1st line brain cancer initiated → 1st cohort top-line data target Oct-2020 → 2nd cohort top-line data target Q1-2021 → 3rd cohort top-line data target mid-2021 ▪ Top-10 Pharma conducting preclinical evaluation on NOX-A12 for undisclosed additional indication ▪ Cash position >€10m in June 2020 from recent financings provides security to clinical data-points ▪ Full conversion of outstanding Acuitas warrants (20 April 2020) and recent reduction of Yorkville warrants through exercises have simplified capital structure 19
NOXXON: Corporate Profile & Financials
▪ NOXXON Pharma N.V. is a Dutch management holding company listed on Euronext Growth Paris
(ALNOX) and located in Berlin, Germany
▪ NOXXON Pharma AG is the operational subsidiary from which all clinical development is carried out
and where all intellectual property is held
▪ ~ 10 employees, headquarters in Berlin, Germany
▪ Cash & equivalents (as of 16 June 2020): >€10 million and €11.5 million gross capacity still available via
Atlas Convertible Bond vehicle
Financials and Shareholding structure
Public listing 28 September 2016
ISIN Code NL0012044762
Ticker ALNOX
Euronext Growth Paris
Market
(ex-Alternext)
Market Cap ~ €23 M (03/07/2020)
Shares outstanding 39,937,419 (17/06/2020)
*All percentages as per June 2020 (rounded to one decimal place)
20Thank you
You can also read