INTERN MANUAL SURVIVAL GUIDE - LOYOLA INTERNAL MEDICINE 2020 - 2021 Academic Year - Loyola Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
LOYOLA INTERNAL MEDICINE
INTERN MANUAL
&
SURVIVAL GUIDE
2020 - 2021 Academic Year
11th Edition
A handbook of tips, tricks and
approaches to the most common
intern calls, pages and diagnostic
challenges
Name/Pager #: ____________________ NOTES
Locker #: ____________________
How to Page or Call to and from Loyola to Hines?
To page a Loyola pager from Loyola or Hines: dial 9-643– then 4 digit
pager number, after prompt enter call back number, then #
To page a Hines pager from Hines or Loyola: Dial 9 then the pager num-
ber, after prompt enter call back number, then # (Hint: Hines pagers start
with 988)
To call from Loyola to Hines: dial 9-202-VETS (8387) then the 5-digit ex-
tension, then # (Hint: Hines ext. almost always start with 2)
To call from Hines to Loyola: dial 9-216 then last 4 numbers
To call Loyola from outside - dial 708-216 then last 4 numbers
To call Hines from outside: dial 9-202-VETS (8387) then the 5-digit exten-
sion, then #
If ever having trouble reaching an attending to staff a patient, call the Loy-
ola answering service at 66400.
You can also always use your Cureatr app for paging and texting as well,
but do not rely on this for urgent needs. It is always best to actually talk
with someone over the phone if it is an urgent matter!
How to Consult? This will get you to the name and pager # of the person
on various consult services.
At Loyola: in EPIC, go to “Web” > “Web On Call” > “Quick AM” or “Quick
PM” if after 5 PM
At Hines: in CPRS, go to Tools — Clinician Tools — Clinical Resources
(left hand column) —VISN 12 On Call Schedule —Hines-Day On Call
Schedule or Evening if after 5 PM
At Hines, there is also a link to “VISN 12 On Call Schedule” on the Inter-
net Explorer homepage found on the desktop
Please talk with your senior resident before placing a consult
How to know who’s on call & your call schedule?
1. Go to www.Amion.com
2. Password: “loyolaim”
Here you will find who is on call each day, including your personal sched-
ules, clinics, and call days for the year
How to find someone’s pager or number in the hospital
• Refer to the Green card for Loyola or the Yellow Card for Hines.
Search Loyola faculty: in EPIC, go to “Web” > under phone directory click
“search” (near the middle left of page) > you can then search by first and
last name or reverse search a pager number
Search Hines faculty: open the Internet Explorer homepage > click on
“Phonebook” (near middle of page) > you can search by first and last
name
2 59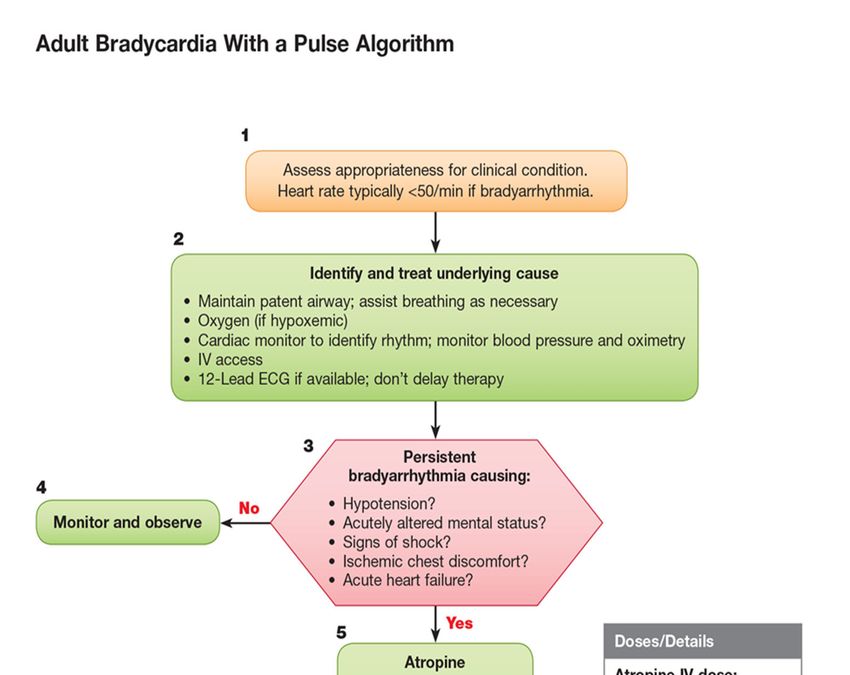
NOTES TABLE OF CONTENTS
A Day in the Life of an Intern……………….… ..... 4
Sign-Out ………………………...………….….. ..... 5
Discharge Summaries…………………………. .... 6
Expiring Meds & Restraints / Incident Reporting… 7
Hines Gen Med Discharge Process…………. ..... 8-9
Useful Equations…………..…..…...................... .. 10
Sepsis…………………………...……...…… .......... 10-13
Hospital Prophylaxis……………………………..... 14
Transfusions / Consent / Death exam……..…..... 15
Electrolyte Disturbance……………………..……. . 16-20
Heme/Onc Emergencies…….……….……....…. .. 20
Acid-Base Disturbance….. …..………………...…. 21-22
Insulin, Glycemic control & DKA………...…......... 23-24
Sleep Issues………………………….……………. 25
Altered Mental Status…………………….............. 25
Pain Control………………………...… .................. 26
Falls…………………………………….. ................. 27
Fever……………...… ........................................... 27
Neurology…………………………….…………… .. 28
Alcohol Withdrawal………… ................................ 29
Anemia………...…… ............................................ 29
Chest pain / Acute Coronary Syndrome.…… ...... 30
Blood Pressure…………………...…..................... 31
EKG Interpretation……………………………….. .. 32-33
Post-Cath Groin Check………….......................... 34
Atrial Fibrillation……………………………............ 34
CHADSVASC, HAS-BLED & “bridging”………… 35
Pre-op Cardiac Risk Stratification………….… ..... 36
Dyspnea / Hemoptysis………...….… ................... 37
LVADs……… ....................................................... 38-39
Mechanical Ventilator / PFTs…………………… .. 40-41
GI bleed, Abdominal Pain & GI Symptoms…. ..... 42
Low Urine Output / Urology Issues…………….. .. 43
ENT Pearls……..……………………...……. ......... 44
Helpful Contacts and Numbers…………….. ........ 45
ACLS Algorithms…….…………………….. .......... 46-49
COVID-19……..………………….………………… 50-51
How to Log Admissions ………………………….. 52
How to Log Procedures…………………………… 53
Personal Notes…………………………………. .... 54-59
58 3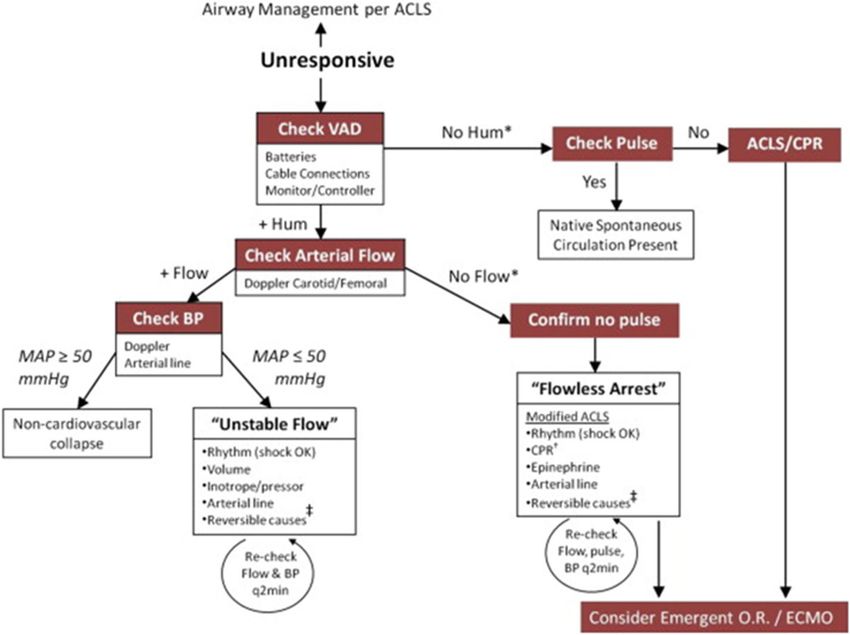
A DAY IN THE LIFE OF AN INTERN
NOTES
There are many tasks and responsibilities on any given day so it’s
important to find a system to stay organized and efficient.
If you follow these steps to structure your day you’re bound to be a
successful, effective, and efficient intern.
When you first arrive in the morning...
1. Un-forward personal pager and collect team pager (if any)
2. Get sign-out from cross-coverage
3. Check if any new admissions
4. Assess and respond to urgent issues if any
5. Print out new list > start making check boxes (“To do list’) for the
day
6. Make sure no meds/orders are falling off, renew if appropriate
7. Review chart information over the last 24hrs (should record
details and bring with you for rounds):
a. Nursing notes
b. Consult team notes
c. SW / other ancillary staff notes
d. Review vitals, I/Os, weights
e. Review medication administration if pertinent
f. Glycemic control (accuchecks, how much CF insulin given)
g. Labs– replete electroytes & adjust insulin right away
h. Imaging, other studies
8. Pre-round (see ALL of your patients)
9. Attending teaching rounds
10. Round with SW, case manager/PCC at scheduled times (see
your rotation specific instructions for times and location)
11. Place urgent orders and consults
12. Get to noon conference ON TIME! Bring your lunch!
13. Work on discharges
14. Place less urgent orders and calls
15. Get the rest of the work done: other orders, procedures, family
calls/updates, patient re-evaluation/care issues
16. Write progress notes
17. Complete discharge summaries
18. Incorporate teaching/learning for your team (lead by attendings,
senior residents, interns or med students!)
20. Update sign out report
21. Sign out (time specific to your rotation)
22. Forward pager to cross coverage
23. Read something specific to your patients that evening
4 57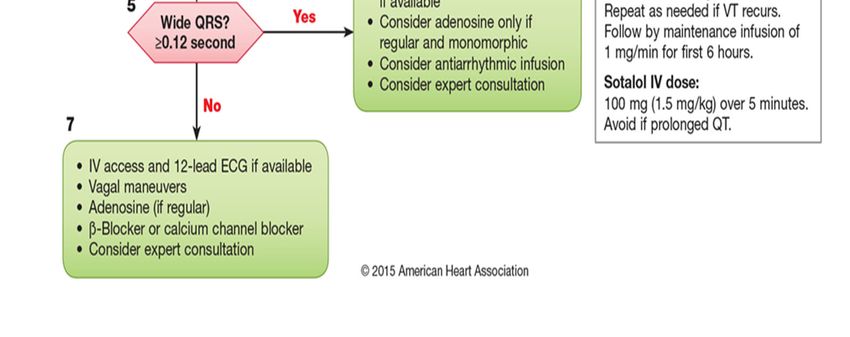
NOTES SIGN-OUT
How to edit and print Sign Out:
LUMC/EPIC: Pt Lists tab > write handoff > edit information in pop-up box > close >Print
Handoff
HVA/CPRS: While signed into CPRS > Tools > Hand Off Tool > edit pop-up box > file
> print
Components of Sign-Out
1) Age
2) Sex
3) Brief PMH significant to their presentation / hospitalization
4) Pertinent presenting signs & symptoms
5) Significant work up and findings (i.e. CT PE today +)
6) Working Diagnosis and treatments (i.e. heparin gtt)
7) Important events of the day
8) On Call to do list: use [ ] boxes (if need to f/u with something, give advice what to
do with results. (i.e. [ ] 16:00 BMP, replete K prn) (NTD=nothing to do)
9) Code Status MUST be listed, even if full code
10) “Anticipated events” list things to watch for / what to do (i.e. high risk for respiratory
failure or high risk for volume overload)
11) Contact info if pertinent (family member #)
12) Identify and communicate the patients you are most concerned about
Tips:
- Make sure labs and meds are ordered as desired and not falling off
- If there is a commonly requested treatment that you DON’T want your pt to get, list it in
the “anticipated events” section (i.e. no opiates, no changing pain meds, no IV Benadryl,
not allowed to leave AMA, etc)
- If a lab or test result would never require overnight intervention, then don’t make it a
checkbox!
- Be sure to update daily, don’t let old events stay on your signout indefinitely!
- Think about what you would want to know about a patient and their condition if you were
the cross-cover resident!
56 5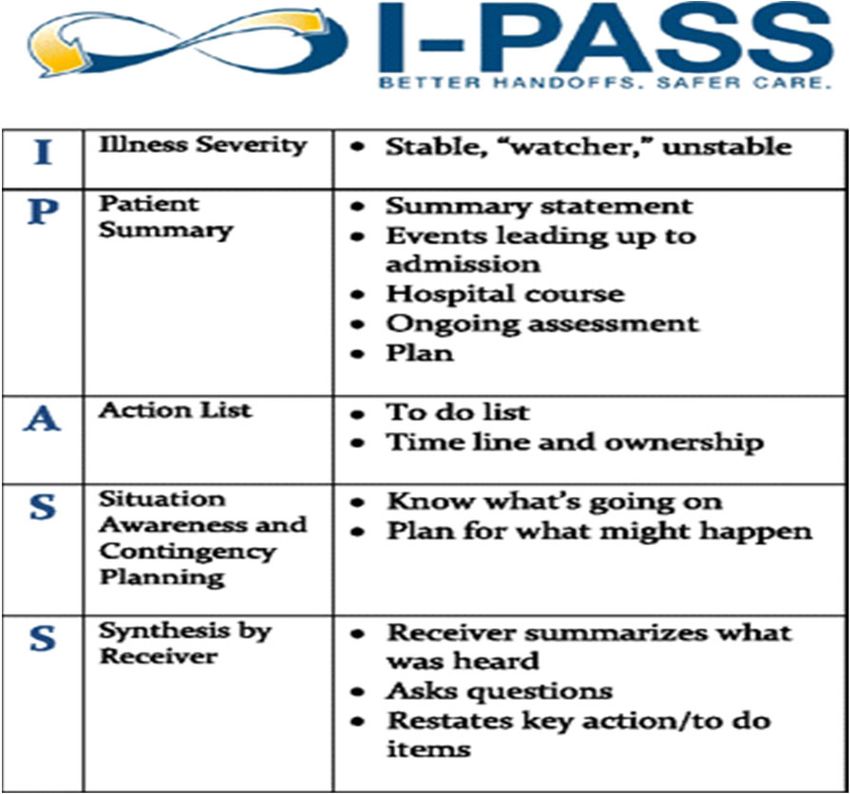
DISCHARGE SUMMARIES NOTES
HVA: see page 8
Loyola : Note type is Discharge Summary, template is “IP dis-
charge summary”
MUST be completed within 24 hours of discharge!!
Include the following:
1. Date of admission and discharge
2. Primary Diagnosis: Main reason for hospitalization
3. Secondary Diagnoses: The rest of the medical problems ad-
dressed during the hospitalization. If you gave a med for it, include
it as a secondary diagnosis. Type these in yourself, do not rely on
computer to auto-populate them as they are frequently incorrect!
4. CONCISE summary of the presentation and hospital care:
Summary of the main points of the reason for admission with the
focus on the hospital course and what was the treatment. Refer
only to *key* labs/studies as appropriate. Always include medica-
tion changes and outstanding labs that need follow up. DO NOT
COPY AND PASTE!
5. Physical exam? You can count your discharge summary as the
day’s Progress Note if you include a physical exam in the dis-
charge summary. If you have written an additional progress note
for the day, there’s no need to document a physical exam.
6. Discharge medications: Make sure it is clear for both patient
and future reader of your discharge summary EXACTLY what the
patient is going home on. Make sure this is accurate—remember
that if you make a medication change after you’ve started your dis-
charge summary, you’ll need to refresh the template that autopopu-
lates the medication or the change will be missed.
7. Follow up: include appointments, labs, studies ordered / sched-
uled
8. Don’t forget to send a copy to the PCP (this is NOT done auto-
matically)
CPRS/GUI: add PCP as additional co-signer to h/p and d/c
summary
Important discharge pearls to include in summary:
- Discharge weight in CHF patients
- Pending cultures that haven’t been finalized
- Follow up labs needed and when
- Be careful with abbreviations, always better to type it out if there
could be any potential confusion
6 55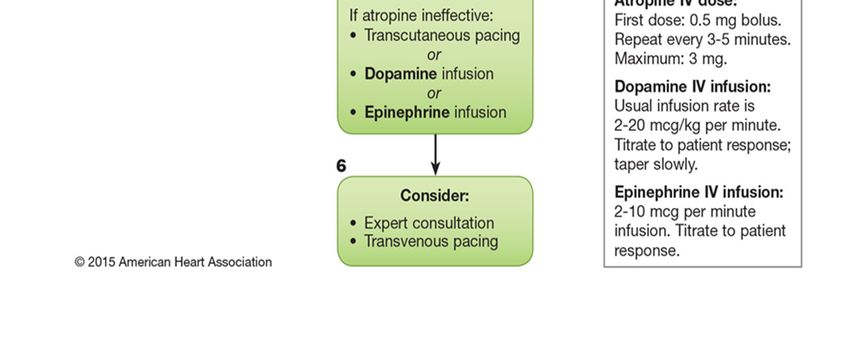
EXPIRING MEDS & LABS
NOTES RESTRAINTS ORDERS
-This should be checked every morning and evening prior to leaving for
the day.
Be mindful that certain antibiotics will fall off if initially approved for a
short duration (they will need to be renewed)
If ordering medications on admission, set duration for a long period to
avoid them falling off the MAR
To easily see expiring orders in EPIC, go to the “Manage Orders” tab >
in the “sort by” dropdown menu select to “expiring”
• At Hines labs need to be entered daily. Review view alerts daily for
notifications of expiring orders
• Restraint orders are to be entered every 24 hrs (only if truly needed)
INCIDENT REPORTING
At Loyola:
• Should you witness a significant harm event, you should report it
immediately to Risk Management/Patient Safety (listed in Web On
Call). They will be able to assist you in handling the event and af-
termath.
• Otherwise, all incidents and near misses can be reported through
the VOICE system found on the portal under the link “Patient Safety
Reporting”.
At Hines:
• All incidents and near misses can be reported through the EPER
system. The link for this can be found on the Hines VA desktops.
Additionally, you should notify your senior resident, attending and
fellow as well as the Hines Chief Resident.
54 7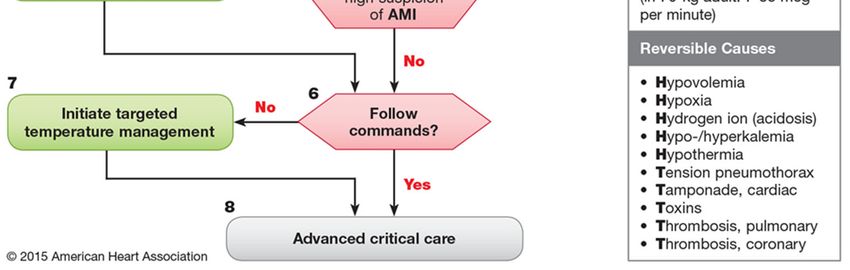
HINES GEN MED DISCHARGES
HOW TO LOG PROCEDURES
These instructions are for Hines Gen Med ONLY—we are not using Please log your procedures in New Innovations (https://new-
this process for other Hines rotations. If you need help with this, ask!! innov.com/login). You will need to have an adequate num-
ber of procedures supervised by a senior resident, fellow or
1. Go to Notes tab —> New Note—>enter note title GEN MED Prelimi-
nary Discharge Document” attending and logged in New Innovations before you may do
2. Set-up for your dual monitors: Drag the note over to the secondary them independently. You will also have procedures logged
screen and maximize it. **You must drag the note back to the primary during simulation assessments (ABG, central line placement,
screen before you sign the note!** On the primary screen, select the ACLS mock codes, IO lines, peripheral IVs)—these will be en-
Meds tab. Maximize the Outpatient Medications section and make sure tered by Jill Wallock.
you can visualize the status of each med (Active, Expired, Discontinued).
3. Complete med rec by comparing inpatient meds within the note to the
outpatient meds. 1. On the dark blue menu bar, choose Logger
4. Assign the medication status in the note—mark the status of each med 2. Choose Procedures
listed (the status selection is not an order). 3. Enter the patient MRN (or first initial+last 4 of SS# for
5. Update the outpatient medication orders in the Outpatient Medications Hines patients) and DOB
section as you go through the inpatient meds listed in the note. 4. Enter the date you performed the procedure
6. Make any needed changes to non-VA meds and other outpatient medica-
tions. 5. Use Location to indicate Loyola or Hines
7. Go to the Orders tab and sign all the med changes but DON’T SIGN 6. Select the procedure from the drop down menu. If nec-
THE NOTE YET! essary, you may select other and then enter the type of
8. Complete the remainder of the Preliminary Discharge Document and procedure in the comment box. CPT code is not required.
click “Finish” once you’ve signed the med orders. (If the “Finish” button 7. Select a supervisor (your attending) from the drop down
is locked, see Troubleshooting)
9. In the next window, hit “Click Here” to place the Pharmacy Consult if it menu. If your attending is not listed, you may choose Dr.
is between 8 and 3 PM on non-holiday weekdays. If it is not during Simpson and type your attending’s name in the comment
these times, click the alternative option which will skip the consult. If box.
you accidentally skip the consult, see Troubleshooting.
10. Click “Accept” to accept the Anticipated Discharge Order.
11. Go to File —> Refresh Patient Information. A window will pop up with Procedure Number needed
things for you to sign. Now you can sign all remaining orders and notes. ACLS participant (indicate role)** 3
12. Go the Notes tab and make sure you have signed the Preliminary Dis- Arterial line placement 5
charge Document Note. Arthrocentesis (site in comments) 5
13. If a Pharmacy consult is ordered, await the consult reply (up to 2 hours). Central line placement 5
14. When the pharmacy calls you (or writes note), immediately revise any
orders as needed.
Central line removal 5
15. Go to the Notes tab and enter note title GEN MED Patient Discharge Abscess I&D 3
Instructions (TAKE-HOME) BETA. Revise/rewrite any medication IO line placement 3
instructions to the patient as needed. Lumbar puncture 3
16. Enter and sign the discharge order. Do not delete the discharge order if a Nasogastric intubation 5
nurse asks you to (refer to CR or inpatient leadership team as needed).
Pap smear/endocervical culture 3
17. Go the D/C Summary tab and complete GEN MED Discharge Sum-
mary note within 24 hours of discharge if it is your progress note Paracentesis 5
(contains physical exam) or within 48 hours of discharge if it is additional Peripheral IV placement 3
to the day’s progress note. Note: you cannot start this until the GEN Peripheral blood draw 3
MED Preliminary Discharge Document is completed! Thoracentesis 5
**You do not have to participate in 3 codes before running one—we are just
keeping track of numbers for this category
8 53
HOW TO LOG ADMISSIONS
Troubleshooting/Tips:
**If the Finish button on the GEN MED Preliminary Discharge Docu-
ment is locked…
You are responsible for doing at least 50 admissions (initial ...and all information has been completed in the note, go to the Notes tab and
H&P and admission orders) during your intern year. These select the title of the GEN MED Preliminary Discharge Document on
should be logged in New Innovations (https://new- the left-sided notes column. Return to the open note and click the Finish
innov.com/login). Please update this regularly so that you button.**
don’t lose track of the patient info and then have trouble log- **If you accidentally skip the Pharmacy consult or if you completed the
ging it later. It makes sense to update this at the same preliminary discharge document the previous night…
time you log your duty hours every 2 weeks. ...you can order the consult without repeating the entire process. Go to IN-
PATIENT CONSULTS —> Medicine Consults —> see last item on the
1. On the dark blue menu bar, choose Logger list and click on “Preliminary Medication Reconciliation request.**
2. Choose Log Books **If it has been over 1 hour and you haven’t heard from Pharmacy or if
you have any questions for Pharmacy related to the discharge…
3. Click Add New Entry. The following screen will appear:
...please call or page the pharmacy. Ext 23187 or 23235; pager 988-8616.**
**If you simply must work on your discharge summary before the rest of
the process is done…
...Go to Notes—>enter note title STICKY NOTE and you can start working
on the discharge summary, which can be copied and pasted into your
actual discharge summary later.
Using the Dual Monitor
Every dual monitor computer station has a primary and a secondary
monitor. When you drag notes or CPRS onto the secondary monitor,
please know that you may experience CPRS on a single monitor com-
puter. This is because CPRS “thinks” that you are still using the dual
monitor and therefore the note you are trying to write is not visible to
you because it is being displayed on the non-existent second monitor.
This is a problem with the software. To avoid it: Drag any notes or
CPRS windows back to the primary monitor before signing notes or
closing CPRS. If it happens to you: Call the Help Desk at 4HELP
(44357) and ask them to help you with “Clear Size and Position Settings
for User.”
Contact us for questions/issues/feedback:
4. Enter the date of admission, MRN (or first initial+last 4 1st call: Meghan O’Halloran (Internal Medicine): pager 988-0913, cell 847-
of SS# for Hines patients), Hospital, and Service 736-7331
2nd call: Adam Van Huis, Leo Gozdecki or Fizza Hussain (Chief Residents)
3rd call: Rommel Pardo (Informatics): Ext 27244
52 9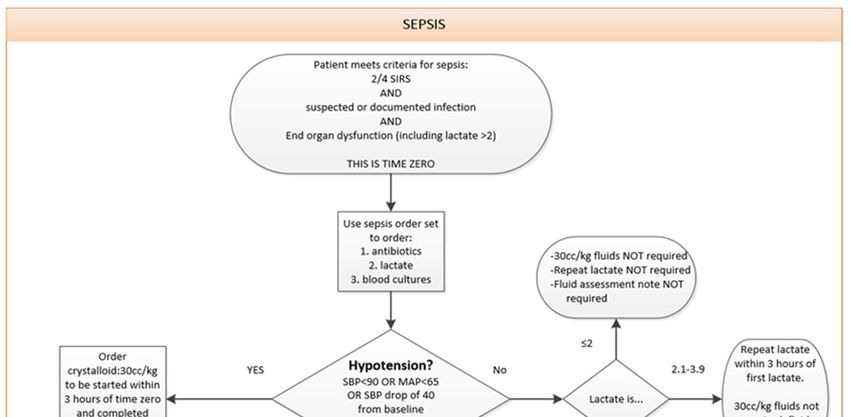
USEFUL EQUATIONS COVID-19
A-a Gradient: (mmHg)
A-a = FiO2 (713) - (PaCO2/RQ) - PaO2
FiO2 = 21% on RA, ↑ ~3-4% per L nasal cannula
713 = [760 (Patmosphere) - 47 (Pwater vapor)] Ancillary Services are available for COVID+ patients:
ABG provides PaCO2 and PaO2 • CT/MRI have protocols in place for scanning COVID+ patients
Respiratory Quotient (RQ) = 0.8 (diet dependent) • Avoid reflex ordering PT/OT/speech to limit unnecessary exposure. But remember that if patients have
been intubated/proned/paralyzed for a prolonged period of time PT/OT will be a critical to their overall
recovery
Estimated normal A-a = (Age/4) + 4
IF patient would benefit from services, place order as usual but specify within order the following:
Fick Cardiac Output: • “Discussed with attending on rounds. Okay to proceed with ancillary services”
Oxygen consumption (L/min)= CO (L/min) x arteriovenous (AV) oxygen difference • “Nursing has initiated or attempted mobility”
(must be measured, approx 125 ml/min/m2) • Prior to speech evaluation, have nurse assess at bedside
** Cardiac Output (L/min)= oxygen consumption/[Hb x 13.6 x (SaO2-SvO2)] • Patients will likely be seen at the end of the day
Protected Codes/RRTs:
Mean arterial pressure (MAP)= [SBP + (DBPx2)]/3 • Fellow and senior should be present for all protected codes and rapid responses
Minute Ventilation (VE)= tidal volume (VT) x RR (nl 4-6 L/min) • Bring blue jump bag (located in 4853) that contains PPE
Corrected Calcium= Measured calcium + [(4-measured albumin x 0.8] • Minimize number of people in room. Ideally (primary RN, RRT RN, RRT RT, primary physician, COVID
Corrected Na in Hyperglycemia= Measured Na+[2.4x[(measured glu-100)/100]] MICU fellow)
Anion Gap (AG)= Na-(Cl+ HCO3) (nl 12) • Most senior physician should be code leader
Calculated Osmoles= (2xNa) + (glu/18) + (BUN/2.8) • Ask RT to place in-circuit spacer to allow for breathing treatments
Osmolar Gap (OG)= Measured osmoles—calculated osmoles (normalSEPSIS
COVID-19
qSOFA SIRS
Hypotension: SBP < 100 mmHg Temp: 38 C
**Disclaimer: our understanding of how to manage and treat patients with COVID-19 is constantly evolv-
ing, so please consider this information as a guideline and refer to the SharePoint documents and corona- RR >20 or pCO2 < 32
virus central on the spirit homepage for more recently updated information. Please see the MICU Manual Tachypnea: RR ≥ 22
for a more detailed guide. HR >90
Clinical Presentation: AMS: GCS < 15
WBC: >12k, 10% bands
• Week 1 prodrome of mild symptoms, week 2 progressive dyspnea with eventual rapid respiratory decom-
pensation
• Symptoms: cough, dyspnea, fever, GI, URI sx, loss of sense of smell and taste SOFA Sepsis-2 Organ Dysfunction
• High Risk Features: age, CAD, HF, CKD, COPD, DM, immunocompromised/HIV Resp PaO2/FiO2 12 4 aPTT >60
• Tocilizumab (IL-6 inhibitor) should be considered to prevent cytokine storm (this decision is made by ID Heme PlateletsSEPSIS INITIAL Rx ALGORITHM ACLS: BRADYCARDIA 12 49
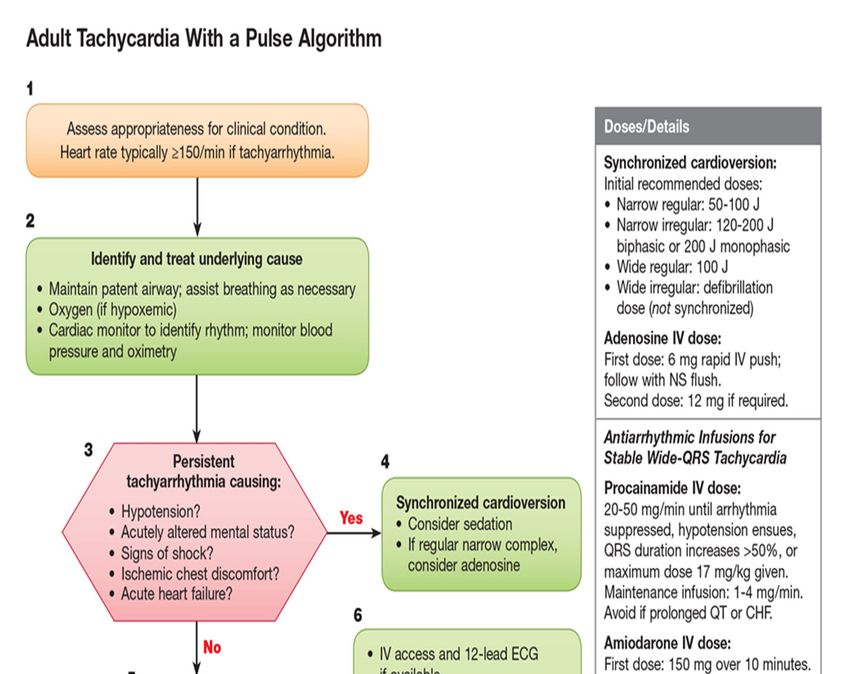
ACLS: TACHYCARDIA SEPSIS INITIAL Rx ALGORITHM
1 What to do at “Time Zero”?
Type “sepsis” into order sets and choose IP SEPSIS OR-
DER SET ADULTS ONLY. Use this to order antibiotics,
blood cultures, and lactate and crystalloid if needed.
Order empiric antibiotics, based on clinical judgement
What counts as hypotension?
2
SBP < 90 or MAP < 65 or SBP drop of 40 from baseline
Which fluids are crystalloid?
3
Saline (use 0.9%) and Lactated Ringer’s
How much should I give?
30 cc/kg started within 3 hours of time zero and completed
within 6 hours of time zero infused as boluses
What is the fluid reassessment note?
4
In any progress note or H&P, type “.6”. 2 options will ap-
pear: 6HRSEPSISCVP and 6HRSEPSISFOCUS. You
may use either depending on which clinical information you
have.
6HRSEPSISCVP: Need at least 2 of the following: CVP,
beside ultrasound of IVC, pulse pressure for passive leg
raise
6HRSEPSISFOCUS: Document physical exam for mucus
membranes, cardiac, pulmonary, cap refill, pulses, and
skin exam
Remember that if this note is needed, it needs to be done
within 6 hours of time zero!
Sepsis Workflow
48 13HOSPITAL PROPHYLAXIS ACLS: ROSC / POST-CODE CARE
Primum non nocere- First do no harm
Every patient needs to have the following addressed and documented in notes:
• IS (incentive spirometer)
-order on admission for everyone that isn’t intubated
-decreases rates of atelectasis and HAP
-ensure patient knows how to use it (show them)
-should be used 10 x every waking hour
• GI prophylaxis for stress ulcers (SRMD-stress related mucosal disease)
-ICU patients have ↑ gastric acid secretion and ↓ protective barriers
-Current guidelines recommend NO routine prophy for Non-ICU med/surg
patients
-In short, give it to all ICU patients, but stop at discharge, don’t give a PPI
to floor patients unless there’s a good reason.
PPI Dosing Loyola Hines
PO PO pantoprazole 40mg daily PO omeprazole 20mg daily
PO via feeding tube lansoprazole 30mg daily per tube Lansoprazole 30mg daily per tube
IV (only use if strict NPO) IV pantoprazole 40mg daily IV pantoprazole 40mg or IV Famotidine
• VTE prophylaxis
-order for every patient hospitalized for an acute medical illness
-Pharmacologic prophylaxis is preferred over SCDs (as long as there is no contra-
indication to anti-coagulation)
Dosing Contraindications Comments
SCDs - • Evidence of leg *Use if anticoagulation is
ischemia from PVD contraindicated
• Evidence of DVT
Heparin sq 5000 units q8hrs • Hx of HIT Short acting– TID dosing
Risk of developing HIT=2.6%.
• ↑bleeding risk
Hypothermia Protocol (at LUMC):
LMWH sq Enoxaparin 40mg daily • Creatinine >1.5 Only once daily dosing • Start within 1 hour of arrest (approved in ED, MICU, CCU, and 2ICU)
Risk of developing HIT=0.2%.
• hx of HIT • Contact:
• ↑bleeding risk - Cards fellow (pg 12191)
- Neuro consult prior to paralysis (pg 91516)
• Details:
EPIC web tab → Clinical Protocols → LUMC Order sets/Guidelines → Ctrl+F
“hypothermia” for “Therapeutic Hypothermia” Practice Guideline
TIME IS BRAIN!
14 47ACLS: PULSELESS ARREST BLOOD TRANSFUSION / CONSENT
1) Transfuse for HgbELECTROLYTE DISTURBANCES HELPFUL CONTACTS / NUMBERS
PAGER PROBLEMS
HYPERkalemia • Parking Office: x60297
- First confirm it’s legitimate and sample is not hemolyzed. Repeat if so.
- Etiology:
EMR HELP
ARF / CRF / Type IV RTA Endocrinopathies (Addison’s, • CRPS: x22777 (can also contact LaWanda below)
Meds (spironolactone, ACEIs, hypoaldosteronism) • CPRS remote access: see LaWanda below
ARBs, BBs, Digoxin, calcineurin Cellular destruction (Tumor • VA desktop login: x44357
inhibitors, etc.) Lysis Syndrome, rhabdo, burns, • EPIC: x63270 or x62160
K+ in IV infusions / TPN etc.)
RESIDENT SUPPORT STAFF
Emergency if: Rapid increase or EKG changes (peaked T’s, no P’s, wide QRS, • Jill Wallock (Loyola): x66053
sine wave)
• Stephen White (Loyola): x65522
TREATMENT • LaWanda Urqhart (Hines): x24564
Temporary (cellular shift): Used as bridge while waiting for effects of long-term GME office: x65620 or x64533
1) IV Calcium– stabilizes cell membranes (lasts 30 min), essential if EKG changes
• Human Resources / Benefits / Payroll: x63242 x63234 x62030
Ca Gluconate 1-2 g (↓ risk of necrosis, but ↓ elemental Ca)
Ca Chloride 1-2g (central line if possible to avoid necrosis) PATIENT AND EMPLOYEE SAFETY
2) Insulin/Dextrose-10units regular insulin + 1 Amps D50 IV push (lasts 2-4 hrs)
3) Bicarb (1-3 Amps IV push - only useful in acidosis)
• Security (Loyola): 911 or x69077
4) Albuterol neb (lasts 30-90 minutes) • Security (Hines): x22013 or x23200
**Rebound hyperkalemia • Risk management & Patient safety: x64215 or Pg. 708-643-0875
likely if only temporary
Long-term (Permanent Elimination): Start simultaneously with measures used** • Ethics service: 708-327-9219
temporary measures
1) Kayexalate- 30-90g PO/enema- (onset 1-2 hrs)
• Needle Stick or bloodborne pathogen exposure: Page 708-643-0833
2) Lasix IV- CAUTION as pts often dry, usually need high doses immediately. Then go to Spirit homepage and in lower right corner under the
(onset 30min) “Quality and Safety” section click “Employee Safety” and follow instructions
3) Hemodialysis —Follow up K+ q4-8hrs & treat underlying illness for needle stick/bloodborne pathogen exposure
• Too fatigued to drive home? Utilize any rideshare (Uber or Lyft) or Way to
Go taxi to get home and to get back to work in AM. Keep receipts and turn
HYPOkalemia (Replace if < 4.0) into GME office for reimbursement
-Si/Sx: Nausea, vomiting, weakness, muscle cramps. ECG with U waves, ectopy
-Causes: Alkalosis (diuresis/vomiting), Acidosis (RTA, DKA), Cellular shifts
(Insulin, catecholamines), mineralocorticoid excess, hypomagnesemia
Depressed? Stressed? Overwhelmed? Feelings of hurting yourself?
(must correct first), diuretics • EAP (Employee Assistance Program) - 24/7 availability: 1-800-437-0911
• Page the on-call chief pager and talk about care for caregiver program
TREATMENT:
Choose route/formulation/dose: Can combine IV & PO if severe deficit,
- For every 0.1 MM/L deficit, replace 10mEq of K Adverse patient care event or unintended outcome? Near misses? Disrup-
- Always replete the Mg before (or simultaneously with) K tive staff behavior? Medication errors? Equipment failures?
• Tablet= KCl (K-Dur)= preferred, faster, less side effects, less dangerous. • VOICE reporting: anonymous system to help identify and fix system prob-
Max dose = 60 mEq at a time. HUGE pill = DIFFICULT TO SWALLOW lems/failures or staff issues.
• Powder= KCl (K-Lor)= same as K-Dur, but TASTES AWFUL, use if feeding tube • Go to Spirit homepage and in lower right corner under the “Quality and
• IV= KCl or K+acetate= only use if NPO or severe deficit. Max infusion rate is Safety” section click “VOICE” and follow instructions
10mEq/hr peripherally, 20meq/hr centrally (arrhythmias). Peripheral infusion
often BURNS.
Use K-acetate ONLY if pt has acidosis or hyperchloremia • 24/7 on-call chief: 708-643-0718
Monitor/Reassess: Mild - q12hrs, Severe - q6hrs • Nkiru Osude (Loyola): 708-643-1625
• Stephen Morris (Hines): 708-643-4867
Note: • Colette Williams (Outpatient): 708-643-2309
-ARF/CKD - be gentle (half dose or less, double interval, or don’t treat) • Poornima Oruganti (QIPS): 708-643-2474
-DKA - be aggressive (keep K >4-4.5mEq/L) • Stefanie Milner (QIPS): 708-643-4334
-Hypomagnesemia causes refractory hypokalemia
• Michelle Lundholm (Research): 708-643-8017
16 45ENT PEARLS ELECTROLYTE DISTURBANCES
Epistaxis HYPOmagnesemia (Replace if call ENT: cautery, anterior packing (+/- ABX), posterior Can give up to 4g IVPB at a time
packing (ICU monitoring) • 1.6-2.0mg/dl give 2-4gm IVPB (usually infused at 1mg/hr)
- Control BP, control coagulopathy as able • 1.0-1.6mg/dl give 4-8gm IVPB total, divide doses BID-TID
• 2-2.5mg/dL)
- Laryngectomies: NO connection b/t mouth and trachea (don’t bag mask the -ARF/CRF - be gentle (half dose, double interval, or don’t treat)
mouth to ventilate!)
• Trach supplies
- Know the trach details: Brand, Cuffed (DCT)/Cuffless (CFS), and Size
- Have spare trach, obturator, inner cannula, and suction at bedside HYPOphosphatemia (nl = 2.6-4.4)
• Trach fell out? Causes: refeeding syndrome, DKA, Vit D deficiency, malabsorption, alcoholism,
- w/in 1 week from placement → page ENT to replace! inadequate TPN
- > 1 week → can use obturator insert and replace yourself!
Complications of low phos: Skeletal, smooth and cardiac muscle issues due to
• Complications insufficient P causing low ATP levels > rhabdo, dia-
- tracheitis → ABX phragm weakness, arrhythmias, ileus
- mucus plugging → change inner cannula Phos equivalents:
- displacement/decanulation 8mmol = 14mEq
TREATMENT:
- bleeding < 48 hrs after placement → typically self-limited, procedural • Neutraphos packet = 8mmol Phos + 7mEq K+
- bleeding > 48 hrs after placement → think sentinel bleed, TI Fistula! • IV K+ Phos IVPB = 27mmol Phos + 40mEq K+
• IV Na+Phos IVPB available if need to replace Phos, but already high K+
Mild/Moderate (1.5-2.4mg/dL)
Tracheoinnominate fistulas → ENT emergency! 1-2 packets Neutraphos up to TID
Severe (ELECTROLYTE DISTURBANCES LOW URINE OUTPUT
Check for accuracy
HYPOcalcemia Classification:
1) Foley? Improvement with flushing?
- Causes: CKD, Vit D def., hypoparathyroidism, pseudo-hypoparathyroidism, Oliguria: < 500 cc/day
2) In’s and Out’s
“hungry-bone” syndrome, pancreatitis, citrate infusion (PRBC), rhabdo, TLS or
3) Incontinent / diaper?
Correct for albumin or check an ionized calcium 4) Bathroom privileges? 350 place foley
- Si/Sx: “stones” - nephrolithiasis / nephrogenic DI 6) Urine indices if AKI (Urine lytes, urea, osm, protein,
cre; calc FENa, FeUrea) FeNa= 2= ATN
“psychiatric overtones” - fatigue, confusion/AMS, depression Treatment:
Polyuria and dehydration 1) If dry, replace fluids FeUrea (used when on loop diuretics)
TREATMENT 2) If intrinsic renal, work up 350 cc PVR (make
1.) Total Body Water (TBW) = weight (kg) x 0.6 for males or 0.5 for females sure pt was told to void prior to measuring PVR!)
(decrease to 0.5 and 0.45, respectively if elderly) 4) Hematuria
Urology can see pt. in am unless patient is passing blood clots / mas-
2.) Free H20 deficit (L) = [(Serum Na — 140) / 140] x TBW sive bleeding
5) Scrotal pain
3.) Correct Na by ≤ 0.5 mEq / L /hr (avoid cerebral edema / “locked in” syndrome)
Get a scrotal US then call Urology
Δ Serum Na per L fluid = (Serum Na — Fluid Na content) / (TBW +1) Note: Call urology immediately for urologic emergencies:
- Fournier’s gangrene, Testicular torsion, Priapism, Paraphimosis, Obstructing
-Remember Na content changes depending the type of IVF (i.e. D5W, 1/2 NS, etc) kidney stone
-Increasing free H20 flushes for patients with tube feeds is also an option
-Monitor levels frequently (q6 or 8 hrs) and adjust IVF rates accordingly
18 43GI BLEED ELECTROLYTE DISTURBANCES
1) Upper (hematemesis, melena) vs. Lower bleed (BRBPR/ Hematochezia)- though HYPOnatremia
some overlap - Excess H20 relative to Na, almost always driven by elevated ADH (appropriately
2) Hemodynamically stable (HR, BP)? Check orthostatics or inappropriately)
- Almost all cases are hypotonic hyponatremia or due to elevated glucose levels
*Tachycardia and decreased UOP occurs before hypotension, if orthostatic consider
ICU evaluation
Serum Na 8 if active cardiac ischemia) Hyponatremia
5) Call GI Fellow
6) PPI drip (pantoprazole 80 mg bolus x 1 + 8mg/hr IV x 72 hrs)—needs to be or- Iso: hyperlipidemia or paraproteinemia Hypotonic Hyponatremia
dered by GI fellow or pharmacy approval (MM / plasma cell dyscrasia)
7) Start octreotide gtt if evidence of portal HTN/cirrhosis and evidence of UGIB Urine Osm 6 units transfused Hyper: ↑ BG, mannitol, sorbitol
9) Dispo: Non-urgent → floor, Urgent → ICU, Emergent → scope ASAP
No Yes
ABDOMINAL PAIN & GI Sx Excess Water Intake /
“tea and toast”
Questions: New? Recurrent? Blood? New medications? (opiates)
Don’t Miss: Check urine sodium
1) Acute abdomen- Get acute abd series (upright CXR + 3 views of abd), Gen Surg consult
2) Ischemic bowel (pain > exam findings), leukocytosis, lactate elevation >30 mmolELECTROLYTE DISTURBANCES PULMONARY FUNCTION TESTS
Spirometry:
FVC (%predicted):
-HYPOnatremia (continued) 80-120 NL
60-80 Mild
TREATMENT 40-60 Moderate
-Asymptomatic or chronic: correct Na by ≤ 0.5 mEq / L /hr (avoid cerebral edema /VENTILATORS ACID-BASE DISTURBANCE
Initial Post-intubation Settings:
Mode A/C 1) Acidemic or Alkalemic? [Normal pH (ABG)=7.40]
Rate 12 (ideally, pt should take 4 breaths over vent/min) 2) Primary disturbance respiratory or metabolic or both?
VT 500 (6 cc/kg) HCO3- (BMP): ↑=met. alk.; ↓=met. acid. (normal=24)
Flow 60 PaCO2 (ABG): ↑=resp. acid.; ↓=resp. alk. (normal=40)
FiO2 100% (titrate down as able,ACID-BASE DISTURBANCE (Contd.) LVAD LOW-FLOW ALARM
DIFFERNTIAL DIAGNOSIS 1. Assess patient – EMERGENTLY (think STEMI page)
a. Are they bleeding?
AG Metabolic Acidosis (MUDPILES): b. What is their blood pressure (mean arterial pressure if no pulse)?
Methanol (formic acid) c. How do they clinically look like?
Uremia d. What are the patient’s last lab results?
DKA
Paraldehyde / Propylene glycol 2. Page the Heart Failure (HF) attending physician
Isoniazid / Iron overload a. If no response after 10 minutes, page again
Lactic acidosis (hypoperfusion or metfomin) b. If STILL no response, page another HF attending OR the CV surgery fellow on-call
Ethylene glycol c. You may also page the VAD coordinator (all numbers listed in Web On-Call)
Salicylates (salicylic) 3. Report the following information to attending, fellow, VAD coordinator (get them ready
beforehand)
Non-AG Metabolic Acidosis (USEDCARS + infusion of acids): a. Your assessment of patient (see above)
Ureteral diversions (including fistulas) b. The latest LVAD parameters (Flow, Speed, Power, PI or PI amplitudes if HVAD)
Sniffing glue c. Trends of the MAPs and Flows
Endocrinopathies (VIPoma) d. Urine output
Diarrhea e. Most recent last lab results
Carbonic anhydrase inhibitors / Cholestyramine
hyper-Alimentation (TPN) 4. You will likely have to Order the following, plus any other orders rec’d by the attending…
Renal tubular acidosis a. New set of labs including PT/INR
Type: 1 (Distal) ↓H+ secr.; 2 (Prox) ↓HCO3 resorp.; 4 hypoaldosteronism b. ECHO to assess RV, LV fxn, inlet cannula obstruction
Saline
Infusion of HCl– or Ammonium Cl–
Respiratory Acidosis:
1. CNS depression (sedatives, CNS dz, obesity, hypoventilation)
CARDIAC ARREST IN LVAD
2. Pleural disease (ie PTX, or large effusion)
3. Lung disease (COPD, ARDS, PNA, PE)
4. Musculoskeletal (Kyphoscoliosis, Guillain-Barre, MG, botulism, myositis)
Metabolic Alkalosis: (increased HCO3), almost always due to #1, #2, or #3
1. Intravascular volume contraction (loss via GI, renal, resp, skin, or 3rd spacing)
2. Hypokalemia
3. Vomiting / NG suction
3. Increased glucocorticoids or mineralocorticoids
4. Alkali intake (HCO3 infusion, milk alkali syndrome)
5. Bartter’s syndrome (genetic defect in Na/Cl/K pump– acts as loop diuretic)
Respiratory Alkalosis (CHAMPS breathe fast):
CNS (catastrophic CVA) or Cirrhosis
Hypoxia / Hyperventilation
Anxiety / Pain Refer to page 35 for
Mechanical ventilation the 5H’s and T’s; also
Progesterone / pregnancy / pulmonary (fibrosis, edema, pneumonia) include Thrombosis
Sepsis / salicylates of LVAD and empha-
size Hypovolemia
from GI bleeding
22 39LVAD PARAMETERS INSULIN & GLYCEMIC CONTROL
There are four parameters monitored on the HeartMate II: Speed, Flow, Power, and Pulsatility
Hypoglycemia: Glycemic control goals:
Index. No single parameter is a surrogate for monitoring a patient’s clinical status. It is important
1) Juice or 1amp D50 Floor: Premeal < 140
to consider trends. Each patient’s values are specific to their pump. 2) Recheck Accucheck after 15min Postmeal INP Pharmacy Quick Order by Category > Diabetes
If flow falls below 2.5 L/min, the device will alarm “low flow” medication: insulin > Insulin sliding scale/correction factor > follow prompts
as indicated”
Afterload Sensitive: If afterload (blood pressure) is high, the pump will not increase speed
- Insulin infusion: “INP Orders > Hines PROTOCOLS and PATHWAYS > Endotool Order
to overcome the high outflow pressure. Because power demand is not increased, the dis- Set > follow prompts as indicated”
played flow read out may not change or, potentially, decrease, even though the true flow out -Insulin pump protocol (any pt with pump requires endocrine consult):
of the pump is hindered by the high aortic pressure “Tools > Medical library/Clinical resources > Clinical protocol & pathways
At any given speed, increased blood pressure will decrease flow! > Diabetes Mellitus protocol”
PULSATILITY INDEX Loyola Insulin Protocols:
- Sliding scale: “Manage orders > Order Sets > search ‘IP INSULIN ADULT
Pulsatility Index (PI) is the left ventricle’s (LV) pulsatile contribution to the pump: SUBCUTANEOUS’ > follow prompts as indicated”
LV full → greater stretch → greater contractility = ↑Pulsatility Index - Insulin infusion: “Manage orders > Order Sets > search ‘Endotool’ > follow prompts as
LV empty → less stretch → little contractility = ↓Pulsatility Index indicated ”
PI as it relates to changes in patient’s status:
- Remember to have a hypoglycemia protocol ordered anytime there is active insulin order:
Indicative of changes in volume status due to altered preload - Hines: “INP Orders > INP Pharmacy Quick Order by Category > Diabetes
indicative of changes to the natural heart’s contraction medication: insulin > Hypoglycemia protocol”
- Loyola: Imbedded within the above order sets
PI as it relates to changes in pump speed:
As pump speed is increased, the PI goes down
As pump speed is decreased the PI goes up
PI EVENT
A PI event occurs when there is a 45% + or – change from the previous 15 second running
average. Possible causes of events:
Suction Event: the Dehydration, Arrhythmia, Right heart failure,
inflow cannula is bleeding, increased Vasovagal response Increased PA pressure
obstructed diuresis
If a PI event is detected, the pump speed will automatically reduce to the low speed limit and
then gradually ramps back up at 100rpm/sec to the fixed speed.
38 23DYSPNEA
DIABETIC KETOACIDOSIS
1) Recent sedatives/narcotics?
1) Recent respiratory treatments?
Diagnosis is in the name: 1.) Hyperglycemia 2.) Anion gap metabolic acidosis 2) Pulmonary edema/effusions—In’s and Out’s?
3.) +Ketones in urine or serum (β-hydroxybutyrate) 3) Hypoxia?- Pulse ox correlate with the pulse? Test on your finger.
4) Hypercapnea?- somnolence, asterixis, pursed lip, poor air movement–Get ABG
Symptoms: abd pain, N/V, polyuria, polydipsia, dehydration, fatigue, weakness, 6) Do they have “the look”?
AMS/coma, Kussmaul breathing (deep, rapid)
Main Concerns: Diagnosis:
Precipitants: Always need to work up the source! Remember the 6 I ‘s: PE 1) Listen to patient’s story/look at
-Infection Pneumothorax sign out
-Inflammatory (i.e. pancreatitis/cholecystitis, etc.) COPD/Asthma 2) Focused exam
-Ischemia/Infarction (MI, colonic, stroke, etc.) CHF/Pulm edema 3) Stat CXR
-Insulin non-compliance Large effusion 4) ABG (hypoxia, hypercapnea)
-Intoxication Pneumonia/aspiration 5) Supplemental O2
-Iatrogenic (steroids)
Treatment: Depends on etiology/severity
Labs:
• BMP: ↑ AG, ↓ HCO3, ↑ BG, ↓ or ↑ K, +/- ↑ BUN/Cr if severely dehydrated Duonebs up to q4h on floor, more often or continuous needs ICU transfer
• UA: +Ketones or ↑ serum β-hydroxybutyrate Supp oxygen: NC / face mask > Ventimask > NRB > CPAP/BIPAP > Intubate
• CBC: +/- ↑WBC Caution with high O2 in COPD—may decrease respiratory drive
• Other diagnostic studies aimed at suspected precipitant (see above) Diuresis if overloaded—usually at least 40 mg IV lasix
Treatment: Admit to ICU BiPAP (start at IPAP 10/ EPAP 5) considered in the following:
• Aggressive IVF (these patients are on average 5 L down, sometimes more!) a) COPD exacerbation
- NS initially > 1/2 NS when euvolemic or Na normalizes b) Pulm edema in CHF
- Switch to D5 +1/2 NS when BGPRE-OP CARDIAC RISK STRAT
SLEEP ISSUES
1.) Emergent surgery? - acknowledge the risk and go to OR without further
testing 1) What has worked in the past?
2) Any standing order for sleep meds?
2.) Any very high risk features? - Rx as indicated prior to OR +/- cardiology TREATMENT:
consult 1) Lights off, TV off, relaxing environment
• MI within 30 days 2) Benadryl (diphenhydramine) 25-50mg PO/IV (avoid if >65yrs - anticholinergic)
3) Ambien (zolpidem) 2.5-10mg PO (caution if 1st time use)
• Severe aortic stenosis 4) Restoril (Temazepam) 7.5-30mg PO (caution in elderly)
• Symptomatic mitral stenosis 5) Haldol 1-2mg IV (useful in delirium, dementia, sundowning)
• Decompensated CHF
• Significant arrhythmia (Mobitz II, high grade AVB, CHB, new VT, Note:
uncontrolled SVT with HR >100) Caution in elderly, risk of falls, MS changes, urinary retention
Avoid in liver failure
3.) Calculate RCRI score — low risk ( 2.0 mg/dL • Two = 2.4% Vital signs? New change vs. Baseline?
• Three = 5.4%
Common in-hospital causes:
4.) RCRI score w/ elevated risk (≥1% or ≥1 RF)? -
Assess functional status -Head trauma/ -infection (CXR, Cx, U/A) -meds (anticholinergic, sedatives,
• 1 MET = self care, dressing, toileting falls etc)
• 4 MET = walking up 1 flight of stairs or level ground at 3-4 mph -seizure -toxic/illicits (UDS) -hypoxia
• 4-10 MET = gardening, sweeping, scrub floors, move furniture, -stroke -hypoglycemia -hypercapnea (consider ABG)
≥2 flights of stairs -hypotension -hepatic encephalopathy -sundowning
• ≥ 10 MET = swimming, tennis, competitive team sports, jogging -bradycardia -uremia -ICU psychosis
9:00 mile -bleeding -other metabolic
5.) Function capacity ≥ 4 MET? — no further testing, proceed to OR WORKUP:
1) Neuro exam
2) O2 sat and Accucheck
6.) < 4 MET or unknown? 3) CT head if ANY focal findings (esp. with head trauma)
• Will further testing impact OR decision making? 4) Other work-up directed at suspected etiologies on above DDx
• Further cardiac evaluation and intervention (i.e., stress testing and PCI
for new ACS/UA, etc.) only for standard indications in the absence of TREATMENT: Directed at suspected causes above. Consider:
1) Narcan 0.1-0.2mg IV q2-3mins PRN, if suspect narcotic OD
the proposed surgery* 2) Flumazenil 0.2-0.5mg IV q30-60 seconds PRN, if suspect benzo OD (be careful
• If it will not change OR management, proceed to OR in chronic benzo pts, alcoholics, seizure history as can predispose to seizure)
• If it will, can pursue stress testing and if abnormal can consider 3) Haldol 2mg IV/IM/PO if agitated (Do NOT use if QTc >500ms)
re-vascularization prior to OR. If normal, proceed to OR 4) Turn off TV / lights etc. at night
5) Consider 1:1 sitter or restraints
*This is because studies have shown re-vascularization (PCI or CABG) prior
to OR does not improve peri-operative outcomes
36 25PAIN CONTROL CHADSVASC / ANTI-COAG “BRIDGING”
General guidelines (what was tried before?): - Acute mild-mod pain: trial of
▪Pain >7 increase prior dose by 50% to 100% -Risk calculator for annual stroke risk in patient’s with AFib (higher score = higher risk)
non-opiates > escalate prn
▪Pain 4-7 increase dose by 25% to 50% - Acute severe pain: short
▪PainPOST-CATH GROIN CHECK FALLS
*The main purpose for groin check is to rule out a large bleed
Exam: 1) Go see the patient
• A post-cath groin should be soft, normal-colored, minimal to no bruising and only mildly 2) Were guard rails up? How high is the bed?
tender
• Check for oozing– a small amount is okay– consider bandage change, but call your senior Assessment:
or the cards fellow if concerning 1) Neuro exam
2) Consider CT head if: anticoagulated (incl ASA), Head trauma, AMS, Neuro deficits
• Check pulses (posterior tibial & dorsalis pedis)- compared to Pre-cath exam H&P note 3) Document incident as a cross-cover / progress note (at VA use Fall template)
• Loss of distal pulses could be compression of femoral a. by large hematoma 4) Ensure Fall precautions are ordered and maintained
• Listen for bruit– suggests fistula
• if present, may need U/S in AM as determined by primary team
• Most small bruits resolve spontaneously
• Assess for hypotension or back pain
• Acute hypotension +/- back pain should be assumed to have RP bleed FEVER (>38 C or 100.4 F)
• Apply FIRM (will hurt your hands and the patient), occlusive pressure
PROXIMAL to site of needle insertion
• CALL cards or interventional fellow IMMEDIATELY if this occurs 1) Is this new?
2) When were last cultures sent?- if not in the last 24hrs, probably want to re-culture
3) Is this neutropenic fever? (ANC < 500, do not do internal rectal exam, but do
visual exam for peri-rectal abscess)
ATRIAL FIBRILLATION 4)
5)
Are antibiotics already on board? Are there holes in coverage?
Has the patient received Tylenol/ibuprofen?
Causes: “The 5 W’s + M”
Diagnosis: -Irregularly irregular rhythm on exam Wind: pneumonia, atelectasis
-EKG: no p-waves or “fibrillating” baseline before QRS complex
that are irregular Wound: surgical site, pressure ulcer, IV phlebitis
Etiology: ~50% without regularly identifiable cause Water: UTI
- CHF exacerbation, ischemia, ↑ BP
- Hypoxia, anemia, COPD, PNA, PE, OSA Walk: DVT, hematoma
- Infection, post-op (esp. cardiac surgery), hyperthyroidism, electrolytes issues Wonder drug: Carbamazepine, phenytoin, Phenobarb, beta-lactams, nitrofurantoin,
- Alcohol, drugs (cocaine, amphetamines), caffeine sulfa, allopurinol, bleomycin, NMS, serotonin syndrome, etc.
- Intracranial processes (SAH or ischemic stroke)
- Work up (if new): EKG, CXR, BMP, CBC, Mg, TFTs
Malignancy: lymphomas, renal and hepatic tumors
- Troponin is not necessary unless there are other ischemic symptoms WORKUP: (perform if not done within 24hrs)
- Further work up based on suspected etiology 1) Blood cultures x 2 different sites (4 bottles total)
2) U/A and urine culture
Treatment: - 2 main goals: 1.) Rate or rhythm control 2.) Decreasing stroke risk 3) CXR (PA & Lat preferred)
- No mortality difference between rate or rhythm control 4) Examine external sites (lines, ulcers, wounds)
- Goal HR in rate control strategy isEKG INTERPRETATION
NEUROLOGY
STROKE Location Coronary supply EKG leads
-Si/Sx: dysarthria/aphasia, facial asymmetry, limb weakness/numbness, imbalance/clumsiness
-What to do immediately: Septum LAD, posterior interventricular V1, V2
1.) Have RN call CODE STROKE Anterior LAD V3, V4
2.) Information to have for stroke team: Brief HPI, last known normal, POC glucose
level, creatinine, INR, medication list including blood thinners Lateral Circumflex, LAD I, AvL, V5V6
3.) If hypoglycemic, give thiamine 100mg IV + D50 1 amp IV STAT II, AvF, III, con-
- Imaging orders (discuss with neuro first): CT head non-contrast stat, if (-) —-> CT head Inferior RCA, R marginal sider right-sided
perfusion and CT angio head & neck stat EKG
Circumflex, RCA, PDA V1-V3, consider
SYNCOPE (adapted from JACC 2006) Posterior
(PDA= Posterior Descending Artery) posterior EKG
Anatomy Coronary supply
RA RCA
RV RCA, R marginal, LAD
LA Circumflex
LV LAD, diagonal, L marginal, circumflex
SAN RCA (60%), LCA (40%)
AVN RCA (80%)
Bundle LAD
7) Blocks
1° AV: PR>200ms
2° AV Mobitz type I (Wenckebach): progressive PR prolongation before dropped QRS
2° AV Mobitz type II: dropped QRS w/o PR prolongation
3° AV: complete block, P wave/QRS dissociation
RBBB: (precludes RVH diagnosis)
1) QRS >120ms (incomplete RBBB if QRS 120ms (incomplete LBBB if QRS if hypoglycemic, give thiamine 100mg IV + D50 1 amp IV STAT 5) +/- PRWP, LAD, Q waves in inferior leads
- Labs: CMP, CBC, UDS and AED levels if appropriate Left Anterior Fascicular Block
- If persists >3 min —> Lorazepam 2 mg IV stat (if no IV access, Midazolam 10 mg IM stat) 1) QRSEKG INTERPRETATION
ALCOHOL WITHDRAWAL
1) RATE: Normal 60-100bpm, bradycardia < 60bpm, tachycardia >100 bpm
Major Symptoms:
1) When was their last drink?
Box counting method (1 large box) 2) What is their risk for withdrawal? Seizures (6 - 48 hrs)
Alcohol consumption > 3 – 4 times per week
1 = 300 BPM 2 = 150 BPM 3 = 100 BPM 4= 75 BPM 5 = 60 BPM 6 = 50 BPM
Hallucinations (12 - 48 hrs)
Consumption of 5+ drinks on one occasion
History of morning drinking Delirium (48 - 96 hrs)
2) RHYTHM 1 small box = 1 mm = 40 msec History of impaired control over drinking Autonomic instability / fever (DTs)
Sinus: upright P wave before every QRS 1 large box = 5 mm = 200 msec History of withdrawal episodes or seizures
Current abuse history of other drugs Minor Symptoms: (Starts in 6-36 hrs)
Junctional: regular retrograde or hidden P waves all leads
A-Fib: irr. irregular, P wave ~350-600bpm, QRS ~120-180bpm If +sx or “at risk” for withdrawal, start treatment
Tremor
A-Flutter: regular or irreg P wave ~250-350bpm, saw tooth **At HVA: use “Alcohol Withdrawal Protocol Order Sets…” Irritability
**At Loyola use an order set “IP ICU ALCOHOL WITHDRAW- Anorexia / Nausea
SVT: regular, retrograde P waves, QRS ~150-250bpm AL PROTOCOL” or “IP NON-ICU ALCOHOL WITHDRAWAL
MAT: ≥ 3 different P wave morphologies, QRS ~100-200bpm PROTOCOL”.**
Protocol includes:
PAC: P wave and QRS are early but morphology normal 1) Benzodiazepines, titrate to calm patient
PVC: QRS early and wide without preceding P wave Ativan 1-4mg PO/IV q2hrs PRN
Librium 50-100mg PO PRN (max: 300mg/day)- avoid in liver dz
VT: ≥3 consecutive PVCs, 120-200bpm, unlike SVT has wide QRS and is slightly
irreg. (Non-sustained VT: < 30 sec, Sustained VT: > 30 sec)
2) Fluids and vitamins
Torsades de pointes (polymorphic VT): spiraling VT If can take PO= oral fluids + 100mg PO thiamine + 1mg PO folate + daily MVI
If needs IV= Banana bag = 1L D5 + 100mg thiamine + 1mg Folate + IV vitamins
3) AXIS
Normal ( –30° to +90°) 3) Nursing monitoring for s/s of worsening withdrawal or oversedation (CIWA)
Usually normal if + deflection in both I and aVF Other considerations:
-elevated BP in the setting of worsening withdrawal sx should be treated as
4) INTERVALS withdrawal with benzos rather than with antihypertensives
PR 120-200ms -for autonomic instability consider clonidine start 0.1mg PO q6hr, titrate up
-if refractory, consider using propofol or precedex or barbiturates in ICU
QRS 60-120ms
Prolonged QT: QTc >440ms,concern when >500ms
(Eye ball test: is the QT >50% of the R-R interval)
5) CHAMBER ENLARGEMENT
ANEMIA
Check Retic Index= (retic count x Pts Hct/normal Hct) /maturation factor
Maturation factor for given Hct: 45%=1.0, 35%=1.5, 25%=2.0, 20%=2.5
LVH RVH
1) R in V5 or V6 + S in V1 or V2 > 35mm 1) Right axis deviation > +100° • RI >2% HIGH = Increased destruction or loss
2) R in aVL > 11mm; R in I > 14mm 2) R > S wave in V1 - Hemolysis (high LDH, high bili, low hapto)
3) Left axis deviation < -30° 3) S in V5 ≥ 7mm or R in V1 > 7mm - Acute blood loss (s/s of bleeding) nl abs retic ct = 50K. Should go
4) Cornell: S in V3 + R in aVL >24 (men) 4) R in aVR ≥ 5mm • RI 20 (women) HIGH MCV = Folate def, B12 Def, Liver dz, ETOH, hypothyroid,
LAE RAE meds
1) Can fit >1 small box in 2nd phase of 1) Can fit >1 small box in 1st phase NL MCV = Sideroblastic, AoCD, microcytic overlap/pure red cell aplasia
P wave in V1 of P wave in V1 LOW MCV= IDA, thalassemias, normocytic overlap
2) Biphasic P wave >120ms in II 2) P wave height >2.5mm in II
5) QRST CHANGES Fe TIBC Ferritin % Iron sat
ST Elevation DDx: AMI, pericarditis (diffuse STE), early repolarization, coronary IDA < 18%
spasm, ventricular aneurysm (chronic persistent STE)
ST Depression DDx: ischemia, digoxin effect, hypokalemia ( +/- U wave) AoCD > 18%
Q waves: Significant if: (never normal in V2, V3, or V4 regardless of size) Thalassemias nl nl nl -
1) > 0.04 sec in duration
2) Depth >25% height of R wave in that complex Sideroblastic nl -
32 29You can also read