Le chimeric antigen receptor (CAR) T-cells nella leucemia e nei linfomi - Prof. Paolo Corradini - CARTS milano educaz SIE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Le chimeric antigen receptor
(CAR) T-cells nella leucemia e
nei linfomi
Prof. Paolo Corradini
Divisione di Ematologia -Trapianto Midollo Osseo,
Fondazione IRCCS Istituto Nazionale dei Tumori di Milano
Cattedra di Ematologia, Università di Milano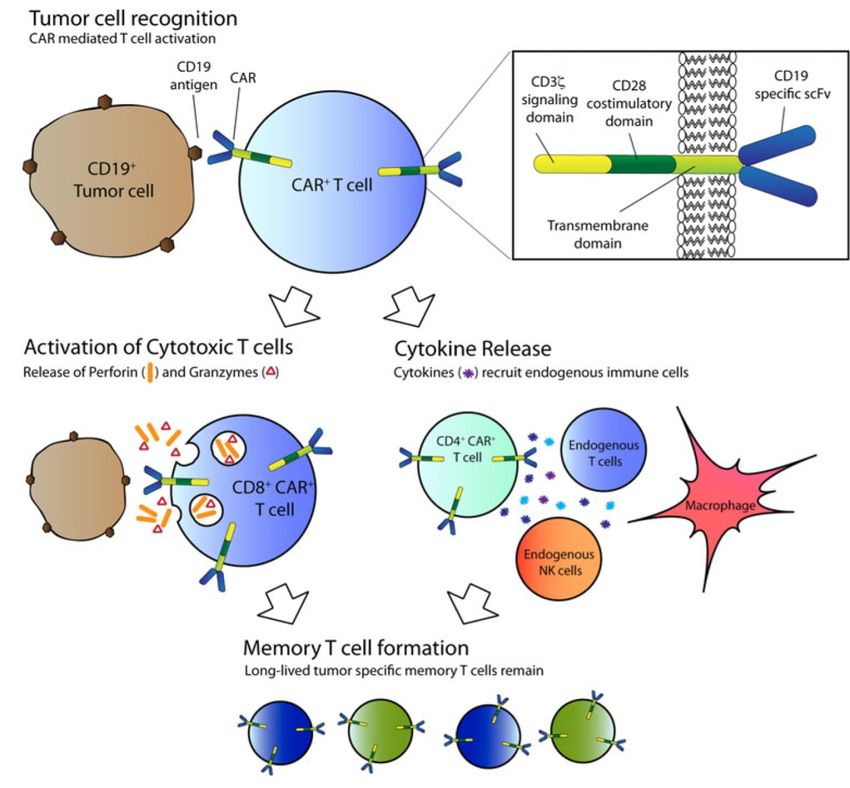
CAR T cells
• Chimeric an+gen receptor (CARs) are proteins
that incorporate an an+gen recogni+on
domain, cos+mulatory domains, and T-cell
ac+va+on domains.
• T cells gene+cally modified to express CARs
specifically recognize and eliminate malignant
cells expressing a target an+gen (CD19, BCMA
etc)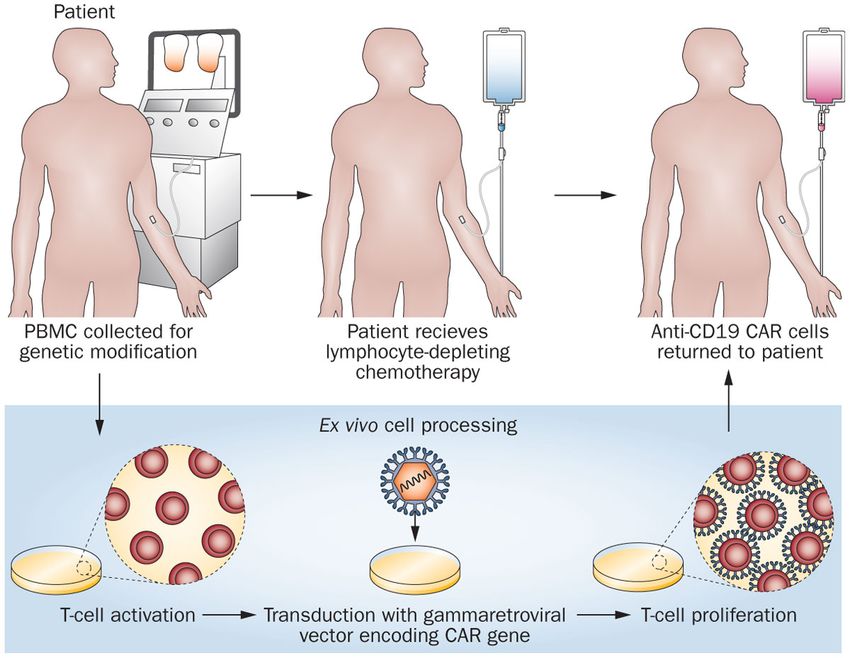
CARTS 1. Come funzionano e quanto funzionano 2. Le tossicità acute E’ una terapia che ha l’intento di guarire una malattia che non ha più terapie disponibili, questa è una differenza importante con molti altri farmaci oncologici.
4
UNA STORIA DI SUCCESSO
DELL’IMMUNOTERAPIA
Sadelain M, Cell 2017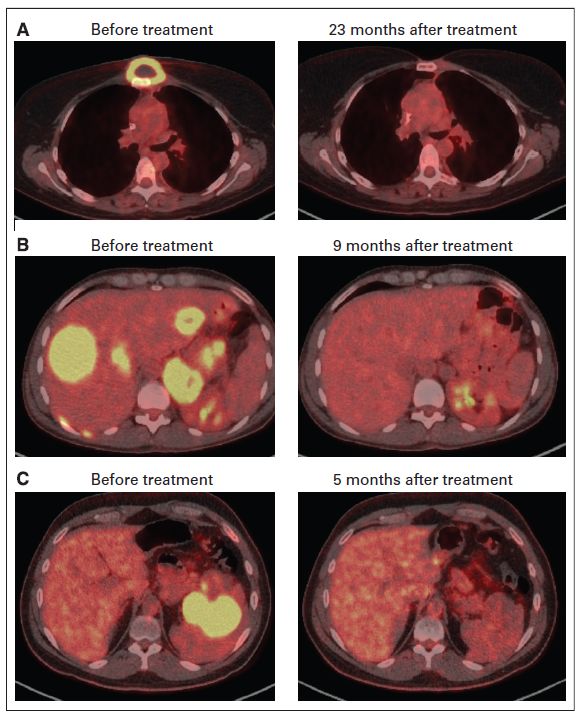
5
STRUTTURA
Brentjens et al JCO 2015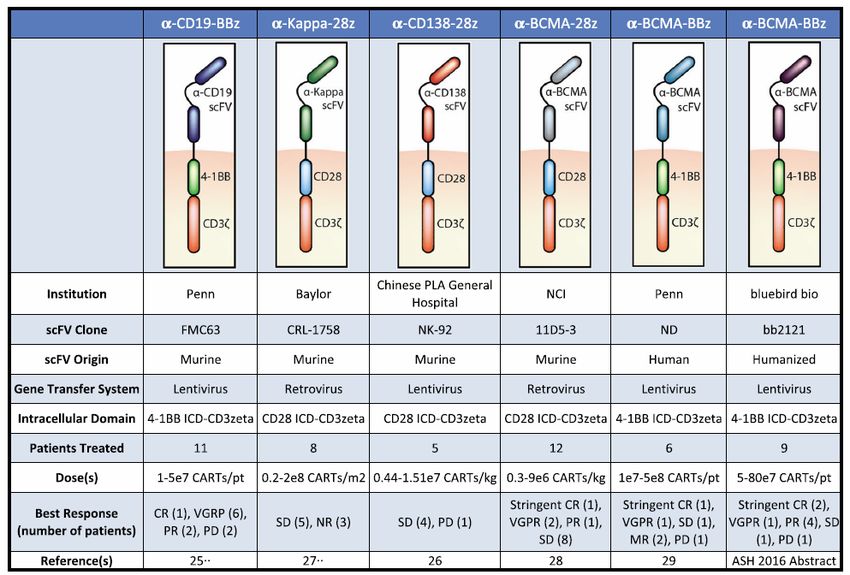
CAR Signaling Domains Program Cells for Metabolic Fitness
BBz CAR
CAR-specific Persistence
Central memory pool
activation SRC
Mitochondrial biogenesis
Oxidative metabolism
T cell
28z CAR
Persistence
CAR-specific Effector memory pool
SRC
activation Mitochondrial biogenesis
Glycolytic metabolism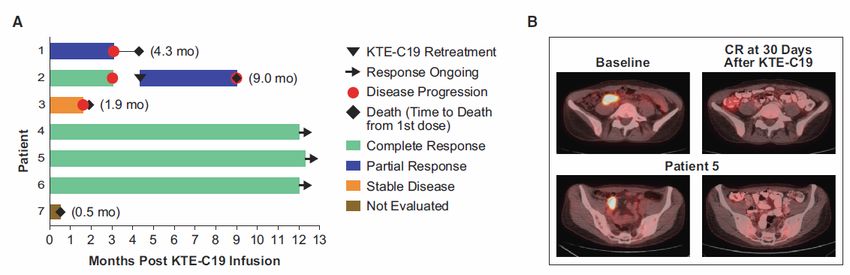
CAR T Cells: they are bionic ! ! CAR scFv or TCR can reprogram specificity of T cells for tumor target. Specificity is important to avoid toxicity ! CAR signaling domains can reprogram T cell metabolism. This can enhance survival in tumor microenvironment and effector function: • CD28 domains: enhance glycolysis via “Warburg” effect. This leads to enhanced effector function and decreased persistence • 4-1BB domains: enhance mitochondrial biogenesis, and are associated with enhanced persistence • ICOS domains: enhanced persistence and cellular respiration in CD4 CAR T cells
8
CRISPR technology for CARTS
Sadelain M, Nature 2018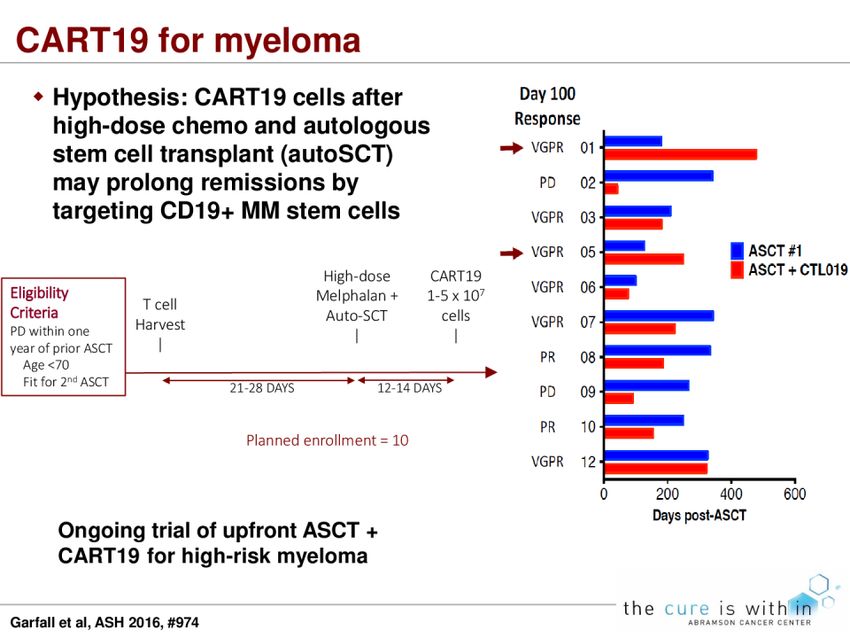
9 CRISPR technology is a simple yet powerful tool for editing genomes. It allows researchers to easily alter DNA sequences and modify gene function. Its many potential applications include correcting genetic defects, treating and preventing the spread of diseases and improving crops. However, its promise also raises ethical concerns. In popular usage, "CRISPR" (pronounced "crisper") is shorthand for "CRISPR-Cas9." CRISPRs are specialized stretches of DNA. The protein Cas9 (or "CRISPR-associated") is an enzyme that acts like a pair of molecular scissors, capable of cutting strands of DNA. CRISPR technology was adapted from the natural defense mechanisms of bacteria and archaea (the domain of single-celled microorganisms). These organisms use CRISPR-derived RNA and various Cas proteins, including Cas9, to foil attacks by viruses and other foreign bodies. They do so primarily by chopping up and destroying the DNA of a foreign invader. When these components are transferred into other, more complex, organisms, it allows for the manipulation of genes, or "editing."
10
MECCANISMO D'AZIONE
Davila Int J Hem 201311
LA TEMPISTICA PER LA COSTRUZIONE DELLE
CARTS E LA SOMMINISTRAZIONE RICHIEDE
CIRCA 3-4 SETTIMANE
Buechner J, Hemasphere 201812
COME SI EFFETTUA LA TERAPIA CON CARTS?
Kochenderfer JN, Nat Rev 201313
DOPO LA REINFUSIONE DELLE CARTS:
• FASE PRECOCE (giorno 0 al +30):
La somministrazione è una semplice infusione
endovenosa, può avvenire in regime di ricovero
(solitamente di pochi giorni). Il rischio di tossicità
acute è esclusivo di questo periodo.
• FASE POST INFUSIONE (dal giorno +30):
Il paziente viene monitorato ambulatorialmente
per complicanze lungo termine (neurotossicità) e
risposta di malaYa. Il rischio di oncogenesi virale
viene monitorato fino a 15 anni dalla reinfusione.
Giralt S, BBMT 201814
TOSSICITA' DELLE CARTS
1) SINDROME DA RILASCIO CITOCHINICO (CRS): risposta infiammatoria sistemica
causata da rilascio di citochine dopo infusione di cellule immuni effeVrici.
15-50% di CRS grave (grado 3-4) negli studi, differente a seconda di +po di
CART e di malaYa.
Manifestazioni simili alla sindrome da aYvazione macrofagica.
2) NEUROTOSSICITA’: diffusione passiva di citochine e di cellule immunitarie nel
sistema nervoso centrale. Tipicamente si manifesta come encefalopa+a
globale, afasia, EEG rallentamento diffuso o convulsioni, liquor posi+vo per
CARTs, la risonanza mostra edema in casi più gravi.
PREVALENZA 5-30% negli studi
Esordio bifasico: 1) giorni 0-5, +picamente associato a sintomi di CRS; 2) dopo
gg +5, compare quando sintomi da CRS diminuiscono
3) INFEZIONI: incidenza simile alle altre chemio di salvataggio
Hill et al, Blood 2018In quali patologie sono sta\ faY degli
studi clinici:
1. leucemia linfoblas+ca acuta del bambino e del giovane adulto
2. linfoma diffuso a grandi cellule B e linfoma follicolare
3. leucemia linfa+ca cronica
4. mieloma mul+plo
SONO STATE APPROVATE COME USO “COMMERCIALE” E NON
SPERIMENTALE DALLA FDA AMERICANA NELLA LEUCEMIA
LINFOBLASTICA DEL BAMBINO E DEL GIOVANE ADULTO
E NEL LINFOMA DIFFUSO A GRANDI CELLULE B
15Key CAR-T Results: Pediatric/Young Adult ALL
CTL019 (anti-CD19) JCAR017 (anti-CD19) JCAR018 (anti-CD22) KTE-C19 (anti-CD19)
Trial [sponsor] Phase I/IIa, NCT01626495 / Phase I/II, Phase I, NCT02315612 Phase I, NCT01593696
CHP959 NCT02028455 / PLAT-02 [National Cancer Institute] [National Cancer Institute]
[Univ of Pennsylvania] [Seattle Children’s Hospital]
Patient population 4-24 yrs*, ≥2nd r/r ALL (N=59), ≥2nd 1-26 yrs, r/r ALL 7-22 yrs, r/r ALL, (N=9, 7 4-27 yrs, r/r ALL or NHL
relapse or refractory (majority (N=37, evaluable N=32); assessed) (N=46 infused; ALL n=45, DLBCL
refractory to multiple prior therapies) majority (>75%) have had 1 or all had undergone ≥1 prior n=1).
[*enrolled adults too; efficacy data 2 relapses; alloHSCT and had been previously Prior transplant history not stated.
here is for pediatric cohort only] ~2/3 have had transplant treated with a CAR-T
Dosing Varied lymphodepleting Varied lymphodepleting Induction chemotherapy with Initial 21 pts and all w low burden:
chemotherapy regimens used. strategies used fludarabine 25 mg/m2 days -4,- low-dose chemo: fludarabine (25
Target dosing 107-108 cells/kg. 4 dose levels: 5x105-1x107 3,-2 and cyclophosphamide 900 mg/m2/day days -4 to -2) and cyc
Median 4.3x106 cells/kg infused cells/kg; MTD 5x106 cells/kg mg/m2 on day -2 (900 mg/m2 day -2)
better risk-benefit profile with Lowest dose: 3x105 cells/kg (6 High disease burden: high-dose
much lower 5x105 cells/kg pts treated). individualized chemotherapy
dose Next dose: 1x106 cells/kg (3 regimen
pts treated) Dose-finding: 1x106 or 3x106
cells/kg; MTD was 1x106 /kg
Response rate CR 93% (55/59) at 1 month, CR 91% (21/22) as of Sept (Preliminary data) 2/7 pts had CR 60%
median f/u 12 mo 2015 data cut-off; CMR 91% MRD-negative CR (1 at each
(85% MRD-negative) dose), 2 with SD, 3 with PD, 2
pts too early to assess
Response durability 18 pts in remission >1 yr, 13 Longest CR: 7 mos In the 1 MRD-negative CR pt, Longest CR 28 mo (in pt with
without further therapy sustained at 2 mo (relapsed at 3 primary refractory ALL) Median
LFS 17.7 mo (45.5% probability
mo) of LFS at 18 mo), based on 20
pts who achieved MRD-negative
CR
Persistence of CAR T Detectable 3 yrs or longer 3 mos In the 1 MRD-negative CR pt, 68 days
cells 19% CAR T cells in bone
marrow at 2 mo
Safety sCRS in 27% (8/30) among early CRS 27% (n=22) Max CRS was gr 2; no dose- sCRS 7/46 (15%);
(N=30) cohort/ CRS (all grades) 18% (n=22) neurotoxicity. limiting CRS. grade 3/4 neurotox 3/46 (7%); no
88% of larger pediatrics cohort No deaths reported At lowest CAR-T dose, 1 pt had gr permanent neurocognitive decline
(N=59). Severe AEs: 43% (13/30) 3 diarrhea.
neurotoxicity; self-limiting. No deaths reported No deaths reported.
3 CRS-related deaths among adult
pts (none among pediatric pts)93% CR rate for r/r ALL afer CTL019 >200 patients with CLL, ALL, NHL, MM have gotten CTL019 • 59 r/r pediatric ALL pts: 55 in CR at 1 mo (93%) median f/u 12 mo • 6 went to subsequent transplant, 1 to DLI • 6 mo RFS: 76% (95%ci 65-89%) 12 mo RFS: 55% (95%ci 42-73%) • No relapses past 1 year • 18 pa+ents in remission beyond 1 year
CTL019 Phase I Trial for r/r CLL: 5 yr follow up
Summary of patient baseline characteristics
N= 14 patients, protocol 04409 (NCT01029366)
Characteristics Statistics, N(%)
N 14
Age at infusion in years
Mean (SD) 66.9 (8.1)
Median (range) 66 (51-78)
Gender
Male
Female
12 (85%)
! ORR: 57%
2 (14%)
! CR 4/14 (28%)
Number of prior therapies
Mean (SD) 5.3 (2.8) ! PR 4/14 (28%)
Median (range) 5 (1-11)
P53 or 17p deletion
! NR 6/14 (43%)
No 8 (57%)
Yes 6 (43%)
IGHV mutation
No 9 (64%)
Yes 4 (29%)
Porter et al, Science Trans Med 201519
SOMMARIO STUDI CLINICI CARTS in NHL
Studio
(adults)
CAR design Istologia #Pts ORR(%) CR(%) Tossicità grado
3-4 (%)
NCI, CD19/CD3z/CD28 with DLBL,NHL,CLL 15 80 53 CRS 50%
2015 Cy/Flu (hi-dose) Neurotox 30%
NCI , CD19/CD3z/CD28 DLBCL,MCL,CLL, 20 40 30 CRS 50%
2016 post alloSCT ALL Neurotox 5%
U Penn, CD19/CD3z/4-1BB DLBLCL,FL,MCL 28 57 51 CRS 14%
2016 variable conditioning Neurotox 7%
FHCRC, CD19/CD3z/4-1BB DLBCL,FL,MCL 18 72 50 CRS 13%
2016 with Cy/Flu Neurotox 28%
NCI, CD19/Cd3z/CD28 with DLBLCL,FL,MCL 22 73 55 NO SEVERE CRS
2017 Cy/Flu (lo-dose) Neurotox 55%
ZUMA1 Cd19/CD3z/4-1BB DLBCL,TFL,PMBC 101 82 54 CRS 13%
Kite with Cy/Flu L
JULIET Cd19/CD3z/4-1BB DLBCL 51 59 43 Neurotox 28%
Novartis with Cy/Flu
TRASCEND CD19/Cd3z/ DLBCL,MCL,PMB 69 75 56 CRS 1
Juno 4-1BB;fixed CD43/ CL,FL Neurotox 14%
CD8 with Cy/Flu20
Terapie con CART anti-CD19 nei linfomi
CTL0191-4 KTE-C194,5 JCAR0174,6
Trial phase 2 (NCT02030834) 2 (NCT02348216) 1 (NCT02631044)
Vector Lentiviral Gammaretroviral Lentiviral
Costim domain 4-1BB CD28 4-1BB
r/r DLBCL, non-GC DLBCL, r/r DLBCL, NOS,
Disease state r/r DLBCL, TFL/PMBCL
DHL, TFL, FL tDLBCL, FL3B
• Age ≥18 years
• Age ≥18 years
• Age ≥18 years • ECOG 0-1
• ECOG 0-2
Key inclusion • ECOG 0-1 • Stable or progressive disease as best
• R/R disease after at
criteria • R/R disease after ASCT or response to last line of therapy, or
least 2 lines of therapy
ineligible for ASCT disease progression ≤12 months after
or after ASCT
ASCT
• Uncontrolled systemic
• Infections that are uncontrolled or
infection
require IV antimicrobials for
• Uncontrolled active infection • Active hepatitis B/C
management
• Active hepatitis B/C • Therapeutic doses of
Key exclusion • HBaAG-positive or anti-HCV positive
• Concurrent use of steroids steroids within 7 days
criteria • detectable CSF malignant cells, brain
• Active CNS involvement of leukapheresis or 72
metastases, history of CNS lymphoma,
• Patients in CR hours prior to infusion
CSF malignant cells or brain
• Active CNS
metastases
involvement
ASCT, autologous stem cell transplant; CNS, central nervous system; CR, complete response; CSF, cerebrospinal fluid; DHL, double-hit lymphoma; DLBCL, diffuse large
B-cell lymphoma; ECOG, Eastern Cooperative Oncology Group; FL, follicular lymphoma; FL3B, FL grade 3B; GC, germinal center; HCV, hepatitis C virus; NHL, non-
Hodgkin lymphoma; NOS, not otherwise specified; PMBCL, primary mediastinal B-cell lymphoma; R/R, relapsed or refractory; tDLBCL, transformed DLBCL; tFL,
transformed FL.
2
1. Schuster, SJ, et al. Blood. 2015;126(23) [abstract 183]; 2. Schuster, SJ, et al. Blood. 2016;128(22) [abstract 3026]; 3. Chong EA, et al. Blood. 2016;128(22) [abstract
1100]; 4. www.clinicaltrials.gov. Accessed April 25, 2017; 5. Locke FL, et al. AACR 2017 [abstract CT019]. 6. Abramson JS, et al. Blood. 2016;128(22) [abstract 4192].
021
Per riassumere i bisogni clinici
insoddisfatti
1. Pazien+ refraVari primari o ricadu+ entro un anno dalla
chemioterapia di prima linea
2. Pazien+ che falliscono il trapianto autologo o non idonei al
trapianto. Va ricordato che il trapianto allogenico è una strategia
pra+cabile solo nel 10-20% dei pazien+, principalmente a causa della
malaYa chemiorefraVaria, della età o delle comorbidità
3. Pazien+ ricadu+ dopo trapianto allogenico
21Salvage regimens: R-ICE vs R-DHAP
Event grade 3-4, n (%) R-ICE R-DHAP
Infection with neutropenia 33 (17) 31 (16)
Infection without neutropenia 11 (6) 15 (8)
Renal 2 (1) 11 (6)
Platelet transfusions, % 35 57
Toxic deaths, n 1 3
Gisselbrecht C et al, J Clin Oncol 2010NOT ELIGIBLE TO TRANSPLANT: R-GEMOX
REGIMEN N^ Median RR% CR % FFS F.U.
age
(R ) GEMOX 32 65 78 50 9 mos 42mosNOT ELIGIBLE TO TRANSPLANT: R-bendamustine
REGIMEN N^ Median RR% CR % PFS F.U.
age
R-BENDA 59 67 63 37 6.7 mos 5 mosAllo-SCT in refractory/relapsed DLBCL
Analysis of the EBMT Registry
Inclusion Criteria:
" first allo-SCT in relapsed DLBCL after a previous ASCT between 1997
and 2006.
" age at allo-SCT >= 18 years
" availability of an HLA-identical sibling or a matched unrelated donor
101 pa\ents; median age, 46 years (18-66)
Van Kampen RJW et al, J Clin Oncol 2011Allo-SCT in refractory/relapsed DLBCL: EBMT Registry
101 pa\ents; median follow-up for survivors 36 months
Van Kampen RJW et al, J Clin Oncol 2011Allogeneic transplanta\on in B-cell lymphomas:
OS and PFS curves
-R-condi+oning versus control group-
OS Rituximab group PFS Rituximab group
Controls Controls
65% (R)
56%
65%
48% (R)
p= 0.708 p= 0.509
Dodero A et al., BBMT 2017Grak versus host disease and relapse free survival
(GRFS) in B-cell lymphomas: a novel endpoint
All Pa\ents
56% 1 year
43% 4 years
p= 0.644
Dodero A et al., BBMT 201729
Nello studio mul+centrico ZUMA-1 di fase 1, hanno valutato KTE-C19, una
terapia autologa basata su cellule T ingegnerizzate (CART specifiche per
l’an+gene CD3z/CD28), in pazien+ con DLBCL refraVario. I pazien+ hanno
ricevuto chemioterapia condizionata a basse dosi con concomitante
ciclofosfamide (500 mg/m2) e fludarabina (30 mg/m2) per 3 giorni, seguita
da KTE-C19 a una dose target di 2x10e6 cellule CART/kg.
Endpoint primario: l'incidenza di tossicità dose-limitante (DLT)
La risposta globale è stata del 71% (n = 5/7) e la risposta
completa(CR) del 57% (n = 4/7). Tre pazienti hanno CR in
corso (tutti a 12 mesi)
Locke FL, et al. Mol 29
Ther. 2017;25(1):285-295.30
Efficacia clinica dopo infusione di KTE-C19
Durata della risposta e sopravvivenza dopo l'infusione con KTE-C19
CR a 30 gg dopo l'infusione di KTE-C19 nel pz 5
Scansioni PET-CT alla malaYa basale e 30
giorni dopo l'infusione di KTE-C19 in un
paziente con recidiva di DLBCL dopo
precedente terapia con R-CHOP, R-ICE e ASCT
con Rituximab-gemcitabina-
busulfanmelphalan + azaci+dina-vorinostat
Locke FL, et al. Mol Ther. 2017;25(1):285-295. 3031
James N. Kochenderfer et al.
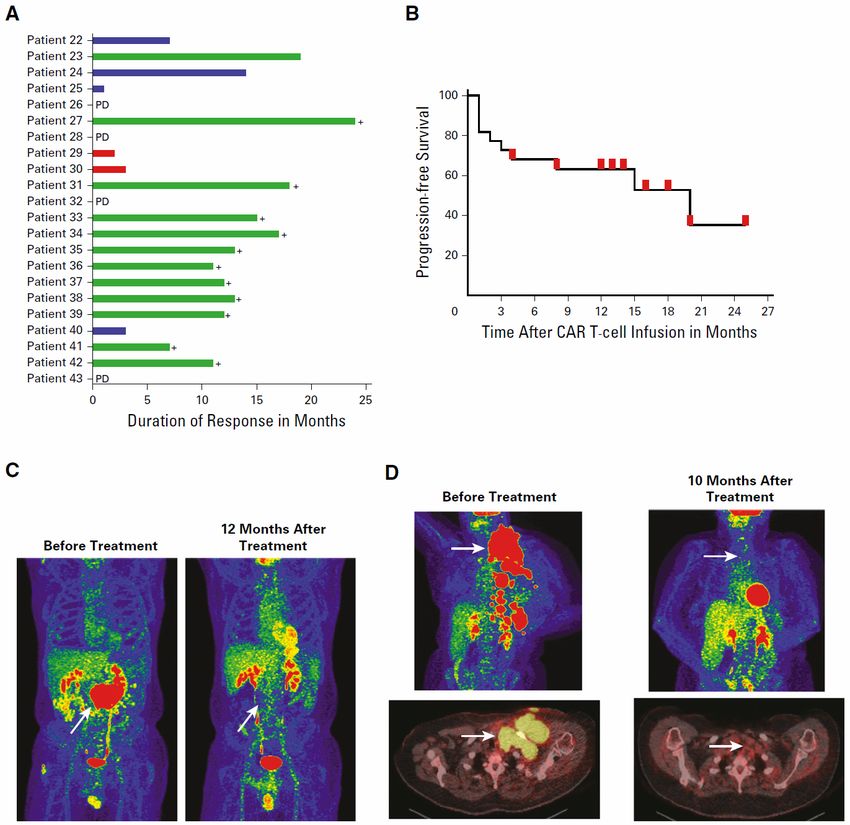
RISULTATI
22 pazien+: il tasso totale di remissione (ORR) è stato del 73% con il 55% di
remissioni complete (CR) e il 18% di remissioni parziali (PR). Sono in corso 11
di 12 CR; Il 55% dei pazien+ aveva tossicità neurologiche di grado 3 o 4
completamente risolte. Il regime di condizionamento a chemioterapia a basso
dosaggio ha ridoVo i linfoci+ del sangue e ha aumentato la IL-15 nel siero. I
pazien+ che hanno raggiunto una remissione avevano un picco mediano di
cellule CAR+ di 98/mcl e quelli che non avevano oVenuto una remissione
avevano un picco medio di cellule CAR+ di 15/mcl (P = 0,027).32
Le cellule CART hanno mandato in remissione dei linfomi
chemio-refranari
A B
B) PFS a par+re dal giorno dell'infusione cellulare e
termine il giorno della progressione della malaYa
è mostrato per tuY i pazien+. I segni rossi
indicano pazien+ con CR in corso al momento
dell'ul+mo FU con un'eccezione: il segno rosso a 4
A) Rappresentazione grafica dei +pi di mesi dopo l'infusione delle CART indica il punto
risposta an+-linfoma e la durata delle temporale in cui il paziente 40 è stato soVoposto
risposte. ad AlloSCT mentre era in remissione parziale. Due
pazien+ sono sta+ censorizza+ ai 13 mesi, 3
pazien+ a 14 mesi, ma c'è un solo segno rosso sul
James N. Kochenderfer et al. JCO 2017 grafico per ciascuno di ques+ pun+ temporali.33 Eradicazione dei PMBCL/DLBCL cloni Kochenderfer JCO 2015
34 Primary Analysis of JULIET: A Global, Pivotal, Phase 2 Trial of Tisagenlecleucel (CTL019) in Adult Pa\ents With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Stephen J. Schuster et al. - Lymphoma Program, Abramson Cancer Center, University of Pennsylvania JULIET è un trial di fase II a braccio unico, in aperto, mul+centrico, di +sagenlecleucel in pazien+ adul+ con DLBCL R/R (NCT02445248) I pazien+ hanno ricevuto una singola infusione con una dose target che variava da 1×108 a 5×108 di +sagenlecleucel CAR T cells
35
Studio Proof-of-Concept
Tisagenlecleucel è stato esaminato in uno studio monocentrico di fase II su adul+ con
Linfomi CD19+ R/R.
- Il tasso di risposta globale (ORR) era del 64% (18/28); risposta completa (CR), 57%
(16/28)
- La coorte DLBCL ha avuto un ORR del 50% (7/14); CR, 43% (6/14)
- TuY i pazien\ in CR sono rimas\ in CR al follow-up mediano di 29 mesi36 Arruolamento dei dei pazienti
37
Efficacia
• Il set di analisi di efficacia includeva tuY i pazien+ che hanno ricevuto un'infusione di
+sagenlecleucel con ≥ 3 mesi di follow-up
• Degli 81 pazien+ valuta+, il 40% aveva un CR
• L'endpoint primario è stato raggiunto: ORR, 53% (95% CI, 42% -64%; P38 Durata della Risposta
39
Sicurezza
• Nessun decesso è stato osservato a causa di +sagenlecleucel, sindrome da rilascio di
citochine (CRS) o edema cerebrale
• Il tempo mediano di insorgenza del CRS è stato di 3 giorni (intervallo, 1-9 giorni)
• Dei pazien+ traVa+ per CRS, il 15% ha ricevuto tocilizumab e l'11% ha ricevuto
cor+costeroidi
Tabella 3. Even\ avversi di par\colare interesse40
Conclusioni
1) La terapia con cellule CART an+-CD19 è promeVente, faYbile e
può indurre remissioni complete durature in pazien+
chemorefraVari.
2) Con una formazione appropriata, la tossicità può essere ges+ta,
ma è ancora un problema da considerare seriamente.
3) È necessario migliorare il tempo di produzione per essere
efficacemente e ampiamente u+lizzato nella pra+ca clinica.
4) La selezione dei pazien+ in base al rischio di malaYa (COO,
DHL, THL, ecc.) sarà essenziale per oYmizzare i risulta+ a lungo
termine.
5) Vanno studia+ interven+ aggiun+vi per i pazien+ in remissione
parziale.
4041
LE 2 TERAPIE CON CARTS APPROVATE DA FDA:
KYMRIAH e YESCARTA
Giralt SA, BBMT 201842 TOSSICITA' “ON-target” e “OFF-tumor” ON target# CARTs riconoscono correnamente la proteina di superficie cellulare CD19 OFF tumor# altre cellule CD19+ non tumorali sono distrune dalle CARTs (B cell aplasia)
43
TOSSICITA' DELLE CARTS
1) SDR DA RILASCIO CITOCHINICO (CRS): risposta infiammatoria sistemica causata da
rilascio di citochine dopo infusione di cellule immuni effenrici.
15-50% di CRS grave (grado 3-4) negli studi, differente a seconda di \po di CART e di
malaYa
Manifestazioni simili a HLH
2) NEUROTOSSICITA'(CRES): diffusione passiva di citochine e di cellule immunitarie
in SNC. Tipicamente si manifesta come encefalopa\a globale, afasia, EEG
rallentamento diffuso o convulsioni, CSF posi\vo per CARTs, MRI mostra edema
in casi più gravi.
PREVALENZA 5-30% negli studi
ONSET bifasico: 1) giorni 0-5, \picamente associato a sintomi di CRS; 2)dopo gg +5,
compare quando sintomi da CRS diminuiscono
3) INFEZIONI: incidenza simile alle altre chemio di salvataggio1
Hill et al, Blood 201844
Conclusioni -1
1) Con una formazione appropriata, la tossicità può
essere gestita, ma è ancora un problema da
considerare seriamente.
2) È necessario migliorare il tempo di produzione per
essere efficacemente e ampiamente utilizzato
nella pratica clinica.
4445
Conclusioni -2
1) La selezione dei pazienti in base al rischio di
malattia sarà essenziale per ottimizzare i risultati
a lungo termine e contenere i costi.
2) Vanno studiati interventi aggiuntivi per i pazienti in
remissione parziale dopo la terapia.
3) E’ la prima terapia cellulare commerciale per una
malattia neoplastica, i medici ed i sistemi sanitari
dovranno imparare a gestire questa nuova
opportunità.
4546
Compara\ve descrip\on of CAR T cell strategies used as
immunotherapies against Mul\ple Myeloma47 This was the first in humans clinical trial of chimeric an+gen receptor (CAR) T cells targe+ng BCMA (B-cell matura+on an+gen). T cells expressing the CAR used in this work (CAR-BCMA) specifically recognized BCMA expressing cells. Our findings demonstrate an+-myeloma ac+vity of CAR-BCMA T cells 12 pa+ents received CAR-BCMAT cells in this dose-escala+on trial. Among the 6 pa+ents treated on the lowest 2 dose levels, limited an+-myeloma ac+vity and mild toxicity occurred. On the 3d dose level, 1 pa+ent obtained a VGPR.
48 4th dose level of 9 x 106 CAR+ T cells/kg body weight: Before treatment, the first pa+ent on the 4th dose level had chemotherapy resistant MM, making up 90% of BM cells. Afer treatment, BM plasma cells became undetectable by flow cytometry, and the pa+ent entered a stringent CR that lasted for 17 weeks. The second pt on the 4th dose level had chemotherapy-resistant MM making up 80% of BM before treatment. 28 weeks afer this pa+ent received CAR-BCMA T cells, BM plasma cells were undetectable by flow cytometry, and the serum MC had decreased by >95%. This pa+ent is in an ongoing VGPR. Both pa+ents had toxicity consistent with CRS.
49
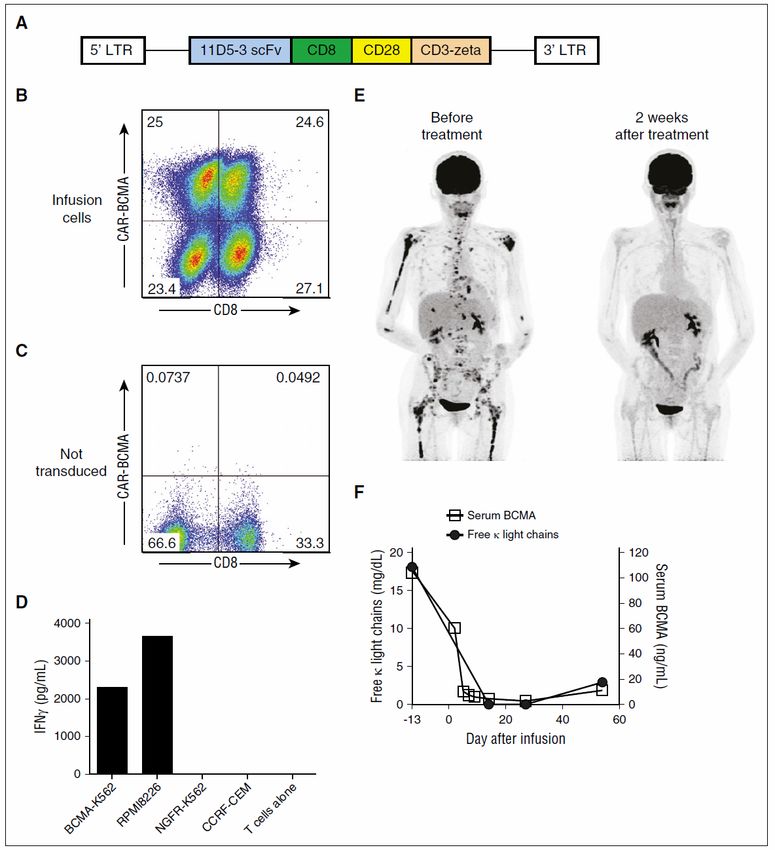
CAR-BCMA T cells specifically recognized BCMA in vitro and
exhibited an\-myeloma ac\vity in humans
Figure 1
(A) Diagram of the MSGV-11D5-3-CD828Z g-retroviral vector encoding the an+-BCMA CAR (CAR-BCMA) is
shown. (B) CAR-BCMA expression on the surface of the infusion T cells of pa+ent 10 was detected by staining
with a PE-BCMA-Fc protein reagent. The plot is gated on live CD31 lymphocytes. (C) Demonstra+ng
specificity, the PE-BCMA-Fc reagent did not stain PBMCs that were not transduced with the CAR-BCMA gene.
(E) Pa+ent 8 who had MM that was progressing despite 8 prior lines of therapy obtained a very good par+al
remission (VGPR) afer infusion of CAR-BCMA T cells. PET–computed tomography scans from before and
afer treatment show elimina+on of a large number of MM bone lesions.50
Conclusions
• Serum BCMA served as a tumor marker because substan+al decreases in
serum BCMA occurred in the 3 pa+ents with the most impressive an+-
myeloma responses (Figure 4D).
• These results demonstrate for the first +me that CAR T-cells targe+ng an
an+gen other than CD19 can induce complete remissions of a hematologic
malignancy.
• It has been shown that CAR-BCMA T cells have powerful ac+vity against MM
that was resistant to standard therapies.
• These results should encourage further efforts to enhance an+-BCMA CAR T
cell therapies. The striking ac+vity of an+-BCMA CAR T cells against MM
indicates that CAR T cells targe+ng BCMA have great poten+al to be an
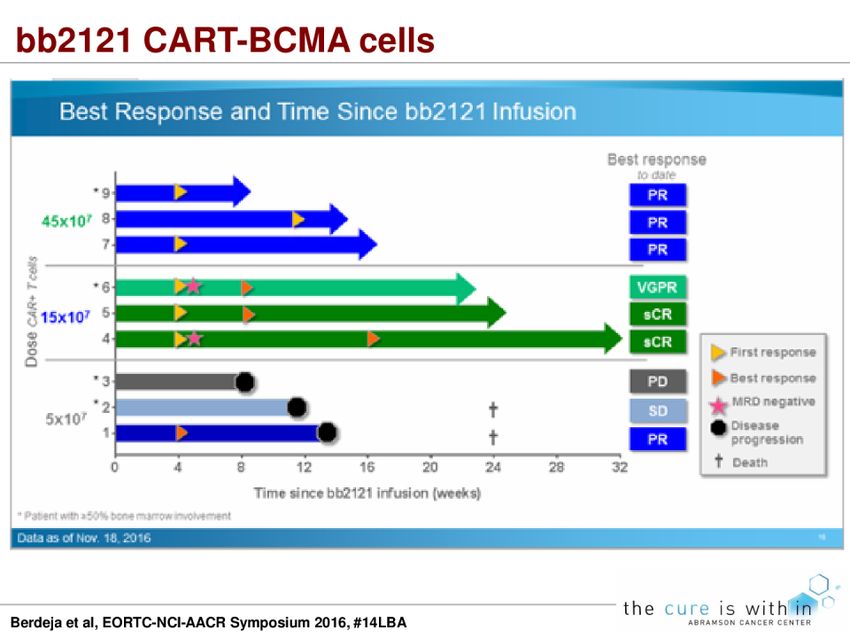
effec+ve new treatment of MM.51
52 12 enrolled, 10 treated and 3 had bener PFS compared to first Mel
53
54
55
CARTS
1. Come funzionano e quanto funzionano?
2. Le tossicità acute
3.I programmi di gesCone isCtuzionali e
cosC56
PROGRAMMA GESTIONE CARTS MDACC:
CARTOX COMMITTEE57
PROGRAMMA GESTIONE CARTS MDACC:
CARTOX COMMITTEE
1) Incontri seYmanali di discussione pazien\ in terapia con
CARTs
2) Gruppo mul\disciplinare di ges\one CARTs
3) Creazione di protocolli di ges\one pazien\ in terapia
4) Adeguata formazione del personale che u\lizzerà CART
(medici, infermieri, farmacis\)
5) Discussione dei trial in corso e dei risulta\ pubblica\
LA SOMMINISTRAZIONE DI CARTs AVVIENE SOLO IN AMBIENTI
SPECIFICI DELL’OSPEDALE58
PROGRAMMA GESTIONE CARTS MDACC:
CARTOX COMMITTEE
• Team NEUROLOGI: valutazione status neurologico del
paziente giornaliera
• Team INTENSIVISTI: valutazione condizioni cliniche
giornaliera, se peggioramento rapido assiste il
trasferimento del paziente in ICU
• Team FARMACISTI: si assicurano della disponibilità di
farmaci salvavita per ges\one CRS (tocilizumab, almeno 2
dosi per paziente secondo FDA)
• Supporto ELETTRONICO: strumen\ informa\ci che
facilitano la raccolta omogenea dei da\ circa la valutazione
delle tossicità delle CARTs (CRS, CRES)59
PROGRAMMA GESTIONE CARTS MSKCC
Giralt SA, BBMT 201860
RACCOMANDAZIONI EUROPEE SU
GESTIONE CARTS
Buechner J, Hemasphere 201861
OGNI PAESE HA UN ENTE REGOLATORIO
DI RIFERIMENTO PER LE TERAPIE
CELLULARI
Buechner J, Hemasphere 201862
LA SITUAZIONE REGOLATORIA EUROPEA
REQUISITI EUROPEI
1)CARTS comprese nella categoria “Advanced Therapy
Medicinal Products” (Regula\on EC n°1394/2007 e direYva
2001/18/EC)
2)CARTS considerate come OGM pertanto vanno seguite
norme di protezione ambientale e del personale specifiche
(DireYva 2001/18/EC e Decisione della Commissione
2002/623/EC)
Buechner J, Hemasphere 201863
LA SITUAZIONE REGOLATORIA EUROPEA
REQUISITI NAZIONALI SPECIFICI
Buechner J, Hemasphere 201864
RIMBORSI FDA
1. KYMRIAH, Novar\s (pediatric ALL) # 475.000 USD
2. YESCARTA, Gilead (adult NHL) # 373.000 USD
Nel prezzo non è compresa la spesa per ges\re ricovero e
possibili complicanze del paziente. In tale caso possibili
anche spese aggiun\ve comprese tra 100.000 USD e
300.000 USD.
(Rimborsabilità trapianto allogenico cellule staminali pari a
80.000-100.000 euro + spese aggiun\ve per complicanze)
www.medscape.com accessed 08/03/201865
PROPOSTE
1. Implementazione standard di qualità per terapie cellulari (e
iden\ficazione centri di riferimento):
• regolare EFFICIENTEMENTE la ges\one dei trial
(creazione di rete interospedaliera di riferimento)
• maneggiare IN SICUREZZA le CARTS (creazione di
standard di qualità terapie cellulari, vedi FACT-IEC)
• amministrare il prodono IN SICUREZZA (personale
formato e creazione di rete intraospedaliera)
2. Creazione di un registro nazionale/europeo per raccolta
da\ su terapia cellulari (vedi esempio CIBMTR ed EBMT)You can also read

















































