Les actualités PEC des cancers bronchiques au stade précoce - DAVID.PLANCHARD GUSTAVE ROUSSY Head of Thoracic Group Villejuif - FRANCE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
les actualités PEC des cancers
bronchiques au stade précoce
DAVID.PLANCHARD
GUSTAVE ROUSSY
Head of Thoracic Group
Villejuif - FRANCE
M-MA-00000097
Le contenu et l’interprétation de ces diapositives reflètent le point de vue Les informations présentées pourraient comporter des données relatives à des produits non enregistrés ou à des indications non La cadre de cette présentation est scientifique et nullement promotionnel.

Pour toute information médicale sur les produits Roche, veuillez nous contacter à l’adresse :
email: morocco.medinfo@roche.com, par téléphone : 05 22 95 90 00 ou par fax : 05 22 95 90 01
Pour toute notification d’évènements indésirables, veuillez nous contacter à l’adresse :
email: morocco.drug_safety@roche.com, par téléphone : 06 61 05 31 70/ 05 22 95 90 58
ou par fax : 05 22 95 90 59
Roche Maroc S.A. Ivoire 05, Casablanca Marina Bvd Sidi Mohamed Ben Abdellah Casablanca, MAROC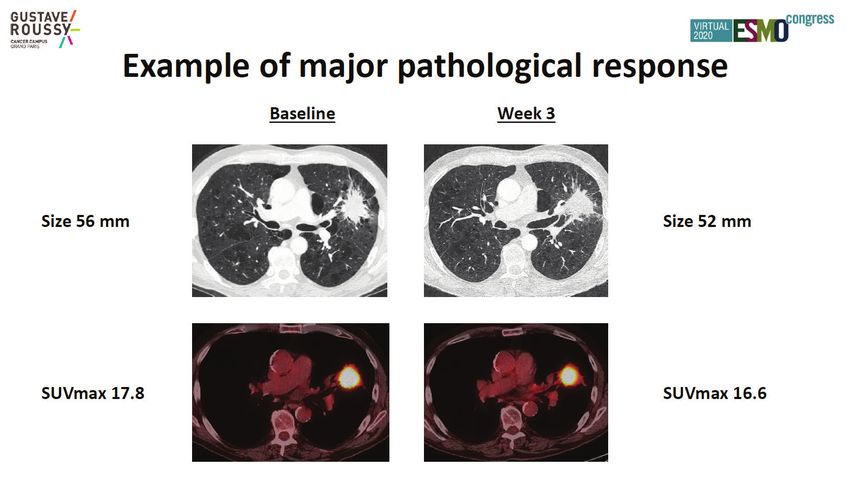
DISCLOSURE SLIDE Consulting, advisory role or lectures: AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Merck, Novartis, Pfizer, prIME Oncology, Peer CME, Roche, Samsung Honoraria: AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Eli Lilly, Merck, Novartis, Pfizer, prIME Oncology, Peer CME, Roche, Samsung Clinical trials research as principal or co-investigator (Institutional financial interests): AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Pfizer, Roche, Medimmun, Sanofi-Aventis, Taiho Pharma, Novocure, Daiichi Sankyo Travel, Accommodations, Expenses: AstraZeneca, Roche, Novartis, prIME Oncology, Pfizer
Early Stage I - IIIB
T1 T2 T3 T4
N0 N1 N2 N3
M0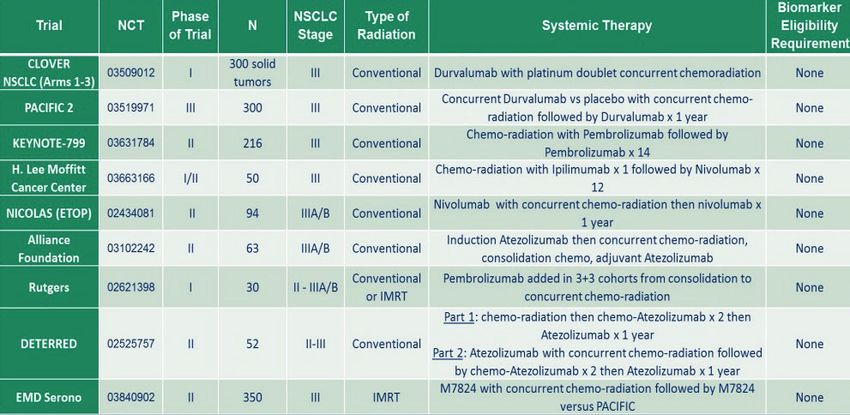
4 questions in early-stage NSCLC : PORT in completely resected early-stage N2 NSCLC ? Targeted therapy in completely resected early-stage ? IO in completely resected early-stage ? IO in unresectable early-stage ?

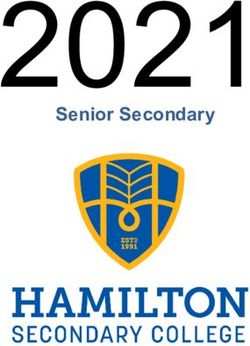
Postoperative cisplatin-based chemotherapy
significantly improves survival LACE meta-analysis
5-year absolute benefit of
5.4% from chemotherapy
Stage IA: No Adj therapy recommended
HR:0.89
Stage IB: Not for routine use
(8th TNM > 4cm : T2b ou T3, T4 : IIA-IIIA)
Stage IIA/B and IIIA: Adjuvant cisplatin-
based chemoT recommended
HR:0.84
Jean-Pierre Pignon et al, JCO 2008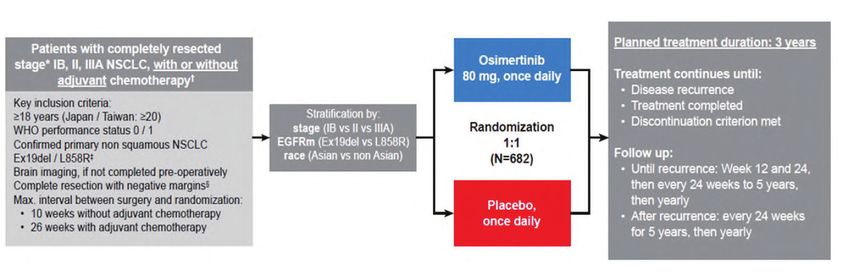
Postoperative radiotherapy
In a meta-analysis of rather old
studies PORT found to be
detrimental if given to patients
with N0 and N1 disease
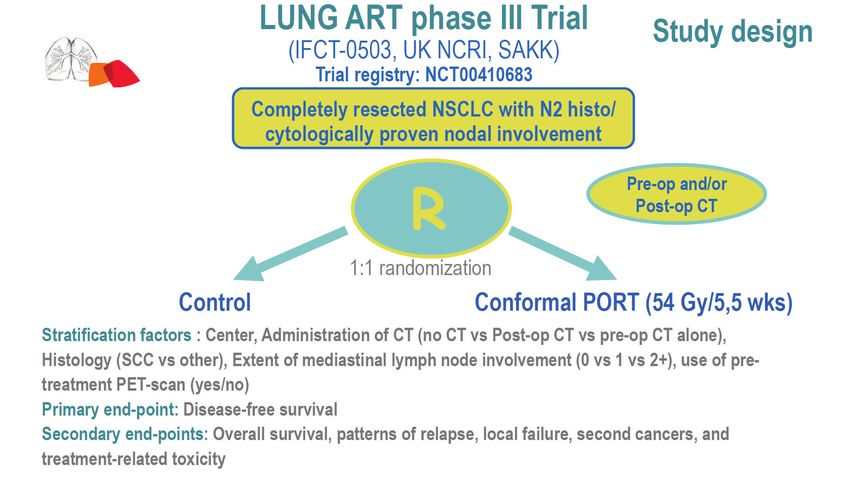
The case for unexpected N2
disease discovered at surgery is
less clear, and currently
evaluated in a large clinical trial
Cochrane Database Syst Rev 2005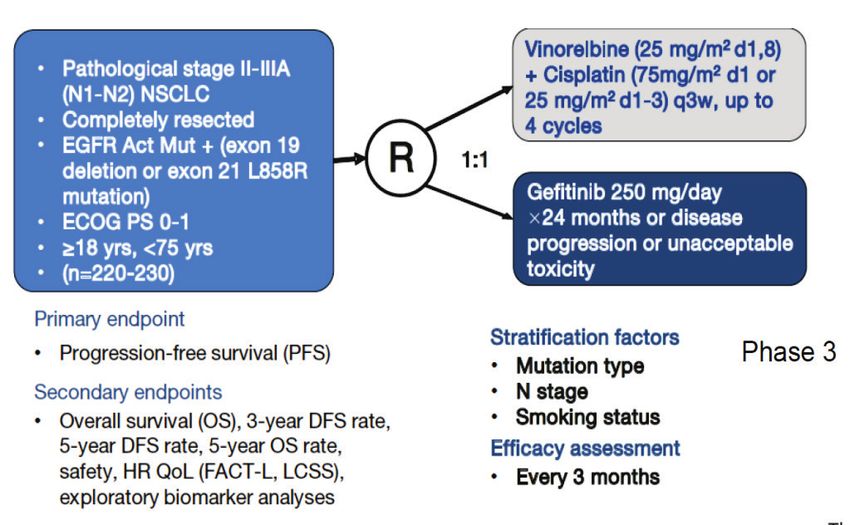
IMPACT OF POSTOPERATIVE RADIATION THERAPY ON SURVIVAL
IN PATIENTS WITH COMPLETE RESECTION (pN2)
4483 resected pts N2 30.552 pts treated for stages II–IIIA SURVIVAL IN PATIENTS WITH COMPLETE
National Cancer Data Base in National Cancer Database RESECTION AND STAGE I, II, OR IIIA
(ANITA trial)
N2 pN2
Post-op RT
CT +PORT
OS: 45.2 v 40.7 months
Cliff G. Robinson et al, JCO 2015
Christopher D. Corso et al, JTO 2015 Douillard JY et al, Radiation onco 2008
C.Le Pechoux et al ESMO 202
C.Le Pechoux et al ESMO 2020
30.5 vs 22.8mo
C.Le Pechoux et al ESMO 2020C.Le Pechoux et al ESMO 2020
3Y: 66.5 vs 68.5%
C.Le Pechoux et al ESMO 2020C.Le Pechoux et al ESMO 2020
4 questions in early-stage NSCLC : PORT in completely resected early-stage N2 NSCLC ? Not recommended Targeted therapy in completely resected early-stage ? IO in completely resected early-stage ? IO in unresectable early-stage ?
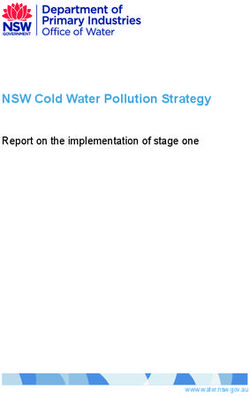
ADJUVANT trial stage II–IIIA (N1–N2)
Adjuvant gefitinib led to significantly longer DFS compared in patients with completely
resected stage II–IIIA (N1–N2) EGFR-mutant NSCLC
DFS (ITT population)(update at 3 and 5 years)
HR: 0.56
- duration of benefit with gefitinib after 24 months might be limited and overall
Zhong W.Z et al, lancet 2018 Zhong WZ et al, JCO 2020Overall survival (ITT population)
HR: 0.92
Zhong WZ et al, JCO 2020Stage IB-IIIA
Slide 5
Ramalingam SS et al, NEJM 2020DFS
stage II IIIA stage IB IIIA
HR: 0.17 HR: 0.20
Ramalingam SS et al, NEJM 2020DFS by disease stage
stage IB stage II stage IIIA
HR: 0.39 HR: 0.17 HR: 0.12
Ramalingam SS et al, NEJM 2020DFS assessment with and without adjuvant chemoT
Received adjuvant chemoT no adjuvant chemoT
HR: 0.16 HR: 0.23
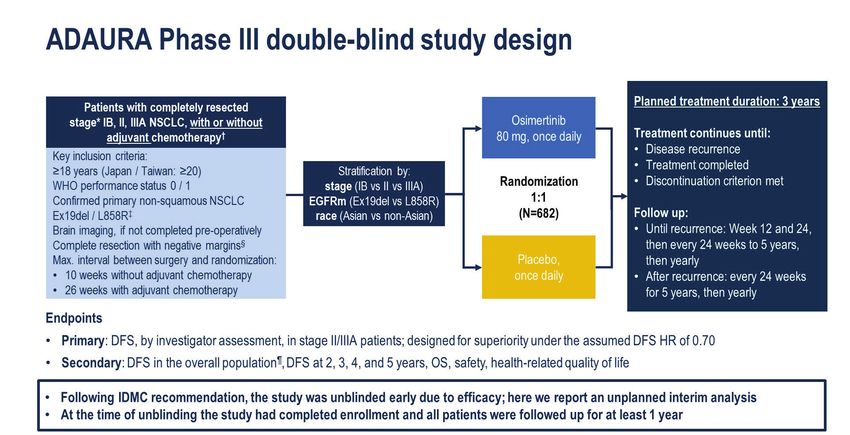
Ramalingam SS et al, NEJM 2020ADJUVANT trial II–IIIA (N1–N2) ADAURA
stage II IIIA
HR: 0.56 HR: 0.17
Ramalingam SS et al, NEJM 2020Type of disease recurrence
Masahiro Tsuboi et al, ESMO 2020Sites of disease recurrence CNS DFS in the overall population
Masahiro Tsuboi et al, ESMO 2020Post Hoc Analysis of the ADJUVANT Trial (CTONG 1104)
ChemoT
disease-free survival (CNS)
24%
HR: 0.75
Gefitinib
ChemoT
Gef
27%
Song-Tao Xu et al, JTO 2018EGFR and ALK Stage IB-IIIA NSCLC The ALCHEMIST Screening Trial ALINA Trial (ALK-Alectinib)
4 questions in early-stage NSCLC : PORT in completely resected early-stage N2 NSCLC ? Not recommended Targeted therapy in completely resected early-stage ? EGFRmut – Osimertinib: resounding justification for the rapid implementation of this approach into clinical practice IO in completely resected early-stage ? IO in unresectable early-stage ?
Neoadjuvant IO monotherapy
Neoadjuvant Chemo IO trials
Benjamin Besse et al, ESMO 2020
Partial response (RECIST1.1) :7%
Benjamin Besse et al, ESMO 2020MPR 14%
Benjamin Besse et al, ESMO 2020Benjamin Besse et al, ESMO 2020
Benjamin Besse et al, ESMO 2020
Marie Wislez et al, ESMO 2020
Marie Wislez et al, ESMO 2020
Marie Wislez et al, ESMO 2020
IO in adjuvant, phase 3 on going…
Strategy Trial Clinical Treatment Patients target Primary
phase endoint
Adjuvant IB (>4cm) -IIIA ANVIL 3 Nivo vs 714 DFS
Observation OS
Adjuvant IB (>4cm) -IIIA PEARLS 3 Pembro vs 1380 DFS
Placebo
-IIIA Impower010 3 Atezo vs BSC 1127 DFS
Adjuvant IB (>4cm) -IIA BR31 3 Durva vs 1100 DFS
placebo4 questions in early-stage NSCLC : PORT in completely resected early-stage N2 NSCLC ? Not recommended Targeted therapy in completely resected early-stage ? EGFRmut – Osimertinib: resounding justification for the rapid implementation of this approach into clinical practice IO in completely resected early-stage ? Not yet in clinical practice IO in unresectable early-stage ?
Unresectable stage III: Concurrent is superior to sequential CT-RT
Concomitant a standard of care
Progression-free
Overall Survival3
Survival3
Sequential CRT Concurrent CRT
Sequential CRT Concurrent CRT
25% 23.8% 25%
20% 18.1% 20%
15.1% 16%
15% 15% 13.1% 11.6%
10.6%
9.4%
10% 10%
5% 5%
0% 0%
3 Years 5 Years 3 Years 5 Years
Overall survival: absolute benefit
2 years 3 years 5 years
5.3% 5.7% 4.5%
Concomitant CRT is the standard of care for unresectable stage III NSCLC
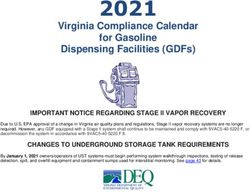
Anne Auperin et al, JCO 2010PACIFIC Trial - durvalumab vs Placebo post RTCT
UPDATED PFS
mPFS 17.2 vs 5.6 mo
Corinne Faivre-Finn et al, ESMO 2020; JTO 2021UPDATED OS
mOS: 47.5 vs 29.1 mo
Corinne Faivre-Finn et al, ESMO 2020; JTO 2021Stages I-III: immunotherapy trials
Replacing chemotherapy with IO trials ?
Concurrent immunotherapy + CTRT Trials
SBRT – immunotherapy trials (consolidation)
A.S.Tsao, ASCO 20194 questions in early-stage NSCLC : PORT in completely resected early-stage N2 NSCLC ? Not recommended Targeted therapy in completely resected early-stage ? EGFRmut – Osimertinib: resounding justification for the rapid implementation of this approach into clinical practice IO in completely resected early-stage ? Not yet in clinical practice IO in unresectable early-stage ? Consolidation with Durvalumab as a standard
MERCI ! @dplanchard
Benjamin BESSE
Thierry LE CHEVALIER
Jean-Charles SORIA
Fabrice BARLESI
Charles NALTET
Anas GAZZAH
Pernelle LAVAUD
Cécile LE PECHOUX
Angéla BOTTICELLA
Antonin LEVYPour toute information médicale sur les produits Roche, veuillez nous contacter à l’adresse :
email: morocco.medinfo@roche.com, par téléphone : 05 22 95 90 00 ou par fax : 05 22 95 90 01
Pour toute notification d’évènements indésirables, veuillez nous contacter à l’adresse :
email: morocco.drug_safety@roche.com, par téléphone : 06 61 17 83 67/ 05 22 95 90 58
ou par fax : 05 22 95 90 59
Roche Maroc S.A. Ivoire 05, Casablanca Marina Bvd Sidi Mohamed Ben Abdellah Casablanca, MAROCYou can also read