Comorbid Insomnia: Current Directions and future Challenges
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
n report n
Comorbid Insomnia: Current Directions
and Future Challenges
Thomas Roth, PhD
V
arious studies suggest that the vast majority of insomnia
patients seen in psychiatric practices, and about 50%
Abstract
of those seen in primary care practices, have comorbid
Insomnia is a leading cause of absentee-
conditions.1,2 Thus, the issue of insomnia with associ-
ism, presenteeism (lost productivity when
employees are at work), accidents, and ated comorbidities, whether the result of, as a contributing factor to,
errors in the workplace. Overall direct and or as a separate entity from the insomnia appears to be a significant
indirect costs exceed $30 billion annually. A patient as well as public health issue,3 although to what extent
significant portion of these costs are attrib- remains unclear given the lack of consistent diagnosis for insomnia in
utable to patients with comorbid insomnia,
primary care practices.4 There is also little research on the economic
making these conditions a significant clini-
cal public health issue. These comorbid
and quality-of-life repercussions of comorbid insomnia versus primary
conditions include mood and anxiety disor- insomnia, defined as insomnia with no identifiable cause.
ders; chronic pain; respiratory, urinary, and The phrase “comorbid insomnia” emerged from the 2005 National
neurologic conditions; diabetes; and car- Institutes of Health’s (NIH) State-of-the-Science Conference on
diovascular diseases. Traditional treatment Manifestations and Management of Chronic Insomnia in Adults,
for insomnia with comorbid conditions has
to describe the presence of insomnia in the context of a medical
focused on treating the comorbid condition
with the expectation that the insomnia will psychiatric disorder.3 Previously, the condition was known as “sec-
resolve. Recent studies, however, suggest ondary insomnia.” The International Classification of Sleep Disorders-2
this approach is not the most appropriate. defines it in 2 ways: “Other Insomnia Due to a Mental Disorder,”
Instead, treating both conditions simultane- for all psychiatric-related comorbidities; “Other Insomnia Due to
ously may improve the outcomes for each.
a Known Physiological Condition,” for all medical comorbidities.
(Am J Manag Care. 2009;15:S6-S13)
The former requires insomnia as well as a mental disorder classified
under the Diagnostic and Statistical Manual of Mental Disorders, Fourth
© Managed Care &
Edition (DSM-IV) criteria, with the insomnia related in time to the
Healthcare Communications, LLC
mental disorder. Although the severity of each varies together, that
of the insomnia exists beyond what might be typically expected as a
symptom of the psychiatric condition. The latter requires the pres-
ence of insomnia as well as a medical condition known to affect
sleep.5 Under DSM-IV, however, the insomnia may be “related” to an
Axis I or Axis II disorder, but the temporal continuity is not required
between the 2 disorders.6 The problem with both definitions is that
each assumes that the insomnia is “secondary” to the primary medical
or psychiatric condition. However, as articulated in the 2005 NIH
conference, the causal relationships appear to be more complex in
most disorders.3 This article explores that assumption and highlights
its implications for treatment.
Impact of Insomnia
Insomnia has a significant impact on individuals’ health and qual-
For author information and disclosures see end of text. ity of life, particularly those with comorbid conditions affecting the
central nervous system (CNS).7,8 The impact appears related to the
S6 n www.ajmc.com n february 2009Comorbid Insomnia: Current Directions and Future Challenges
effect on daytime functioning as well as the status bid insomnia compared with primary insomnia have
of their comorbid condition. For instance, various yet to be investigated, it is likely that they account for
studies found that patients with chronic insomnia the majority of the annual $30 billion to $35 billion
have significantly higher risks for falls and acci- in costs for chronic insomnia simply because comor-
dents.1,9 One study reported that 8% of workers bid insomnia is so much more prevalent.17,20
with severe insomnia were involved in industrial
accidents compared with 1% of good sleepers (P = Comorbid Insomnias: Untangling the
.0150).10 Other studies have shown sleep-onset Complexities
insomnia to be a statistically significant risk factor As noted earlier, the prevalence of comorbidi-
in being involved in a traffic accident11; in fact, ties and insomnia is significant. Kuppermann et al
those suffering from insomnia are more than twice examined the records of 369 employees together
as likely to have an automobile accident.12 with a telephone screen to evaluate various aspects
In addition, adults with severe insomnia miss of their physical and mental health and sleep
twice as many workdays as those without insomnia, quality, and found those reporting a current sleep
even when matched for work type and schedule.10 problem were 4 times more likely to have a possible
In fact, insomnia may be the greatest predictor of mental health problem as those reporting no sleep
absenteeism in the workplace.13 Employees with difficulties. They were also significantly more likely
severe insomnia have been shown to make signifi- to report gastrointestinal problems, frequent head-
cantly more errors at work (15% vs 6%; PReport
insomnia, is it incidental to the insomnia, or is rect diagnosis of comorbid versus primary insomnia
it comorbid? The complexity increases when the is particularly important when determining the
influence of sleep-related disorders on sleep quality appropriate treatment plan.
and insomnia are considered, including sleep apnea
and periodic limb movements. Similarly, circadian Medical Comorbid Conditions With Insomnia
rhythm disorders, such as shift work disorder (Drake Becoming aware of the more common comor-
Sleep) or phase delay, are associated with disturbed bidities, which encompass a wide variety of medical,
sleep. These result in insomnia symptoms and rep- psychiatric, and sleep disorders, may assist clinicians
resent special cases of comorbid insomnia. Thus, in managing the condition.
insomnia may be comorbid with medical, psychiat- Taylor et al found the following prevalence of
ric, circadian, or sleep disorders. conditions in those with chronic insomnia com-
An accurate history from the patient and pos- pared with those without insomnia: chronic pain
sibly even the bedpartner is paramount in correctly (50.4% vs 18.2%), high blood pressure (43.1%
diagnosing comorbid insomnia. Clinicians should vs 18.7%), gastrointestinal problems (33.6% vs
consider comorbid insomnia when the onset of the 9.2%), breathing problems (24.8% vs 5.7%), heart
sleep disturbances coincides with or shortly follows disease (21.9% vs 9.5%), urinary problems (19.7%
that of the comorbid condition; when the course vs 9.5%), and neurologic disease (7.3% vs 1.2%)
of the insomnia remits and recurs in conjunction (Table 1).20
with fluctuations in the comorbid disorder; or can In addition, they found that people with the
be directly linked to some feature of the comorbid following medical problems reported significantly
disorder, such as pain from chronic arthritis disrupt- more chronic insomnia than those without insom-
ing sleep. Complicating the diagnosis, however, is nia: breathing problems (59.6% vs 21.4%), gastro-
the fact that insomnia often precedes a comorbid intestinal problems (55.4% vs 20.0%), chronic pain
disorder, in some instances serving as an early warn- (48.6% vs 17.2%), high blood pressure (44.0% vs
ing sign of an occurrence or recurrence.23,24 Finally, 19.3%), and urinary problems (41.5% vs 23.3%)
it is important to consider that the treatment of the (Table 2).20
comorbid condition may lead to the insomnia. Thus, Leigh et al found insomnia in 31% to 81%
respiratory stimulants, selective serotonin reuptake of those with osteoarthritis,26 while other stud-
inhibitors (SSRIs), beta-blockers, and many other ies found high levels in those with other chronic
drugs are associated with reports of disturbed sleep. pain conditions, including rheumatoid arthritis and
Yet, as noted later in this article and in the fibromyalgia.27 Those with myocardial infarction
article by Neubauer25 in this supplement, the cor- have a 1.9 OR of mild insomnia, those with conges-
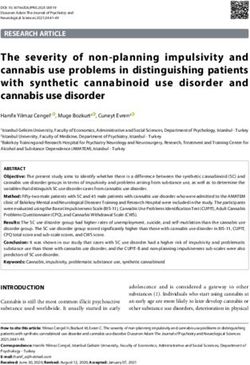
n Table 1. People With Chronic Insomnia Reporting Medical Conditions20
Prevalence
Odds Ratioa
Chronic Insomnia, (95% Confidence
Medical Condition % No Insomnia, % Interval) P
Chronic pain 50.4 18.2 3.19 (1.92-5.29)Comorbid Insomnia: Current Directions and Future Challenges
n Table 2. People With Medical Conditions Reporting Chronic Insomnia20
Prevalence
Odds Ratioa
Chronic Insomnia, No Insomnia, (95% Confidence
Medical Condition % % Interval) P
Chronic pain 48.6 17.2 2.27 (1.33-3.89)Report
The timing of insomnia vis à vis psychiatric dis- This is particularly interesting given that patients
orders may depend on the disorder itself. Most stud- with chronic insomnia do show physiologic signs of
ies find that insomnia tends to precede or appear at hyperarousal, including increased levels of cate-
the same time as a mood disorder episode (whether cholamines, increased basal metabolic rate45 and
initial episode or relapse). In one study, insomnia elevated core body temperature, altered heart rate,
preceded the onset of depression in 69% of cases increased level of CNS as well as systemic meta-
evaluated.37 In contrast, insomnia tends to appear bolic rate, and elevated fast frequency electroen-
at the same time or to follow an anxiety disorder cephalograph activity.46 Many of these variables are
episode (whether initial episode or relapse).38 also implicated in the development and progression
of cardiovascular disease.47
Insomnia and Major Depression
Several studies of comorbid insomnia show that Treating Comorbid Insomnia
depression appears as the condition most likely The treatment paradigm for comorbid insomnia
to exist in conjunction with chronic insomnia has traditionally focused on treating the medical or
(Figure).35,39-42 Patients with physician-diagnosed psychiatric disorder with the expectation that the
major depression have a 2.6 OR of mild insomnia insomnia will also resolve.48
and an 8.2 OR of severe insomnia.28 Meanwhile, This paradigm has affected treatment modalities
Pigeon et al, in evaluating elderly patients with for insomnia, with cognitive behavioral therapy
major depressive disorder (MDD) and/or dysthymia, (CBT) and hypnotics as monotherapy typically used
found that those with persistent insomnia were 1.8 only in those with primary insomnia, and psychiat-
to 3.5 times more likely to remain depressed com- ric interventions reserved for those with comorbid
pared with those without insomnia (P = .05).43 insomnia.49 It has also affected research on the
In addition to the above-reported link between appropriate treatment for comorbid insomnia.48
insomnia and depression persistence and recur- Yet while treatment may resolve most symptoms
rence, concurrent insomnia and depression may of the comorbid disorder, it often does not improve
contribute to the higher rates of cardiovascular the insomnia. Nierenberg et al reported that 45% of
disease associated with MDD and depressive symp- patients treated for 8 weeks with fluoxetine to MDD
toms.22 The Sequenced Treatment Alternatives remission still exhibited disturbed sleep. Given that
to Relieve Depression (STAR*D) study of 4041 91% of patients with posttreatment insomnia also
outpatients with MDD found cardiac disease asso- had pretreatment insomnia, the authors concluded
ciated with symptoms of sympathetic arousal and that the symptom was a residual one not related
early-morning insomnia.44 to medication side effects.50 Katz and McHorney
showed that the majority of patients with comorbid
conditions still had insomnia 2 years later.28 This
n Figure. Insomnia as a Risk Factor for Major Depressive compares to 6% in those with primary insomnia at
Disorder (MDD)35,39-42 1 year.2 They also showed that 23% developed new-
onset insomnia at the 2-year follow-up.28
Conversely, treating the insomnia as a separate
entity may prove more effective.51-55 A report of
several patients receiving CBT for posttraumatic
stress disorder (PTSD) showed the therapy success-
fully resolved the patients’ PTSD, but patients still
complained of insomnia. After CBT for insomnia,
however, their insomnia resolved.56
Other research finds that treating the insomnia
and other medical or psychiatric condition concur-
rently improves insomnia in conditions as diverse
as alcohol discontinuation,57 rheumatoid arthritis,55
menopausal-associated insomnia,53 and generalized
S10 n www.ajmc.com n february 2009Comorbid Insomnia: Current Directions and Future Challenges
anxiety disorder.58 Eaton et al hypothesized that Conclusion
47% of the incidence of depression at the 1-year The prevalence of chronic insomnia coexist-
follow-up could have been prevented by addressing ing with 1 or more psychiatric or medical condi-
existing insomnia at baseline.59 tions is significant, with particularly high rates
In addition, treating both the insomnia and the seen in patients with depression, chronic pain,
comorbid condition simultaneously may improve respiratory conditions, and diabetes. Although the
the comorbid condition more than treating it specific economic and quality-of-life repercussions
alone. Krystal et al randomized 545 patients with of comorbid insomnia have not been differenti-
insomnia and comorbid MDD to either fluoxetine ated from those with primary insomnia, they are
with nightly eszopiclone (3 mg) or placebo for 8 likely quite significant. It is clear that insomnia and
weeks followed by 2 weeks of continued fluox- comorbid conditions have a bidirectional effect,
etine plus single-blind placebo (n = 387).60 The with the status of each impacting the other, poten-
cotherapy group showed greater improvement in tially affecting the treatment course and outcome.
the 17-item Hamilton Depression Rating Scale Treating insomnia and the comorbid condition
(HAMD-17) scores at week 8 (P = .0004) than the simultaneously as separate conditions may result in
monotherapy group, an improvement that was greater improvements in each than treating either
maintained at week 10 (PReport
6. American Psychiatric Association. Diagnostic and 26. Leigh TJ, Hindmarch I, Bird HA, Wright V. Comparison
Statistical Manual of Mental Disorders. 4th ed. of sleep in osteoarthritic patients and age and sex
Washington, DC: American Psychiatric Association; matched healthy controls. Ann Rheum Dis. 1988;47(1):
1994. 40-42.
7. Roth T. Insomnia: definition, prevalence, etiology, 27. Ancoli-Israel S. The impact and prevalence of chronic
and consequences. J Clin Sleep Med. 2007;3(5 suppl): insomnia and other sleep disturbances associated
S7-S10. with chronic illness. Am J Manag Care. 2006;12(8
8. Roth T, Jaeger S, Jin R, Kalsekar A, Stang PE, Kessler
suppl):S221-S229.
RC. Sleep problems, comorbid mental disorders, and 28. Katz DA, McHorney CA. Clinical correlates of insom-
role functioning in the National Comorbidity Survey nia in patients with chronic illness. Arch Intern Med.
Replication. Biol Psychiatry. 2006;60(12):1364-1371. 1998;158(10):1099-1107.
9. Roth T. Prevalence, associated risks, and treatment 29. George CFP, Bayliff CD. Management of insomnia in
patterns of insomnia. J Clin Psychiatry. 2005;66(suppl patients with chronic obstructive pulmonary disease.
9):10-13. Drugs. 2003;63(4):379-387.
10. Leger D, Guilleminault C, Bader G, Levy E, Paillard M. 30. Phillips BA, Cooper KR, Burke TV. The effect of sleep
Medical and socio-professional impact of insomnia. loss on breathing in chronic obstructive pulmonary
Sleep. 2002;25(6):625-629. disease. Chest. 1987;91(1):29-32.
11. Sagberg F. Driver health and crash involvement: a 31. Skomro RP, Ludwig S, Salamon E, Kryger MH. Sleep
case-control study. Accid Anal Prev. 2006;38(1):28-34. complaints and restless legs syndrome in adult type 2
diabetics. Sleep Med. 2001;2(5):417-422.
12. Passaro EA. Insomnia. Last updated: October 27,
2008; http://www.emedicine.com/neuro/topic418.htm. 32. Gottlieb DJ, Punjabi NM, Newman AB, et al.
Accessed November 18, 2008. Association of sleep time with diabetes mellitus
and impaired glucose tolerance. Arch Intern Med.
13. Leigh JP. Employee and job attributes as predictors
2005;165(8):863-867.
of absenteeism in a national sample of workers: the
importance of health and dangerous working condi- 33. Mannino DM. COPD: epidemiology, prevalence, mor-
tions. Soc Sci Med. 1991;33(2):127-137. bidity and mortality, and disease heterogeneity. Chest.
2002;121(5 suppl):121S-126S.
14. Hatoum HT, Kong SX, Kania CM, Wong JM, Mendelson
WB. Insomnia, health-related quality of life and health- 34. Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence
care resource consumption. A study of managed- of diabetes and impaired fasting glucose in adults in
care organisation enrollees. Pharmacoeconomics. the U.S. population: National Health and Nutrition
1998;14(6):629-637. Examination Survey 1999-2002. Diabetes Care.
2006;29(6):1263-1268.
15. Novak M, Mucsi I, Shapiro CM, Rethelyi J, Kopp MS.
Increased utilization of health services by insomniacs— 35. Breslau N, Roth T, Rosenthal L, Andreski P. Sleep
an epidemiological perspective. J Psychosom Res. disturbance and psychiatric disorders: a longitudinal
2004;56(5):527-536. epidemiological study of young adults. Biol Psychiatry.
1996;39(6):411-418.
16. Stoller MK. Economic effects of insomnia. Clin Ther.
1994;16(5):873-897. 36. Crum RM, Storr CL, Chan Y-F, Ford DE. Sleep distur-
bance and risk for alcohol-related problems. Am J
17. Walsh JK, Engelhardt CL. The direct economic costs Psychiatry. 2004;161(7):1197-1203.
of insomnia in the United States for 1995. Sleep.
1999;22(suppl 2):S386-S393. 37. Johnson EO, Roth T, Breslau N. The association of
insomnia with anxiety disorders and depression:
18. Simon GE, VonKorff M. Prevalence, burden, and treat- exploration of the direction of risk. J Psychiatr Res.
ment of insomnia in primary care. Am J Psychiatry. 2006;40(8):700-708.
1997;154(10):1417-1423.
38. Ohayon MM, Roth T. Place of chronic insomnia in the
19. Ozminkowski RJ, Wang S, Walsh JK. The direct and course of depressive and anxiety disorders. J Psychiatr
indirect costs of untreated insomnia in adults in the Res. 2003;37(1):9-15.
United States. Sleep. 2007;30(3):263-273.
39. Chang PP, Ford DE, Mead LA, Cooper-Patrick L, Klag MJ.
20. Taylor DJ, Mallory LJ, Lichstein KL, Durrence HH, Riedel Insomnia in young men and subsequent depression.
BW, Bush AJ. Comorbidity of chronic insomnia with The Johns Hopkins Precursors Study. Am J Epidemiol.
medical problems. Sleep. 2007;30(2):213-218. 1997;146(2):105-114.
21. Kuppermann M, Lubeck D, Mazonson P, et al. Sleep 40. Dryman A, Eaton WW. Affective symptoms associ-
problems and their correlates in a working population. ated with the onset of major depression in the commu-
J Gen Intern Med. 1995;10(1):25-32. nity: findings from the US National Institute of Mental
22. Spitzer RL, Kroenke K, Linzer M, et al. Health-related Health Epidemiologic Catchment Area Program. Acta
quality of life in primary care patients with mental dis- Psychiatr Scand. 1991;84(1):1-5.
orders. Results from the PRIME-MD 1000 study. JAMA. 41. Livingston G, Blizard B, Mann A. Does sleep distur-
1995;274(19):1511-1517. bance predict depression in elderly people? A study in
23. Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang inner London. Br J Gen Pract. 1993;43(376):445-448.
NY, Klag MJ. Depression is a risk factor for coronary 42. Roberts RE, Shema SJ, Kaplan GA, Strawbridge
artery disease in men: the precursors study. Arch WJ. Sleep complaints and depression in an aging
Intern Med. 1998;158(13):1422-1426. cohort: a prospective perspective. Am J Psychiatry.
24. Perlis ML, Giles DE, Buysse DJ, Tu X, Kupfer DJ. Self- 2000;157(1):81-88.
reported sleep disturbance as a prodromal symptom in 43. Pigeon WR, Hegel M, Unützer J, et al. Is insomnia
recurrent depression. J Affect Disord. 1997;42(2-3):209- a perpetuating factor for late-life depression in the
212. IMPACT cohort? Sleep. 2008;31(4):481-488.
25. Neubauer DN. Current and new thinking in the man- 44. Fraguas R Jr, Iosifescu DV, Alpert J, et al. Major
agement of comorbid insomnia. Am J Manag Care. depressive disorder and comorbid cardiac disease:
2009;19:S24-S32. is there a depressive subtype with greater cardio-
S12 n www.ajmc.com n february 2009Comorbid Insomnia: Current Directions and Future Challenges vascular morbidity? Results from the STAR*D study. pausal insomnia: a 4-week, randomized, multicenter, Psychosomatics. 2007;48(5):418-425. double-blind, placebo-controlled study. Clin Ther. 45. Bonnet MH, Arand DL. 24-Hour metabolic rate in 2004;26(10):1578-1586. insomniacs and matched normal sleepers. Sleep. 54. Fava M, McCall WV, Krystal A, et al. Eszopiclone co- 1995;18(7):581-588. administered with fluoxetine in patients with insom- 46. Roth T. A physiologic basis for the evolution of nia coexisting with major depressive disorder. Biol pharmacotherapy for insomnia. J Clin Psychiatry. Psychiatry. 2006;59(11):1052-1060. 2007;68(suppl 5):13-18. 55. Walsh JK, Muehlbach MJ, Lauter SA, Hilliker NA, 47. Kamarck TW, Everson SA, Kaplan GA, et al. Schweitzer PK. Effects of triazolam on sleep, daytime Exaggerated blood pressure responses during mental sleepiness, and morning stiffness in patients with rheu- stress are associated with enhanced carotid athero- matoid arthritis. J Rheumatol. 1996;23(2):245-252. sclerosis in middle-aged Finnish men: findings from 56. DeViva JC, Zayfert C, Pigeon WR, Mellman TA. the Kuopio Ischemic Heart Disease Study. Circulation. Treatment of residual insomnia after CBT for PTSD: 1997;96(11):3842-3848. case studies. J Trauma Stress. 2005;18(2):155-159. 48. Stepanski EJ, Rybarczyk B. Emerging research on 57. Le Bon O, Murphy JR, Staner L, et al. Double-blind, the treatment and etiology of secondary or comorbid placebo-controlled study of the efficacy of trazodone in insomnia. Sleep Med Rev. 2006;10(1):7-18. alcohol post-withdrawal syndrome: polysomnographic 49. Buysse DJ, Reynolds CF 3rd, Kupfer DJ, et al. Effects of and clinical evaluations. J Clin Psychopharmacol. diagnosis on treatment recommendations in chronic 2003;23(4):377-383. insomnia—a report from the APA/NIMH DSM-IV field 58. Pollack M, Kinrys G, Krystal A, et al. Eszopiclone coad- trial. Sleep. 1997;20(7):542-552. ministered with escitalopram in patients with insomnia 50. Nierenberg AA, Keefe BR, Leslie VC, et al. Residual and comorbid generalized anxiety disorder. Arch Gen symptoms in depressed patients who respond acutely Psych. 2008;65(5):551-562. to fluoxetine. J Clin Psychiatry. 1999;60(4):221-225. 59. Eaton WW, Badawi M, Melton B. Prodromes and 51. Asnis GM, Chakraburtty A, DuBoff EA, et al. Zolpidem precursors: epidemiologic data for primary preven- for persistent insomnia in SSRI-treated depressed tion of disorders with slow onset. Am J Psychiatry. patients. J Clin Psychiatry. 1999;60(10):668-676. 1995;152(7):967-972. 52. Nolen WA, Haffmans PM, Bouvy PF, Duivenvoorden HJ. 60. Krystal A, Fava M, Rubens R, et al. Evaluation of Hypnotics as concurrent medication in depression. A eszopiclone discontinuation after cotherapy with fluox- placebo-controlled, double-blind comparison of fluni- etine for insomnia with coexisting depression. J Clin trazepam and lormetazepam in patients with major Sleep Med. 2007;3(1):48-55. depression, treated with a (tri)cyclic antidepressant. 61. Manber R, Edinger JD, Gress JL, et al. Cognitive J Affect Disord. 1993;28(3):179-188. behavioral therapy for insomnia enhances depression 53. Dorsey CM, Lee KA, Scharf MB. Effect of zolpidem on outcome in patients with comorbid major depressive sleep in women with perimenopausal and postmeno- disorder and insomnia. Sleep. 2008;31:489-495. VOL. 15, No. 1 n The American Journal of Managed Care n S13
You can also read