Neurofibromatosis Type 1: Review and Update on Emerging Therapies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
R EVIEW A RTICLE
Neurofibromatosis Type 1:
Review and Update on Emerging Therapies
Tanya Karaconji, FRANZCO,*† Eline Whist, BMed, MPHTM, FRANZCO,*‡
Robyn V. Jamieson, PhD, FRACP,§¶ǁ**Maree P. Flaherty, FRANZCO, FRACS, FRCOphth,*††
and John R.B. Grigg, MD, FRANZCO*¶ǁ‡‡
this complex disorder will be discussed in this review.
Abstract: Neurofibromatosis type 1 (NF1) is an autosomal dominant
neurocutaneous disorder affecting 1:3000 births. This familial tumor pre-
disposition syndrome is diagnosed clinically and affects the skin, bones, EPIDEMIOLOGY
and nervous system. Malignant tumors can arise in childhood or adult- Neurofibromatosis 1 is one of the most common genetic dis-
hood and are the commonest cause of mortality in this population. Early orders with no sex or racial predilection. It occurs in approximate-
diagnosis and management led by a multidisciplinary team remains the ly 1 in 3000 people.3 Estimates of the prevalence of NF1 range
standard of care, particularly in the management of optic pathway glioma. from 1/21904 to 1/7800.5 Some of the difficulties with accurate
Emerging concepts in the genetic patterns of this condition have led to the prevalence data for this condition may be due to ascertainment
introduction of new treatment modalities that target the mitogen activated bias6 partly due to the wide variability in the expression of the
protein kinase (MAPK) and the mammalian target of rapamycin (mTOR) condition, whereby mild cases may escape study inclusion par-
pathways. The role of the ophthalmologist and approach to screening for ticularly in studies dependent on an affected individual coming to
optic pathway glioma is outlined based on previous recommendations. medical attention.7 Reduced prevalence in later adulthood may be
Updates on choroidal involvement, as a diagnostic criterion, will also be due to increased mortality seen in individuals with NF1 or to un-
discussed, further highlighting the pivotal role of the ophthalmologist in derascertainment of adult patients.8 The physician Mark Akenside
the diagnosis and management of this complex condition. first recognized the disorder in 1768. Robert Smith, an Irish sur-
geon, published further details on the disease in 1849. However,
Key Words: NF1, choroidal nodules, optic pathway glioma, it was the German pathologist Friedrich von Recklinhausen who
phakomatoses is credited with its recognition in 1882.1
(Asia-Pac J Ophthalmol 2018;0:0–0)
GENETICS AND PATHOPHYSIOLOGY
The inheritance of NF1 is autosomal dominant with 100%
N eurofibromatosis 1 (NF1) is an inherited neurocutaneous
disorder. It is characterized by the presence of multisystem
tumors throughout the skin and central nervous system (CNS),
penetrance but highly variable expressivity.1,3,9 Importantly, a
high spontaneous mutation rate of up to 42% exists.3 The NF1
gene is located on chromosome 17q11.2 and was cloned in 1990.
which carries a risk of malignant transformation.1 The hallmark It was originally cloned by the Wallace group10 along with the
clinical features of NF1 include multiple café au lait macules, Cawthon and Viskochil group.11 It is an important tumor suppres-
neurofibromas, intertriginous freckling, osseous lesions, Lisch sor gene found throughout the nervous system.12
nodules, and optic pathway gliomas.2 An evolving understanding The NF1 gene encodes the protein neurofibromin, which
of both the genetic and newly recognized ophthalmic features of influences multiple signalling pathways affecting many cellular
processes throughout the body. Importantly, it acts as a negative
regulator of cell growth and proliferation.2 Several pathways are
From the *Discipline of Ophthalmology, Save Sight Institute, Sydney Medical
School, University of Sydney, Sydney, Australia; †Manchester Royal Eye
thought to be involved in the development of tumors associat-
Hospital, Manchester, United Kingdom; ‡Royal Darwin Hospital, Darwin, ed with NF1. Loss of neurofibromin increases rat sarcoma viral
Australia; §Disciplines of Paediatrics, Genomic Medicine and Ophthalmology,
Sydney Medical School, University of Sydney; ¶Eye Genetics Research
oncogene homologue (RAS) activity. This increased RAS ac-
Unit, Children’s Medical Research Institute, University of Sydney, Sydney; tivity causes unopposed cell growth and activation of important
ǁSave Sight Institute and Eye Genetics Clinics, The Children’s Hospital at
Westmead; **Westmead Hospital, Sydney; ††Department of Ophthalmology,
downstream intermediates such as the mitogen activated protein
The Children’s Hospital at Westmead, Sydney; and ‡‡Sydney Eye Hospital, kinase (MAPK) and the mammalian target of rapamycin (mTOR)
Sydney, Australia.
Received for publication May 1, 2018; accepted August 23, 2018.
pathways.2,9
J.R.B.G. and R.V.J. are supported in part by NHMRC Centre for Research Neurofibromin is also involved in the regulation of cyclic
Excellence APP1116360. E.W. is supported in part by Sydney Eye Hospital
Foundation.
adenosine monophosphate levels, which has been shown to affect
The other authors have no funding or conflicts of interest to declare. the CNS in animal models, importantly in optic pathway glioma
Reprints: Tanya Karaconji, FRANZCO, Discipline of Ophthalmology, Save Sight
Institute, Sydney Medical School, University of Sydney, NSW 2006, Australia.
formation.12–14
E‑mail: tkaraconji.@gmail.com. Although NF1 may result in a combination of benign and
Copyright © 2018 by Asia-Pacific Academy of Ophthalmology
ISSN: 2162-0989
malignant tumors of the central and peripheral nervous system,
DOI: 10.22608/APO.2018182 the initial event in tumor formation is the germline mutation
Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018 www.apjo.org | 1
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.
Karaconji et al Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018
in the NF1 tumor-suppressor gene. The “second hit” in this Skin
“2-hit hypothesis” pathway is a somatic mutation, causing loss Café au lait macules and skin fold freckling do not usually
of heterozygosity of the NF1 gene, and consequently leading to cause complications and have no malignant potential.23 They are
Schwann cell neurofibromas along with other tumors.9 an important component of the diagnostic criteria. Café au lait
patches are usually the first identified clinical manifestation in
NF1.24 They are usually present within the first 2 years of life.18
CLINICAL PRESENTATION They present as well-defined hyperpigmented macular lesions
Neurofibromatosis 1 is a neurocutaneous disorder with an that are generally absent from the scalp and eyebrows along with
age-dependent, variable clinical presentation. This often leads to the palms and soles (Fig. 2).18 Histologically these lesions are due
difficultly in establishing an early diagnosis. Despite this, NF1 to increased proliferation of epidermal melanocytes with basal
has well-recognized diagnostic criteria as outlined by points 1 to hyperpigmentation of the epidermis.
7 in Table 1.15 Although these “classical” criteria are widely used Axillary and inguinal freckling usually presents after the de-
and agreed upon, recent years have seen additional new cutane- velopment of café au lait macules by the age of 5–8.24 Typically,
ous and extracutaneous features described (Table 1). An example they present as small freckles less than 5 mm in size in the axillary
of this is the presence of unidentified bright objects on imaging. or inguinal area.18,24,25 They may also present in areas where skin
These are seen as hyperintense lesions on T2 weighted brain folds are in apposition, including the neck and under the breasts in
magnetic resonance imaging (MRI) images, which may represent women.7 These are given the eponymous name, Crowe sign, after
aberrant gliosis pathognomonic of NF1.16 Additionally, advanced the physician Frank Crowe who first described their association
molecular analysis is now available, refining our knowledge of
the NF1 gene mutation.17
TABLE 1. National Institutes of Health (NIH) Diagnostic Criteria for
A small subset of patients present with a somatic mutation or
“segmental” NF1 where the clinical features only affect a specific NF12,6,9,14,15 and Other Common Findings.
area of the body and neither parent is affected.18 Other phenotyp- The NIH Diagnostic Criteria Are Met if 2 or More of the
ic presentations in patients with an NF1 gene mutation include Following Are Found
neurofibromatosis-Noonan syndrome, which may occur in up to
12% of these patients. Clinical features are an overlap between 1. 6 or more café au lait macules over 5 mm in greatest diameter in
the 2 named syndromes and include the Noonan features of short prepubertal individuals and over 15 mm in greatest diameter in
stature, ocular hypertelorism, low-set ears, and downslanting pal- postpubertal individuals
pebral fissures.19 2. 2 or more neurofibromas of any type or 1 plexiform neurofibroma
3. Freckling in the axillary or inguinal regions
Lisch Nodules 4. Optic glioma
Austrian ophthalmologist Karl Lisch in 1937 was the first 5. 2 or more Lisch nodules (iris hamartomas)
to emphasise what are now called Lisch nodules and their as- 6. A distinctive osseous lesion such as sphenoid dysplasia or thin-
sociation with NF1.20 Histologically Lisch nodules are melano- ning of long bone cortex
cytic hamartomas, consisting of a condensation of spindle cells 7. A first degree relative with NF1 by above criteria
on the anterior iris surface. Stromal iris nevi underlie the pig-
mented nodules.21 They are present on the anterior iris surface or Nondiagnostic Cutaneous and Extracutaneous Signs to Consider
in the angle. They are well-defined yellow-brown dome-shaped in Addition to the “Classical” Diagnostic Criteria When
elevated lesions and can range in size from pinpoint to large Evaluating Patients With NF1
(Fig. 1).20,22 Lisch nodules do not cause ocular morbidity or
disability but are important, as they are one of the diagnos- Genetic analysis Molecular analysis of the NF1 gene
tic criteria for NF1. Their presence is age-dependent. Although Cutaneous signs Anemic nevus
they are unusual before the age of 2, they are seen in half of Juvenile xanthogranuloma
5-year-olds, 75% of 15-year-olds, and almost 100% of adults over Mixed vascular hamartomas and
the age 30.22 cherry angiomas
Hypochromic macules
“Soft-touch” skin
Hyperpigmentation
Extra-cutaneous Choroidal hamartomas
Large head circumference &
hypertelorism
Unidentified bright objects on
neuroimaging
Cerebrovascular dysplasia,
moyamoya
Learning, speech and behavioural
disabilities, headache and
seizures
Neoplasms
FIGURE 1. Slit lamp photograph demonstrating multiple Lisch nodules.
2 | www.apjo.org © 2018 Asia-Pacific Academy of Ophthalmology
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.
Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018 Emerging Therapies for NF1
Unlike cutaneous neurofibromas, plexiform neurofibromas
can infiltrate surrounding soft tissue and arise from multiple nerve
fascicles, with multiple discrete tumors forming along nerve
trunks.23 Growth of these tumors is often unpredictable and is
usually rapid during the first decade of life, resulting in significant
disfigurement and functional impairment.25 Palpebral plexiform
neurofibromas typically affect the upper eyelid unilaterally ap-
pearing in infancy or early childhood and may result in significant
functional impairment including amblyopia.25 This may be due to
a mechanical ptosis causing astigmatism. As always in pediatric
patients, regular refraction, dilated examination, and amblyopia
treatment are of utmost importance, particularly in NF1 patients
presenting with eyelid plexiform neurofibromas.
Unfortunately, MPNST have a poor prognosis with a 5-year
survival of up to 60%, warranting ongoing careful surveillance
with a low threshold for investigation.31 Poor prognosis is associ-
ated with early metastasis and poor response to systemic chemo-
therapy. Delayed diagnosis remains an issue. Features including
increased growth rate, irregular contour, and pain in existing neu-
FIGURE 2. Café au lait macules.
rofibromas are symptoms and signs that may indicate malignant
transformation. These symptoms may also be present in benign
with café au lait macules in the diagnosis of NF1 in 1964.26 lesions.31,32
Although a histological diagnosis remains the gold standard
Neurofibromas in differentiating benign from malignant lesions, imaging with
Neurofibromas are a hallmark feature of NF1, present in al- positron emission tomography and computed tomography com-
most all patients over the age of 30.25 They are benign soft tissue bined with a flurodeoxyglucose tracer provides a noninvasive
tumors of Schwann cell origin that arise on peripheral nerves.27 In technique to identify malignant transformation based on in vivo
addition to neoplastic Schwann cells, they also contain fibroblasts, glucose metabolism.31 Definitive diagnosis of a MPNST does re-
macrophages, and mast cells.28 Clinically, neurofibromas can be quire pathological identification.
further classified as cutaneous, subcutaneous, or plexiform. The
latter can be further divided into nodular or diffuse. The features Neurofibroma Treatment
of each are outlined in Table 2.24 Although they typically present Plexiform neurofibromas are notoriously difficult to treat
symptomatically on the skin, they can also develop deep within surgically due to their infiltration of adjacent normal tissue and
the body and may remain largely asymptomatic.24 the commonly reported risk of regrowth after excision.33 Targeted
Like most features in NF1, the presence of neurofibromas chemotherapeutic agents such as imatinib (tyrosine kinase inhib-
is age-dependent. Although neurofibromas tend to increase with itor) have also been studied but have only demonstrated a modest
age, the presence of plexiform neurofibromas may manifest at reduction in tumor volume size in a phase 2 trial in affected pa-
birth and are most active during the first decade of life, develop- tients with clinically significant plexiform neurofibromas due to
ing in 25% to 50% of individuals with NF1.29 NF1.34 Interferons exert antitumor activity via a number of mech-
The morbidity associated with plexiform neurofibromas is anisms including antiproliferative, antiangiogenesis, and cytotox-
2-fold. In addition to the disfigurement, bony destruction, and ic effects. A phase 1 trial of pegylated interferon-alpha-1beta in
pain associated with these lesions, they also carry an 8–13% young patients with progressive and unresectable plexiform neu-
lifetime risk of malignant transformation [malignant periph- rofibromas has demonstrated a promising reduction and stabiliza-
eral nerve sheath tumors (MPNST)].23,24 This rate of malignant tion of plexiform neurofibroma size.35
transformation is higher than previously thought.30 Clinical trials with biologic agents including mTOR and
TABLE 2. Clinical Features of Established Neurofibroma Subtypes17–19
Neurofibroma Types Location Clinical Signs Presentation
Cutaneous Epidermis and dermis Moves with skin, blueish tinge, local Asymptomatic; most common type;
pruritis. Size range ~2 mm to 3 cm. presents in late teens
Subcutaneous Deep to dermis Skin moves over, firm and rounded feel, Tenderness on palpation; tingling in
located along peripheral nerves. distribution of affected nerve
Size 3–4 cm.
Nodular plexiform Localized interdigitation “Bag of worms” feel May be present from birth, enlarges
with normal tissues during first decade of life
Diffuse plexiform Infiltrate widely and deeply Smooth slightly irregular skin
thickening
© 2018 Asia-Pacific Academy of Ophthalmology www.apjo.org | 3
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.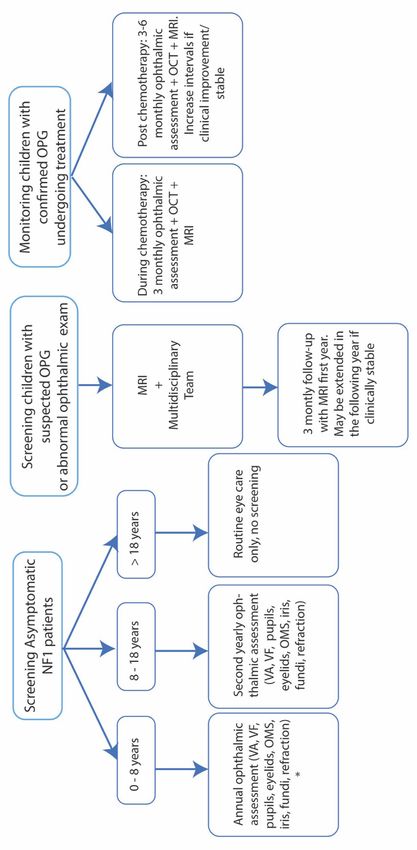
Karaconji et al Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018
mitogen-activated protein kinase kinase (MEK) inhibitors are involvement as a new diagnostic criterion for NF1. In particular,
underway.36 Studies looking at MEK inhibitors in mouse models the use of NIR imaging to detect these choroidal abnormalities is
have demonstrated that blocking MEK signalling was sufficient gaining increasing interest particularly among ophthalmologists
to profoundly shrink existing neurofibromas.37 Clinical trials with as a possible screening tool, as it is noninvasive and can be ap-
MEK inhibitors for plexiform neurofibromas are ongoing or in plied to the pediatric population, at least in older children.46,47
development and will allow further evaluation of the utility of the Additional choroidal changes that have also been described
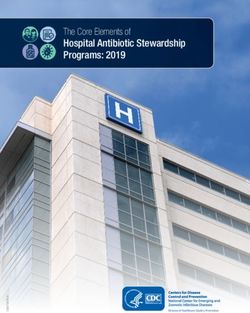
mouse model in predicting response in humans. include a reduction in mean choroidal thickness, which may be
Although these studies have shown promising results in related to altered choroidal circulation in the presence of choroi-
plexiform neurofibromas, unfortunately they have only demon- dal nodules (Fig. 4).48 Another case report has identified increased
strated a transient benefit in the treatment of MPNST in mice mod- subfoveal choroidal thickness in a case of NF1.49 Pigmentary ha-
els.36,38 In contrast, mTOR pathway inhibitors such as rapamycin matomas (choroidal nevi) may also involve the posterior uveal
suppress the growth of these MPNST but have not demonstrated tract in up to 30% of affected patients.50
tumor regression.39 The mTOR pathway is critically deregulated Although the association of glaucoma and neurofibromato-
in NF1 mutant MPNSTs, hence the role of mTOR inhibitors.39 sis has been described in the literature as a rare association, the
However, when combined with heat shock protein 90 (HSP90) mechanism is not well understood and is most likely related to
inhibitors, potent tumor regression is observed.40 angle closure.25,51,52 A retrospective histological study by Edwards
et al51 analyzed the eyes from 5 patients with NF1 and glaucoma,
Anterior Segment and Uvea ranging in age from birth to 13 years. They identified endotheli-
The presence of choroidal abnormalities in neurofibroma- alization of the anterior chamber angle, which they hypothesized
tosis was reported as early as the 1930s.41 These lesions were may be related to overexpression of the RAS-MAPK genes in
identified on enucleated specimens and attributed to proliferating these eyes.51 Clinically, infiltration of the iris and angle with neu-
Schwann cells arranged as concentric rings around axons.42,43 rofibromas may obstruct the angle resulting in secondary angle
More recently, a number of case series have used confocal closure.25 Other anterior segment features include congenital ec-
near-infrared reflectance (NIR) imaging as a means of identifying tropion uvea, iris heterochormia, developmental anomaly of the
these choroidal lesions in NF1 patients.44–47 In each of these stud- angle, and posterior embryotoxon, which may all predispose to
ies, the choroidal abnormalities identified were not visualized by glaucoma.51 Interestingly, Morales et al53 found ipsilateral glau-
simple ophthalmoscopic examination or fundus fluorescein angi- coma and increased axial length in 23% of 95 patients with orbi-
ography.46 Further studies have found that these choroidal abnor- tofacial involvement.
malities tend to increase with age and are particularly localized
around the posterior pole.45 Skeletal Anomalies
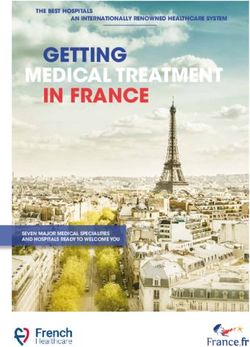
Near-infrared reflectance imaging at 815 nm and optical co- A number of skeletal manifestations are recognized in NF1
herence tomography (OCT) have further elucidated the presence patients. These may present as either generalized or focal bony
of these choroidal bright patchy nodules in patients with NF1.46 abnormalities. Generalized bony changes include osteopenia,
Viola et al46 found choroidal bright patches in 82% of NF1 pa-
tients compared with only 7% of normal controls with a diag-
nostic sensitivity of 83% and specificity of 96%. These choroidal A
abnormalities have been further categorized as either “dome-
shaped” or “placoid-like.”48 These lesions are also reported at a
high frequency in pediatric NF1 patients.47 The appearance of
these lesions on NIR imaging is demonstrated in Figure 3.
These studies highlight the potential importance of choroidal
B
FIGURE 3. The NIR images of the right and left eyes of a patient with
NF1 demonstrating bright patchy areas localized to the posterior pole
and vascular arcade. White arrows indicate 2 of multiple lesions in FIGURE 4. Choroidal changes in a patient with NF1 as seen on NIR
each eye (images courtesy of Francesco Viola Università degli Studi di imaging. Corresponding OCT through the choroidal lesions in the right
Milano). (A) and left (B) eye.
4 | www.apjo.org © 2018 Asia-Pacific Academy of Ophthalmology
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.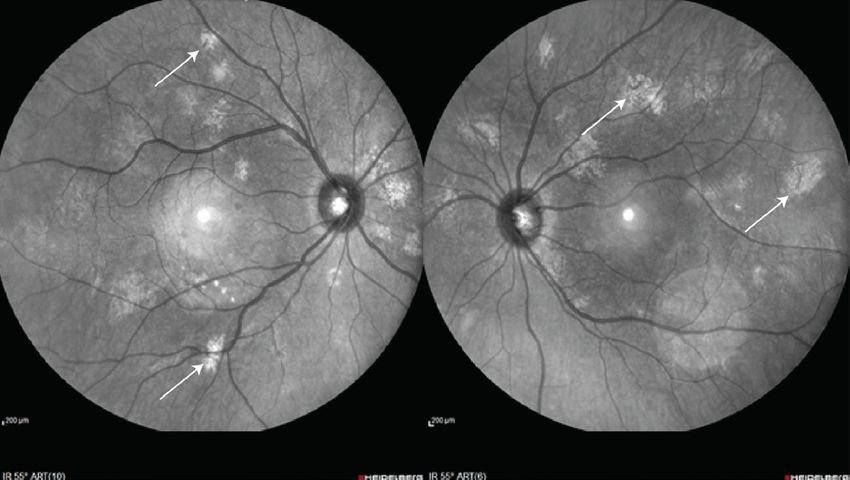
Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018 Emerging Therapies for NF1
short stature, and macrocephaly.36 In NF1 patients older than 40, TABLE 3. Characteristic Features of the Most Common Type of OPG in
a 5-fold increase in fracture risk has been reported, with a 3-fold NF113,54
risk in children younger than 16.54
Focal bony abnormalities include tibial dysplasia/pseu- Features Pilocytic astrocytoma
doarthrosis (2%), sphenoid wing dysplasia (1–6%), scoliosis Histological features GFAP-staining in cell cytoplasm
(10–15%), nonossifying fibrosis, pectus deformities of the chest, and presence of Rosenthal fibers;
and rarely, defects in the occipital bone.24,36,55 Of particular signif- contains piloid cells and astrocytes
icance to the ophthalmologist is the presence of sphenoid wing Incidence (per 0.48
dysplasia that may present with asymmetric orbits, proptosis, or 100,000 per year)
enophthalmos.24 More specifically, these patients usually present Association with NF1 Mainly OPG (50%)
with pulsatile proptosis due to herniation of the temporal lobe into Age 5–19 y
the orbit.23 Importantly, absence or thinning of the sphenoid wing WHO grade I
may be due to the presence of an orbital plexiform neurofibroma.24 Location Cerebellum/brainstem/optic pathway
Though the mechanisms underlying these osseous mani-
festations remain poorly understood, studies have demonstrated
that neurofibromin plays a critical role in regulating mesenchy- presentations. Many OPGs are asymptomatic. They may become
mal stem/progenitor cell differentiation into osteoblasts, affecting evident either as a result of patient signs or symptoms or as an
collagen synthesis and mineralization.36,56 A defect in this process incidental finding on ‘‘baseline’’ neuroimaging studies.66 A study
is likely to contribute in part to some of these clinical features. by Listernick et al67 in 1989 demonstrated that, if all children with
Ideally, specialized pediatric orthopedic surgeons should manage NF1 undergo screening neuroimaging, 15% of them will have ra-
these children. diographic evidence of OPG with only half of these children de-
veloping symptoms or signs related to the OPG.60,67,68 Symptomat-
Optic Pathway Gliomas ic OPG in children with NF1 generally result in decreased visual
Optic pathway gliomas (OPGs) account for 5% of pediat- acuity, diminished visual fields, abnormal pupillary function, or
ric intracranial tumors.57 Traditional figures suggest that from proptosis. It is important to note that young children rarely com-
15–20% of children with NF1 will develop a low-grade glial plain of vision loss, necessitating the use of reliable, reproducible
neoplasm.58,59 A large retrospective review of 861 patients seen measures to detect visual changes.58 Reduction in visual acuity
at the tertiary referral neurofibromatosis clinic at the Children’s is the most common finding on screening.61 Other less common
Hospital at Westmead in Sydney found a prevalence of 6.6% in ocular presentations include strabismus, proptosis, nystagmus,
their population.60 afferent pupil defect, and abnormal color vision.61 Clinically, the
Optic pathway gliomas can occur anywhere in the brain or optic discs usually appear pale. Low-grade glial tumors may also
spine in children with NF1; however, they are most common in present with systemic manifestations such as precocious puberty
the optic pathway, hypothalamus, and (to a lesser extent) brain- or rarely, diencephalic syndrome.68 Although it is extremely rare,
stem.24,61 The traditional Dodge classification (DC) of OPGs the latter may occur in cases with tumor involvement of the thal-
proposed in 195862 defines tumors anatomically as involving the amus or hypothalamus and presents with failure to thrive, vomit-
optic nerves alone (stage 1), the chiasm with or without nerve ing, headaches, and vision abnormalities.69
involvement (stage 2), and the hypothalamus or other adjacent Minimum requirements for cranial MRI at diagnosis include
structures (stage 3). The DC has long been used to select patients T2-weighted, T1-weighted, and gadolinium contrast–enhanced
for resection of optic nerve tumors and to provide an important T1-weighted sequences and flair-attenuated inversion recovery.
indicator of prognosis with tumors at the optic chiasm having a This is used to diagnose and monitor progression of these tumors.
poorer outcome. More recently, a modified DC has introduced an Typical features include fusiform enlargement, tortuosity, and
imaging-based method using MRI scans and is referred to as the kinking of the optic nerves. There may also be involvement of the
PLAN score.63 This updated score provides a more detailed ana- chiasm (best visualized on coronal sections), optic tract, or optic
tomical description that can help to categorize and select tumors radiation with diffuse enlargement.70 Optic pathway gliomas are
at higher risk of visual morbidity to better guide treatment and isointense or slightly hypointense to normal optic nerve on T1 im-
detect change. The study by Taylor et al63 found that NF1-positive aging and hyperintense on T2 imaging71,72 (Fig. 5). Although they
cases more commonly involved both optic nerves and multiple may demonstrate gadolinium enhancement, not all do. Abnormal
locations at other sites whereas NF1-negative tumors more com- perineural tissue within the nerve sheath may also be present.71,72
monly involved the central chiasm and the hypothalamus. Most The screening guidelines and management pathways of patients
will be diagnosed before 6 years of age,61 though other series have with NF1 are outlined in Figure 6.60,61
found that up to 30% of children presented with OPGs after the
age of 6.60,64 Table 3 outlines the features of the most common Treatment
subtype, pilocytic astrocytoma (PA). Although PAs are common Current imaging is virtually always diagnostic, so biopsy
in NF1 patients and usually follow an indolent course, they may of suspected tumors is no longer warranted.70 Surgery is rec-
spontaneously resolve without intervention.36,65 Pilomyxoid as- ommended for OPG cases with severe vision loss and disfigur-
trocytoma, another subtype, is less common in the context of ing proptosis only when assessed by a multidisciplinary team,
NF1.2 Neurofibromatosis 1–associated OPGs have active MAPK as surgery in NF1 OPG is rarely useful and will often sacrifice
signalling and rarely transform into high-grade tumors with no whatever vision remains.73
malignant potential.2 A combination of carboplatin-based chemotherapy, often
These tumors may have a wide range of clinical in conjunction with vincristine, remains the gold standard for
© 2018 Asia-Pacific Academy of Ophthalmology www.apjo.org | 5
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.Karaconji et al Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018
centers at the same frequency as neuroimaging. These provide
A B additional objective evidence for visual pathway dysfunction
when performed in laboratories experienced with visual electro-
physiology in children. Multifocal visual evoked potentials offer
a method for assessing the topographic optic nerve function, pro-
viding an objective measure of visual field function.79,80 Optical
coherence tomography of the optic nerve has also proved to be an
effective, noninvasive tool to assess for progressive retinal nerve
fiber layer thinning secondary to OPGs in NF1 patients; though it
is not considered standard surveillance, it has proved a potential
biomarker of vision in NF1 OPGs.59,81
The decision on when to treat children with OPGs remains
FIGURE 5. A, MRI brain (T2 coronal): bilateral optic nerve enlargement
controversial and relies on input from a multidisciplinary team.
with tortuosity. B, T2 axial MRI brain and orbits demonstrating Treatment is reserved for progressive disease, which may include
enlargement and tortuosity of both optic nerves, consistent with an either reduced vision or radiographic tumor growth, or a combi-
optic pathway glioma. nation of the 2.59,70
NF1-associated low-grade gliomas requiring treatment.74 The CNS and Other Systems
5-year progression-free survival in these patients has been shown
to be as high as 69%.74 This regime also has lower toxicity and Other CNS Tumors
side effect profile than other comparable agents.74 Other tradi- Gliomas can present throughout the CNS in individuals with
tional chemotherapeutic agents have also been associated with a NF1.73 It is important to recognize that among patients with NF1
worrisome risk of secondary malignancies.36 In recurrent, refrac- who are older than age 10, the relative risk of a brain tumor is
tory tumors alternative agents such as vinblastine have proven 100 times higher than in patients without NF1.82 Most brain tu-
to be efficacious, although it is poorly tolerated due to extensive mors in children with NF1 are low-grade gliomas [World Health
bone marrow suppression in many patients.36 Pretreatment vision Organization (WHO) grade I–II], and the majority of those are
is an important prognostic indicator of final visual acuity after WHO grade I.9 These tumors do have malignant potential and can
chemotherapy.36 infiltrate the brain.9
Newer therapies targeting inhibitors of MEK and mTOR Brainstem gliomas associated with NF1 have been described
pathways are currently under trial.70 Drugs targeting tumor angio- and, in contrast to the general population, they tend to have a
genesis, such as bevacizumab, have shown objective responses more indolent course and may not require treatment.83
radiologically and on vision testing in cases of refractory OPG.75
A study by Avery et al76 in 2014 looked at the use of intravenous Non–CNS Tumors
bevacizumab in 4 cases of pediatric OPGs who demonstrated pro- A range of other, non–CNS tumors has also been reported in
gressive visual acuity or visual field loss despite prior treatment patients with NF1 including pheochromocytomas, which may ini-
with chemotherapy or proton-beam radiotherapy. All 4 subjects tially present with hypertension.9 Gastrointestinal fibromas have
demonstrated a marked improvement in their visual acuity, vi- also been described.9
sual field, or both while receiving bevacizumab-based therapy.76 The lifetime breast cancer risk is 4 times higher in women
Although further studies are required, this presents a promising with NF1 who are under the age of 50 compared with the general
treatment in addition to standard therapies. The Pediatric Brain population.84 Women with NF1 also have an increased risk for
Tumour Consortium study is currently evaluating the use of selu- invasive breast cancer, across all age groups.84
metinib, an MEK inhibitor, in children with recurrent or refracto-
ry low-grade gliomas with promising results.77 Learning Difficulties; Speech, Language, and Cognitive
Impairment
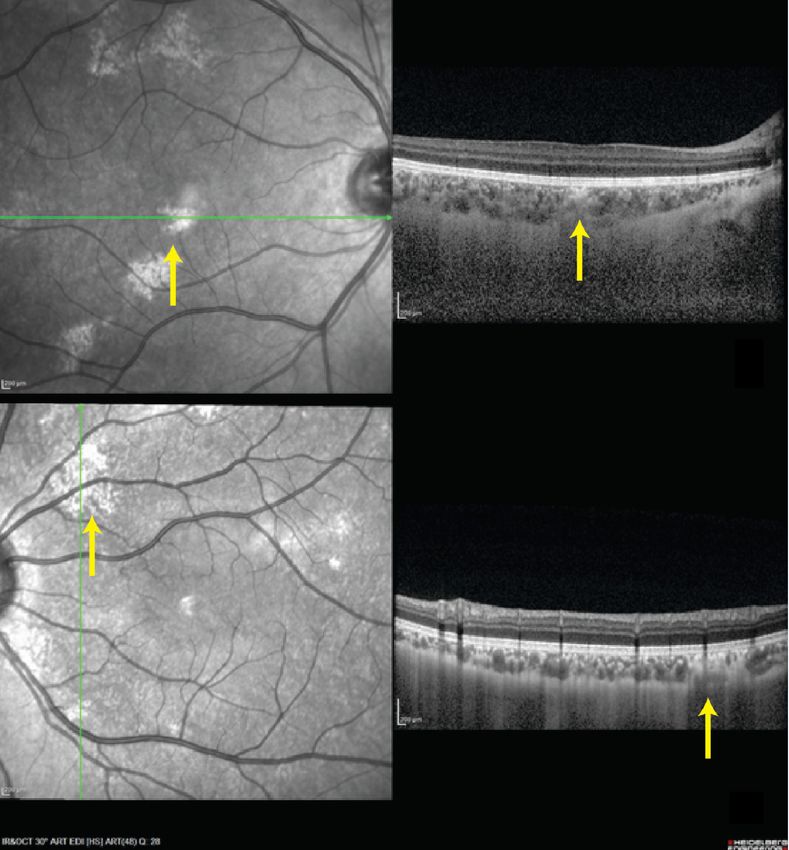
Screening for Optic Pathway Tumors in NF1 Learning difficulties and cognitive impairment remain the
One of the critical roles that ophthalmology plays in the commonest NF1 neurological complication in children. The
management of children with NF1 is the regular monitoring and mean full-scale intelligence quotient (IQ) is in the low to average
screening for OPGs. Given the high frequency of learning and be- range.23 The incidence of true cognitive delay in NF1 is, how-
havioral problems in NF1 children, this regular screening should ever, lower than expected.85 There are increased rates of autism
be in the context of a multidisciplinary team.23 spectrum disorder, attention deficit hyperactivity, and sleep dis-
Routine screening remains the commonest means to identify turbances in these patients.86 Language difficulties, particularly
OPGs.61 The neuro-ophthalmic examination is a key component receptive language and language structure, have been identified
in the diagnosis and management of OPGs. In children with NF1, as issues in children with NF1.87 In view of these findings, ear-
examination guidelines have been developed by expert consen- ly neuropsychological screening assessment to help evaluate and
sus58 and are outlined in Figure 6. The Response Evaluation in support these children as they enter school should be considered.24
Neurofibromatosis and Schwannomatosis Visual Outcomes Com- This also supports the need for ongoing routine screening, which
mittee recommends that visual acuity should be the primary out- is best performed in dedicated NF multidisciplinary clinics.
come measure to assess for tumor progression, guide treatment
decisions, and evaluate treatment effect.78 Vascular Complications
Pattern visual evoked potentials are performed in some A number of cardiovascular abnormalities have also been
6 | www.apjo.org © 2018 Asia-Pacific Academy of Ophthalmology
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018 Emerging Therapies for NF1
FIGURE 6. Proposed screening guidelines and management pathways of patients with NF1. If unable to accurately assess a child clinically, then
there may be a role for neuroimaging. Some centers do perform baseline neuroimaging in new diagnosis NF1. MDT indicates multidisciplinary team
(pediatrician, neurologist, oncologist, neurosurgery, geneticist); OMS, ocular movements; VA, visual acuity; VF, visual fields (age-appropriate).
described in NF1 patients. Congenital heart disease, particularly ACKNOWLEDGMENT
pulmonary stenosis, accounts for as many as 50% of these abnor- The authors would like to thank Francesco Viola, Università
malities.88 Other NF1-related vascular abnormalities include re- degli Studi di Milano, UO Oculistica, Fondazione IRCCS Cà
nal and cerebral artery stenosis, moyamoya, aneurysmal lesions, Granda Ospedale Maggiore Policlinico, Milan, Italy, who con-
and arteriovenous fistula malformations.36 tributed OCT images.
Interestingly, both adult and pediatric patients with NF1 have
a significantly increased risk of stroke when compared with the
general population.89 Although the risk is most notable for hemor- REFERENCES
rhagic strokes, it is also increased for ischemic strokes in children 1. Tadini G, Milani D, Menni F, et al. Is it time to change the neurofibromatosis
due to a number of underlying vascular lesions.89,90 Various asso- 1 diagnostic criteria? Eur J Intern Med. 2014;25:506–510.
ciations have included moyamoya arteriopathy,91 cerebral aneu- 2. Helfferich J, Nijmeijer R, Brouwer OF, et al. Neurofibromatosis type 1
rysms, and ectatic cerebral vessels.90 associated low grade gliomas: a comparison with sporadic low grade
gliomas. Crit Rev Oncol Hematol. 2016;104:30–41.
Prognosis 3. Kissil J, Blackeley J, Ferner R, et al. What's new in neurofibromatosis?
In children with NF1-associated OPG after chemotherapy, Proceedings from the 2009 NF Conference: new frontiers. Am J Med Genet
approximately a third will regain some vision with treatment.92 A. 2010;152A:269–283.
Unlike vision, which will largely remain stable or may even 4. Fuller LC, Cox B, Gardner RJ. Prevalence of von Recklinghausen
improve, NF1 reduces average life expectancy by 10–15 years, neurofibromatosis in Dunedin, New Zealand. Neurofibromatosis. 1989;2:
and malignant tumors are the most common cause of death in 278–283.
individuals with this syndrome.7 It is important to remember 5. Sergeyev AS. On the mutation rate of neurofibromatosis. Humangenetik.
that NF1 patients have a 5-fold risk for cancer and more than a 1975;28:129–138.
2000-fold risk for neurogenic malignancies compared with the 6. Friedman JM. Epidemiology of neurofibromatosis type 1. Am J Med Genet.
general population.93 1999;89:1–6.
7. Rasmussen S, Freidman J. NF1 gene and neurofibromatosis 1. Am J
Epidemiol. 2000;151:33–40.
CONCLUSIONS 8. Clementi M, Barbujani G, Turolla L, et al. Neurofibromatosis-1: a maximum
As NF1 remains a multisystem disease with life-threatening likelihood estimation of mutation rate. Hum Genet. 1990;84:116–118.
complications, a multidisciplinary approach with close collabo- 9. Brems H, Beert E, de Ravel T, et al. Mechanisms in the pathogenesis of
ration among NF1 clinicians will facilitate a uniform method for malignant tumours in neurofibromatosis type 1. Lancet Oncol. 2009;10:
diagnosis and management of this condition. Ophthalmologists 508–515.
have a crucial role in diagnosis and in monitoring visual function. 10. Marchuk DA, Saulino AM, Tavakkol R, et al. cDNA cloning of the type 1
The recent characterization of the choroidal hamartomas empha- neurofibromatosis gene: complete sequence of the NF1 gene product.
sizes this role. Genomics. 1991;11:931–940.
Despite the recent and exciting new advances in NF1 re- 11. Cawthon RM, Weiss R, Xu GF, et al. A major segment of the
search, including MEK and mTOR inhibitors, there still remain neurofibromatosis type 1 gene: cDNA sequence, genomic structure, and
many questions about the disease. The continuing challenge for point mutations. Cell. 1990;62:193–201.
clinicians is the detection of progression of OPG as early as pos- 12. Rodriguez F, Stratakis CA, Evans D. Genetic predisposition to peripheral
sible so that effective treatment can be instigated to maximize the nerve neoplasia: diagnostic criteria and pathogenesis of neurofibromatosis,
preservation of vision. Carney comple and related syndromes. Acta Neurophthol. 2012;123:
© 2018 Asia-Pacific Academy of Ophthalmology www.apjo.org | 7
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.Karaconji et al Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018
349–367. alpha-2b in young patients with plexiform neurofibromas. Neurology. 2011;
13. Buchanan ME, Davis RL. A distinct set of drosophilis brain neurons 76:265–272.
required for NF type 1-dependant learning and memory. J Neurosci. 2010; 36. Widemann BC, Acosta MT, Ammoun S, et al. CTF meeting 2012:
30:10135–10143. translation of the basic understanding of the biology and genetics of NF1,
14. Warrington NM, Gianino SM, Jackson E, et al. Cyclic AMP suppression in NF2, and schwannomatosis toward the development of effective therapies.
sufficient to induce glioma-genesis in a mouse model in NF 1. Cancer Res. Am J Med Genet A. 2014;164A:563–578.
2010;70:5717–5727. 37. Jessen WJ, Miller SJ, Jousma E, et al. MEK inhibition exhibits efficacy in
15. NIH. National Institutes of Health consensus development conference human and mouse neurofibromatosis tumors. J Clin Invest. 2013;123:
statement: neurofibromatosis. Arch Neurol. 1988;45:575–580. 340–347.
16. DiPaolo DP, Zimmerman RA, Rorke LB, et al. Neurofibromatosis type 1: 38. Patel AV, Eaves D, Jessen WJ, et al. Ras-driven transcriptome analysis
pathologic substrate of high-signal-intensity foci in the brain. Radiology. identifies aurora kinase A as a potential malignant peripheral nerve sheath
1995;195:721–724. tumor therapeutic target. Clin Cancer Res. 2012;18:5020–5030.
17. Sabbagh A, Pasmant E, Imbard A, et al. NF1 molecular characterization 39. Johannessen CM, Johnson BW, Williams SM, et al. TORC1 is essential for
and neurofibromatosis type 1 genotype-phenotype correlation: the French NF1-associated malignancies. Curr Biol. 2008;18:56–62.
experience. Hum Mutat. 2013;34:1510–1518. 40. De Raedt T, Walton Z, Yecies JL, et al. Exploiting cancer cell vulnerabilities
18. Riccardi VM. Von Recklinghausen neurofibromatosis. N Engl J Med. 1981; to develop a combination therapy for ras-driven tumors. Cancer Cell. 2011;
305:1617–1627. 20:400–413.
19. De Luca A, Bottillo I, Sarkovzy A, et al. NF1 gene mutations represent the 41. Freeman D. Neurofibroma of the choroid. Arch Ophthalmol. 1934;11:
major molecular event underlying neurofibromatosis-Noonan syndrome. Am 641–645.
J Hum Genet. 2005;77:1092–1101. 42. Woog JJ, Albert DM, Craft J, et al. Choroidal ganglioneuroma in
20. Lubs M, Bauer MS, Formas M, et al. Lisch nodules in neurofibromatosis neurofibromatosis. Graefes Arch Clin Exp Ophthalmol. 1983;220:25–31.
type 1. N Engl J Med. 1991;324:1264–1266. 43. Kurosawa A, Kurosawa H. Ovoid bodies in choroidal neurofibromatosis.
21. Williamson TH, Garner A, Moore AT. Structure of Lisch nodules in Arch Ophthalmol. 1982;100:1939–1941.
neurofibromatosis type 1. Ophthalmic Paediatr Genet. 1991;12:11–17. 44. Yasunari T, Shiraki K, Hattori H, et al. Frequency of choroidal
22. Ragge NK, Falk, R, Cohen WE, et al. Images of Lisch nodules across the abnormalities in neurofibromatosis type 1. Lancet. 2000;356:988–992.
spectrum. Eye (Lond). 1993;7(Pt 1):95–101. 45. Nakakura S, Shiraki K, Yasunari T, et al. Quantification and anatomic
23. Ferner R, Huson S, Thomas N, et al. Guidelines for the diagnosis and distribution of choroidal abnormalities in patients with type I
management of individuals with neurofibromatosis 1. J Med Genet. 2007; neurofibromatosis. Graefes Arch Clin Exp Ophthalmol. 2005;243:980–984.
44:81–88. 46. Viola F, Villani E, Natacci F, et al. Choroidal abnormalities detected
24. Hirbe AC, Gutmann D. Neurofibromatosis type 1: a multidisciplinary by near-infrared reflectance imaging as a new diagnostic criterion for
approach to care. Lancet Neurol. 2014;13:834–843. neurofibromatosis 1. Ophthalmology. 2012;119:369–375.
25. Abdolrahimzadeh B, Piraino DC, Albanese G, et al. Neurofibromatosis: an 47. Vagge A, Camicione P, Capris C, et al. Choroidal abnormalities in
update of ophthalmic characteristics and applications of optical coherence neurofibromatosis type 1 detected by near-infrared reflectance imaging in
tomography. Clin Ophthalmol. 2016;10:851–860. paediatric population. Acta Ophthalmol. 2015;93:e667–e671.
26. Crowe FW. Axillary freckling as a diagnostic aid in neurofibromatosis. Ann 48. Abdolrahimzadeh S, Felli L, Plateroti R, et al. Morphologic and vasculature
Intern Med. 1964;61:1142–1143. features of the choroid and associated choroid-retinal thickness alterations
27. Hajdu SI. Peripheral nerve sheath tumours. Histogenesis, classification, and in neurofibromatosis type 1. Br J Ophthalmol. 2015;99:789–793.
prognosis. Cancer. 1993;72:3549–3552. 49. Rao RC, Choudhry N. Enhanced depth imaging spectral-domain optical
28. Munchhof AM, Li F, White HA, et al. Neurofibroma-associated growth coherence tomography findings in choroidal neurofibromatosis. Ophthalmic
factors activate a distinct signaling network to alter the function of Surg Lasers Imaging Retina. 2014;45:466–468.
neurofibromin-deficient endothelial cells. Hum Mol Genet. 2006;15: 50. Huson S, Jones D, Beck L. Ophthalmic manifestations of
1858–1869. neurofibromatosis. Br J Ophthalmol. 1987;71:235–238.
29. Prada CE, Rangwala FA, Martin LJ, et al. Pediatric plexiform 51. Edward DP, Morales J, Bouhenni R, et al. Congenital ectropion uvea and
neurofibromas: impact on morbidity and mortality in neurofibromatosis mechanisms of glaucoma in neurofibromatosis type 1. Ophthalmology.
type 1. J Pediatr. 2012;160:461–467. 2012;119:1485–1494.
30. Evans DG, Baser ME, McGaughran J, et al. Malignant peripheral nerve 52. Al Freihi SH, Edward DP, Nowilaty SR, et al. Iris neovascularization and
sheath tumours in neurofibromatosis 1. J Med Genet. 2002;39:311–314. neovascular glaucoma in neurofibromatosis type 1: report of 3 cases in
31. Tovmassian D, Razak MA, London K. The role of [18F]FDG-PET/CT in children. J Glaucoma. 2013;22:336–341.
predicting malignant transformation of plexiform neurofibromas in 53. Morales J, Chaudhry IA, Bosley TM. Glaucoma and globe enlargement
neurofibromatosis-1. Int J Surg Oncol. 2016;2016:6162182. associated with neurofibromatosis type 1. Ophthalmology. 2009;116:1725–
32. Stucky CC, Johnson KN, Gray RJ, et al. Malignant peripheral nerve sheath 1730.
tumors (MPNST): the Mayo Clinic experience. Ann Surg Oncol. 2011;19: 54. Heervä E, Koffert A, Jokinen E, et al. A controlled register-based study of
878–885. 460 neurofibromatosis 1 patients: increased fracture risk in children and
33. Needle MN, Cnaan A, Dattilo J, et al. Prognostic signs in the surgical adults over 41 years of age. J Bone Miner Res. 2012;27:2333–2337.
management of plexiform neurofibroma: the Children's Hospital of 55. Raj A, Krishnapada B, Ghosh S, et al. Neurofibromatosis 1. Ophthalmology.
Philadelphia experience, 1974-1994. J Pediatr. 1997;131:678–682. 2009;116:598–599.
34. Robertson KA, Nalepa G, Yang FC, et al. Imatinib mesylate for plexiform 56. Wu X, Estwick S, Chen S, et al. Neurofibromin plays a critical role in
neurofibromas in patients with neurofibromatosis type 1: a phase 2 trial. modulating osteoblast differentiation of mesenchymal stem/progenitor cells.
Lancet Oncol. 2012;131:678–682. Hum Mol Genet. 2006;15:2837–2845.
35. Jakacki RI, Dombi E, Potter DM, et al. Phase I trial of pegylated interferon- 57. Rakotonjanahary J, De Carli E, Delion M, et al. Mortality in children with
8 | www.apjo.org © 2018 Asia-Pacific Academy of Ophthalmology
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.Asia-Pacific Journal of Ophthalmology • Volume 0, Number 0, Month 2018 Emerging Therapies for NF1
optic pathway glioma treated with up-front BB-SFOP chemotherapy. PLOS children with optic pathway gliomas treated with bevacizumab. JAMA
One. 2015;10:e0127676. Ophthalmol. 2014;132:111–114.
58. Listernick R, Ferner RE, Liu GT, et al. Optic pathway gliomas in 77. Banerge A, Jakacki RI, Onar-Thomas A, et al. A phase I trial of the MEK
neurofibromatosis-1: controversies and recommendations. Ann Neurol. inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or
2007;61:189–198. refractory low-grade glioma: a Pediatric Brain Tumor Consortium (PBTC)
59. de Blank PM, Fisher MJ, Lui GT, et al. Optic pathway gliomas in study. Neuro Oncol. 2016;19:1135–1144.
neurofibromatosis type 1: an update: surveillance, treatment indications, and 78. Fisher MJ, Avery RA, Allen JC, et al. Functional outcome measures for
biomarkers of vision. J Neuro-Ophthalmol. 2017;37:S23–S32. NF1-associated optic pathway glioma clinical trials. Neurology. 2013;
60. Thiagalingam S, Flaherty M, Billson F, et al. Neurofibromatosis type 1 and 81(Suppl 1):S15–S24.
optic pathway gliomas: follow-up of 54 patients. Ophthalmology. 2004;111: 79. Balachandran C, Klistorner AI, Billson F. Multifocal VEP in children: its
568–577. maturation and clinical application. Br J Ophthalmol. 2004;88:226–232.
61. Fisher MJ, Avery RA, Allen JC, et al. Functional outcome measures for 80. Klistorner AI, Graham SL, Grigg J, et al. Objective perimetry using the
NF1-associated optic pathway glioma clinical trials. Neurology. 2013; multifocal visual evoked potential in central visual pathway lesions. Br J
81(Suppl 1):S15–S24. Ophthalmol. 2005;89:739–744.
62. Dodge HW, Love JG, Graig VM, et al. Gliomas of the optic nerves. AMA 81. Chang L, El-Dairi MA, Frempong TA, et al. Optical coherence tomography
Arch NeurPsych. 1958;79:607–621. in the evaluation of neurofibromatosis type-1 subjects with optic pathway
63. Taylor T, Jaspan T, Gregson R, et al. Radiological classification of optic gliomas. J AAPOS. 2010;14:511–517.
pathway gliomas: experience of a modified functional classification system. 82. Gutmann DH, Rasmussen SA, Wolkenstein P, et al. Gliomas presenting
Br J Radiol. 2008;81:761–766. after age 10 in individuals with neurofibromatosis type 1 (NF1). Neurology.
64. Segal L, Darvish-Zagar M, Dilenge ME, et al. Optic pathway gliomas in 2002;59:759–761.
patients with neurofibromatosis type 1: follow-up of 44 patients. J AAPOS. 83. Milstein JM, Geyer JR, Berger MS, et al. Favorable prognosis for
2010;14:155–158. brainstem gliomas in neurofibromatosis. J Neurooncol. 1989;7:367–371.
65. Parazzini C, Triulzi F, Bianchini E, et al. Spontaneous involution of optic 84. Sharif S, Moran A, Duson S, et al. Women with neurofibromatosis 1 are at
pathway lesions in neurofibromatosis type 1: serial contrast MR evaluation. a moderately increased risk of developing breast cancer and should be
AJNR Am J Neuroradiol. 1995;16:1711–1718. considered for early screening. J Med Genet. 2007;44:481–484.
66. King A, Listernick R, Charrow J, et al. Optic pathway gliomas in 85. Huson SM, ed. The Neurofibromatoses: Pathogenic and Clinical Overview.
neurofibromatosis type 1: the effect of presenting symptoms on outcome. London: Chapman and Hall; 1994.
Am J Med Genet. 2003;122A:95–99. 86. Johnson H, Wiggs L, Stores G, et al. Psychological disturbance and sleep
67. Listernick R, Charrow J, Greenwald MJ, et al. Optic gliomas in children disorders in children with neurofibromatosis type 1. Dev Med Child Neurol.
with neurofibromatosis type 1. J Pediatr. 1989;114:788–792. 2005;47:237–242.
68. Listernick R, Darling C, Greenwald M, et al. Optic pathway tumors in 87. Brei NG, Klein-Tasman BP, Schwarz GN, et al. Language in young children
children: the effect of neurofibromatosis type 1 on clinical manifestations with neurofibromatosis-1: relations to functional communication, attention,
and natural history. J Pediatr. 1995;127:718–722. and social functioning. Res Dev Disabil. 2014;35:2495–2504.
69. Cavicchiolo ME, Opocher E, Daverio M, et al. Diencephalic syndrome as 88. Lin AE, Birch P, Korf BR, et al. Cardiovascular malformations and other
sign of tumor progression in a child with neurofibromatosis type 1 and optic cardiovascular abnormalities in neurofibromatosis 1. Am J Med Genet.
pathway glioma: a case report. Childs Nerv Syst. 2013;29:1941–1945. 2000;95:108–117.
70. Avery RA, Fisher MJ, Liu GT. Optic pathway gliomas. J Neuroophthalmol. 89. Terry AR, Jordan JT, Schwamm L, et al. Increased risk of cerebrovascular
2011;31:269–278. disease among patients with neurofibromatosis type 1. Stroke. 2016;47:
71. Imes RK, Hoyt WF. Magnetic resonance imaging signs of optic nerve 60–65.
gliomas in neurofibromatosis 1. Am J Ophthalmol. 1991;111:729. 90. Rosser TL, Vezina G, Packer RJ. Cerebrovascular abnormalities in a
72. Brodsky MC. The "pseudo-CSF" signal of orbital optic glioma on magnetic population of children with neurofibromatosis type 1. Neurology. 2005;64:
resonance imaging: a signature of neurofibromatosis. Surv Ophthalmol. 553–555.
1993;38:213–218. 91. Koss M, Scott RM, Irons MB, et al. Moyamoya syndrome associated
73. Korf BR. Malignancy in neurofibromatosis type 1. Oncologist. 2000;5: with neurofibromatosis type 1: perioperative and long-term outcome after
477–485. surgical revascularization. J Neurosurg Pediatr. 2013;11:417–425.
74. Dodgshun A, Maixner WJ, Heath JA, et al. Single agent carboplatin for 92. Fisher MJ, Loguidice M, Gutmann DH, et al. Visual outcomes in children
pediatric low-grade glioma: a retrospective analysis shows equivalent with neurofibromatosis type 1-associated optic pathway glioma following
efficacy to multiagent chemotherapy. Int J Cancer. 2016;138:481–488. chemotherapy: a multicenter retrospective analysis. Neuro Oncol. 2012;14:
75. Packer RJ, Jakacki R, Horn M, et al. Objective response of multiply 790–797.
recurrent low-grade gliomas to bevacizumab and irinotecan. Pediatr Blood 93. Peltonen S, Kallionpaa RA, Peltonen J. Neurofibromatosis type 1 (NF1)
Cancer. 2009;52:791–795. gene: beyond café au lait spots and dermal neurofibromas. Exp Dermatol.
76. Avery RA, Hwang EI, Jakacki RI, et al. Marked recovery of vision in 2016;26:645–648.
© 2018 Asia-Pacific Academy of Ophthalmology www.apjo.org | 9
Copyright © 2018 Asia-Pacific Academy of Ophthalmology. Unauthorized reproduction of this article is prohibited.You can also read