New Treatments for Type 2 Diabetes: Implications of Cardiovascular Outcome Trials
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
New Treatments for Type 2 Diabetes:
Implications of Cardiovascular Outcome Trials
Richard Pratley, M.D.
Samuel Crockett Chair in Diabetes Research
Director, Florida Hospital Diabetes Institute
Senior Investigator, Translational Research Institute
Adjunct Professor, Sanford Burnham Prebys Medical Discovery Institute
Orlando, Florida
Neal B et al. N Engl J Med. 2017 Jun 12.
Disclosures
Advisory Board / Consultant: Boehringer-Ingleheim,
GSK, Lilly, Merck, Novo Nordisk, Pfizer, Takeda
Research Support: Lexicon, Lilly, Merck, Novo Nordisk,
Pfizer, Sanofi, Takeda
All honoraria directed toward a non-profit which
supports education and research
Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practice
Multiple Metabolic Defects Contribute to
Hyperglycemia in T2DM
Islet -cell
Decreased
Incretin Effect
Increased
Impaired Lipolysis
Insulin Secretion
Islet -cell
Increased Increased Glucose
Glucagon Secretion Reabsorption
Increased
Decreased Glucose
HGP
Neurotransmitter Uptake
Dysfunction
From DeFronzo, Diabetes: 2009
Type 2 Diabetes: A Progressive Disease
Type 2
Normal IGT Diabetes
Complications Disability
Death
Prediabetes Clinical Complications
state disease
86 million 29 million
Primary Secondary Tertiary
Prevention Prevention Prevention
IGT = impaired glucose tolerance
CDC National Diabetes Statistics Report, 2014. www.CDC.gov
Microvascular Complications of T2DM
● In 2005-2008, of adults ≥40 years of age with diabetes, 4.2
million (28.5%) had diabetic retinopathy.
655,000 (4.4%) had advanced diabetic retinopathy
● In 2010, about 73,000 non-traumatic lower-limb
amputations were performed in adults ≥20 years of age
with diabetes.
● About 60% of non-traumatic lower-limb amputations
among adults ≥20 years of age are in people with
diabetes.
● Diabetes was listed as the primary cause of kidney
failure in 44% of all new cases in 2011.
Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its
Burden in the United States, 2014. Atlanta, GA: U.S. Department of Health and Human Services; 2014.
Diabetes Doubles the Risk for Vascular
Outcomes
Number
of Cases HR (95% CI) I2 (95% CI)
Coronary heart disease* 26,505
2.00 (1.83–2.19) 64 (54–71)
Coronary death 11,556 2.31 (2.05–2.60) 41 (24–54)
Nonfatal MI 14,741 1.82 (1.64–2.03) 37 (19–51)
Stroke subtypes*
Ischemic stroke 3,799 2.27 (1.95–2.56) 1 (0–20)
Hemorrhagic stroke 1,183 1.56 (1.19–2.05) 0 (0–26)
1.84 (1.59–2.13) 33 (12–48)
Unclassified stroke 4,973
1.73 (1.51–1.98) 0 (0–26)
Other vascular deaths 3,826
1 2 4
HR = hazard ratio; CI = confidence interval; MI = myocardial infarction.
Emerging Risk Factors Collaboration. Lancet. 2010;375(9733):2215–2222.
12 Classes of Antihyperglycemic
Agents for T2DM
A1c Hypo- Weight Dosing
Class Other Safety Issues
Reduction glycemia Change (times/day)
GI, lactic acidosis, B12
Metformin 1.5 No Neutral 2
deficiency
Basal insulin analog 1.5–2.5 Yes Gain 1, injected Hypoglycemia
Rapid-acting insulin 1.5–2.5 Yes Gain 1-4,injected
Sulfonylureas 1.5 Yes Gain 1 Allergies, secondary failure
Thiazolidinediones 0.5–1.4 No Gain 1 Edema, CHF, bone fractures
Short-acting GLP-1 RAs 0.5–1.0 No Loss 2, injected GI, ? pancreatitis, ARF
Long-acting GLP-1 RAs ~1.5 No Loss 1, injected GI, ? pancreatitis, ?MTC, ?ARF
Repaglinide 1–1.5 Yes Gain 3
Nateglinide 0.5–0.8 Rare Gain 3
Alpha-glucosidase inhibitors 0.5–0.8 No Neutral 3 GI
Amylin mimetics 0.5–1.0 No Loss 3, injected GI
DPP-4 inhibitors 0.6–0.8 No Neutral 1 Pancreatitis
Bile acid sequestrant 0.5 No Neutral 1 or 2 GI
Bromocriptine quick release 0.7 No Neutral 1 GI
SGLT2s 0.8-1.0 No Loss 1 Genital mycotic infections
GI = gastrointestinal; GLP-1 = glucagon-like peptide-1; RA = receptor agonist; CHF = congestive heart failure; ARF = acute renal failure; MTC
= medullary thyroid carcinoma; DPP-4 = dipeptidyl peptidase-4; SGLT2 = sodium-dependent glucose cotransporter -2.
Adapted from: Nathan DM, et al. Diabetes Care. 2007;30(3):753-759. Nathan DM, et al. Diabetes Care. 2006;29(8):1963-1972. Nathan DM, et al.
Diabetes Care. 2009;32(1):193-203. ADA. Diabetes Care. 2008;31:S12-S54. Buse J, et al. Lancet. 2009;374(9683):39-47.
Complementary Mechanisms of Action of
Current Diabetes Medications
GLP-1 RA
Insulin Islet -cell DPP-4 inhibitors
Sulfonylureas
Megltinides Decreased
Incretin Effect
Increased
Impaired Lipolysis
Insulin Secretion
Islet -cell
SGLT-2
inhibitors
GLP-1 RA
DPP-4 inhibitors
Increased Increased Glucose
Glucagon Secretion Reabsorption
Metformin TZDs
Increased
Bromocryptine
Decreased Glucose
HGP
Neurotransmitter Uptake
Dysfunction
From DeFronzo, Diabetes: 2009
Properties of Established Anti-
Hyperglycemic Agents
Class Mechanism Advantages Disadvantages Cost
Biguanides • Activates AMP- • Extensive experience • Gastrointestinal Low
(Metformin) kinase • No hypoglycemia • Lactic acidosis
• Hepatic • Weight neutral • B-12 deficiency
glucose production • ? CVD events • Contraindications
SUs / • Closes KATP • Extensive experience • Hypoglycemia Low
Meglitinides channels • Microvascular risk • Weight gain
• Insulin • Low durability
secretion • ? Ischemic
preconditioning
TZDs • Activates PPAR- • No hypoglycemia • Weight gain Low
• Insulin • Durability • Edema / heart
sensitivity • TGs, HDL-C failure
• ? CVD events (pio) • Bone fractures
• ? MI (rosi)
• ? Bladder ca (pio)
Diabetes Care 2012;35:1364–1379. Diabetologia 2012;55:1577–1596The Incretin Defect in T2DM
Substantial impairment – 40% of normal response
Not due to impaired secretion of GLP-1 or GIP
Absent insulinotropic response to GIP
Beta-cell GIP receptor down-regulation
Decreased response to GLP-1
Can be overcome by achieving higher than physiologic GLP-1
levels
GLP-1 infusions that achieve higher levels effective at
enhancing insulin secretion and suppressing glucagon
in a glucose-dependent manner
Nauck et al. Diabetologia. 1986;29:46–52. Laakso et al. Diabetologia. 2008;51:502‐11. Nauck et al. Diabetologia. 2011;54:10‐8.
Højberg et al. Diabetologia. 2009;52:199‐207. Vilsbøll et al. Diabetologia. 2002;45:1111–19. Nauck et al. Diabetologia.
1993;36:741–44.Incretin Therapies to Treat T2DM
Incretin effect is impaired in T2DM
Natural GLP-1 has extremely short half-life
Add GLP-1 analogues Block DPP-4, the
with longer half-life:
enzyme that degrades
Injectables GLP-1:
Oral agents
• Sitagliptin
Exendin-4 Based: Human GLP-1:
• Saxagliptin
• Exenatide • Liraglutide
• Linagliptin
• Exenatide QW • Albiglutide
• Alogliptin
• Dulagutide
Drucker. Curr Pharm Des. 2001;7(14):1399-1412. Drucker. Mol Endocrinol. 2003;17(2):161-171.Comparison of DPP-4 Inhibitors
Sitagliptin Alogliptin Saxagliptin Linagliptin
Usual Phase 3
25, 50, 100 mg QD 6.25, 12.5 25 mg QD 2.5, 5 mg QD 5 mg QD
Dose
Half Life (t1/2) 12.4h 12.5 to 21.1h (25mg) 2.2 to 3.8h 40 h
DPP-4 inhibition at 75% at 24 h
~80% at 24h ~78% at 24h (25 mg) 5 mg: ~55% at 24h
24h
Kidney
Kidney Liver and kidney Bile (mostly
Elimination (mostly
(mostly unchanged) Active metabolite unchanged)
unchanged)
Renal Dose
Adjustments Yes Yes Yes No
Required
>2600 fold vs >400 fold vs DPP-8
Selectivity for >10,000 fold vs DPP- >10,000 fold vs
DPP-8 >10,000 fold
DPP-4 8/9 >100 vs DPP-9 DPP-8/9
vs DPP-9
Strong CYP3A4/5 Strong CYP3A4/5
Potential for DDI Low Low
inhibitorsd inhibitorsd
Food effect No No No NoEfficacy of DPP-4 Inhibitor Therapy Added
to Metformin
Sitagliptin Saxagliptin Linagliptin Alogliptin
BL A1C (%)
≥7–≤10
7.7
≥7–≤10
8.1
≥7–≤10
≥7–≤10
≥7–≤10
8.0
7.7
7.7
8.1
—
n=273 n=743 n=701
n=701
n=743 n=743 n=527
n=701
n=743
n=273
n=273
Sitagliptin 100 mg Saxagliptin 5 mg
n=190 Rosiglitazone Saxagliptin 10 mg
Placebo Linagliptin 5 mg
Saxagliptin 2.5 mg Alogliptin 12.5–25 mg
1. Charbonnel. Diabetes Care. 2006;29:2638‐43. 2. Raz et al. Curr Med Res Opin. 2008;24:537‐50.
3. Scott et al. Diabetes Obes Metab. 2008;10:959‐69. 4. DeFronzo et al. Diabetes Care. 2009;32:1649‐55.
5. Taskinen et al. Diabetes Obes Metab. 2011;13:65‐74. 6. Nauck et al. Int J Clin Pract. 2009;63:46‐55.
14DPP-4 Inhibitors vs Sulfonylureas Added to
Metformin – 2-Year Results
ALO (25 mg)1,a LINA (5 mg)2,b SAXA (5 mg)3,c SITA (100 mg)4,d
GLIP1,3,4 GLIM2
P = .01 Noninferiority vs SU
Agent Δ Weight, kg Hypoglycemia, %
DPP-4i SU DPP-4i SU
ALO1,a −0.9e +1.0 1.4 23.2
LINA2,b −1.4e +1.3 7e 36
1.
SAXA3,c
Del Prato et al. Diabetes Obes Metab. 2014;16:1239‐46.
−1.5 +1.3 3.5 38.4
2. Gallwitz et al. Lancet. 2012;380:475‐83. SITA4,d −1.6 +0.7 5 34
3. Göke et al. Int J Clin Pract. 2013;67:307‐16.
4. Seck et al. Int J Clin Pract. 2010;64:562‐76.
5. Nauck et al. Diabetes Obes Metab. 2007;9:194‐205.GLP-1 Receptor Agonists
GLP-1 RA
His Gly Glu Gly Thr Phe Thr Ser Asp Leu
Ser
Lys
Phe Leu Arg Val Ala Glu Glu Glu Met Gln
Ile
His Ala Glu Gly Thr Phe Thr Ser Asp
Glu
Trp Leu Lys Asn Gly Gly Pro Ser Ser
Gly Exendin-4 Human GLP-1 Val
Ser
analogues Analogues[4]
Ala
Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Ser Pro Pro Pro
Glu
Phe
Ile Ala Trp Leu Val Lys Gly Arg Gly
Lixisenatide Exenatide BID Exenatide QW Liraglutide Albiglutide Dulaglutide Semaglutide*
Structural modifications confer albumin (liraglutide,
*Not approved albiglutide) or IgG Fc fraction (dulaglutide) binding
1. Christensen M, et al. Idrugs. 2009;12:503-513. 2. Ratner RE, et al. Diabet Med. 2010;27:1024-1032.
3. Stewart M, et al. ADA 2008, poster 522-p. 4. Glaesner, et al. Diabetes Metab Res Rev. 2010;26:287-296. 5. Meier JJ. Nat Rev Endocrinol. 2012;8:728-
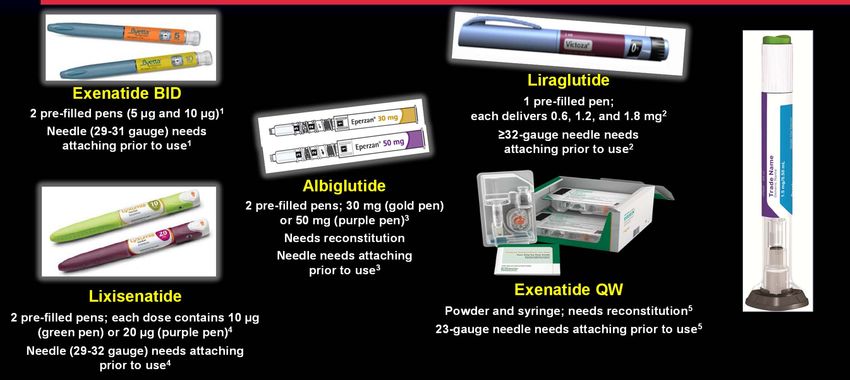
742.GLP-1 RA Administration and Devices
*
Dulaglutide
Automatic Injection
Hidden needle
*Not FDA approved
1. BYETTA Prescribing Information.
2. Victoza Summary of Product Characteristics.
3. Eperzan Summary of Product Characteristics.
4. Lyxumia Summary of Product Characteristics.
5. BYDUREON Prescribing Information.Short-Acting vs. Long-acting GLP-1 RAs:
Pharmacokinetic Differences
Category Agent Half-life Tmax
Exenatide BID1 2.4 h 2h
Short-acting GLP-1 RAs
Increasing protraction
Lixisenatide2 2.7–4.3 h 1.25–2.25 h
Liraglutide3 13 h 8–12 h
Dulaglutide4 90 h 24–48 h
Long-acting GLP-1 RAs Albiglutide5 5 days 3–5 days
Semaglutide6 ~7 days 1–1.5 days
Exenatide OW7 7–14 days 6–7 weeks
OD, once daily; Tmax, time to reach maximum concentration
1. Byetta. Summary of Product Characteristics; 2. Lyxumia. Summary of Product Characteristics; 3. Victoza. Summary of Product Characteristics;
4. Barrington et al. Diabetes Obes Metab 2011;13:434–8; 5. Eperzan. Summary of Product Characteristics; 6. Novo Nordisk data on file; 7. Fineman et al.
Clin Pharmacokinet 2011;50:65–74GLP-1RA Duration Influences FPG, PPG
and A1c
Short-acting Long-acting
FPG PPG FPG PPG
FPG, fasting plasma glucose; PPG, postprandial plasma glucose
Fineman MS et al. Diabetes Obes Metab 2012;14:675-688.Head-to-Head Trials Comparing Efficacy
of GLP-1 RAs
EXN BID 10 mcg LIRA 1.8 mg EXN QW 2.0 mg ALBI 50 mg DULA 1.5 mg
LEAD-61 DURATION-52 DURATION-63 HARMONY-74 AWARD-15 AWARD-66
b
a
a,b c
a a
Added to Added to Added to Added to Added to Added to
MET ± SU Drug-naïve Drug-naïve MET ± SU MET ± TZD MET
or or ± TZD
MET ± SU MET ± SU
± TZD ± TZD aP < .05 between groups.
b Noninferiority vs LIRA not met.
1. Buse JB, et al. Lancet. 2009;374:39-47; 2. Blevins T, et al. J Clin Endocrinol Metab. 2011;96:1301-1310; 3. Buse JB, et al. Lancet. c DULA noninferior to LIRA, P < .0001.
2013;381:117-124; 4. Pratley R, et al. Lancet Diabetes Endocrinol. 2014;2:289-297; 5. Wysham C, et al. Diabetes Care. 2014;37:2159-
2167; 6. Dungan K, et al. Lancet. 2014; 384(9951):1349-1357.GLP-1 RAs vs DPP-4 Inhibitors
Added to Metformin
ΔA1c From Baseline, %
PSGLT-2 Inhibition
Insulin-Independent Reversal of Glucotoxicity
Tubular
Proximal Lumen
Tubule
Insulin sensitivity
3Na+
in muscle1,2
ATP
2K+
SGLT-2 Insulin sensitivity
GLUT-2 in liver2
Na+/ 3Na+
Glucose
Gluconeogenesis2,3
ATP
Glucose 2K+
SGLT-1
GLUT-1 Glucose
Na+ Improved β-cell
function4,5
Glucose
GLUT-2, glucose transporter 2.
1. DeFronzo RA, et al. Diabetes Obes Metab. 2012;14(1):5-14; 2. Merovci A, et al. J Clin Invest. 2014;124(2):509-514;
3. Marsenic O. Am J Kidney Dis. 2009;53(5):875-883; 4. Ferrannini E, et al. J Clin Invest. 2014;124(2):499-508;
5. Polidori D, et al. Diabetologia. 2014;57(5):891-901.SGLT2 Inhibitors: FDA-Approved Agents
FDA-approved SGLT2 Inhibitors
Agent Administration
Canagliflozin • Oral, once daily
• Taken before the first meal of the day
Dapagliflozin • Oral, once daily
Empagliflozin • Taken in the morning with or without
foodSGLT-2 Inhibitors vs Sulfonylureas
Added to Metformin
Noninferior
ΔA1c From Baseline, %
vs SU
Δ Weight, Hypoglycemia,
kg % of patients
Agent
SGLT-2 SGLT-2
Inhibitor
SU SU
Inhibitor
CANA1,a −4.0a +0.7 5a 34
DAPA2,b −3.2a +1.4 3a 41
EMPA3,c −3.2a +1.6 2a 24
CANA (300 mg)1,b GLIP
DAPA (10 mg)2,c GLIM
EMPA (25 mg)3,d
aPOutline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practiceDiabetes and Cardiovascular Disease: The Perfect Storm Nissen SE, Wolski K. N Engl J Med 2007;356:2457-2471.
2008 FDA Guidance for Industry on Evaluating the
Cardiovascular Risk of New Antidiabetic Therapies
For completed studies prior to NDA:
● Integrated meta-analysis of phase
2/3 trials to compare CV events in
patients randomized to
investigational drug vs. control
● Demonstrate new therapy will not
result in an unacceptable CV risk
Evaluated by Major Adverse
Cardiovascular Events (MACE)
Estimated risk ratio for upper bound
of the 2-sided CI for the
investigational drug should beTraditional CV Outcome Trials vs Diabetes
CV Safety Trials
Traditional (eg, LDL-C) CV Outcome Diabetes CV Safety Trials
Trials Primarily Designed to Demonstrate CV
Designed to Demonstrate CV Benefit1,2 Safety3–5
Lower CV risk vs Placebo or Active comparator No increased CV risk vs Placebo as part of standard
care
Initiation of blinded treatment
Initiation of blinded treatment or
or placebo or active comparator
placebo
No adjustment Adjustment
to maintain to maintain
LDL-C levels HbA1c levels
the same in the same in
both groups both groups
Difference in LDL-C between treatment Small or no difference in HbA1c
and placebo or active comparator between treatment and placebo
CV benefit of treatment demonstrated No increased CV risk (CV safety) of
by significant reduction in CV outcomes treatment demonstrated by
noninferiority
CV = cardiovascular; DPP-4 = dipeptidyl peptidase-4; LDL-C = low density lipoprotein cholesterol.
1.Heart Protection Study Collaborative Group. Lancet. 2002;360:7–22. 2. Heart Protection Study Collaborative Group. Lancet. 2003;361:2005–2016. 3. White
WB et al. N Engl J Med. 2013;369:1327–1335. 4. Scirica BM et al. N Engl J Med. 2013;369:1317–1326. 5. Green JB et al. Am Heart J. 2013;166:983–989.e7.Cardiovascular Outcomes Trials in Diabetes
SUSTAIN 6 CANVAS-R VERTIS CV (NCT01986881)
(Semaglutide, GLP-1RA) (Canagliflozin, SGLT-2i) (Ertugliflozin, SGLT-2i)
n=3297; duration ~2.8 years n=5826; duration ~3 years n=8000; duration ~6.3 years
Q3 2016 - RESULTS Completion Q1 2017 Completion Q4 2019
EMPA-REG OUTCOME CANVAS DECLARE-TIMI-58
(Empagliflozin, SGLT-2i) (Canagliflozin, SGLT-2i) (Forxiga, SGLT-2i)
n=7000; duration up to 5 years Q2 2015 n=4418; duration 4+ years n=17,276; duration ~6 years
- RESULTS Completion Q1 2017 Completion Q2 2019
EXAMINE ELIXA FREEDOM REWIND CREDENCE (cardio-renal)
(Nesina, DPP4i) n=5380; (Lyxumia, GLP-1RA) (ITCA 650, GLP-1RA in DUROS) (Dulaglutide, QW GLP-1RA) (Canagliflozin, SGLT-2i)
follow-up ~1.5 years n=6000; duration ~4 years n=4000; duration ~2 years n=9622; duration ~6.5 years n=3700; duration ~5.5 years
Q3 2013 – RESULTS Q1 2015 – RESULTS Q2 2016 - COMPLETED Completion Q3 2018 Completion Q1 2020
SAVOR TIMI-53 LEADER EXSCEL HARMONY OUTCOME
(Onglyza, DPP-4i) (Victoza, GLP-1RA) (Bydureon, QW GLP-1RA) (Tanzeum, QW GLP-1RA)
n=16,492; follow-up ~2 years n=9341; duration 3.5–5 years n=14,000; duration ~7.5 years n~9400; duration ~4 years
Q2 2013 – RESULTS Q2 2016 - RESULTS Completion Q2 2018 Completion Q2 2019
TECOS DEVOTE CARMELINA CAROLINA
(Januvia, DPP-4i) (Insulin degludec, insulin) (Tradjenta, DPP-4i) (Tradjenta, DPP-4i vs. SU)
n=14,000; duration ~4–5 years n=7637; duration ~5 years n=8000; duration ~4 years n=6000; duration ~8 years
Q4 2014 - RESULTS Q3 2016 - COMPLETED Completion Q1 2018 Completion Q1 2019
2013 2014 2015 2016 2017 2018 2019 2020 2021
DPP-4i GLP-1RA SGLT-2i Insulin
Boxes with broken lines are for completed CVOTs
CVOT, cardiovascular outcomes trial; DPP-4i, dipeptidyl peptidase 4 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist; QW,
once weekly; SGLT-2i, sodium glucose co‐transporter 2 inhibitor; SU, sulphonylurea
Source: clinicaltrials.gov (October 2016)T2DM Patients in CV Outcomes Trials
● 25 Trials Ongoing/Completed
● 8 classes of medications
● >200,000 planned participants
2008
FDA guidance
Holman RR et al. Lancet 2014; 383: 2008–17.Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practicePROactive: Significant Reduction in
Secondary Outcome
All-cause mortality, nonfatal MI*, stroke
25
20
Placebo
358 events
15 16% RRR
Events HR 0.84 (0.72–0.98)
(%) P = 0.027
10
Pioglitazone
301 events
5
0
0 6 12 18 24 30 36
Time from randomization (months)
*Excluding silent MI
Dormandy JA et al. Lancet. 2005;366:1279-89.PROactive: HF Hospitalization and
Mortality
N = 5238
Pioglitazone Placebo
n (%) n (%) P
HF leading to hospital
admission* 149 (5.7) 108 (4.1) 0.007
Fatal HF 25 (0.96) 22 (0.84) NS
*Non-adjudicated
Dormandy JA et al. Lancet. 2005;366:1279-89.● 5½-year study
● 338 centers
● 23 countries in
Europe,
Australia, and
New Zealand
Home P et al. Lancet. 2009 373(9681):2125-35.Home P et al. Lancet. 2009 373(9681):2125-35.
IRIS: Pioglitazone for Stroke Prevention NEJM: Published on-line: February 17, 2016 DOI: 10.1056/NEJMoa1506930
IRIS: Trial Design
Eligibility: Recent TIA or Ischemic Stroke
Non-Diabetic
Insulin Resistant (HOMA > 3.0)
No CHF
5 years
Placebo Fatal/non-fatal MI
R Fatal/non-fatal stroke
N=3895*
Pioglitazone 5 years
15mg→45 mg
*90% power to detect a 20% RRR from 27% in the placebo group to
22% in the pioglitazone group at an alpha level of 0.05
ClinicalTrials.gov Identifier:
Viscoli CM et al. Am Heart J 2014;168:823
NCT00091949IRIS: Primary Outcome
100%
Pioglitazone
95%
Cumulative
Event-Free 9.0%*
Survival
90% Placebo
Probability
HR 0.76
85% 11.8%*
95% CI, 0.62 to 0.93
P=0.007 *cumulative event rates
80%
‐0 20 40 60
Months in Trial
Kernan WN et al. N Engl J Med, published on-line Feb 17, 2016 DOI: 10.1056/NEJMoa1506930Summary: Thiazoladinedione Cardiovascular Outcomes Trials ● No apparent increased risk of MI or MACE Some benefit apparent with pioglitazone Cannot assume that this is a class effect ● Increased risk for heart failure No increased risk for heart failure deaths ● Increased risk for fractures
Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practiceCardiovascular Outcomes Trials for DPP-4
Inhibitors
Primary Endpoint Hazard Ratio
SAVOR-TIMI 531
1.00
CVD or CRFs Saxagliptin Median CV death, (95% CI
follow-up nonfatal MI, or 0.89, 1.12)
A1c 6.5–12.0%
2.1 years nonfatal stroke p=0.99
n=16,492 Placebo
EXAMINE2
0.96
Alogliptin Median (upper boundary
ACS CV death,
follow-up of 1-sided
A1c 6.5–11.0% nonfatal MI, or repeated CI 1.16)
1.5 years nonfatal stroke
n=5,380 Placebo p=0.315
TECOS3 0.98
CV death, (95% CI 0.88, 1.09)
Median
Sitagliptin nonfatal MI, or p=0.645
CVD follow-up
nonfatal stroke, or
A1c 6.5–8.0% (superiority)
3 years UA requiring
n=14,735 hospitalization
Placebo
0.99
CV death, (95% CI 0.89, 1.10)
nonfatal MI, or p=0.84
Randomization Year 1 Year 2 Year 3 nonfatal stroke (superiority)
Median Duration of Follow-up
. Scirica BM, et a. NEJM. 2013;369:1317-1326; 2. White W, et al. NEJM. 2013;369:1327-1335; 3. Green JB, et al. NEJM, 2015Cardiovascular Outcomes Trials for DPP-4
Inhibitors
Saxagliptin Alogliptin Sitagliptin
(SAVOR-TIMI 53 Trial1) (EXAMINE Trial2) (TECOS Trial3)
N=16,492 N=5380 N=14,671
14 24
12 15 Placebo
10 18
Patients, %
Placebo Placebo
8 10 Sitagliptin
12
6 Saxagliptin Alogliptin
4 Hazard ratio: 1.00 Hazard ratio: 0.96 5 Hazard ratio: 0.98
6 (95% CI: 0.89, 1.08)
2 (95% CI: 0.89–1.12) (upper boundary of one-
P < 0.001 (noninferiority) sided repeated 95% CI: 1.16) P=0.65
0 0 0
0 180 360 540 720 900 0 6 12 18 24 30 0 4 8 12 18 24 30 36 42 48
Days Months Months
Composite of CV death, MI, or Composite of CV death, nonfatal MI, Composite of CV death, nonfatal
ischemic stroke or nonfatal stroke. MI, nonfatal stroke, or
hospitalization for unstable angina
1. Scirica, BM, et al. New Eng J Med. 2013 Oct 3;369(14):1317-26.
2. White WB, et al. N Engl J Med. 2013 Oct 3;369(14):1327-35.
3. Green JB, et al. N Engl J Med. 2015 Jul 16;373(3):232-42.SAVOR-TIMI 53, EXAMINE, and TECOS:
MACE Outcomes
Study Drug Placebo Hazard 95% p-
n/N (%) n/N (%) Ratio CI Value
SAVOR-TIMI 613/8280 609/8212 1.00 0.89, 1.12 0.99
(saxagliptin vs placebo) (7.4%) (7.4%)
EXAMINE 305/2701 316/2679 0.96 NA, 1.16 * 0.315
(alogliptin vs placebo) (11.3%) (11.8%)
TECOS 745/7332 746/7339 0.99 0.89, 1.10 0.844
(sitagliptin vs placebo) (10.2%) (10.2%)
SAVOR + EXAMINE 1663/18313 1671/18230 0.99 0.92, 1.06
+ TECOS (9.1%) (9.2%)
0 1 2
Test for heterogeneity for 3 trials: Favors Favors
p=0.877, I2=0% Treatment Placebo
*Lower Confidence Limit not given for EXAMINE trial; MACE = major adverse cardiac events.
1. Scirica BM, et al. N Engl J Med. 2013;369:1317–1326. 2. White WB, et al. N Engl J Med. 2013;369:1327–
1335. 3. Green JB, et al. N Engl J Med. 2015;373(3):232–242.SAVOR-TIMI 53, EXAMINE, and TECOS:
Hospitalization for Heart Failure
Study Drug Placebo Hazard 95%
n/N (%) n/N (%) Ratio CI p-Value
SAVOR-TIMI 289/8280 228/8212 1.27 1.07, 1.51 0.009*
(saxagliptin vs placebo) (3.5%) (2.8%)
EXAMINE 106/2701 89/2679 1.19 0.89, 1.58 0.238
(alogliptin vs placebo) (3.9%) (3.3%)
TECOS 228/7332 229/7339 1.00 0.83, 1.20 0.983
(sitagliptin vs placebo) (3.1%) (3.1%)
0 1 2
Favors Treatment Favors Placebo
*Statistically significant increase in hospitalizations for heart failure associated with saxagliptin use in SAVOR-TIMI.
1. Scirica BM, et al. N Engl J Med. 2013;369:1317–1326. 2. White WB, et al. N Engl J Med. 2013;369:1327–1335.Summary: DPP-4 Inhibitor Cardiovascular Outcomes Trials ● All trials met the primary goal of demonstrating that there is no increased risk of CVD No benefit is apparent Cannot assume that this is a class effect There may be heterogeneity with respect to heart failure ● These large trials have been useful for evaluating other potentially beneficial effects of the drugs Decreased rates of albuminuria ● More precise estimates of the risk of other rare events
Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practiceZinman B,. N Engl J Med. 2015 Nov 26;373(22):2117-28
EMPA-REG Outcomes Trial: Design
Placebo
(n=2333)
Randomised and
Screening Empagliflozin 10 mg
treated
(n=11531)
(n=7020)
(n=2345)
Key inclusion criteria: Empagliflozin 25 mg
• Adults with type 2 diabetes (n=2342)
• BMI < 45 kg/m2
• HbA1c 7-10%
• Established cardiovascular disease Median treatment
duration = 2.6 years
Key exclusion criteria:
• eGFR < 30 mg/min/1.73 m2 (MDRD)
Zinman B,. N Engl J Med. 2015 Nov 26;373(22):2117-28EMPA-REG Outcomes Trial: Main Results
20 Cumulative Incidence of the Primary Outcomea Placebo
Patients With
15 P=0.04 for superiority
Event, %
Hazard ratio, 0.86 (95.02% CI, 0.74–0.99)
10
5
Empagliflozin
0
0 6 12 18 24 30 36 42 48
9 Cumulative Incidence of Death From CV Causes Placebo
Patients With
PEMPA-REG Outcomes Trial: CV Death,
MI and Stroke
Patients with event/analysed
Empagliflozin Placebo HR (95% CI) p-value
3-point MACE 490/4687 282/2333 0.86 (0.74, 0.99)* 0.0382
CV death 172/4687 137/2333 0.62 (0.49, 0.77)EMPA-REG Outcomes Trial:
Renal Outcomes
Lower rates of acute renal failure and kidney injury (5.2%
vs 6.6% and 1.0% vs 1.6%, respectively; P < .05 vs
placebo)1
A1C reduction of –0.52% to –0.68% vs placebo in CKD
stage 2-3 (eGFR ≥ 30 to < 90 mL/min/1.73m2), P < .00012
Equivalent adverse event rates as placebo in patients in
CKD stage 2-32
1. Zinman B, et al. N Engl J Med. 2015;373:2117-2128; 2. Barnett AH, et al. Lancet Diabetes Endocrinol. 2014;2:369-384.Neal B et al. N Engl J Med. 2017 Jun 12.
Baseline Demographics and Disease
History
Neal B et al. N Engl J Med. 2017 Jun 12.CANVAS: Primary MACE Outcome Neal B et al. N Engl J Med. 2017 Jun 12.
CANVAS: MACE Components and HF Neal B et al. N Engl J Med. 2017 Jun 12. 56
CANVAS: Renal Outcomes Neal B et al. N Engl J Med. 2017 Jun 12.
CANVAS: Amputation Risk Neal B et al. N Engl J Med. 2017 Jun 12.
Summary: SGLT-2 Inhibitor Cardiovascular Outcomes Trials ● Both trials met the primary goal of demonstrating that there is no increased risk of CVD MACE benefit with both empagliflozin and canagliflozin Heart failure benefit for both empagliflozin and canagliflozin Mortality benefit with empagliflozin but not canagliflozin ● These large trials have been useful for evaluating other potentially beneficial effects of the drugs Decreased rates of albuminuria ● More precise estimates of the risk of other rare events Amputation and fracture risk with canagliflozin
Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practiceELIXA Study: Lixisenatide vs. Placebo
6,068 subjects with T2DM and recent ACS event
randomized to lixisenatide vs placebo
Trial information
Lixisenatide
Lixisenatide, 20 μg maximum dose • Multi-centre
10 μg
Placebo • Double-blind
Placebo Placebo
• Parallel-group
Run-in Titration • Event-driven
1 week 2 weeks 203±1 weeks • Randomised
Randomisation End of
(1:1) treatment
Run-in period Titration
• Patients were trained in self-administration • Lixisenatide or matching placebo (1:1)
of daily subcutaneous volume-matched • Initial dose 10 μg/day
placebo • Down- or up-titration permitted to
maximum of 20 μg/day
• Glucose control was managed by site investigators’ judgement
Bentley-Lewis R et al. AHJ 2015; 169:631-638.e7; Results of ELIXA, oral presentation 3-CT-SY28. Presented at the American Diabetes Association 75th annual scientific sessions,
Boston, 8 June 2015ELIXA Study: Primary Composite Endpoint
Time to first occurrence of the primary CV event: CV death, non-
fatal MI, non-fatal stroke or hospitalisation for unstable angina1
20
15
Patients with event (%)
HR=1.02 (0.89, 1.17)
10
5
Lixisenatide: 406/3034 = 13.4%
Placebo: 399/3034 = 13.2%
0
0 12 24 36
Months
Number at risk
Placebo 3034 2759 1566 476
Lixisenatide 3034 2785 1558 484
CV, cardiovascular; MI, myocardial infarction
1. Clinicaltrials.gov. Available at https://clinicaltrials.gov/ct2/show/NCT01147250. Accessed May 2015
Results of ELIXA, oral presentation 3-CT-SY28. Presented at the American Diabetes Association 75th annual scientific sessions, Boston, 8 June 2015ELIXA Study: Lixisenatide vs Placebo
Lixisenatide Placebo HR
Outcome n=3034 n=3034 (95% CI)
Primary outcome
(CV death, nonfatal MI, nonfatal stroke, or 13.4% 13.2% 1.02 (0.89–1.17)
hospitalization for UA)
Primary outcome plus hospitalization for HF 15% 15.5% 0.97 (0.85–1.10)
Hospitalization for HF 4.0% 4.2% 0.96 (0.75–1.23)
All-cause mortality – – 0.94 (0.78–1.13)
ELIXA = Evaluation of Lixisenatide in Acute Coronary Syndrome;
ACS = acute coronary syndrome; UA = unstable angina; HF = heart failure.
Trial data presented by Pfeffer, MA et al, ADA Scientific Sessions, June 8 2015, Boston Patients followed for a mean of 2.1 yearsLEADER: Liraglutide vs. Placebo
Cardiovascular Outcomes Trial
R N=9340 Standard of care
Key inclusion criteria Placebo* run-in A + liraglutide
N
period of ≥2 D
(0.6–1.8 mg once daily)
Adult T2D patients:
• HbA1c 7.0% weeks O
M
• Antidiabetic drug naïve; or I
3.5–5 year follow-up
Patients demonstrating S
• Treated with one or more OADs;
≥50% adherence to A
or Standard of care
regimen and willingness T
• Treated with basal or premix I + placebo*
to continue with injection
insulin (alone or in combination O
protocol for duration of
with OADs) N
trial proceeded to (1:1)
• High-risk CV profile
randomisation
*Daily single-blind subcutaneous injection of placebo
CV, cardiovascular; OAD, oral antidiabetic drug; T2D, type 2 diabetes
Marso et al. Am Heart J 2013;166:823–30.e5LEADER: Primary and Secondary
Outcomes with Liraglutide
Primary Outcomea Cardiovascular- Death From
Hazard ratio, 0.87
Related Death Any Cause
20 20 20
(95% CI, 0.78–0.97)
PLEADER: Time to First Renal Event
Macroalbuminuria, doubling of serum creatinine, ESRD, renal death
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-
hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54
months. CI: confidence interval; ESRD: end-stage renal disease; HR: hazard ratio.
Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.SUSTAIN 6: Primary and Secondary
Outcomes With Semaglutide
Marso et al. NEJM, Oct 2016Top-line Results from Exscel and Freedom-CVO
Summary: GLP-1 Receptor Agonist Cardiovascular Outcomes Trials ● All trials met the primary goal of demonstrating that there is no increased risk of CVD ● LEADER (liraglutide) and SUSTAIN 6 (semaglutide) demonstrated a benefit on MACE and mortality (liraglutide) ● ELIXA (lixisenatide), EXSCEL (exenatide) and FREEDOM (exenatide) did not demonstrate a CV benefit ● These large trials have been useful for evaluating other potentially beneficial effects of the drugs Decreased rates of albuminuria ● More precise estimates of the risk of other rare events No increased rate of pancreatitis
Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practiceDEVOTE: Trial Design
Insulin degludec once daily (blinded vial) + Follow-up
Standard of care period
7637
patients
IGlar U100 once daily (blinded vial) + Follow-up
randomized
Standard of care period
Randomization Interim analysis End of
30 days
(150 MACE accrued) treatment
(633 MACE
accrued)
Time from randomization to first occurrence of a 3-point
Primary endpoint MACE: cardiovascular death*†, non-fatal myocardial
infarction* or non-fatal stroke*
• Rate of severe hypoglycemic episodes*‡
Secondary endpoints
• Incidence of severe hypoglycemic episodes*‡
Marso S. et al. NEJM, June14, 2017Study Drugs
Insulin degludec IGlar U100
Type of New generation long-acting First generation basal insulin
insulin basal insulin analog analog
Mode of Forms soluble Precipitates as
protraction multihexamers microcrystals
Half life ~25 hours ~12 hours
Day-to-day
variability Coefficient of variation 20% Coefficient of variation 80%
(AUCGIR,0–24h)
AUCGIR, area under the curve for glucose infusion rate; IGlar U100, insulin glargine U100
Insulin glargine image data on file; Jonassen et al. Pharm Res. 2012;29:2104–14; Heise et al. Expert Opin Drug Metab Toxicol 2015;11:1193–
201; Heise et al. Diabetes Obes Metab 2012;14:859–64DEVOTE: Time to First 3-point MACE
12
356 patients
IGlar U100 Rate:
Insulin degludec 4.71/100 PYO
Patients with an event
10
325 patients
8
HR: 0.91
(%)
6 [0.78; 1.06]95% CI
Non-inferiority confirmed
4 Rate: pDEVOTE: Glycemic Control and Severe Hypoglycemia ● Glycemic control (insulin degludec vs. IGlar U100): End of treatment mean HbA1c values 7.55% vs. 7.50% Change in FPG levels -39.9 mg/dL vs. -34.9 mg/dL ● 27% fewer patients experienced severe hypoglycemia with insulin degludec ● 40% rate reduction of severe hypoglycemia ● 53% rate reduction of nocturnal severe hypoglycemia
Outline
Overview of new classes of diabetes drugs
Rationale for CVOTs in diabetes
Cardiovascular safety of new diabetes drugs:
evidence to date
Thiazolidinediones
DPP-4 Inhibitors
SGLT-2 Inhibitors
GLP-1 Receptor Agonists
Insulin
Implications of CVOTs for clinical practicePutting the Mortality Rates From EMPA-
REG and LEADER into Perspective
e
ARB +
a b c d Neprilysin f g
ARB ACE inhibitor Beta blocker MRA inhibitor Empagliflozin Liraglutide
0%
% Decrease in mortality
-10%
-20%
-30%
-40%
Study
duration 38 41 10-12 21-24 27 36 46
(months)
ACE, acetylcholinesterase; ARB, Angiotensin II Receptor Blocker; HF, heart failure; MRA, Mineralocorticoid receptor antagonist
aSOLVD Treatment; bCHARM Alternative; cCOPERNICUS and MERIT-HF; dRALES and EMPHASIS-HF, ePARADIGM, fEMPA-REG OUTCOME, gLEADER
Fitchett DH et al. Eur J Heart Fail 2016;doi: 10.1002/ejhf.633Considerations for Selecting Therapies
● Current HbA1c and magnitude of reduction needed to reach
goal
● Potential effects on body weight and BMI
● Potential for hypoglycemia – age, lack of awareness of
hypoglycemia, disordered eating habits
● Effects on CVD risk factors – blood pressure and blood
lipids
● Comorbidities – CAD, heart failure, CKD, liver dysfunction
● Patient factors – adherence to medications and lifestyle
changes, preference for oral vs injected therapy, economic
considerations
Inzucchi et al. Diabetes Care 2012; 35:1364‐79.How Do Comorbidities Affect
Anti-Hyperglycemic Therapy in T2DM?
Coronary Heart Renal Liver Hypo-
Disease Failure Disease Dysfunct glycemia
ion
Metformin: Metformin: ↑ risk of Most Emerging
CVD benefit May use hypoglycemia drugs not concerns
(UKPDS) unless Metformin & tested in regarding
Avoid condition is lactic acidosis advanced association with
hypoglycemia unstable or US: half‐dose liver increased
? SUs & severe @GFR < 45 & disease morbidity /
ischemic Avoid TZDs stop @GFR < 30 Pioglitaz mortality
precondition‐ Avoid Caution with one may Proper drug
ing saxagliptin SUs help selection is key
? Pioglitazone Empagliflozin, DPP4‐Is – dose steatosis in hypoglycemia
& CVD Canagliflozin adjust for most Insulin prone
events Avoid exenatide best DPP‐4i, GLP‐1
Liraglutide if GFR < 30 option if RA, SGLT‐2i
Empagliflozin, SGLT‐2i disease Degludec
Canagliflozin severeADA Glycemic Treatment
Recommendations for T2DM
Healthy eating, weight control, increased physical activity, diabetes education
Monotherapy Metformin
Not at target
HbA1c after ~3
months + + + + + +
Dual therapy Insulin
SU TZD DPP-4i SGLT2i GLP-1 RA
Metformin + (basal)
Not at target Metformin + Metformin + Metformin + Metformin + Metformin + Metformin +
HbA1c after ~3 SU + TZD + DPP-4i + SGLT2i + GLP-1 RA + Insulin (basal) +
months
TZD SU SU SU TZD
Triple therapy SU
DPP-4i DPP-4i TZD TZD DPP-4i
Not at target or SGLT2i or SGLT2i or or TZD or SGLT2i
HbA1c after ~3 SGLT2i DPP-4i or
GLP-1 RA GLP-1 RA Insulin GLP-1 RA
months* Insulin Insulin
Insulin Insulin
Combination
injectable Metformin + basal insulin + mealtime insulin or GLP-1 RA
therapy
DPP-4i, dipeptidyl peptidase-4 inhibitor; fxs, fractures; GI, gastrointestinal; GLP-1 RA, glucagon-like peptide-1 receptor agonist; GU, genitourinary; HbA1c, glycosylated hemoglobin; HF,
heart failure; SU, sulfonylurea; SGLT2-i, sodium-glucose co-transporter 2 inhibitor; TZD, thiazolidinedione.
American Diabetes Association. Diabetes Care 2016;39(Suppl. 1):S52-S59.ADA Glycemic Treatment Recommendations for T2DM 2017
Summary
Completed long-term CV safety trials have demonstrated no increased
risk of CV events associated with newer antihyperglycemic agents
DPP-4 inhibitors not associated with an increased overall risk
Investigation continues to identify mechanisms and/or factors that may
explain the potential for increased HF risk with some DPP-4 inhibitors
The LEADER trial (liraglutide) and SUSTAIN-6 trial (semaglutide)
demonstrated some CV benefit, whereas ELIXA (lixisenatide) EXSCEL and
FREEDOM (exenatide) did not
The EMPA-REG Outcomes Trial (empagliflozin) and CANVAS
(canagliflozin) demonstrated a CV benefit, decreased mortality
(empagliflozin) and less heart failure hospitalizations
Label recently updated to reflect this
Guidelines are evolving rapidly to reflect the new evidenceYou can also read

















































