NSW HEALTHY CHILDREN INITIATIVE - The first five years July 2011 - June 2016
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NSW HEALTHY CHILDREN INITIATIVE The first five years July 2011 – June 2016

ACKNOWLEDGEMENTS
Childhood obesity affects our whole society and it is only through
partnerships with many individuals and organisations that change
can be achieved. We gratefully acknowledge all those who have been
involved in the NSW Healthy Children Initiative (HCI) planning, delivery
and evaluation over the last five years, particularly our major partners
including the NSW Department of Education, Office of Sport, Heart
Foundation and NSW Department of Premier and Cabinet. We also
acknowledge the contribution from state-wide teams at the NSW
Ministry of Health and the NSW Office of Preventive Health to each
of the health promotion teams based in Local Health Districts. We
particularly acknowledge the work of the Program Managers who have
tirelessly driven each of the HCI programs and other investments.
We pay our respects to the traditional custodians of the lands across
NSW, to Elders past and present and to all Aboriginal people.
We gratefully acknowledge the valuable contributions that Aboriginal
Elders, organisations, community members, staff
and families have made to HCI.
NSW OFFICE OF PREVENTIVE HEALTH
Don Everett Building, Liverpool Hospital
LIVERPOOL BC NSW 1871
Tel. (02) 8738 6284
Fax. (02) 8738 6371
www.preventivehealth.net.au
This work is copyright. It may be reproduced in whole
or in part for study or training purposes subject to
the inclusion of an acknowledgement of the source. It
may not be reproduced for commercial usage or sale.
Reproduction for purposes other than those indicated
above requires written permission from the NSW
Ministry of Health.
© NSW Ministry of Health 2017
SHPN: (CPH) 170514
ISBN: 978-1-76000-725-6 (Print)
978-1-76000-726-3 (Online)
Further copies of this document can be downloaded
from the NSW Office of Preventive Health website
www.preventivehealth.net.au
Suggested citation: Innes-Hughes C, Bravo A, Buffett
K, Henderson L, Lockeridge A, Pimenta, N, Radvan D,
Rissel C (2017) NSW Healthy Children Initiative: The first
five years July 2011 – June 2016. NSW Ministry of Health.
CONTENTS
EXECUTIVE SUMMARY 4
THE HEALTHY CHILDREN INITIATIVE 7
Childhood Obesity in NSW 7
HCI Funding and Policy Context 8
Framework for HCI Action 9
Overview of Current Programs and Other Investments 10
The Innovative HCI Delivery Model 13
Implementation and Performance Monitoring 15
A Commitment to Equity 17
Ongoing Quality Improvement 19
Future Directions 20
FLAGSHIP PROGRAMS 23
Munch & Move® 23
Live Life Well @ School 26
Crunch&Sip ®
28
NSW Healthy School Canteen Strategy 30
Go4Fun® 32
Finish with the Right Stuff 34
ADDITIONAL INVESTMENTS 36
The Healthy Kids Website 36
Healthy Supported Playgroups 37
Active Travel for Children 38
yhunger 39
REFERENCES 40
The first five years July 2011 – June 2016 03
EXECUTIVE SUMMARY
The NSW Healthy Children Initiative (HCI) was established
in 2011 to provide a comprehensive, coordinated approach to
childhood obesity prevention across NSW. HCI is funded by
the NSW Ministry of Health and delivered through the NSW
Office of Preventive Health and Local Health Districts.
HCI delivers evidence-based programs across a range NSW Ministry of Health, Local Health Districts and key
of settings. The structure and delivery of the initiative service delivery partners in mutually beneficial ways.
are unique in terms of the scope, population reach,
This report reflects upon the actions and outcomes of
framework for action and focus on implementation
the first five years July 2011 – June 2016, and sets
and performance monitoring, notably in response to
directions for the future to achieve the Premier’s
equity issues. Genuinely reciprocal partnerships
Priority target of reducing childhood overweight and
across NSW and enhancement of the existing health
obesity by 5 percent by 2025.
promotion workforce draws upon the strengths of the
04 NSW Healthy Children Initiative
FLAGSHIP
PROGRAMS
HCI comprises a suite of childhood obesity prevention Munch & Move® is being
programs delivered in childrens’ settings, including Munch implemented in over 3,000
& Move, Live Life Well at School, Go4Fun, Finish With The centre-based early childhood
Right Stuff and yhunger. services across NSW (91% of all
• Over 2,000 NSW primary schools have introduced a services), 92% of which have
Crunch&Sip® strategy to schedule a daily in-class break met or exceeded the performance
for students to eat fruit or vegetables and drink water, targets related to implementing
promoting healthy living. health promotion practices.
•
The new NSW Healthy School Canteen Strategy is in
development with the NSW Department of Education
to reinforce the benefits of healthy eating and provide
healthier food and drink choices at school.
•
Finish with the Right Stuff assists junior community
sports clubs and associations to promote water as a
drink of choice and provide healthier food and drink Live Life Well @ School is being
options to children, families and spectators. implemented in over 2,000
primary schools across NSW
•
The Healthy Kids Website provides a “one stop shop” (84% of all primary schools),
of current and credible information and support 80% of which have met or
materials for teachers, parents, carers, coaches, health exceeded the performance
professionals, kids and teens. targets related to implementing
•
Healthy Supported Playgroups promotes and models health promotion practices.
healthy eating and active play through playgroups that
will reach disadvantaged children and parents, many
of whom do not access other HCI settings such as
childcare.
• ctive Travel for Children is working across the NSW
A
Government and with non-government agencies to
explore ways to increase walking, cycling, scootering,
skateboarding or any similar transport where human
energy is spent to travel, for a range of health, social Go4Fun® has delivered over
and environmental benefits. 800 programs to over 7,800
children and their families,
• yhunger, a Sydney Local Health District Program,
resulting in reduced weight,
recognises the complex challenges of food access and
improved nutrition, increased
physical activity options for young people aged 12-24
physical activity and additional
years of age who are experiencing or are at risk of
benefits including improved
homelessness, and works with youth workers and
fitness and self-esteem.
services to reach and support this important
marginalised population.
The first five years July 2011 – June 2016 05
06 NSW Healthy Children Initiative

THE HEALTHY
CHILDREN INITIATIVE
Childhood Obesity in NSW
The World Health Organization Intervention during childhood • Facilitate preventive health
describes childhood obesity therefore has the potential for research and knowledge
prevention as one of the most both short-and long-term benefits. translation into policy and
urgent public health priorities for There is growing evidence for the practice
this century1. The prevalence of potential of childhood obesity
• Support the NSW Local Heath
overweight and obesity in NSW prevention9, 10 including strategies
District (LHD) health promotion
children aged 5 to 16 years was delivered in settings such as early
workforce to deliver key state-
22% in 20152. This is a cause for childhood services11, 12 and schools13, 14.
wide preventive health
concern, and the Premier has To be effective and sustainable, it
programs
accordingly identified it as a top is important that comprehensive
priority for the NSW Government3, 4. childhood obesity prevention takes • Provide high level evidence-
This cross-government a population-wide approach, based advice to the NSW
commitment is described in the includes community-based Ministry of Health on matters
NSW Healthy Eating and Active interventions, and has strong relating to delivery of
Living Strategy5 that drives major leadership, policies, dedicated preventive health programs
health promotion investments funding, monitoring and and strategies.
across NSW. infrastructure in place to support
health promotion action1. The The NSW Healthy Children
Childhood obesity is associated establishment of the NSW Office Initiative (HCI) was established
with compromised health6 and of Preventive Health (OPH) in July in July 2011 to provide a
significant reductions in quality of 2012 provided the ideal mechanism comprehensive, coordinated
life7, 8 . Children above a healthy for this to be enabled in NSW, with approach to childhood obesity
weight may develop health stated OPH objectives being to15: prevention across NSW. HCI is
problems in childhood, such as funded by the NSW Ministry of
asthma, sleep problems, hip, knee • Manage the planning, Health and delivered through the
and ankle problems, and high implementation, support and OPH and LHDs.
cholesterol or blood pressure. evaluation of priority state-wide
Children who are above a healthy preventive health programs
weight are also much more likely
• Report on outcomes of NSW
to become overweight adults
priority-funded preventive
putting them at risk of health
health programs, including
problems like heart disease,
economic analyses
diabetes and cancer1, 9.
The first five years July 2011 – June 2016 07
HCI Funding and Policy Context
Although numerous childhood obesity prevention NSW Government Priority
programs and projects were being delivered in NSW
prior to the establishment of HCI, they were not of the In late 2015 the NSW Premier committed to 12 key
scope, scale nor coordinated intent that is described personal priorities to make NSW a better place to
herein. Initial funding through the Council of work and live, including reducing the prevalence of
Australian Governments (COAG) National Partnership childhood overweight and obesity by 5% in 10 years,
Agreement on Preventive Health made HCI possible16. which would result in 62,000 more children who are
All jurisdictions in Australia received this funding a healthy weight in NSW3.
stream for childhood obesity prevention to “help HCI is an important strategic component of this
assure Australian children of a healthy start to life” Premier’s Priority, providing coordinated state-wide
(p5) with particular focus on: leadership of childhood obesity prevention programs.
• Building on existing efforts, while adapting them to HCI is complemented by more than 50 cross
suit demographic and other factors in play at government actions, including3:
various sites • Enhancing the Make Healthy Normal social
• Covering physical activity, healthy eating, and marketing campaign with new messages for
primary and secondary prevention families
• In settings such as child care centres, pre-schools, • Supporting GPs and health professionals to identify
schools, multi-disciplinary service sites, and children above a healthy weight and refer them to
children and family centres appropriate programs
• Including family based interventions, settings • Supporting the NSW menu labelling initiative to
based initiatives, environmental strategies in and help people make lower-kilojoule choices when
around schools, and breastfeeding support eating out
interventions. • Creating guidelines for the planning, design and
When that funding stream ended in July 2014, development of healthy built environments.
programs in other jurisdictions were concluded or
scaled back. However the HCI infrastructure in NSW
was sufficiently robust to remain in place as the
central focus of childhood obesity prevention in NSW.
HCI continues to deliver key programs under the
cross-government NSW Healthy Eating and Active
Living Strategy5. Specifically, HCI provides access to
state-wide healthy eating and active living programs
(Strategic Direction 2). The key settings for
implementing these programs include early childhood
education and care services, schools, junior
community sport and the community more broadly.
“We’re determined
to protect children from
the poor health and
wellbeing outcomes
associated with
being overweight
or obese.”
(Former) NSW Premier Mike Baird3
08 NSW Healthy Children Initiative
Framework for HCI Action
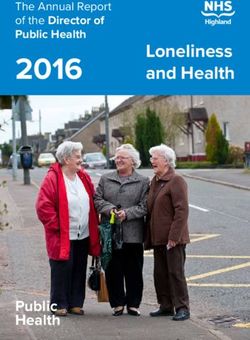
Figure 1: HCI Framework for Action
, population-lev
e - wide el p
tat rog
d s ra
te d
m
n a ona n Comm de
d i n tati
n itorin g i tme l
r e
m em
o ntt
o
iv
e
p l an c
o
eq
er
Co
Im rm ui
ty
y
fo
er
p
el
od
qu
ry M
alit
Ong rovement
y im
Innovative Delive
oing
p
Improving the
Supporting environments
children and in which they
families live, learn
and play
H
E VE
T
HE TI
AL TI A
T HY
N I NI
CHILDRE
The Primary Teenagers
early years school age and youth
0-5 years 5-12 years 13-18 years
A comprehensive framework for HCI action is
represented in Figure 1. This recognises that:
•
The scope of action is broad, focussing not just •
The approach is coordinated and strategic. This
on children and families but also the settings in includes an innovative delivery model that builds
which they spend time, to create supportive strong reciprocal partnerships between the OPH
environments and a culture that is more conducive and LHDs, implementation and performance
to healthy eating and active living. monitoring for both insight and accountability,
a strong commitment to equity and ongoing
• HCI programs and other investments are tailored
investments in innovation and research (see
to context and needs across a range of ages
more from page 13).
and stages, including the early years (0-5 years),
primary school age (5-12 years) and teenagers • This framework for action collectively provides
and youth (13-18 years). an opportunity for coordinated state-wide,
population-level program delivery.
The first five years July 2011 – June 2016 09
Overview of Current Programs
and Other Investments
HCI was initially built upon a number of existing and the following tables provide a snapshot summary
programs which were scaled-up for delivery across of each. “Flagship programs” are highlighted as those
NSW. It continues to evolve through further innovation with greatest population reach and a substantial focus
and research. Figure 2 provides an overview of current and resource allocation.
HCI programs and other investments by age and stage,
Figure 2: HCI programs and other investments by age and stage
Age 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
The early years Primary school age Teenagers and youth
0-5 years 5-12 years 13-18 years
FLAGSHIP PROGRAMS
NSW Healthy School Canteen Strategy
investments
Additional
Healthy supported
playgroups
Active Travel for Children
010 NSW Healthy Children InitiativeTable 1: Snapshot of current flagship programs
PROGRAM TARGET GROUP SETTING BRIEF DESCRIPTION
Encourages healthy eating,
Children aged 0-5 years, increased physical activity and
Early childhood
parents/carers, early reduced small screen recreation
education and
childhood educators in children attending early
care services
and staff childhood education and care
services.
Enhances teacher’s knowledge
and skills in teaching nutrition
Children aged 5-12
and movement. Supports schools
years, parents/carers, Primary schools
to create environments which
teachers, principals
enable children to eat healthily
and be physically active.
Encourages primary schools to
schedule a daily in-class break
Children aged 5-12
for students to eat fruit or
years, parents/carers, Primary schools
vegetables and drink water, in
teachers, principals
addition to their usual recess and
lunch breaks.
Encourages all primary and
Children aged 5-18
secondary schools to provide
NSW Healthy School years, parents/carers, Primary and
a healthy and nutritious food
Canteen Strategy canteen staff and secondary schools
service that is consistent with
volunteers, principals
the Australian Dietary Guidelines.
Helps children above a healthy
weight and their parent/
carer(s) to modify family
lifestyles, improve nutrition
and activity levels, promote
Children aged 7-13 years, weight management and
Community
parents/carers increase wellbeing and self-
esteem. Delivered by trained and
qualified health professionals,
with prioritisation for delivery
within disadvantaged
communities.
Encourages junior sporting clubs
Children aged 5-16 and associations to provide
years, parents/carers, Sporting clubs and promote healthier food at
sporting clubs and and associations club canteens and encourages
associations children to drink water before,
during and after the game.
The first five years July 2011 – June 2016 011Table 2: Snapshot of additional HCI investments
PROGRAM TARGET GROUP SETTING BRIEF DESCRIPTION
This website provides a “one
Children and young
stop shop” of current and
people, parents/carers,
Online credible information and
HCI project partners,
resources about healthy eating
communities
and physical activity.
Provides recommendations
and online information to
create environments and
Children aged 0-5
Healthy supported Supported deliver consistent, appropriate
playgroups years, parents/carers,
playgroups messages and learning
playgroup facilitators
experiences that support healthy
eating, active play and oral
health to parents/carers.
Provides an overarching
School aged children, strategy on active travel for
Active Travel
parents/carers, partner Community children, in collaboration with
for Children
organisations key government and non-
government agencies.
Helps disadvantaged youths
to develop healthy eating
and physical activity skills
Young people 12-
by training youth workers to
24 years who are
Youth workers provide healthy, nutritious
experiencing or at risk
and services food and encourage regular
of homelessness. Youth
physical activity. Delivered
a workers and services
through specialist youth health
and homelessness services and
alternate education providers.
a
yhunger is a Sydney LHD-funded program with HCI contribution towards resource development and evaluation.
012 NSW Healthy Children InitiativeThe Innovative HCI Delivery Model
One of the greatest challenges in health promotion is LHDs implement HCI programs through dedicated,
the concept of scalability – increasing the scale and funded positions. Resourcing these local positions is a
adoption of health promotion interventions to achieve central component of the delivery model, to ensure
state-wide, population-level program delivery and capacity for local intervention delivery. LHD teams
outcomes17, 18 . The innovative delivery model of HCI is also have the best understanding of their local
central to achieving effective program delivery at communities and project partners, and can adapt the
scale, notably across our flagship programs. flagship interventions accordingly, while maintaining
fidelity, hence value-adding locally. Each LHD has
Traditional, top-down models are often characterised
worked for many years to establish the vital local
by state-level determination of broad priorities for
partnerships that are essential to practice, and build
action, with funding provided to local areas for action
their capacity to promote and support healthy
within the agreed scope. Another common delivery
lifestyles, particularly in relation to equity investments
approach is central coordination, often through non-
such as working with Aboriginal organisations and
government organisations without an on-the-ground
communities. The implementation experiences of
workforce. There is often little further coordination or
LHDs are shared between one another and fed back
collaboration. In contrast, HCI has seen the
to inform the central coordination of HCI, completing
establishment of genuinely reciprocal partnerships
the ongoing quality cycle in a truly collaborative
across NSW with enhancement of the existing health
manner.
promotion workforce. This draws upon the strengths
of each group in mutually beneficial ways. The HCI delivery model can therefore deliver much
more than the sum of its parts. Each group builds the
OPH is well-placed to conduct centralised planning
capacity of the others. This has particular benefits for
and coordination. OPH can negotiate within the health
rural and remote LHDs who might otherwise be
system and build partnerships with other
working in relative isolation with minimal resources.
organisations at the state level to facilitate HCI
funding, design, delivery, research and evaluation. This model builds a critical mass that benefits all.
OPH investments in centralised or commissioned Long-term funding enables OPH and LHDs alike to
research and intervention development can be shared recruit personnel, and develop and sustain the state-
state-wide, avoiding duplication and improving wide health promotion workforce as a whole. This
evidence-based practice. Similarly, OPH can support includes recruiting to identified positions such as the
LHDs by funding a pilot study or evaluation of a Aboriginal Leaders who deliver programs such as
locally-developed intervention, building the potential Go4Fun® for Aboriginal families.
for wider adoption across the state. The resulting
improved impact of programs which are delivered
state-wide is also desirable when working with other
state-wide organisations such as the Department of
Education. Finally, centralised implementation
monitoring provides information which is used to
inform program review and quality improvements.
The efficiencies of centralised systems also maximise
the resources that can be directed into local
intervention delivery.
The first five years July 2011 – June 2016 013Examples of the state-wide, population-level reach and impacts achieved across NSW,
July 2011 to June 2016, through the innovative HCI delivery model include the following.
MUNCH & MOVE®
3,231 (91%) of centre-based early
childhood services across NSW participate
LHD performance target = 70% of
participating services achieving in the Munch & Move® program.
≥70% of practices
This performance target
has been exceeded, 95% include 96% include 97% have a
rising from 36% in 2012 active play time fruit and written policy
to 92% in 2016. vegetables daily on nutrition
LIVE LIFE WELL @ SCHOOL
2,050 (84%) of primary schools across NSW
participate in the Live Life Well @ School program.
LHD performance target = 70% of
participating services achieving
≥70% of practices
This performance target 92% encourage 89% have a 81% provide
has been exceeded, students to be fruit, vegetable nutrition and
physically active and water physical activity
rising from 32% in 2012 during recess break information
to 80% in 2016. and lunch to families
GO4FUN® On average, participating children have achieved:
7,821
overweight
and obese
children and
their families
Reduced Improved Increased Additional
have weight: nutrition: physical benefits:
participated BMI reduced Statistically activity: Improved
in 807 by 0.5kg/m2 significant Increase by fitness and
increases in 3.6 hours self-esteem
Go4Fun®
both fruit and per week
groups vegetable intake
014 NSW Healthy Children InitiativeImplementation and
Performance Monitoring
The scale of the investment in HCI demands that An information management system was
comprehensive and systematic monitoring be commissioned to report data in real time by LHD staff
undertaken. This is in line with World Health and is used by the Ministry of Health to report HCI
Organization recommendations that highlight the data for performance monitoring and by OPH for
importance of information and accountability1. program monitoring. Known as the Population Health
Intervention Management System (PHIMS), this
There are two distinct elements of this in HCI: system comprises multiple components including
• implementation monitoring by OPH to inform software to enable data entry, analysis and reporting,
HCI delivery; and and a tailored user interface for LHDs, the Ministry of
Health and OPH. PHIMS was developed as a flexible,
• quality improvement, and performance monitoring scalable and sustainable information technology
by the NSW Ministry of Health as part of Service solution, with due consideration of issues such as
Level Agreements between the Ministry and access and confidentiality. The system has 150 users
individual LHDs. who account for the monitoring and reporting of over
6,500 intervention sites.
IMPLEMENTATION MONITORING
Data on the practices are obtained by health
Effective scaling up requires the systematic use promotion officers in each LHD as a result of their
of evidence, and it is essential that data from direct contact with the service or school and are
implementation monitoring are linked to decision- entered into PHIMS. Data are reported quarterly and
making throughout the scaling up process18 . To that used to inform quality improvements in the programs.
end, a framework was developed to guide the
monitoring, evaluation and quality review of Munch In addition to the PHIMS data describing Munch
& Move® and Live Life Well @ School, both of which & Move® and Live Life Well @ School, Go4Fun®
would be implemented at a large scale19. implementation data are also routinely gathered and
monitored. These data are entered into a service
Program adoption indicators known as practices are provider data system, Better Health Data, and
a key feature of this monitoring approach. These analysed and reported as part of a contractual service
program-specific practices relate to organisational provision. Data describing the number of families
changes in early childhood services and primary registering, enrolling and completing the Go4Fun®
schools which reflect program adoption to a high program are reported by LHD and at state level.
standard. Practices relate to healthy eating, physical Aggregated participant outcome data are also
activity and sedentary behaviours (see full lists later in reported and include changes in self-esteem, BMI,
this document). Each practice was developed, piloted consumption of both healthy and unhealthy indicator
and subsequently analysed for sensitivity, then clearly foods and time spent in physical activity and
defined in a Monitoring Guide to ensure consistent sedentary behaviours.
determination of achievement across NSW.
The first five years July 2011 – June 2016 015PERFORMANCE MONITORING
Performance monitoring relates to procedures As the programs have become established over time
between the NSW Ministry of Health and individual and their achievements have grown, the KPIs too
LHDs. The data used for performance monitoring are have increased to reflect this, and to drive ongoing
extracted from the PHIMS and Go4Fun® data sources performance improvement. Having achieved good
described above. program participation or reach, the focus of KPI
increases has been on program adoption through
Key performance indicators (KPIs) and measures
achievement of program practices. The targets for
were developed to describe program reach and
June 2016 were as follows:
adoption for Munch & Move® and Live Life Well @
School. KPIs for Go4Fun® relate to enrolments against
a defined target and completion rates.
• Munch & Move®: 80% of all centre-based
KPIs are reported at both the state and LHD level.
services participate in the program and
Annual LHD targets were established for KPIs. Annual 70% of services achieve 80% of the
incremental targets were set to achieve progress program practices.
towards the June 2015 targets as follows:
• Munch & Move®: 80% of all centre-based • Live Life Well @ School: 80% of all
services participate in the program and primary schools participate in the
60% of services achieve 70% of the program and 70% of schools achieve 80%
program practices. of the program practices.
• Live Life Well @ School: 80% of all • Go4Fun ®: an additional 1,694 children
primary schools participate in the enrolled across NSW from July 2015 to
program and 60% of these schools June 2016 with 85% of them completing
achieve 70% of the program practices. the program.
Key performance indicators were embedded in the
• Go4Fun ®: 7,000 children enrolled in the in the annual Service Level Agreements between
program across NSW with 85% of them the NSW Ministry of Health and LHDs20. These
completing the program. Service Agreements comprise the performance and
service delivery requirements of LHDs19. As part of
the NSW performance framework, Chief Executives
of each LHD are required to participate in quarterly
performance reviews against the annual service
agreement. Incorporating HCI KPIs in this process
enables state and local level monitoring of HCI
program implementation, facilitates LHD
accountability, and provides feedback to inform
local HCI program delivery planning. It also
encourages ongoing investment in child obesity
prevention at the state level.
There is always some risk that a systematic and
centrally directed approach to implementation and
performance monitoring may act as a barrier to local
innovation, and even compromise program fidelity19.
However, within the context of HCI, whilst the
outcomes and targets are centrally directed, LHD
implementation to achieve these targets remains
locally determined. A balance is therefore achieved
between local innovation and central management.
016 NSW Healthy Children InitiativeA Commitment to Equity
An important function of implementation monitoring
THE HCI
is to ensure equitable access and participation and
equitable outcomes. These are critical considerations
PRIORITY
for the fair, universal delivery of HCI programs and
other investments across NSW. Certain groups in our GROUPS ARE:
communities experience poorer health than the rest of
the NSW population21, 22. The NSW State Health Plan:
Towards 2021 calls upon health services and programs
to make sure that health gains are shared by everyone
and across every community in NSW21.
HCI recognises that the following equity principles are
important to achieve this23:
• Identify barriers that prevent or limit children from
Children
priority groups from participating in HCI programs
living in low
• When necessary, tailor programs to meet the socioeconomic
needs of priority groups population
groups
• Promote the sustainability of equity principles by
building them into the policies and programs
• Monitor and evaluate programs in terms of their
accessibility to and impacts upon priority groups. Aboriginal &
Torres Strait
The need for more coherent planning is also Islander
emphasised, as is the importance of strengthening the children
infrastructure underpinning program delivery, and the
need to increase partnerships between health and
other government-delivered services. State-wide
stakeholder consultation also determined a need for Children from
something more concrete and practical tools to guide culturally and
program activity. As a result, The HCI Equity Toolkit23 linguistically
was developed through a Delphi consensus process. diverse (CALD)
The toolkit identifies and describes practical actions backgrounds
across three “other platforms for action” relating to
community needs assessment, identifying
opportunities for collaborative action and prioritising
equity and sustainability across all programs. Highly
marginalised
The toolkit has subsequently been enhanced by more children and
specific tools and resources such as a checklist for youth
considering and incorporating the priorities and needs
of culturally and linguistically diverse communities
when implementing HCI programs and other
investments.
In practice, this commitment to equity is evidenced Children from
throughout the ongoing cycle of planning, remote NSW
development, implementation and evaluation –
notably a strong focus on equity in the performance
monitoring of HCI programs and other investments,
to ensure HCI does not widen the health differential
by ensuring that it has broad reach including those
who need it the most (see next page). Children from
single parent
families
The first five years July 2011 – June 2016 017Reach and Adoption of HCI Programs
Implementation monitoring tracks the reach and adoption of HCI programs in vulnerable populations, as well as
state-wide, to ensure that equity goals are being met.
MUNCH & MOVE®
% that participate % that have achieved the
Focus population/setting
in Munch & Move® practice adoption targets
Early childhood services in areas of
94% 90%
socioeconomic disadvantagea
Early childhood services with high
96% 88%
proportions of Aboriginal childrenb
Early childhood services in outer regional
75% 70%
and remote/very remote locations
ALL EARLY CHILDHOOD SERVICES ACROSS NSW 91% 92%
LIVE LIFE WELL @ SCHOOL
% that participate in % that have achieved the
Focus population/setting
Life Live Well @ School practice adoption targets
Primary schools in areas of socioeconomic
86% 79%
disadvantagea
Primary schools with high proportions
90% 79%
of Aboriginal studentsb
Primary schools in outer regional and
77% 77%
remote/very remote locations
ALL PRIMARY SCHOOLS ACROSS NSW 84% 80%
GO4FUN®
25% of participants 54% of 9% of participating 30% of participants
to date identify as participating families identify as have come from outer
being from a sole mothers hold a being Aboriginal or regional or remote/
parent family health care card Torres Strait Islander very remote localities
a
Defined as being in SEIFA quintiles 1 and 2 b
Defined as being above 10% (greater than population prevalence)
018 NSW Healthy Children InitiativeOngoing Quality Improvement
The scale and longevity of HCI provides a context in
Go4Fun® Quality
which quality improvement can be achieved through
Improvement Case Study
sound, long-term practices and targeted quality
investments. Targeted investments in innovation and
evaluation build stronger HCI programs.
Evidence-based practice is the cornerstone of health
For example, since Go4Fun® was launched
promotion, and HCI is built upon a foundation of
in 2009, there have been ongoing
quality health promotion practice, and is shaped by
investments to evaluate and improve the
policy and research. For example, health promotion in
program. The original program model was
schools was the focus of the work of many health
supported by evidence for efficacy related
promotion professionals across NSW for many years
to weight and psychosocial outcomes25, 26,
prior to the establishment of OPH and HCI24. Building
acceptability to parents25, positive long
upon that evidence and experience of the past and
term outcomes27 and participation by those
the wisdom of current practitioners and partners are
from disadvantaged and ethnic minority
key to effective health promotion delivery.
backgrounds28 .
Ongoing reciprocal communication between OPH
That model included twice-per-week two-
and LHDs occurs through routine contact such as
hour sessions over 10 weeks. Despite
quarterly networking meetings, as well as purpose-run
relatively successful implementation, a
forums. Informal consultation and feedback is
program review in 2012 found that the
continuous. The implementation experiences of LHDs
twice-per-week attendance requirement
are shared between one another and fed back to
was a barrier to participation for some
inform the central coordination of HCI, completing the
families. A program of reduced duration
ongoing quality cycle in a truly collaborative manner.
could potentially remove this barrier, as
For example, feedback regarding the Live Life Well @
well as costing less to deliver. But would
School program shaped the delivery of professional
it still achieve the same results?
development for primary school staff.
OPH undertook a cluster-randomised
Implementation monitoring provides valuable insight
controlled trial between July 2013 and
and intelligence to guide HCI delivery, particularly in
March 2014 to compare the effectiveness
terms of reach. This considers not only the scale of
of a revised, once-per-week program
that reach but also whether individuals and
delivery model with the original twice-per-
communities who experience disadvantage and
week model29. Evaluating outcomes at
inequities in health and wellbeing are accessing and
program completion and six-month follow-
participating in HCI programs and other investments.
up, the study concluded that Go4Fun®
can be delivered once-per-week with no
compromise to health or behavioural
outcomes. The standard mode of delivery
has been once-per-week across NSW since
October 2014.
Through this ongoing program
improvement process, feasibility has been
improved and cost efficiency achieved with
no compromises to program outcomes,
and significant contributions made to the
evidence base29, 30.
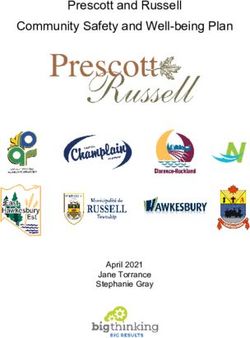
The first five years July 2011 – June 2016 019Future Directions
There are indications that the prevalence of childhood The NSW government Premier’s Priority to reduce
obesity in NSW has stabilised and may be declining. obesity prevalence by 5% by 2025 has provided an
The prevalence of overweight and obesity in children opportunity and an imperative to strengthen the
has been relatively stable in NSW since 2007, with the childhood obesity prevention effort. This will require
2015 prevalence at 22% of 5-16-year-old children a strong effort across childhood obesity prevention
(Figure 3). The 2015 NSW School Physical Activity programs through HCI, food and physical activity
and Nutrition Survey (SPANS) reports objectively environments, the built environment, social marketing
measured height and weight in children from and clinical engagement to identify and manage
Kindergarten to Year 12 and trends over time. SPANS obesity5.
2015 suggests that obesity prevalence has decreased
at entry into school (Kindergarten) and Year 6, while
prevalence remains high in the adolescent years of
secondary school, (Years 8, 10 and 12).
The high reach of HCI programs targeting early
childhood settings and primary schools is likely to
be a contributing factor to these apparent changes,
but the issue remains a high priority for government
action.
Figure 3: Overweight and obesity in children aged 5-16 years, NSW 2007-2015
30
Target 2025
25 16.5%
PERCENT
20
15
10
5
0 07 09 11 13 15 17 19 21 23 25
YEARS
NSW Childhood Obesity Prevalence
020 NSW Healthy Children InitiativeTo move HCI into the future to achieve these targets, •
Focus on building sustainability, through strategies
OPH will: including but not limited to:
•
Maintain the high population reach of flagship HCI - Increasing the relevance and thereby
programs by continuing to deliver flagship acceptability, sustainability and system-wide
programs at scale, notably: reach of HCI strategies, such as ensuring that
training delivered to early childhood educators
- Munch & Move® in early childhood settings
and primary school teachers is accredited.
- Live Life Well @ School in primary school
• Identify opportunities to build evidence to direct
settings.
future investments, such as:
•
Scale up programs where appropriate to improve
- Interventions for parents of children aged 0-2
reach and impact.
years and 2-6 years
- With a major new investment to be provided
- Interventions for adolescents both in the school
through the NSW Premier’s Priority, Finish with
setting and in the community.
the Right Stuff will be implemented in 300 clubs
over the next two years. • argeted delivery to improve reach and impact
T
on vulnerable groups, such as:
• Increase the impact of HCI programs through
strategies including but not limited to: -D
elivering Go4Fun® to the most vulnerable
groups within an LHD and the state-wide
- Increasing the support for less well achieved
development of adapted programs such as
practices (such as teaching fundamental
Go4Fun® for Aboriginal Families, which was
movement skills in early childhood services
piloted in 2015.
and primary schools)
•
Complement the HCI settings based approach
- Exploring more effective implementation
with more direct communication to families,
processes (such as training methods) to achieve
parents and carers through social marketing and
greater reach and sustainability.
development of programs or services which target
• everage off existing policy imperatives and
L this audience directly.
monitoring systems, such as:
- Improving healthy food access and availability in
school canteens and linking this to Department of
Education monitoring systems
- Supporting Department of Education to roll out
and monitor the canteen strategy
- Supporting early childhood services to meet their
requirements under the National Quality
Framework.
• Invest in ongoing quality improvements in each
HCI program to ensure programs are delivered
with fidelity, remain contemporary and are
relevant for the target groups.
- The Best Practice Framework that is routinely
implemented for Go4Fun® incorporates
professional reflection and continuing
professional development as well as providing a
quality check and feedback loop to program
improvement.
evelop a quality framework for Munch & Move®
-D
and Live Life Well @ School.
The first five years July 2011 – June 2016 021022 NSW Healthy Children Initiative
FLAGSHIP PROGRAMS
Munch & Move®
Centre-based early childhood participating in active play have
services including preschool and been associated with higher levels
The Munch & Move®
long day care services are of physical activity in preschools39.
program aims to influence
important settings for childhood Healthy eating and physical
the healthy eating and
obesity prevention11, 12, 31, 32. It has activity strategies have been able
physical activity
been recommended that this to be sustained beyond one year
behaviours of young
should target dietary intake of intervention40.
children from birth to five
and activity behaviours
years who attend NSW Munch & Move® provides state-
simultaneously33 and policies be
early childhood education wide professional development
strengthened to create a healthy
and care services. The training by an early childhood
early childhood environment34.
program offers professional registered training organisation
development and support Evidence shows that educational and support by LHDs. The
across six key health workshops and training for child program also offers:
promoting messages: care providers on nutrition,
• An online refresher module
physical activity and screen-time
• Encouraging and to further reinforce knowledge
behaviours and regulations have
supporting and skills
increased provider knowledge,
breastfeeding
improved centre policies and • Practical resources to support
• Choosing water as a reduced body mass index for policy and practice
drink children in child care centres in the development and
United States35, 36. Within Australia, implementation
• Choosing healthier
preschool-based obesity
snacks • Fact sheets to communicate
prevention interventions have
produced significant changes in with families
• Eating more fruit
and vegetables children’s food intake, movement • Ongoing implementation
skills and indicators of weight support from LHDs.
• Getting active every day status37, reduced the prevalence of
overweight and obesity in early The program is strongly aligned to
• Turning off the
childhood settings38 and improved the National Quality Framework
television or computer
children’s food intake at and it can help services meet the
and getting active.
preschool39. Written physical requirements of the National
activity policy, structured staff-led Quality Standard and the Early
physical activity and staff Years Learning Framework.
The first five years July 2011 – June 2016 023A set of 15 program adoption indicators (also
known as practices) has been developed: There has been a steady growth in the
number and type of early childhood
services participating in Munch & Move®
Service monitors food and drinks since it began as a pilot in 2008.
Practice 1 that are in children’s lunchboxes
every day
Practice 2
Service menu includes fruit and
vegetables at least once per day 91%
Service menu includes only of centre-based early
Practice 3 childhood services
healthy snack options every day
across NSW now
Service supplies age appropriate participate in Munch &
Practice 4
drinks every day Move® (3,231 services)
Service provides structured and
specific learning experiences
Practice 5
about healthy eating at least 2 213,800 children in NSW attend
times per week an early childhood service41.
Nearly 195,000 children attend
Service provides tummy time for a participating service.
Practice 6 babies 0-12 months of age every
day
Service provides physical activity There has been a significant increase in
Practice 7 for 1-5 year olds at least 25% of the number that have implemented 70%
the daily opening hours or more of the Munch & Move® practices:
Service provides fundamental
Practice 8
movement skills for children 3-5
years of age every day, to at least 36% 92%
90% of children in 2012 in 2016
Service use of small screen
Practice 9 recreation by 3-5 year olds is This increase in program adoption has
appropriate been seen across all early childhood
services (preschool, long day care and
Service has a written nutrition occasional care services) and notably
Practice 10
policy by early childhood services that are
Service has a written physical characterised by priority population
Practice 11 groups (high proportion of Aboriginal
activity policy
children attending, services in
Service has a written policy disadvantaged communities and
Practice 12 restricting small screen services in remote communities).
recreation
The strongest increases in individual
Service provided health
practice improvement have related to:
Practice 13 information to families within
past 12 months •
Water or age-appropriate drinks
(Practice 4)
Service has at least 50% of
primary contact educators • ealthy eating learning experiences
H
Practice 14 at least twice per week (Practice 5)
trained in nutrition and at least
50% trained in physical activity • undamental movement skills ages
F
Service monitors and reports 3-5 years (Practice 8)
achievements of healthy eating •
Written physical activity policy
Practice 15
and physical activity objectives (Practice 11)
annually
•
Provision of health information to
families annually (Practice 13)
024 NSW Healthy Children InitiativeThe first five years July 2011 – June 2016 025
Live Life Well @ School
Primary school aged children NSW. It is built on the outcomes
spend a large proportion of their and learning of previous state-wide
Live Life Well @ School is
day at school, which has an programs and was developed in
delivered through a
important role in their lives line with relevant obesity
partnership between NSW
providing a safe and supportive prevention guidelines48, 49 and
Health, the NSW
environment for learning about Department of Education policies50.
Department of Education,
and reinforcing healthy eating and
Catholic and Independent The program offers professional
physical activity behaviours during
school sectors. It is learning for teachers to improve
the formative years13, 42, 43. Research
delivered in NSW primary skills and confidence in teaching
suggests that interventions using a
schools to promote healthy nutrition, fundamental movement
combination of nutrition and
eating and physical activity skills and physical education. LHDs
physical activity interventions are
to students and their provide additional support for
effective in achieving weight
families. program implementation at the
reduction in school settings13, 14,
school via school visits, phone
The program aims to 44-46
. There is convincing evidence
calls and email follow ups to assist
enhance teachers’ that long-running school-based
schools to develop an Action Plan
knowledge, skills and interventions are effective in the
that reflects a whole of school
confidence in teaching short-term in reducing the
approach to nutrition and physical
nutrition and physical prevalence of childhood obesity47
activity, assist in the development
activity as part of the and supporting the beneficial
of school community focused
school curriculum. The effects of child obesity prevention
nutrition and physical activity
program has a “whole of programs on body mass index,
strategies, and provide access to
school” approach particularly those aimed at primary
information and resources that
consistent with classroom school aged children10.
support the teaching and creation
teaching and school
Live Life Well @ School was first of a school environment that
policies, and encourages
implemented in Government promotes physical activity and
links with parents, carers
schools in 2008, and was healthy eating. LHDs also target
and communities.
expanded in 2012 to include schools that have relatively high
Catholic and Independent schools. numbers of Aboriginal and Torres
The program provides a Strait Islander students, schools
framework to consolidate pre- located in disadvantaged
existing nutrition and physical communities and schools that
activity programs, resources and are geographically remote.
strategies being offered across
026 NSW Healthy Children Initiative84%
of primary schools
Like Munch & Move®, Live Life Well @ School across NSW now
established and promotes a core set of evidence- participate in Live
based practices. Life Well @ School
(2,050 schools)
The school provides curriculum
learning experiences regarding
Practice 1 668,685 children in NSW
healthy eating, physical activity
and sedentary behaviour attend a primary school51.
Nearly 562,000 children
The school explicitly addresses attend a participating school.
fundamental movement skill
Practice 2
development as part of the
PDHPE programs
The school provides the 4,617 teachers attended
opportunity for classes to eat workshops between 2008-2014.
Practice 3
vegetables and fruit and drink
water (see also page X)
The school encourages physical 7 conferences were held
Practice 4 activity during recess and/or between January 2014 and
lunch June 2015 with 669 teachers
attending from 595 schools.
The school provides a supportive
environment for healthy eating
Practice 5
(canteens, school activities
involving food and drink) There has been a significant increase in
The school provides information the number that have implemented 70%
to families on healthy eating, or more of the desired practices:
Practice 6 healthy lunchboxes, physical
activity and limiting small screen
recreation 32% 80%
in 2012 in 2016
Teaching staff are provided
with professional learning /
Practice 7 development to promote healthy The strongest increases in individual
eating and physical activity to practice improvement have related to:
students
• Physical activity during recess and/or
The school has an identified lunch (Practice 4)
team / committee with executive
• Teacher professional learning /
Practice 8 membership to support the
development on healthy eating and
implementation of LLW@S or
physical activity (Practice 7)
similar initiatives
• School team/committee with
School planning processes executive membership to support the
(e.g. strategic, annual, implementation (Practice 8)
Practice 9
operational plans) incorporate
LLW@S strategies • School planning processes
incorporate practices (Practice 9)
The school monitors and reports
annually on the implementation • School monitors and reports annually
Practice 10 on Live Life Well @ School strategies
and outcomes of LLW@S
strategies (Practice 10)
The first five years July 2011 – June 2016 027Crunch&Sip®
The implementation across NSW is supported by
the Healthy Kids Association and OPH, including:
Crunch&Sip encourages primary schools to
®
schedule a daily in-class break for students to • A school implementation guide
eat fruit or vegetables and drink water, in
addition to their usual recess and lunch • Food and nutrition focused classroom activities
breaks. Crunch&Sip® provides extra nutrition, that fit within the NSW primary schools Personal
helps to prevent dehydration and normalises Development, Health and Physical Education
drinking water, as well as giving children an curriculum and also meet other cross-curricula
opportunity to try new vegetables and fruit. outcomes
• Activity ideas based around healthy eating
Crunch&Sip® takes a whole-of-school approach, • Background nutrition information and helpful
with the program incorporated into school policy. resources for teachers.
Originating in Western Australia in 2002, Crunch&Sip®
has been operating in NSW since 2008. A vegetable,
fruit and water break such as Crunch&Sip® is part of
the Live Life Well @ School program, although schools
can participate in Crunch&Sip® separately.
Crunch&Sip® schools have a positive
impact on students by:
Creating an enjoyable daily
routine that increases fruit and
vegetable intake
Promoting a positive attitude
towards fruit, vegetables and
water
Incorporating nutrition education
into key learning areas of the
curriculum
Crunch&Sip® is currently
being implemented
across NSW in over
78%
(2,022) of
primary schools
028 NSW Healthy Children Initiative“We were concerned at the amount
of processed foods students were
consuming. To encourage healthier
eating habits, the school introduced
Crunch&Sip®. The outcomes have “It’s well worth the time
demonstrated the positive and it takes to have Crunch&Sip®,
life-changing influences that to improve students’
we, as teachers, can have concentration for
upon our students.” the remainder of
the morning.”
Feedback from teachers and schools
The first five years July 2011 – June 2016 029NSW Healthy School
Canteen Strategy
The Fresh Tastes @ School NSW There have been significant
Healthy School Canteen Strategy developments in this area since
A key action point of the
was jointly developed in 2004 by the introduction of the Strategy
NSW Healthy Eating Active
the NSW Ministry of Health, the more than ten years ago, most
Living Strategy5 is
NSW Department of Education, notably an update of the Australian
improving the availability
the Catholic Education Dietary Guidelines57 and
of healthy food and drink
Commission NSW and the accompanying Australian Guide to
in a range of settings, and
Association of Independent Healthy Eating49, the release of
implementing the
Schools of NSW. Implementation National Healthy School Canteen
Australian Dietary
of the Strategy is a requirement Guidelines58 and introduction of
Guidelines within all
for government schools and the voluntary national Health Star
nutrition initiatives.
encouraged in Independent and Rating system on packaged foods
Catholic schools. in 2014. In this developing context,
a review of the Fresh Tastes @
School canteens are an important The Strategy requires that
School NSW Healthy School
setting to target in this context, nutritious food and drink to be
Canteen Strategy was required to
with evidence that: promoted and made readily
ensure consistency with the new
available to NSW school students.
guidelines, improve
• Around 60% of NSW students Food and drink with minimal
implementation, and increase
report purchasing their lunch nutritional value is to be offered
healthy food and drinks sold in
from the school canteen at infrequently and should not be
school canteens. The review was
least once per week52 promoted. The NSW Canteen
led by the NSW Department of
Menu Planning Guide 55 outlines the
• Older students (particularly Education jointly with the NSW
requirements of the Strategy and
boys Year 8 and above) are Ministry of Health and was
is based on the 2003 Australian
more likely to report purchasing launched in Term 1 2017.
Dietary Guidelines for Children and
from the canteen more than
Adolescents56. The Menu Planning
once a week, as are students
Guide uses a traffic light system
from a low socio-economic
(red, amber and green) to classify
status background53
the nutritional value of food and
• On average, Australian school- drinks.
age children consume more
than one-third of their daily
energy intake at school. This
includes a combination of foods
purchased from canteens and
food brought from home54.
030 NSW Healthy Children InitiativeYou can also read