ONLINE TRAININGS FOR GENERAL PRACTITIONERS TREATMENT OPTIONS ON COVID-19 - a collaboration between - Effo
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ONLINE TRAININGS
FOR GENERAL PRACTITIONERS
TREATMENT OPTIONS ON COVID-19
a collaboration between
1
Onlinetrainings for GPs: treatment options on COVID-19
Initial respiratory assessment
and care 05.08.
Department of Infectious Diseases and
Respiratory Medicine, Charité
Dr. Alexander Uhrig
Dr. Miriam Stegemann
First procedures in case of
respiratory deterioration: 10.08.
Non-invasive ventilatory
support
Department of Anesthesiology and Intensive
Care Medicine, Charité
Dr. Karin Steinecke
Dr. Björn Weiß
Basic treatment and cure
under non-ICU conditions 12.08.
Department of Infectious Diseases
and Respiratory Medicine, Charité
Dr. Alexander Uhrig
Dr. Miriam Stegemann
Dr. Thomas Cronen
Stabilization of a critical patient
for referral with ambulance 17.08.
Department of Anesthesiology and Intensive Care
Medicine, Charité
Dr. Karin Steinecke
Dr. Björn Weiß 2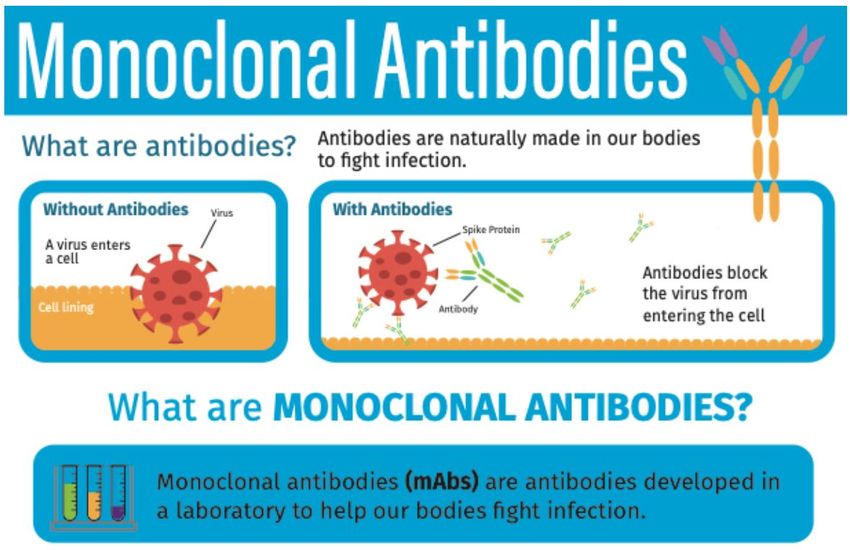
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 3

Learning Objectives • Supportive treatment outside the ICU setting - Oxygen therapy - Awake proning - Anticoagulation • Therapeutic Management - Antiviral therapy - Anti-SARS-CoV-2 Monoclonal Antibodies (mAB) - Immunomodulators • Comfort management 12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 4

heck the patient’s oxygen saturation (SpO2). If the saturation is
ow 90%, start oxygen. Chose the appropriate oxygen mask and the
Oxygen therapy 1
responding oxygen flow rate to achieve saturations of 90% - 96%.
Hypoxemia (SpO2 < 90%)? No oxygen needed
Respiratory Rate > 30/min?
"NO" Re-check patient
"YES"
NasalNasal
cannula : 1L/min
cannula 1-6 – 6 litres / minute Start with Nasal cannula if
Aim for: SpO2 90-92 (96)%
Start with RR
nasal cannula if initial oxygen
< 30/min initial oxygen saturations are 80 – 89%
saturations are 80 – 89%.
"Re-check after 5 Min"
SpO2 > 90%? Keep oxygen flow rate
Non-rebreathe
RR < 30/min?mask : 10 – 15 litres / minute
"YES" Re-check patient
Start with non-rebreathe
"NO"
mask if initial
Non-rebreathe
oxygen mask:
saturations are10 – 15
less litres
than / minute
80%.
Increase oxygen flow
rate (if still < 6 L/min)
Nasal cannula : 1 – 6 litres / minute
Start with nasal"Re-check
cannula after 5 Min"
if initial oxygen
è saturations are
If the patient’s oxygen saturations 80 – 89%.
are already above 90%,Keep
SpO2 > 90%? no additional
oxygen flow rateoxygen is
RR < 30/min? Re-check patient
"YES"
required.
è When oxygen is scare, it is better to "NO"
aim for saturations of 90 – 92% to save
oxygen. Non-rebreathe mask : 10 – 15 litres / minute
è Start
After starting oxygen, with
recheck non-rebreathe mask if initial
the oxygen saturations
Non-Rebreather- after five minutes. If the Start with Non-rebreather facemask if
Facemask 10-15 L/min
Non-rebreathe mask: 10 – 15 initial oxygen saturations < 80%
saturations are stilloxygen saturations
90%? Keep oxygen flow rate
Created by Dr. Rebecca Inglis, www.essentialcriticalcare.org
RR < 30/min?
"YES" Re-check patient
Licensed under http://creativecommons.org/licenses/by-nc-sa/4.0/
è If the patient’s oxygen saturations "NO"
are already above 90%, no additional oxygen is
required.
è When oxygen is scare, it is better to aim for saturations of 90 – 92% to save
Consider
oxygen. "Awake Proning"
è After12.08.2021
starting oxygen, recheck the oxygen Basic treatmentafter
saturations (Non-ICU) – Dr. If
five minutes. Cronen,
the Dr. Uhrig, Dr. Stegemann 5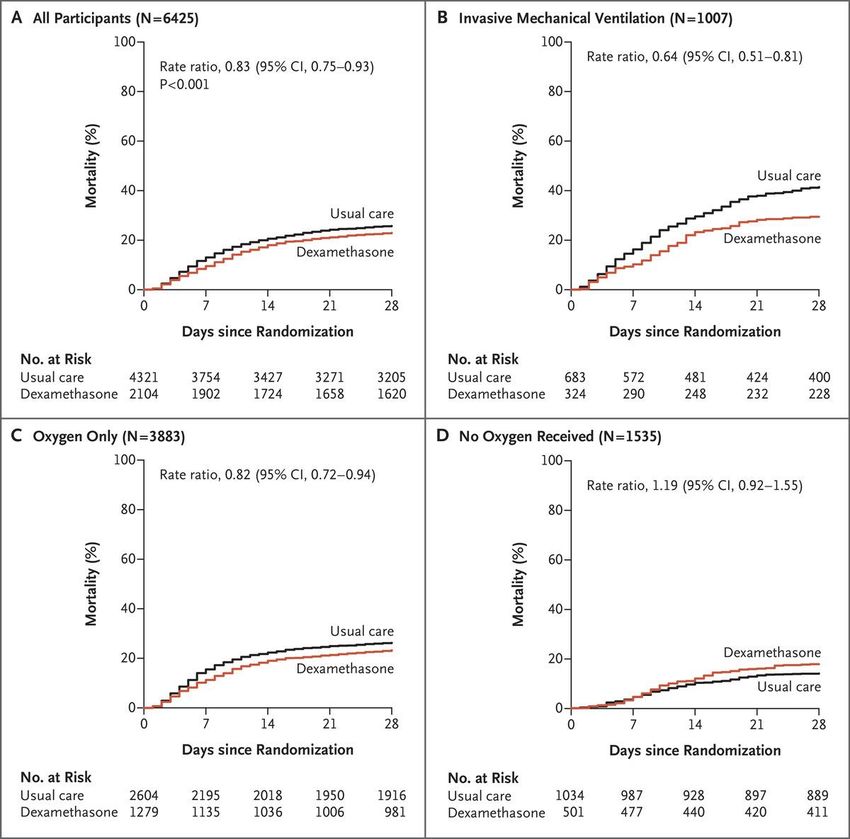
corresponding oxygen flow rate to achieve saturations of 90% - 96%.
COVID
Oxygen therapy 2 1) Check the patient’s oxygen saturation (SpO2). If the saturation is
below 90%, start oxygen. Chose the appropriate oxygen mask and the
corresponding oxygen flow rate to achieve saturations of 90% - 96%.
Consider
"Awake Proning"
"Re-check after 5 Min"
SpO2 > 90%? Keep oxygen flow rate let patient remain in prone position
RR < 30/min?
"YES" NasalRe-check
cannula : 1patient
– 6 litres / minute
(including sleeping in that position)
Start with nasal cannula if initial oxygen
"NO" saturations are 80 – 89%.
Non-rebreathe mask : 10 – 15 litres / minute
Nasal cannula : 1 – 6 litres / minute
Consider:
- adding NC (5 L/min) to
Non-rebreather FM
+
Start with non-rebreathe
Non-rebreathe
oxygen mask:
saturations are10
mask
Start with
– 15
less
if initial
nasal
litres
than 80%./ cannula
minute if initial oxygen
saturations are 80 – 89%.
- HighFlow Nasal Cannula
(40-60 L/min)
15 L/min + 5 L/min
Non-rebreathe mask : 10 – 15 litres / minute
40-60 L/min
è Start above
If the patient’s oxygen saturations are already with non-rebreathe mask if initial
90%, no additional oxygen is
Non-rebreathe
oxygen mask:
saturations are10 –
less 15 litres
than / minute
80%.
"Re-check after 5required.
Min"
è When oxygen is scare, it is better to aim for saturations of 90 – 92% to save
oxygen.
SpO2 > 90%? è After starting oxygen,Keep recheck oxygen flow saturations
the oxygen rate after five minutes. If the
RR < 30/min? Re-check patient
"YES" are stillè
Oxygen therapy: Checking the patient
• Checking of oxygen saturation (SpO2)
• Checking fit of interface (nasal cannula, non-rebreather facemask)
• When using Non-rebreather facemask: is the bag fully inflated?
• Position of the patient
- raising the head of the bed + propping patient up with pillows
- “awake proning” (separate guidance follows)
• Checking the patient’s comfort: Painful breathing?
- give analgesia when necessary 5) Check for painful breathing
- careful dose titration, when using opiates -
-
-
If the patient has painful breathing, give analgesia
Give regular paracetamol
Give a small dose of opiate as required
• Helping the patient to clear secretions: nurse-led physiotherapy
6) Nurse-led physiotherapy to promote sputum clearance (see
separate guide)
- Keep the patient active – encourage them to move and sit them out in a chair
twice a day if possible
- keep the patient active (sitting patient out in a chair twice daily) -
-
Give them exercises to do in bed
Get the patient to ‘huff’ rather than cough to clear sputum if in pain / tired.
- teach “huffing technique” (separate guidance follows) 7) Try adding nasal cannula at 5L / min
- If steps 1 – 6 haven’t worked and the oxygen saturations are still below 90%, cal
doctor to consider what to do next (depending on what is available locally).
- While you are waiting, if there is an oxygen concentrator available, try adding
nasal cannula at 5L / min to the reservoir mask at 15L / min.
è Remember, COVID-19 patients who need oxygen should also receive dexamethason
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 7
6mg once a day for 5 - 10 days. They should also be wearing TEDS stockings and hav
a prophylactic dose of low molecular weight heparin daily to prevent blood clots.
Nurse-led physiotherapy: The huffing technique
• Also known as: “huff-coughing”
• “Huffing” is not as forceful as “Coughing”, but can be less tiring
Principle:
• Taking a breath in, holding it and actively exhaling
• Enabling air to get behind mucus, separating it from airway wall
so it can be coughed out
Procedure:
• Let the patient sit up straight with chin tilted slightly up and mouth open
• Let the patient take a slow deep breath (filling his lungs about ¾ full)
• Let the patient hold his breath for 2 or 3 seconds
• Let the patient exhale forcefully, but slowly, in a continuous exhalation -
like exhaling onto a mirror to steam it up
(moving mucus from the smaller to the larger airways)
• Repeat this maneuver two more times, then follow with one strong cough
(clearing mucus from the larger airways)
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 8
Oxygen therapy: Checking the equipment 1
è Be precise with the oxygen flow rates and read from the centre of the ball
è Be precise with the oxygen flow rates and read from the centre of the ball
Read the flow
from the centre
Read theball.
of the flow 10
from the centre
This flow meter
of the ball.
• Be precise with oxygen flow rates
10
is showing
This
10 litresmeter
flow per
isminute.
showing
10 litres per • Read from the center of the ball
minute.
10
10
è When giving 15L / minute, do not turn the flow above the 15L/ minute mark or it
will waste oxygen
è When giving 15L / minute, do not turn the flow above the 15L/ minute mark or it
will waste oxygen
Do not turn the oxygen up so high that the
ball is at the very top of the flow meter. In
Do
thisnot turn the
theoxygen
flow is up so high that and
the
ball
position
is at the very top of
unpredictable,
the flow meter.
the oxygen may run out more quickly than In • When giving 15 L/min, DO NOT turn
this position the flow is unpredictable, and
expected.
the oxygen may run out more quickly than flow above “15 L/min” mark or it
expected.
will waste oxygen
Modified from www.essentialcriticalcare.org
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 9
Regulator
Cylinder tap
2) Check the equipment is working properly
Flow meter Oxygen therapy: Checking the equipment 2
Regulator
Cylinder tap
ck the equipment is working properly
Oxygen outlet Pressure gauge
• Check that the oxygen regulator is
Locking nut
Regulator
Flow meter Cylinder tap
Humidifier
correctly attached to the cylinder
è
Flow meter
Oxygen outlet Pressure gauge
- Check the oxygen regulator is correctly attached to the cylinder and that the
• Check that the locking nut is tightened
Locking nut
locking nut is tightened with a wrench. Do not use
connection.
oil or soap to lubricate the with a wrench
Humidifier
Oxygen outlet
1.1/8’’ wrench
Pressure gauge
Locking nut
• DO NOT use oil or soap to
Humidifier Cylinder tap
lubricate the connection
è - Check the oxygen regulator is correctly attached to the cylinder and that the
locking nut is tightened with a wrench. Do not use oil or soap to lubricate the
connection.
• Check that the cylinder tap is fully open
Locking nut
(when regulator firmly attached
- Check the the
- Once oxygen regulator
regulator is attached
is firmly correctlyand
attached to the
the locking nut cylinder
tightened,and that the
check
locking
thatnut
theiscylinder
tightened tap iswith
1.1/8’’ wrench fullyaopen.
wrench. Do not use oil or soap to lubricate the and nut tightened)
connection.
REMEMBER: Always close the cylinder tap before adjusting the locking nut or
removing the regulator.
Cylinder tap
• REMEMBER: always close cylinder tap
è
1.1/8’’ wrench before adjusting the locking nut or
Locking nut
- Check that there is oxygen remaining in the tank by looking at the pressure
gauge.
Cylinder tap removing the regulator
- Once the regulator is firmly attached and the locking nut tightened, check
that the cylinder tap is fully open. • Check the remaining oxygen in the tank
Pressure gauge Locking nut
REMEMBER: Always close the cylinder tap before adjusting the locking nut or by looking at the pressure gauge
removing
- Once the theisregulator.
regulator firmly attached and the locking nut tightened, check
that the cylinder tap is fully open.
è • Check that flow meter is showing
- Check that close
therethe is oxygen remaining in adjusting
the tank by looking atnut
the or
pressure
REMEMBER: Always
gauge.
cylinder tap before the locking the desired flow
removing the regulator.
Created by Dr. Rebecca Inglis, www.essentialcriticalcare.org
Licensed under http://creativecommons.org/licenses/by-nc-sa/4.0/ Modified from www.essentialcriticalcare.org
- Check that the ball in the flow meter is showing the desired flow.
12.08.2021
- Check that there is oxygenPressure
remaining Basic
gauge in the tank by treatment
looking (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann
at the pressure 10Oxygen therapy: Checking the equipment 3
è - Check that the humidifier (if using) is tightly attached and that the lid is not
cracked and fully screwed on. This is a common source of leaks.
• Check that the humidifier is
If using a “bubble humidifier”: tightly attached and that the
lid/connector is not cracked and
The lid should be
fully screwed on
screwed on tightly
If the humidifier is
Maximum water line
• Check the humidifier has the
cracked it can leak
and waste oxygen Minimum water line correct amount of water in it:
oxygen is “bubbling”
- Check the humidifier has the correct amount of water in it (between the • Check that oxygen tubing is
maximum and minimum line) and that oxygen is bubbling.
properly attached at both ends
è Check that the oxygen tubing is properly attached at both ends, and that the • Check that oxygen tubing is
tubing is not bent (feel along the length of the tubing to be sure).
è Check that the mask is working, with an intact valve, no holes and the bag is fully NOT bend
inflated
Should we use oxgen humidifiers?
eck the• maskno fits
routine
well topractice to humidify
the patient’s face supplemental oxygen for low flow oxygen
- Tighten theviaelastic
nasalstrapcannula (1-5 L/min)
- Mould the metal
- Check the nose
ball inpiece to their nasal bridge the desired flow.
• tothat
- Explain Oxygen the flow
the patient should
meter
always
the importance
is showing
be humidified
of keeping it on if it bypasses the upper airway and is
introduced through an endotracheal tube/tracheostomy tube
• patient
sition the Always keep the patient hydrated Modified from www.essentialcriticalcare.org
- Sit the patient up in bed by raising the head of the bed and prop them up with
12.08.2021
pillows. Recheck their oxygen saturations.Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 11Oxygen therapy: HighFlow Nasal Cannula (HFNC)
High-flow
air-oxygen blender
with flowmeter
Tube from blender
to humidifier
Heated
Specialized
humidifier
nasal cannula
Tube from
humidifier
• FiO2 can be set from 0.21 to 1.0
• Flow rates up to 60 L/min
• Gas is heated to 37°C with 100% relative humidity
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 12Oxygen therapy: HFNC – the principle behind
To effectively deliver the set FiO2
to the patient in acute respiratory distress
you have to
• Exceed the minute ventilation
• Match the inspiratory demand
(peak inspiratory flow)
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 13Oxygen therapy: HFNC – the principle behind
• Continous high flow oxygen
washes out the upper airways
• Avoids rebreathing of CO2
from the anatomic deadspace,
functionally decreasing
anatomic dead space
Clearance of radioactive tracer from upper airway model,
Gamma camera imaging superimposed on a CT scan
Möller W J Appl Physiol 2017;122:191–197
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 14Instructions
tions for awake proning offor
a awake proning 1
t on oxygen via a reservoir mask
When to try awake proning:
• Try proning any patient with COVID-19
who requires supplemental oxygen to
maintain oxygen saturations above 90%
• DO NOT attempt proning if the patient is
unconscious or has a respiratory rate
greater than 40 breaths/minute
Equipment required:
• Mattress (or pile of folded blankets)
• Bedsheet
• Minimum 3 pillows (or more for obese patients)
• Rolled towel (optional)
y awake proning: • Means for patient to attract attention
patient with COVID-19 who requires supplemental oxygen to maintain
ons above 90%. Don’t attempt proning if the patient is unconscious or has a
(rattle, bell, buzzer, mobile phone)
greater than 40 breaths per minute. • Pulse oximeter
• Additional padding for pressure areas if required
required:
s (or pile of folded blankets) Modified from www.essentialcriticalcare.org
et
m 3 pillows12.08.2021
(more for obese patients) Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 15Instructions for awake proning 2
1. Communicate
Explain to the patient (and his family) that this position will
hopefully help breathing
2. Prepare the equipment and staff members
- gather needed equipment (see check list above)
- have 2 members of staff present
3. Prepare the patient
- take a set of vital signs
- turn up oxygen to 15 L/min (if not at 15 L/min already) for the
duration of the procedure
Modified from www.essentialcriticalcare.org
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 16Instructions for awake proning 3
4. Turn the patientProcedure:
1) COMMUNICATE:
- lay the bed flat Explain what proning will entail to the patient and their family. Explain that this position will
hopefully help their breathing.
- ask the patient to turn onto stomach and position themselves
2) PREPARE THE EQUIPMENT:
comfortably - support patient to turn over
Gather as many pillows, towels and blankets as are available. It is best for the patient to be
lying on a mattress with a bedsheet where possible to avoid pressure sores. If none is
available, use a pile of blankets instead.
- position a first pillow under the chest or chest and abdomen
3) PREPARE THE PATIENT:
Take a set of vital signs then turn up the oxygen to 15L/min (if not at 15L/min already) for the
(depending on patient preference and habitus) and a second
duration of the procedure.
pillow (or rolled towel) under the forehead:
4) TURN THE PATIENT:
With two members of staff present, lay the bed flat. Ask the patient to turn themselves onto
this will leave a gully for the reservoir bag of the oxygen mask
their tummy and position themselves however feels most comfortable. Support them to turn
over. Position a first pillow under their chest or chest and abdomen (depending on patient
to be fully inflated wether the head is straight or to the side
preference and habitus) and a second pillow or a rolled towel under their forehead. This will
leave a gully for the reservoir bag of the oxygen mask to be fully inflated whether the head is
straight or to the side. Ask the patient to orient their head in whatever position they find
- ask the patient to orient the head in whatever position is
most comfortable.
most comfortable
Pillow or rolled
towel to support
head in most
comfortable
position
Pillow under
chest Gully between
pillows to allow
bag to be fully
inflated Modified from www.essentialcriticalcare.org
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 17Instructions for awake proning 4
5. Adjust the oxygen
- adjust the tubing of the reservoir mask so it points directly
towards5)the
ADJUSToxygen source and is NOT caught underneath
THE OXYGEN:
the patient
Adjust the tubing of the reservoir mask so it points directly towards the oxygen source and is
- make sure theunderneath
not caught mask the is NOT
patient. being
Make surepushed
the mask is notagainst the
being pushed patient’s
against the face
patient’s face.
5) ADJUST THE OXYGEN:
Adjust the tubing of the reservoir mask so it points directly towards the oxygen source and is
not caught underneath the patient. Make sure the mask is not being pushed against the
patient’s face.
Tubing should
Tubing should
not point not point
downwards due downwards due Tubing is now
correctly
Tubing is now
to the risk of it
to the risk of it getting bent pointing correctly
under the towards oxygen
getting bent patient source pointing
under the towards oxygen
patient source
The oxygen
tubing should
be clearly
visible and not
bent or twisted
The oxygen
tubing should Modified from www.essentialcriticalcare.org
be clearly
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig,
visible and not Dr. Stegemann 18Instructions for awake proning 5
6) PREVENT PRESSURE SORES:
6. Prevent pressure sores
Position the remaining pillows and other bedding to minimise pressure on the limbs and to
- position the remaining pillows andas comfortable
make the patient other asbedding toshould
possible. The knees minimize
be slightly flexed and the
arms supported at a comfortable angle. Ask them what position is most comfortable for each
pressure on the limbs and limb.
toPlastic
make thewithpatient
gloves filled water can also beasusedcomfortable
to support limbs.
as possible
- the knees should be slightly flexed and the arms supported at a
The patient’s arm
comfortable angle (ask patient
should what
not rest position is most comfortable for each limb)
on the hard metal
bed frame – it
- plastic gloves filled with water can also be used to support limbs
needs padding
underneath
- removing the foot of the bed can also be helpful
6) PREVENT PRESSURE SORES:
- encourage the patient to reposition themselves when required or to
Position the remaining pillows and other bedding to minimise pressure on the limbs and tothe foot of the bed can also be helpful. Encourage the patient to reposition
Removing
make the patient as comfortable as possible. The knees should be slightly flexedthemselves
and the when required or to call for help when they feel uncomfortable.
call for help whem they feel uncomfortable
arms supported at a comfortable angle. Ask them what position is most comfortable for each
limb. Plastic gloves filled with water can also be used to support limbs.
The patient’s arm
Remove the foot
should not rest
of the bed and
on the hard metal
place a pillow
bed frame – it
under the lower
needs padding
legs to reduce
underneath
pressure on the
knees and feet
Modified from www.essentialcriticalcare.org
19
Removing the foot of the bed can also be helpful. Encourage the patient to reposition
12.08.2021
themselves when required or to call for help when they feelBasic treatment (Non-ICU)
uncomfortable. – Dr. Cronen, Dr. Uhrig, Dr. Stegemann
Created by Dr. Rebecca Inglis, www.essentialcriticalcare.orgInstructions for awake proning 6
7. Re-check the patient
- take appropriate set of vital signs (blood pressure, heart rate,
respiratory rate, oxygen saturation)
- adjust the oxygen flow aiming for oxygen saturations of 90-96%
8. Monitor the patient
- keep continous pulse oximetry in place if possible
- give patient some means to attract attention if necessary
(rattle, bell, buzzer, mobile phone)
- make sure a member of staff is nearby when a patient is
in prone position
- ask the patient to remain in this position as long as tolerated
- can alternate with a lateral position or supported upright in bed
Modified from www.essentialcriticalcare.org
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 20Anticoagulation in COVID-19 patients
• COVID-19 is associated with an hypercoagulable state
• Risk of thromboembolic disease is increased in critically ill (and
sometimes well-appearing) individuals
• Thromboembolism is typically venous
but in some cases may be arterial
• Spontaneous bleeding is much less common but can occur
(including intracerebral bleeding)
• Decisions about anticoagulation are made based on clinical criteria,
rather than on isolated laboratory findings such as D-dimer
(primarily used as a measure of disease severity and prognosis)
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 21Anticoagulation in COVID-19 patients
Thromboembolism
- documented?
- strongly suspected
Yes No
Possible acute ischemia/infarction? Already taking anticoagulation?
- acute MI - atrial fibrillation
- acute stroke - post VTE
- massive PE Yes No
- limb DVT/arterial thrombosis
Yes No Anticoagulation should be continued Severity of COVID-19 warrants admission to hospital?
- unless contraindication exists
Thrombolytic therapy (tPA) may be appropriate Anticoagulation is appropriate - switching to shorter-acting parenteral agent in Yes No
- transfer to ICU/follow local protocol - use full-dose anticoagulation hospitalized patients
Prophylactic dose anticoagulation is appropriate Outpatient care as indicated:
- full-dose anticoagulation if tPA not given - follow local protocol - outpatients should continue current therapy
- LMW heparin is usually preferred - continue anticoagulant if already taking
- unfractionated heparin in selected cases - prophylactic anticoagulation only for selected
(CrCl < 15 ml/min or RRT) high-risk patients
- Fondaparinux may be used in case of HIT - all others usually do not require anticoagulation
*
* High-risk features include prior VTE, recent surgery/trauma, immobilization, or morbid obesity.
• there are no high-quality studies to support interventions that go beyond standard indications
• antithrombotic therapies carry risks of increased bleeding
• In the absence of high-quality data to guide management, institutions may vary
in how aggressively they approach prevention/treatment of thromboembolic complications
• Consider laboratory resources, necessary for monitoring more aggressive anticoagulation
• Thromboprophylaxis is generally not continued following discharge, with rare exceptions
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 22Therapeutic Management – Patient #1 presenting to your
A&E
#Case 1
• Male patient, 42yr, no known risk factors
• Fever, coughing and myalgias, onset of symptoms roughly
5 days ago.
• Tested positive for SARS-CoV-2 (PCR) yesterday
• GCS 15, HR 98 bpm, BP 105/65 mmHg, RR 36
breaths/min, T 38.8 °C, SpO2 91% (on room air), on CXR
bilateral pulmonary opacities
• Treatment options?
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 23Therapeutic Management – Patient #2 presenting to your
A&E
#Case 2
• Female patient, 72yr, H/O diabetes, hypertension (BMI 37
kg/m2)
• Fever, fatigue, onset of symptoms roughly 3 days ago
• Tested positive for SARS-CoV-2 (PCR) today
• GCS 15, HR 76 bpm, BP 150/95 mmHg, RR 20
breaths/min, T 38.2 °C, SpO2 96% (on room air)
• Treatment options?
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 24Therapeutic Management - Overview
Dexamethasone • Symptomatic patients with oxygen therapy /
ventilatory support
• Pat. > 12yr and >40kg
• Benefit in case of invasive ventilation greater
than in oxygen therapy / NIV
Remdesivir • Antiviral drug
• COVID-19 pneumonia with
≤ 7d since symptom
oxygen therapy
onset
• Pat. > 12yr and >40kg
• Uncertain evidence
No Low-flow High-flow
Invasive
respiratory oxygen oxygen
ventilation
support therapy therapy / NIV
mAB • Asymptomatic patients with risk
factors
≤ 7d since symptom onset
• Seronegative patients with not
Max. 72h after NAAT+
more than low-flow oxygen
Tocilizumab • Worsening symptoms
and marked
pulmonary
hyperinflammation
despite
dexamethasone
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 25Therapeutic Management - Systemic Corticosteroids
• Since good quality evidence emerged for the use of corticosteroids
in severe or critical COVID-19 patients resulting in reduced
mortality, the administration is universally recommended
RECOVERY
Collaborative
Group
RECOVERY Collaborative
Group. NEJM. 2021;384:693.
NCT04381936.
www.recoverytrial.net.
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 26Therapeutic Management - Systemic Corticosteroids
• Further studies show that the administration of systemic corticosteroids,
compared with usual care or placebo, was associated with lower
mortality in critically ill patients with COVID-19
JAMA. 2020;324(13):1330-1341. doi:10.1001/jama.2020.17023
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 27Therapeutic Management - Systemic Corticosteroids
• Systemic Corticosteroids should be administered to all hospitalized
patients with severe or critical COVID-19, preferably after 7 days of
symptoms onset (however, if in doubt, administration is recommended
within 7 days)
• Dexamethasone 6 mg IV or PO q24h or prednisolone 40 mg IV or PO,
methylprednisolone 32 mg IV (8 mg q6h or 16 mg q12h), hydrocortisone
150 mg IV (50 mg q8h)
• Duration: 10 days
• Very high bioavailability of dexamethasone (but be aware of intestinal
dysfunction in critically ill patients)
• Side effects are rare during short course of treatment. Be aware of
elevation of blood pressure and increased blood glucose level
(measurement of blood glucose level is recommended – not only in
diabetic patients)
• Corticosteroids are on the WHO Model List of Essential Medicines and
almost universally at a low cost available
WHO “Therapeutics and COVID-19: living guideline” 06 July 2021
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 28Therapeutic Management - Remdesivir
Repurposed Antiviral Drugs for Covid-19. Interim WHO Solidarity Trial Results.
N Engl J Med 2021; 384:497-511. DOI: 10.1056/NEJMoa2023184
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 29Therapeutic Management - Remdesivir
• If administration is considered, the following should be noted:
o Only in patients ≥ 12yr and ≥ 40kg
o Contraindicated in liver (ALT ≥ 5xULN) and/or renal (eGFR <
30ml/min) dysfunction
o Loading dose: 200mg IV on day 1, followed by 100mg IV q24h
day 2-5* (*may be increased to 10 days in patients not demonstrating clinical improvement)
o Side effects: headache, nausea, hypersensitivity reaction, liver
dysfunction
• Given the uncertainty of evidence, the unfavourable cost
effectiveness, the need for administration by IV route and the
limited availability, the use of remdesivir is at least disputable
WHO “Therapeutics and COVID-19: living guideline” 06 July 2021
Ansems K, Grundeis F, Dahms K, Mikolajewska A, Thieme V, Piechotta V, Metzendorf M-I, Stegemann M, Benstoem C, Fichtner F. Remdesivir for the
treatment of COVID‐19. Cochrane Database of Systematic Reviews 2021, Issue 8. Art. No.: CD014962. DOI: 10.1002/14651858.CD014962.
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 30Therapeutic Management - IL-6 receptor blockers:
Tocilizumab or Sarilumab
anti-inflammatory
monoclonal antibodies
• Administration
• Single intravenous dose, typically over 1 hour
• A second dose may be administered 12 to 48 hours after the first dose (offered
variably in major clinical trials at discretion of treating clinician)
• Dose
• Tocilizumab: 8 mg per kilogram of actual body weight, up to a maximum of 800 mg
• Sarilumab 400 mg (REMAP-CAP)
• Renal dose adjustment: not currently warranted for either drug
Pelaia, C. et al Therapeutic Role of Tocilizumab in SARS-CoV-2-Induced Cytokine Storm: Rationale and Current Evidence. Int. J. Mol. Sci. 2021, 22, 3059.
WHO “Therapeutics and COVID-19: living guideline” 06 July 2021
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 31Therapeutic Management - IL-6 receptor blockers:
Tocilizumab or Sarilumab
WHO REACT. Association Between Administration of IL-6 Antagonists and Mortality Among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA. July 06, 2021
WHO “Therapeutics and COVID-19: living guideline” 06 July 2021
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 32Therapeutic Management - IL-6 receptor blockers:
Tocilizumab or Sarilumab
• “We recommend treatment with IL-6 receptor blockers for
patients with severe or critical COVID-19”
• IL-6 receptor blockers should be initiated with systemic
corticosteroids (duration: up to 10 days)
• IL-6 receptor blockers have been administered early in the
course of hospitalization in the major clinical trials and clinicians
may consider this approach if possible
• Resources: expensive, recommendation does not take cost-
effectiveness into consideration. Access might be limited.
• WHO recommendation should provide a stimulus to engage all
possible mechanisms to improve global access
WHO “Therapeutics and COVID-19: living guideline” 06 July 2021
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 33Therapeutic Management - Anti-SARS-CoV-2 Monoclonal
Antibodies
(mAB)
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 34Therapeutic Management - Anti-SARS-CoV-2 Monoclonal
Antibodies
(mAB)
• Bamlanivimab plus etesevimab
• REGN-COV2 (Casirivimab plus imdevimab)
• Regdanvimab
• Sotrovimab
• …
• Treatment of mild to moderate COVID-19
• Patients with laboratory-confirmed SARS-CoV-2 infection AND
• who are at high risk of clinical progression (f. ex. immunocompromising condition
or immunosuppressive therapy)
• Treatment should be started as soon as possible after the patient receives a
positive result on a SARS-CoV-2 antigen or PCR and within 7 (- 10) days of
symptom onset
• Treatment of severe COVID-19
• Patients who have not developed an antibody response or who are not expected
to mount an effective immune response to SARS-CoV-2 infection
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 35Therapeutic Management - Anti-SARS-CoV-2 Monoclonal
Antibodies
(mAB)
Antibody resistance of SARS-CoV-2 variants
Susceptible
*Used in combination with Bamlanivimab
** Used as combination Casirivimab/Imdevimab Not Susceptible
https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/COVRIIN_Dok/Monoklonale_AK.pdf?__blob=publicationFile
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 36Therapeutic Management - Anti-SARS-CoV-2 Monoclonal
Antibodies
(mAB) – Literature
• Weinreich DM, Sivapalasingam S, Norton T, et al.: REGN-COV2, a Neutralizing Antibody Cocktail, in
Outpatients with Covid-19. N Engl J Med. 2020 Dec 17. doi: 10.1056/NEJMoa2035002. Epub ahead
of print
• Horby PW, RECOVERY Collaborative Group: Casirivimab and imdevimab in patients admitted to 4
hospital with COVID-19 (RECOVERY): a randomised, 5 controlled, open-label, platform trial.
medRXiv (preprint): https://doi.org/10.1101/2021.06.15.21258542
• Chen P, A. Nirula A, Heller B, et al.: SARS-Cov-2 Neutralizing Antibody Ly-Cov555 in Outpatients
with Covid-19. N Engl J Med 8. Oktober 2020; doi: 10.1056/NEJMoa 2029849
• Wang P, Nair MS, Liu L et al.: Antibody resistance of SARS-COV-2 variants B1.351 and B.1.1.7.
Nature. 2021: 593, 130-135
• Planas D et al.: Reduced sensitivity of infectious SARS-CoV-2 variant B.1.617.2 to monoclonal
antibodies and sera from convalescent and vaccinated individuals
• Gottlieb RL, Nirula A, Chen P, et al.: Effect of Bamlanivimab as Monotherapy or in
Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19: A
Randomized Clinical Trial. JAMA. 2021 Jan 21:e210202. doi: 10.1001/jama.2021.0202 13
• ACTIV-3/TICO LY-CoV555 Study Group, Lundgren JD et al.: A Neutralizing Monoclonal
Antibody for Hospitalized Patients with Covid-19. N Engl J Med. 2020 Dec 22:NEJMoa2033130.
doi: 10.1056/NEJMoa2033130
• O'Brien MP, Forleo-Neto E, Musser BJ et al.: Covid-19 Phase 3 Prevention Trial Team. Subcutaneous
REGEN-COV Antibody Combination to Prevent Covid-19. N Engl J Med. 2021 Aug 4. doi:
10.1056/NEJMoa2109682. Epub ahead of print. PMID: 34347950.
29.07.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 37Therapeutic Management - Anti-SARS-CoV-2 Monoclonal
Antibodies
(mAB)
• .. Role in preventing SARS-CoV-2 infection in household contacts of
infected patients?
• .. Role during skilled nursing and assisted living facility outbreaks?
• Resources: Access might be limited
• availability of measurement of serostatus
• availability of mAB
• high cost of treatment
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 38Therapeutic Management - Ivermectin
• “We recommend not using
ivermectin in patients with
covid-19 except in the
context of a clinical trial”
• “Based on the current very
low- to low-certainty
evidence, we are uncertain
about the efficacy and
safety of ivermectin used
RAPID RECOMMENDATIONS: A living WHO guideline on drugs for covid-19, BMJ 2021
to treat or prevent COVID-
19…Overall, the reliable
evidence available does
not support the use
ivermectin for treatment
or prevention of COVID-19
outside of well-designed
randomized trials.”
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 39Therapeutic Management - Summary of recommendation
RAPID RECOMMENDATIONS: A living WHO guideline on drugs for covid-19, BMJ 2021 https://www.bmj.com/content/370/bmj.m3379
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 40Managing the crisis: Comfort care
“To cure sometimes, to relieve often, and to comfort always.”
... or: What to do, when we think we can do nothing more.
• Many patients with COVID-19 experience distressing symptoms, including
breathlessness and agitation: Treatment of this kind of suffering is an
important part of COVID-19 care, irrespective of prognosis
• Patients with severe COVID-19 may deteriorate rapidly: It is useful to have
a strategy in place for managing deterioration and potential death
(for those not suitable for escalation to intensive care).
This strategy runs alongside the acute medical management plan.
• Clear and timely communication with the patient and his family is
essential: Try to find a balance between hope that treatments will help
and the explicit acknowledgement that patients are sick enough to die.
Ting R BMJ 2020;370:m2710
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 41Managing the crisis: Comfort care
Most common symptoms in patient with severe COVID-19:
• Breathlessness and agitation
• Cough
• Fatigue and drowsiness
Rapid deterioration (median data from China and Italy, 2020)
• Time from first symptom to breathlessness: 5 days
• Time from onset of symptoms to hospitalization: 5 days
• Time from first symptom to ARDS: 8 days
• Time from onset of symtoms to death: 9 days
An anticipatory approach to symptom management is key
Ting R BMJ 2020;370:m2710
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 42How can breathlessness in severe COVID-19 be managed?
• Mainstay of pharmacological management is opioids
• When to consider opioid therapy:
Patients who are severely breathless at rest or on minimal exertion
• Drug of choice (in absence of renal impairment): morphine
• Patient able to take oral medication:
oral immediate release morphine, starting at 2.5mg every 4 hours
• Patient unable to swallow or drowsy/unconscious:
parenteral morphine (bolus dosing or continuous parenteral infusions),
- titrating dose to symptom severity
- infusions reducing the need for frequent “as needed doses”
data from 2 UK studies (outside ICU):
median of 10/16 mg during final 24 hours (subcutaneous infusion)
Ting R BMJ 2020;370:m2710
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 43How can breathlessness in severe COVID-19 be managed?
• Non-pharmacological management:
- staff having a calm and reassuring manner
- using cool wipes on the face (safely disposed after each use)
- use of handheld fans not recommended because of risk of aerosol spread
- no data on symptom relieve through prone positioning
• Oxygen therapy:
- Oxygen therapy may help relieve breathlessness in severe hypoxemia
- no evidence to support the use of oxygen in the absence of hypoxemia
- priority is to treat the symptom of breathlessness
rather than oxygen saturation levels:
ask the patient – measure respiratory rate – look for use of accessory muscles
(observe for signs of increased work of breathing)
- use an interface that the patient is most comfortable with
(nasal cannula instead of facemask?)
- always use an individualized approach
Ting R BMJ 2020;370:m2710
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 44How can agitation and anxiety be managed in severe COVID-19?
Pharmacological treatments:
• Benzodiazepines
- alone or in combination with opioids
- dose titration needed to achieve good symptom relief
• In case of delirium (disorientation to time, place, or person):
Haloperidol (instead of or in addition to benzodiazepines)
Non-pharmacological treatments:
• “Humanize” healthcare workers wearing PPE by writing their names or
pinning photos of their faces onto their PPE
• If a patient with severe covid-19 expresses a fear of dying:
(a) reassure them that they are receiving treatments that aim to support their
bodies to recover from the effects of the virus,
but be honest that there is still a worry they are very sick and could die
(b) reassure them that treatments are available to ensure that
they are comfortable
(c) ask them what is important to them right now and
if there is anyone they would like you to speak to about their situation
Ting R BMJ 2020;370:m2710
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 45What is the best way to communicate with patients and families?
• Use a clear language
• Being honest
Honest conversation delivered well provides patients
and families with the choice to use that information
to organize what is important in their lives and to say Phrases that might be helpful when communicating with patients
what they need to say in the event that they do not with severe COVID-19 and their families and friends
recover
• Communicate in a timely manner
- if needed several times a day -
• Taking into account the urgency of
conveying important updates
if the patient is deteriorating
• Communication can be challenging
when using PPE
• Get accustomed to use phone calls
or video calls for communication
with families
Video calls seem to be enhancing the “therapeutic
presence” of the healthcare professional
Ting R BMJ 2020;370:m2710
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 46End of the third training session
Questions?
12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 47Contact details and legal notice Contact details • EFFO@rki.de Legal Notice • Publisher: www.rki.de | Editor: www.rki.de/zbs7 • Content: www.infektiologie- pneumologie.charite.de/en/services/medical_focus/ • www.charite.de/en/charite/charitecenters/anesthesiology_and_ intensive_care_medicine/ • Illustration: www.goebel-groener.de | Photographs: www.effo.rki.de 12.08.2021 Basic treatment (Non-ICU) – Dr. Cronen, Dr. Uhrig, Dr. Stegemann 48
You can also read