Original Article Association of semi-quantitative cryptococcal antigen results in plasma with subclinical cryptococcal meningitis and mortality ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Medical Mycology, 2021, 59, 1041–1047
https://doi.org/10.1093/mmy/myab038
Advance Access Publication Date: 25 June 2021
Original Article
Original Article
Association of semi-quantitative cryptococcal antigen results in
plasma with subclinical cryptococcal meningitis and mortality
among patients with advanced HIV disease
Downloaded from https://academic.oup.com/mmy/article/59/10/1041/6309311 by guest on 18 November 2021
Nozuko P. Blasich1,2 , Rachel M. Wake1,3 , Ivy Rukasha1 , Yvonne Prince2 and
Nelesh P. Govender 1,4,5,∗
1
National Institute for Communicable Diseases (Centre for Healthcare-Associated Infections, Antimicrobial Resis-
tance and Mycoses), a Division of the National Health Laboratory Service, Sandringham 2131, Johannesburg, South
Africa, 2 Department of Biomedical Sciences, Faculty of Health and Wellness, Cape Peninsula University of Tech-
nology, 7530, Cape Town, South Africa, 3 Institute of Infection & Immunity, St George’s, University of London, SW17
0RE, London, United Kingdom, 4 School of Pathology, Faculty of Health Sciences, University of the Witwatersrand,
2193, Johannesburg, South Africa and 5 Division of Medical Microbiology, Faculty of Health Sciences, University of
Cape Town, 7935, Cape Town, South Africa
∗
To whom correspondence should be addressed: Nelesh Govender, National Institute for Communicable Diseases, 1 Modderfontein
Road, Sandringham 2131, Johannesburg, South Africa. Tel: +27 11 555 0353; E-mail: neleshg@nicd.ac.za
Received 26 March 2021; Revised 21 June 2021; Accepted 23 June 2021; Editorial Decision 23 June 2021
Abstract
Blood cryptococcal antigen (CrAg) titers >160 are associated with concurrent subclinical cryptococcal menin-
gitis (CM). When lumbar puncture (LP) is not immediately available in a CrAg screening program, semi-
quantitative CrAg assays may provide risk stratification for CM. Two semi-quantitative assays (SQ [Immuno-
Mycologics, Norman, OK, USA] and CryptoPS [Biosynex, Strasbourg, France]) were evaluated against a
qualitative lateral flow assay (LFA) using 194 plasma samples from a cohort of HIV-seropositive individuals
with CD4 counts 160. Fifty individuals with antigenemia had an LP; a clinically useful SQ score that identified all ten
cases of subclinical CM was ≥3 (100% sensitivity, 55% specificity). Patients with an SQ score of 3 or 4 also
had a 2.2-fold increased adjusted hazards of 6-month mortality (95% CI: 0.79–6.34; p = 0.13) versus those
with score of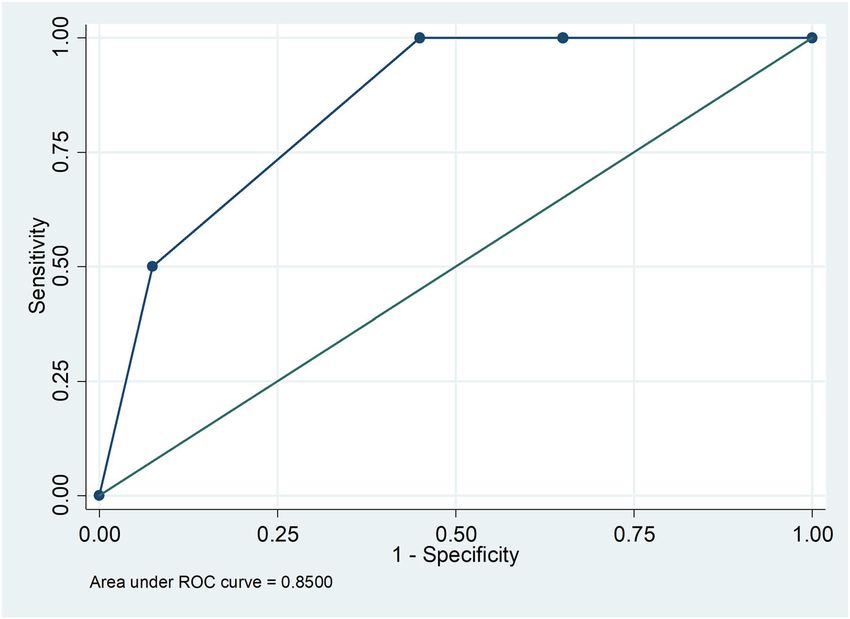
1042 Medical Mycology, 2021, Vol. 59, No. 10 Introduction Methods HIV-associated cryptococcal meningitis (CM), caused by Cryp- A prospective cohort study was conducted at Helen Joseph and tococcus neoformans in the vast majority of cases and less Tambo Memorial hospitals in Johannesburg, South Africa from frequently by Cryptococcus gattii, accounts for an estimated June 2015 through to October 2017.9,13 HIV-seropositive adults 15% of AIDS-related deaths in sub-Saharan Africa.1 A lateral ≥18 years of age with a CD4 count of
Blasich et al. 1043
Table 1. Sensitivity and specificity of the SQ and CryptoPS assays for detection of CrAg in frozen-thawed plasma from HIV-seropositive
patients with a CD4 count of 100 15.19 7.71–29.90
Negative likelihood ratio 0.02 0.00–0.12 0.11 0.05–0.23
Note: Cryptococcal antigen (CrAg) enzyme immune-assay (EIA) results for the 194 participants were positive for 58 and negative for 136. Compared to the EIA, the sensitivity
and specificity of the semi-quantitative (SQ) qualitative results were 100% (58/58) and 99% (135/136) while Crypto PS had 91.4% (53/58) sensitivity and 93.4% (127/136)
specificity.
Downloaded from https://academic.oup.com/mmy/article/59/10/1041/6309311 by guest on 18 November 2021
and CryptoPS assays compared to those of the LFA. We used
the LFA as the primary reference method because this assay has
been validated for use in the national CrAg screening program.
We used EIA results to resolve discrepancies. We also calculated
diagnostic likelihood odds ratios. For LFA-positive samples, we
compared SQ scores and CryptoPS results to titers. For the sub-
set of patients with CSF CrAg results, a receiver operating char-
acteristic (ROC) curve was used to assess cut-off SQ scores for
detecting subclinical CM. A chi-square test was used to assess
the association between CryptoPS results and subclinical CM.
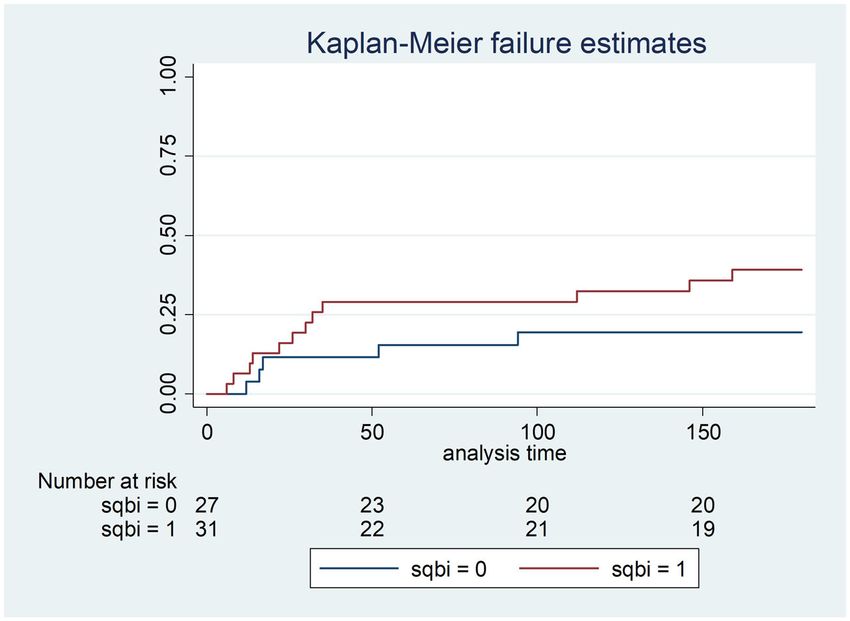
We used a Cox proportional hazards model to determine the as-
sociation between plasma SQ scores and mortality. A high SQ
score was defined as 3 or 4 and a low score as 1 or 2. We plotted
Kaplan-Meier survival curves over 6 months of follow-up for the
cohort by SQ score category. Figure 1. SQ assay scores compared to lateral flow assay (LFA) log2 titers from
HIV-seropositive patients with a CD4 count of
1044 Medical Mycology, 2021, Vol. 59, No. 10
Table 2. Association between SQ assay scores, lateral flow assay titers and subclinical cryptococcal meningitis (CM) for 50 patients with
antigenemia and lumbar puncture results
SQ assay Samples CrAg LFA CrAg LFA Subclinical CM No subclinical
score n = 50 titre ≤160 (n = 33) titre >160 (n = 17) (n = 10) CM (n = 40)
Negative 0 0 0 0 0
1 14 (28%) 14 (42%) 0 0 14 (35%)
2 8 (16%) 7 (21%) 1 (6%) 0 8 (20%)
3 20 (40%) 12 (37%) 8 (47%) 5 (50%) 15 (37%)
4 8 (16%) 0 8 (47%) 5 (50%) 3 (8%)
Downloaded from https://academic.oup.com/mmy/article/59/10/1041/6309311 by guest on 18 November 2021
Figure 2. A receiver operating characteristic curve for plasma semi-quantitative (SQ) scores and subclinical cryptococcal meningitis among 50 asymptomatic
cryptococcal-antigen positive patients.
Table 3. Sensitivity and specificity of SQ assay score cut-offs from ≥1 to ≥4 for detecting subclinical cryptococcal meningitis among
asymptomatic CrAg-positive patients with lumbar puncture results (n = 50)
Cut point Sensitivity % Specificity Positive likelihood ratio Negative likelihood ratio
≥1 100 0 1.0000
≥2 100 35 1.5385 0.0000
≥3 100 55 2.2222 0.0000
≥4 50 92.5 6.6667 0.5405
5 0 100 1.0000
Receiver operating characteristic area = 0.85 (95% CI: 0.75–0.95).
other 4 had positive CryptoPS results (Table 4). Nine of ten pa- Discussion
tients with subclinical CM had a strong-positive CryptoPS re- In this re-evaluation of stored plasma samples from a prospec-
sult versus 10/40 without subclinical CM (pBlasich et al. 1045
Downloaded from https://academic.oup.com/mmy/article/59/10/1041/6309311 by guest on 18 November 2021
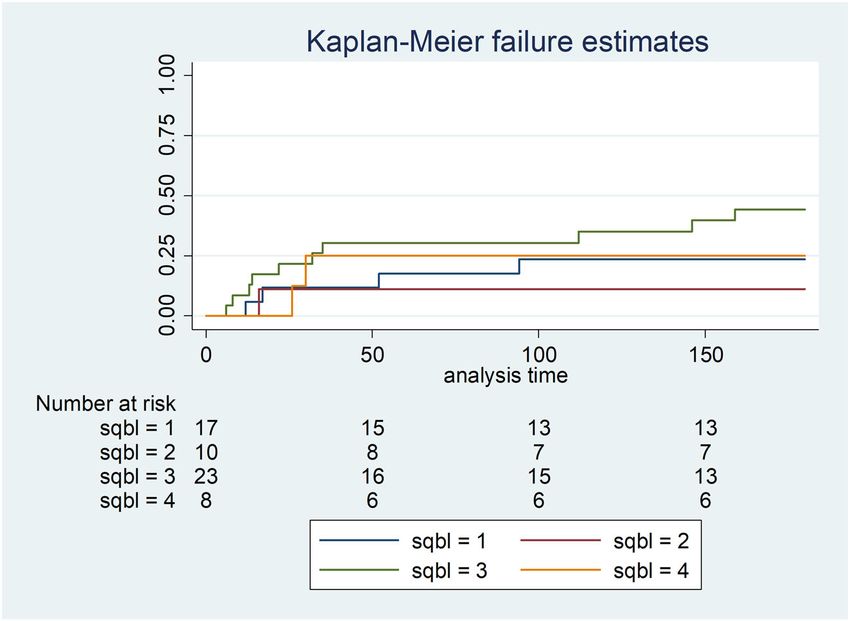
Figure 3. Kaplan-Meier survival estimates in 58 CrAg-positive patients by plasma SQ assay score category (0: score of ≥3 and 1: score of 160 (n = 17) (n = 10) CM (n = 40)
Negative 5 (10%) 5 (15%) 0 0 5 (12%)
Positive 26 (52%) 22 (67%) 4 (24%) 1 (10%) 25 (63%)
Strong positive 19 (38%) 6 (18%) 13 (76%) 9 (90%) 10 (25%)1046 Medical Mycology, 2021, Vol. 59, No. 10
subclinical CM but had low specificity. A cut-off score of ≥4 re- (a composite endpoint of microbiologically confirmed CM
duced the sensitivity of this assay substantially but was much and/or clinical signs of meningitis).14 Individuals with SQ scores
more specific for CM. For the purposes of risk stratification for of 2 or 3 were classified as being at moderate risk of central
subclinical CM among patients with antigenemia, a more sensi- nervous system involvement and mortality, with a preliminary
tive cut-off (i.e., a score of ≥3) is preferable and specificity is a recommendation for more intensive evaluation including lumbar
far less important consideration, given that lumbar puncture is puncture. In our study, a strong-positive CryptoPS result was rel-
now universally recommended. Although the CryptoPS assay did atively sensitive and picked up 9 of 10 cases of subclinical CM
not perform well as a qualitative assay compared to the LFA, a but also 10/40 (25%) of those without CM. The lack of a clearer
strong-positive result was a relatively sensitive screening test for association between the semi-quantitative CrAg results and sub-
subclinical CM, though this was also not specific. clinical CM in our study might be explained by a smaller sample
As previously reported, the SQ assay accurately detected size since we restricted our analysis to patients who had a lumbar
CrAg compared to the LFA.14,15 In our study, only one low-titer puncture. We found that CrAg-positive patients with an SQ score
Downloaded from https://academic.oup.com/mmy/article/59/10/1041/6309311 by guest on 18 November 2021
sample had a negative SQ result. In contrast, the CryptoPS assay of ≥3 had a more than two-fold increase in mortality though the
incorrectly classified a higher proportion (5/33; 15%) of low- 95% CI spanned 1. In contrast to Jarvis et al, we did not find
titer samples as negative and also yielded 7 false-positive results. that the hazards of death increased with each step-wise increase
All 7 participants with false-positive CryptoPS results did not in SQ score. Again, this may be related to a smaller sample size.
receive antifungal treatment and none progressed to CM dur- Compared to testing serial sample dilutions to obtain LFA
ing 6 months of follow-up. In an evaluation of the same assay in titers, the SQ assay was a much less laborious method of obtain-
Botswana, a lower sensitivity (61%) but higher specificity (97%) ing a semi-quantitative CrAg result using a single test strip. SQ
was reported. In this study, 29 patients with false-positive Cryp- testing was easy to perform but reading the SQ test strip was
toPS results were followed up for 3 months and none developed more complex and the result interpretation card was needed to
CM.16 obtain an SQ score. For instance, for a CrAg-negative result, only
Since a blood CrAg titer cut-off of >160 had previously been a control line is positive with the LFA, whereas with the SQ as-
identified as a threshold for subclinical CM,3,13 we evaluated say, both the control and the T2 lines are positive. Moreover,
the accuracy of the two semi-quantitative assays in categoriz- grading of scores 1, 2 and 3 is determined by comparing the
ing plasma samples with a titer ≤160 and >160. All samples but intensity of the T1 and T2 bands. Through an inter-laboratory
one with an SQ score of 160. However, a score of 3 for the LFA in the national CrAg screening program and expect
did not clearly distinguish between these two titer categories. Al- that the complexity of reading the SQ test strips would increase
though a strong-positive CryptoPS result identified 76% of sam- the proportion of erroneous readings. Using automated readers
ples with a CrAg titer of >160, 18% of samples with a titer of to read the SQ test strips could be considered to prevent such
≤160 also had strong-positive results. In their evaluation, Ten- errors. Automated readers may also offer an advantage of inter-
forde et al. also reported a single LFA-negative plasma sample facing CrAg results to the laboratory information system, and
with a strong-positive CryptoPS result.16 therefore reduce transcription errors. In contrast, the CryptoPS
We went on to investigate the relationship between plasma cassette design provided a simple method of semi-quantitative
semi-quantitative assay results and subclinical CM. Semi- CrAg testing without using tubes. Results were available within
quantitative CrAg assays performed on blood are not a substi- 10 min and interpretation was very simple.
tute for lumbar puncture which is universally recommended for The strengths of this study included a prospective cohort de-
all patients with a new diagnosis of antigenemia. However, such sign and enrolment of consecutive eligible CrAg-positive indi-
assays could be used to refine the pre-test probability of subclin- viduals. Patients with asymptomatic antigenemia were enrolled
ical meningitis, especially at the primary healthcare level where after excluding those with clear symptoms and signs of CM and
patients need to be referred to hospital for a lumbar puncture or a relatively large proportion of patients (25%) had a baseline
in settings where a high proportion of patients decline lumbar lumbar puncture. The main limitation was a relatively small sam-
puncture. A score of ≥4 was highly specific for concurrent CM, ple size. In addition, at the time that the cohort study was con-
though half of the cases in our study were missed at this thresh- ducted, the South African guideline recommended that lumbar
old. A lower threshold (score ≥3) included all cases of CM and puncture should be considered for patients with cryptococcal
would thus be a more clinically useful risk prediction cut-off, antigenemia if this procedure was available. Ten of 60 CrAg-
despite also including 18/40 (45%) of cases without subclinical positive patients (17%) did not have a lumbar puncture. When
CM. Based on a sample of 189 screened patients, approximately we compared age, sex, CD4 count and proportion with a mild,
one third of whom had lumbar punctures, the aforementioned non-persistent headache among those who had a lumbar punc-
Botswana study reported a strong association between plasma ture versus those who did not, we found no differences. We also
SQ score and central nervous system involvement at baseline tested stored rather than fresh plasma. To determine if freezingBlasich et al. 1047
and thawing of plasma had an effect on SQ scores, fresh plasma Declaration of interest
samples that were tested using the SQ assay were stored in a No conflict of interest is declared.
−70°C freezer for >6 months. The samples were re-tested after
6 months and fresh and frozen-thawed plasma SQ results were
References
compared. There was excellent result concordance between fresh
1. Rajasingham R, Smith RM, Park BJ et al. Global burden of disease of HIV-
plasma SQ scores and frozen-thawed SQ scores (unpublished associated cryptococcal meningitis: An updated analysis. Lancet Infect Dis. 2017;
data, NICD). 17: 873–881.
2. Boulware DR, Rolfes MA, Rajasingham R et al. Multisite validation of crypto-
coccal antigen lateral flow assay and quantification by laser thermal contrast.
Conclusion Emerg Infect Dis. 2014; 20: 45–53.
3. Rajasingham R, Wake RM, Beyene T, Katende A, Letang E, Boulware DR. Cryp-
We found that two semi-quantitative assays offered a sim- tococcal meningitis diagnostics and screening in the era of point-of-care labora-
ple rapid means of estimating plasma CrAg concentrations. tory testing. J Clin Microbiol. 2019; 57: e01238–18.
Downloaded from https://academic.oup.com/mmy/article/59/10/1041/6309311 by guest on 18 November 2021
While not a substitute for lumbar puncture, using these semi- 4. Govender NP, Glencross DK. National coverage of reflex cryptococcal antigen
screening: a milestone achievement in the care of persons with advanced HIV
quantitative assays for risk stratification could be applied to pa-
disease. S Afr Med J. 2018; 108: 534–535.
tients with antigenemia for whom lumbar puncture is not im- 5. Longley N, Jarvis JN, Meintjes G et al. Cryptococcal antigen screening in patients
mediately available, those who decline a lumbar puncture, even initiating ART in South Africa: a prospective cohort study. Clin Infect Dis. 2016;
62: 581–587.
after careful counselling and those in whom lumbar puncture is
6. Govender NP, Meintjes G, Mangena P et al. Southern African HIV Clinicians
contraindicated. The association between the semi-quantitative Society guideline for the prevention, diagnosis and management of cryptococcal
assay results and mortality was not clear in our study. These as- disease among HIV-infected persons: 2019 update. Southern Afr J HIV Med.
says should not be implemented in routine screening programs 2019; 20: 1–16.
7. World Health Organization. Guidelines for the diagnosis, prevention, and man-
until more prospective data have accumulated from diagnostic agement of cryptococcal disease in HIV-infected adults, adolescents and children,
intervention studies. March 2018: Supplement to the 2016 consolidated guidelines of the use of an-
tiretroviral drugs for treating and preventing HIV infection. Available at: https:
//www.who.int/hiv/pub/guidelines/cryptococcal-disease/en/ (Accessed 28 May
Acknowledgements 2021).
The authors thank Immy and Biosynex for providing CrAg assays for re- 8. Mfinanga S, Chanda D, Kivuyo SL et al. Cryptococcal meningitis screening and
community-based early adherence support in people with advanced HIV infec-
search purposes. Data collection for the original cohort study was by: Neo
tion starting antiretroviral therapy in Tanzania and Zambia: An open-label, ran-
Legare, Sr Matshediso Mkhwenezi and Siphiwe Kutta. The authors thank
domised controlled trial. Lancet. 2015; 385: 2173–2182.
S. Hector for his expert advice and input throughout this project and Nqo-
9. Wake RM, Govender NP, Omar T et al. Cryptococcal-related mortality despite
bile Ngoma for assistance with data cleaning and analysis. fluconazole preemptive treatment in a cryptococcal antigen screen-and-treat pro-
gram. Clin Infect Dis. 2020; 70: 1683–1690.
10. Single Dose Liposomal Amphotericin for Asymptomatic Cryptococcal Antigen-
Author contributions emia (ACACIA). Available at: https://clinicaltrials.gov/ct2/show/NCT03945448
• Conceptualization: R.W., N.P.G., N.P.B. (Accessed 28 May 2021).
• Laboratory testing: N.P.B., I.R. 11. Treatment of cryptococcal antigen-positive patients identified through screening
• Student supervision: N.P.G., Y.P. using fluconazole plus flucytosine vs fluconazole alone. Available at: https://doi.
org/10.1186/ISRCTN30579828 (Accessed 28 May 2021).
• Data analysis and interpretation: N.P.B., R.W., N.P.G.
12. Thakur KT, Mateyo K, Hachaambwa L et al. Lumbar puncture refusal in sub-
• Drafting and revising manuscript: N.P.B., N.P.G.
Saharan Africa: a call for further understanding and intervention. Neurology.
• Manuscript review: All authors
2015; 84: 1988–1990.
13. Wake RM, Britz E, Sriruttan C et al. High cryptococcal antigen titers in blood
are predictive of subclinical cryptococcal meningitis among human immunodefi-
Funding ciency virus-infected patients. Clin Infect Dis. 2018; 66: 686–692.
R.W. received support from the National Institute for Health Research 14. Jarvis JN, Tenforde MW, Lechiile K et al. Evaluation of a novel semi-quantitative
(ACF-2015-16-003); the St George’s Hospital Research Charity; Sir cryptococcal antigen lateral flow assay in patients with advanced HIV disease. J
Ratanji Dalal Research Scholarship and the Meningitis Research Foun- Clin Microbiol. 2020; 58: e00441–20.
dation (1604.0). N.P.B., I.R. and N.P.G. were partly supported by the 15. Skipper C, Tadeo K, Martyn E et al. Evaluation of serum cryptococcal antigen
testing using two novel semiquantitative lateral flow assays in persons with cryp-
National Institute of Allergy and Infectious Diseases of the National Insti-
tococcal antigenemia. J Clin Microbiol. 2020; 58.
tutes of Health under Award Number R01AI118511. The content is solely
16. Tenforde MW, Boyer-Chammard T, Muthoga C et al. Diagnostic accuracy of the
the responsibility of the authors and does not necessarily represent the of-
Biosynex CryptoPS cryptococcal antigen semi-quantitative lateral flow assay in
ficial views of the National Institutes of Health. patients with advanced HIV disease. J Clin Microbiol. 2020; 59: e02307–20.You can also read