Original Article Improve cognitive impairment using mefenamic acid non-steroidal anti-inflammatory therapy: additional beneficial effect found in ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Am J Transl Res 2021;13(5):4535-4543
www.ajtr.org /ISSN:1943-8141/AJTR0126390
Original Article
Improve cognitive impairment using mefenamic acid
non-steroidal anti-inflammatory therapy: additional
beneficial effect found in a controlled clinical
trial for prostate cancer therapy
Valery Melnikov1, Daniel Tiburcio-Jimenez1, Martha A Mendoza‑Hernandez1, Josuel Delgado-Enciso3, Luis
De-Leon-Zaragoza2, Jose Guzman-Esquivel4, Iram P Rodriguez‑Sanchez5, Margarita L Martinez-Fierro6,
Agustin Lara-Esqueda2, Osiris G Delgado-Enciso1,3, Ivan Jacinto-Cortes2, Sergio A Zaizar-Fregoso1, Brenda A
Paz-Michel1, Efren Murillo-Zamora7, Ivan Delgado-Enciso1,2, Hector R Galvan-Salazar2,4
1
Department of Molecular Medicine, School of Medicine, University of Colima, Colima 28040, Mexico;
2
Department of Research, Cancerology State Institute, Colima State Health Services, Colima, Mexico;
3
Department of Research, Foundation for Cancer Ethics, Education and Research of The Cancerology State
Institute, Colima, Mexico; 4Department of Research, General Hospital of Zone No. 1 IMSS, Villa de Alvarez, Colima,
Mexico; 5Molecular and Structural Physiology Laboratory, School of Biological Sciences, Autonomous University of
Nuevo Leon, Monterrey, Nuevo Leon, Mexico; 6Molecular Medicine Laboratory, Academic Unit of Human Medicine
and Health Sciences, Autonomous University of Zacatecas, Zacatecas, Mexico; 7Department of Epidemiology,
Family Medicine Unit No. 19, IMSS, Colima, Mexico
Received November 16, 2020; Accepted March 20, 2021; Epub May 15, 2021; Published May 30, 2021
Abstract: Inflammation is an essential component of prostate cancer (PCa), and mefenamic acid has been reported
to decrease its biochemical progression. The current standard therapy for PCa is androgen deprivation therapy
(ADT), which has side effects such as cognitive dysfunction, risk of Alzheimer’s disease, and dementia. Published
results of in vitro tests and animal models studies have shown that mefenamic acid could be used as a neuropro-
tector. Objective: Examine the therapeutic potential of mefenamic acid in cognitive impairment used in a controlled
clinical trial. Clinical trial phase II was conducted on patients undergoing ADT for PCa. Two groups of 14 patients
were included. One was treated with a placebo, while the other received mefenamic acid 500 mg PO every 12hrs
for six months. The outcome was evaluated through the Mini-Mental State Examination (MMSE) score at six months.
At the beginning of the study, both groups had similar MMSE scores (mefenamic acid vs. placebo: 26.0±2.5 vs.
27.0±2.6, P=0.282). The mefenamic acid group improved its MMSE score after six months compared with the
placebo group (27.7±1.8 vs. 25.5±4.2, P=0.037). Treatment with mefenamic acid significantly increases the prob-
ability of maintained or raised cognitive function compared to placebo (92% vs. 42.9%, RR=2.2, 95% CI: 1.16-4.03,
NNT=2.0, 95% CI: 1.26-4.81, P=0.014). Furthermore, 42.9% of the placebo group patients had relevant cognitive
decline (a 2-point decrease in the MMSE score), while in patients treated with mefenamic acid, cognitive impair-
ment was not present. This study is the first conducted on humans that suggests that mefenamic acid protects
against cognitive decline.
Keywords: Alzheimer’s disease, mefenamic acid, cognitive impairment, non-steroidal anti-inflammatory drugs
Introduction Almost half of those patients will receive andro-
gen deprivation therapy (ADT) to reduce andro-
Cancer is becoming a leading cause of mortali- gens to castration levels which delays tumor
ty, and prostate cancer (PCa) is the most preva- growth while improves survival [2]. ADT has
lent non-dermatologic cancer and the second been used in metastatic disease because it
cause of cancer death in males [1]. Its inci- improves or prevents symptomatology while
dence continues to rise due to the progressive achieving control for 18-24 months before tran-
increase in life expectancy in the population sitioning into a castration-resistant disease
[2]. [2]. Nevertheless, ADT’s side effects, includingMefenamate improves cognitive impairment in prostate cancer patients
deterioration of musculoskeletal health, incre- with ADT, an observational study has estimated
ased cardiometabolic risk, cognitive dysfunc- that the use of statins or aspirin generates a
tion, dementia, and even Alzheimer’s disease, lower risk of cognitive dysfunction [7].
have been reported [3-5].
Neurodegenerative diseases such as Alzhe-
Patients with PCa undergoing treatment with imer’s disease or Parkinson’s disease have an
ADT present an accelerated cognitive deterio- inflammatory component, which can be ob-
ration concerning that expected with aging [3]. served in the latter’s amyloid plaques. Such a
Cognitive impairment is a determinant indepen- finding led to the assumption that anti-inflam-
dently associated with functional decline (the matory treatment with NSAIDs delays disease
limitation of daily living activities) in older per- progression [12]. Even more so, NSAIDs have
sons with cancer [6]. Its control is relevant been found to protect against the cognitive
to maintaining an adequate quality of life. decline that happens naturally with aging [11,
Therefore, it is crucial to search for new thera- 13] while they have also been presumed to
pies that aid in detaining said cognitive de- decrease the incidence of Alzheimer’s disease
terioration. [14, 15], but that is still a subject of debate
[16].
Publish literature has linked testosterone levels
with cognitive functions such as working, talk- Studies in animals with Alzheimer’s disease
ing, and focus, leading to the hypothesis that have shown that mefenamic acid, an NSAID,
ADT affects cognitive function [7]. A Korean has improved cognitive impairment and even
study with PCa patients (n=236,391) has con- reverse memory loss and brain inflammation
firmed the association between ADT and accel- [12, 17]. It has even protected against alcohol-
erated cognitive dysfunction, while the use of induced cognitive impairment [18].
statins or antiplatelets (such as aspirin) de-
Distinct mechanisms of neuroprotection and
creased the risk for cognitive dysfunction [7].
cognitive function improvement have been pro-
However, information against the relationship
posed for mefenamic acid. It targets the NL-
between anticoagulants, antiplatelets, and st-
RP3 inflammasome pathway [17], decreasing
atins with dementia or Alzheimer’s disease in
the free radical production, nitric oxide (NO),
patients with PCa has also been published [7,
and decreases the release of cytochrome C
8].
[18]. Besides, mefenamic acid has been shown
Given the conflicting results, the subject re- to up-regulate the anti-apoptotic protein expr-
mains a controversial one. Preclinical studies ession, Bcl-XL [18], and scavenge radical nitric
have reported decreased inflammation and oxi- oxide in a dose-dependent manner in vitro and
dative stress with aspirin treatment in the cen- reduce NO donor-induced death in the B 65
tral nervous system [9]. However, once again, neuroblastoma cells [19].
the controversy persists since there is also evi- Preclinical trials have shown that mefenamic
dence that low-dose aspirin does not improve acid can be used as a neuroprotector that
in any manner cognitive test scores or prevent attenuates cognitive impairment [12, 18]. How-
cognitive dysfunction [10]. The different doses ever, those findings have not been analyzed in
of non-steroidal anti-inflammatory drugs (NS- humans. One study reported that mefenamic
AIDs) utilized in the preclinical or clinical trials acid therapy decreased biochemical progres-
could cause the variability of the effects sion in PCa [20]. In the present study, we exam-
reported. ine the therapeutic potential of mefenamic acid
in cognitive impairment in PCa patients with
Observational study results have mainly shown
ADT receiving this anti-inflammatory drug as
that statin or NSAIDs use was associated with
part of a clinical trial against cancer.
a lower risk for dementia. A review of clinical
trials revealed the low-to-insufficient quality of Patients and methods
evidence that antihypertensive treatment,
NSAIDs, and statins do not alter the risk for Study design
dementia. There is no evidence on aspirin, dia-
betes, or dementia medications on incident We conducted a prospective, double-blind pha-
dementia or mild cognitive impairment (MCI) se II clinical trial with 2-arms in parallel with
[11]. Specifically, in patients with PCa treated randomized groups. The study was conducted
4536 Am J Transl Res 2021;13(5):4535-4543Mefenamate improves cognitive impairment in prostate cancer patients
according to the “CONSORT statement” guide- was attributable to the administration of the
lines for clinical trials. The main objective of the mefenamic acid, or patients who voluntarily
project was to evaluate the efficacy of mefe- decided to leave the study. The participants
namic acid in preventing cancer progression. were recruited from the “General Hospital in
However, in this report, we only analyzed the Zone No1 of the Mexican Social Security
effects on cognitive impairment. Institute (IMSS)” and the “Cancerology State
Institute of the health services of the State of
The National Scientific Commission (Mexican Colima” (Mexico).
Social Security Institute; Chairperson Name: Dr.
Fabio Salamanca-Gomez) approved the pres- Intervention
ent study (protocol number R-2018-785-058;
June 12, 2018). All patients signed the informed The 6-month intervention was performed in
consent form, and their anonymity was guaran- patients with ADT divided into two arms. One
teed. All procedures performed were under the arm with mefenamic acid, and the other arm
Declaration of Helsinki. The clinical trial was with placebo. Androgen deprivation therapy
registered as MEFEPROST: RPCEC00000248 included administering oral antiandrogens (flu-
in the “Cuban Public Registry of Clinical Trials tamide and bicalutamide), gonadotropin-re-
(RPCEC) Database”. The RPCEC trial registra- leasing hormone agonists (leuprolide and gos-
tion data set is part of the International Platform erelin), or bilateral orchiectomy. The treatment
Registry data set established by the World group took mefenamic acid (500 mg) every 12
Health Organization (WHO). h for six months. The other group took a place-
bo every 12 h for the same amount of time. The
Patients
pills were recommended to be taken with milk
Inclusion criteria: histologic diagnosis of PCa, or with meals to reduce gastrointestinal ad-
metastatic cancer, ADT carried out for six verse events. All patients took one omeprazole
months or longer before recruitment, ADT con- 20 mg tablet daily during the study. The treating
sidered by the treating oncologist to be feasi- physician was blinded to the treatment groups
ble and appropriate in the patient during the and could add any treatment they considered
6-month follow-up period, an ECOG functional necessary (usual medical care), including tax-
status of 0 to 2, and patients with no history of ane chemotherapy [22] or palliative radiothera-
liver or kidney disease (creatinine clearance py [21].
had to be greater than 60 milliliters/minute).
The following exclusion criteria were used: the Outcome measures and follow-up
presence of another primary cancer, uncon-
trolled arterial hypertension or diabetes, leuko- The project’s primary endpoint was to deter-
cyte count of less than 3,000 per microliter or mine the variations in the patients’ serum PSA
platelet count of less than 100,000 per microli- levels at six months. This result was previous-
ter, leukocyte count over 10,000 per microliter, ly published [20]. This report analyzes the
or showing data of systemic infection, blood Mini-Mental State Examination (MMSE) change
hemoglobin level below 9 g/deciliter, alcohol or score at month six as the primary endpoint. The
drug addiction, acid peptic diseases, ulcerative total score is calculated by adding the points
colitis or Crohn’s disease, chronic heart failure, for each item together (the total score ranging
diagnosis of ischemic heart disease, autoim- from 0 to 30 points), with a higher score indi-
mune or neurodegenerative diseases, depres- cating better cognitive status. In the present
sion, and other pathologies decided upon at study, the previously validated Spanish version
the discretion of the investigator. Elimination of the MMSE was employed [23]. Studies have
criteria: patients in whom the treating physician reported an annual cognitive decline at a mean
suspended the mefenamic acid, regardless of of 1.5 points on the MMSE in the first year and
the cause, for more than two weeks, patients 2.5 points after the second year in patients
with severe toxicity (grade 3 or higher) accord- with Alzheimer’s disease [24]. Our patients
ing to the “common terminology criteria for were classified as having “relevant cognitive
adverse events (CTCAE) version 4.0” (US De- decline” based on MMSE score changes, with
partment of Health and Human Services), that a decrease of two or more points after six
4537 Am J Transl Res 2021;13(5):4535-4543Mefenamate improves cognitive impairment in prostate cancer patients
Statistical analysis
Data were presented as mean
± standard error or standard
deviation or percentages. For
inferential statistics, the eq-
uality of variances was con-
firmed by the Levene test, and
the Kolmogorov-Smirnov test
first determined the normal
distribution of the data. Cate-
gorical values were compared
using Fisher’s exact test or
the Chi-square test of the like-
lihood ratio. The Student’s t-
test was used to compare the
numerical variables (with nor-
mal distribution) of the two
groups (mefenamic acid and
placebo). The number needed
to treat (NNT), the relative ri-
sk (RR), and 95% confidence
interval were calculated to
determine the probability of
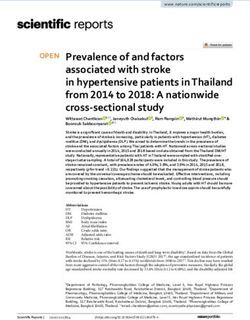
Figure 1. Consort 2010 flow diagram showing the number of patients
screened, included, eliminated, and analyzed in the study.
not having relevant cognitive
decline (a decrease of 2 or
more points on the MMSE),
months. Adverse events related to NSAIDs’ comparing the mefenamic group vs. the pla-
chronic ingestion were evaluated monthly in all cebo group. The statistical analysis was per-
patients through a complete blood count, bio- formed using the SPSS software, version 20
chemical kidney and liver function tests, and a (IBM Corp., Armonk, NY, USA), except for the
clinical interview by the physicians conducting RR and NNT, which were calculated using the
the research. MedCalc v17.7.2 software (MedCalc Software
bvba, Ostend, Belgium). Sample size and the
Blinding posthoc power analysis were calculated using
the ClinCalc.com online software (ClinCalc LLC,
The researchers who evaluated the effective- Indiana, USA). A one-sided PMefenamate improves cognitive impairment in prostate cancer patients
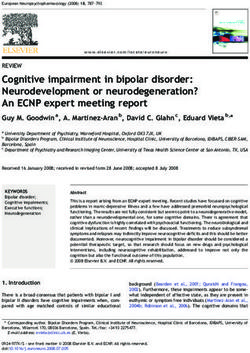
Table 1. Distribution of the main clinical characteristics of the study P=0.037). The patients tre-
subjects. Values are presented numerically (%) or mean ± standard ated with mefenamic acid
deviation raised their MMSE scores
Group (before and after compari-
Clinical characteristic P-value son: 26.0±2.5 vs. 27.7±1.8,
Mefenamic Placebo
P=0.002), whereas the pa-
Age (yrs) 70.8±8.1 69.3±6.5 0.591¥
tients that received place-
Hypertension 50% 42.9% 0.576&
bo tended to lower their
Diabetes 14.2% 14.2% 0.542& scores (27.0±2.6 vs. 25.5±
PVD 28.5% 28.5% 0.617& 4.2, P=0.079). Taking the
Hyperlipidemia 28.5% 28.5% 0.500& initial MMSE value as
Baseline Hemoglobin* 12.6±1.4 13.0±1.0 0.455¥ 100% for each patient, the
Baseline Glucose** 114.4±35.7 100.7±19.9 0.223 ¥ treatment with mefenamic
Final Hemoglobin* 11.4±2.1 12.1±1.6 0.436 ¥ acid produced a mean in-
Final Glucose** 134.7±70.9 111.9±39.9 0.365 ¥ crease of 7.4±8.2% in the
MMSE score, and the tre-
Cancer clinical stage 0.437#
atment with placebo pro-
IIC 14.2% 7.1%
duced a mean decrease
IIIA 14.2% 0% of 5.4±15.7% (107.4 vs.
IIIB 42.9% 42.9% 94.6%, P=0.005). A total
IIIC 0% 7.1% of 92.9% of the patients
IVA 28.5% 42.9% treated with mefenamic ac-
Gleason score 6.2±2.0 6.6±0.8 0.513¥ id maintained or raised th-
Treatments before and during the study eir MMSE score at six mon-
Statins 14.2% 14.2% 0.674 & ths, whereas only 42.9% of
Antihypertensive drugs 50.0% 42.9% 0.576 & the placebo group did the
same (P=0.014, see Table
Antidiabetic drugs 14.2% 21.4% 0.383&
2). It is essential to men-
Antiplatelet drugs 7.1% 7.1% 0.326&
tion that eight patients
Anticoagulant drugs 7.1% 7.1% 0.741& (57.1%) treated with mefe-
Other NSAIDs 0.326& namic acid raised their
Previous cancer treatment MMSE score by 2 points,
Radical prostatectomy 28.5% 28.5% 0.450& compared with only two
Radiotherapy 14.2% 28.5% 0.542& patients in the placebo gr-
Chemotherapy 7.1% 0.0% 0.483& oup (14.3%) (P=0.045). In
Other NSAIDs 7.1% 21.4% 0.326 & contrast, 42.9% of patients
Days with ADT 446±375 499±832 0.832 ¥ treated with placebo had
relevant cognitive impair-
Cancer treatment during the study
ment (a 2-point decrease
Radiotherapy 0.0% 14.2% 0.527&
in MMSE score at six mon-
Chemotherapy 28.5% 7.1% 0.143& ths), while in patients treat-
PVD: Peripheral vascular disease; ADT: androgen deprivation therapy; *g/dL; **mg/dL; ed with mefenamic acid,
¥
Student’s t test; &Fisher’s exact test; #Likelihood ratio Chi-square test.
cognitive impairment was
not present (P=0.071). Al-
1). The clinical characteristics of the patients so, the number needed to treat (NNT) with mef-
that completed the study are shown in Table 1. enamic acid to prevent a patient with PCa
undergoing ADT from presenting with relevant
Based on the MMSE score, there were no dif- cognitive decline was 2.5 (see Table 2).
ferences between the two groups at the begin-
ning of the study (mefenamic acid vs. placebo Regarding the adverse effects possibly relat-
group: 26.0±2.5 vs. 27.0±2.6, P=0.282), but ed to the experimental treatment (mefenamic
at the end of the study, the mefenamic acid acid), 3 (23.0%) patients presented grade 1 or
group had a significantly higher MMSE score 2 gastritis during the follow-up, but temporary
than the placebo group (27.7±1.8 vs. 25.5±4.2, suspension of the mefenamic acid (2 weeks)
4539 Am J Transl Res 2021;13(5):4535-4543Mefenamate improves cognitive impairment in prostate cancer patients
Table 2. Relevant changes in the MMSE at 6 months of follow-up and its association with mefenamic
acid consumption
Mefenamic group Placebo group
Relevant changes RR (CI 95%) NNT (CI 95%) P
N=14 N=14
Patients who maintained or raised their MMSE score 13 (92.9%) 6 (42.9%) 2.2 (1.16-4.03) 2.0 (1.26-4.81) 0.014
Patients who raised their MMSE score by 2 points 8 (57.1%) 2 (14.2%) 4.0 (1.02-15.59) 2.3 (1.34-9.00) 0.045
Patients who reduced their MMSE score by 2 points* 0 (0%) 6 (42.9%) 0.07 (0.00-1.24) 2.5 (1.50-7.50) 0.071
RR: relative risk; NNT: number needed to treat; CI 95%: 95% confidence interval; MMSE: Mini-Mental State Examination. *Patients who had a relevant cognitive decline.
N: sample number.
was required in only one of those patients. However, no previous study on humans has
Symptomatology ceased after insisting that the evaluated its protective or therapeutic effect
patients take the medication with meals. No on the loss of cognitive functions. The present
pathologic alterations were found in the liver study demonstrated that mefenamic acid pre-
function and kidney tests or the complete blood vented cognitive decline in patients with PCa
count. No patient required definitive suspen- undergoing ADT and relevantly raised the cogni-
sion of the experimental treatment due to tive function scores on the MMSE by 2 points in
adverse effects. nearly half the patients, concurring with the
results of preclinical trials on the same theme
Discussion [12, 17]. Nevertheless, it should be pointed out
that the subjects of our study did not present
Treatment with the anti-inflammatory drug mef- with dementia at the beginning of the analysis,
enamic acid significantly increases the proba- albeit they did present with two factors that
bility of maintained or raised cognitive function have significantly been associated with cogni-
in patients with PCa undergoing ADT. After 6 tive decline, which are a mean age close to 70
months of treatment, the mefenamic acid gr- years and undergoing continuous treatment
oup had a significantly higher MMSE absolute with antiandrogens [7].
score than the placebo group. After 6 months,
patients’ MMSE scores that received placebo Mefenamic acid is often used to treat dysmen-
decreased by 5.4%, whereas the patients treat- orrhea and heavy menstrual bleeding, adminis-
ed with mefenamic acid increased by 7.4%. tering an oral dose of 1.5 g per day for 3 to 5
days [28]. The exact dose for prolonged periods
Even though that level of change appears to be
was proposed decades ago [29]. Nevertheless,
minor, it is similar to the change in patients in
its chronic use is not customary. There are
the early stages of Alzheimer’s disease at one
other medications with a similar analgesic or
year, which is a decrease of a mean 1.5 to 2
anti-inflammatory effect and fewer adverse
points in the MMSE score [24]. The present
effects. In particular, there is less risk for over-
study is the first conducted on humans that dose [30]. A dose of mefenamic acid (1 g PO
shows mefenamic acid’s effect on cognitive per day) lower than that recommended daily
function. was used in the present study, but it was ad-
ministered for a more extended time. There
Evidence suggests that fenamates can modu-
were no serious adverse events with that drug
late neuronal functioning by modifying ion ch-
regimen, but there were signs clinically consis-
annel activity, depending on the subunits form-
tent with mild gastritis. Therefore, taking the
ing the GABA receptor complex [25]. Other
medication with meals and receiving omepra-
fenamates (flufenamic acid and niflumic acid)
zole throughout the study was a prime neces-
also inhibit NMDA-activated currents recorded sity. It was decided not to administer the drug
from spinal neurons [26]. Flufenamic acid has for more than six months due to the risk of kid-
been shown to block non-selective calcium- ney damage [31], which did not occur during
activated cation channels in rat hippocampal the study.
CA1 neurons [27]. Those studies in vitro and
animal models have led to the postulation that It is essential to point out that the administra-
mefenamic acid is a neuroprotector or a poten- tion of mefenamic acid for six months in a group
tial therapeutic agent in Alzheimer’s disease. of patients with prostate cancer did not have
4540 Am J Transl Res 2021;13(5):4535-4543Mefenamate improves cognitive impairment in prostate cancer patients
the sole objective of stopping the cognitive References
impairment because perhaps this sole reason
does not ethically justify said prescription. The [1] Fenton JJ, Weyrich MS, Durbin S, Liu Y, Bang H
main objective of the clinical trial was to pre- and Melnikow J. Prostate-specific antigen-
based screening for prostate cancer: evidence
vent the progression of cancer [20]. The effect
report and systematic review for the US pre-
reported here was a finding, which exemplifies ventive services task force. JAMA 2018; 319:
the potential use of this NSAID against cogni- 1914.
tive impairment and could serve as the basis [2] McHugh DJ, Root JC, Nelson CJ and Morris MJ.
for future research. A limitation of the present Androgen-deprivation therapy, dementia, and
study was the small sample size and the dura- cognitive dysfunction in men with prostate
tion of the follow-up period. Further study cancer: how much smoke and how much fire?
should include many patients and a more ex- Cancer 2018; 124: 1326-1334.
tended follow-up period that strictly evaluates [3] Mundell NL, Daly RM, Macpherson H and
adverse effects. Fraser SF. Cognitive decline in prostate cancer
patients undergoing ADT: a potential role for
Conclusions exercise training. Endocr Relat Cancer 2017;
24: R145-R155.
[4] Nead KT, Gaskin G, Chester C, Swisher-
The present study is the first study carried out
McClure S, Dudley JT, Leeper NJ and Shah NH.
on humans, suggesting that mefenamic acid
Androgen deprivation therapy and future
protects against cognitive decline. Even though Alzheimer’s disease risk. JCO 2016; 34: 566-
this clinical trial was conducted on patients 571.
with prostate cancer undergoing androgen de- [5] Nead KT, Gaskin G, Chester C, Swisher-
privation therapy, mefenamic acid’s therapeu- McClure S, Dudley JT, Leeper NJ and Shah NH.
tic potential could include other diseases that Influence of age on androgen deprivation ther-
present with cognitive decline. Future studies apy-associated Alzheimer’s disease. Sci Rep
are needed to strengthen the results of the 2016; 6: 35695.
present analysis. [6] Galvin A, Helmer C, Coureau G, Amadeo B,
Rainfray M, Soubeyran P, Dartigues JF, Pérès
Acknowledgements K, Bellera C, Delva F and Mathoulin-Pélissier S.
Determinants of functional decline in older
The authors would like to thank postgraduate adults experiencing cancer (the INCAPAC
study). J Geriatr Oncol 2019; 10: 913-920.
students Carlos E. Barajas-Saucedo and Mario
[7] Tae BS, Jeon BJ, Shin SH, Choi H, Bae JH and
A. Gaytan-Hinojosa (Postgraduate program in Park JY. Correlation of androgen deprivation
medical sciences at the University of Colima, therapy with cognitive dysfunction in patients
Mexico) for excellent assistance in placing the with prostate cancer: a nationwide population-
clinical data in the different platforms for their based study using the national health insur-
analysis. The authors of this study was funded ance service database. Cancer Res Treat
by grant no. 272792, 2016-FOSISS-CONACYT 2019; 51: 593-602.
(author IDE). [8] Khosrow-Khavar F, Rej S, Yin H, Aprikian A and
Azoulay L. Androgen deprivation therapy and
Disclosure of conflict of interest the risk of dementia in patients with prostate
cancer. JCO 2017; 35: 201-207.
None. [9] Wang YP, Wu Y, Li LY, Zheng J, Liu RG, Zhou JP,
Yuan SY, Shang Y and Yao SL. Aspirin-triggered
Address correspondence to: Hector R Galvan- lipoxin A4 attenuates LPS-induced pro-inflam-
Salazar, Department of Research, Cancerology matory responses by inhibiting activation of
State Institute, Colima State Health Services, Ave. NF-κB and MAPKs in BV-2 microglial cells. J
Neuroinflammation 2011; 8: 95.
Liceo De Varones 401, Colonia la Esperanza, Colima
[10] Veronese N, Stubbs B, Maggi S, Thompson T,
28085, Mexico. E-mail: hector_rgs@hotmail.com;
Schofield P, Muller C, Tseng PT, Lin PY, Carvalho
Ivan Delgado-Enciso, Department of Molecular
AF and Solmi M. Low-dose aspirin use and cog-
Medicine, School of Medicine, University of Colima, nitive function in older age: a systematic re-
Ave. Universidad 333, Colonia las viboras, Colima view and meta-analysis. J Am Geriatr Soc
28040, Mexico. Tel: +52 312 3161099; Fax: +52 2017; 65: 1763-1768.
312 3161099; E-mail: ivan_delgado_enciso@ucol. [11] Fink HA, Jutkowitz E, McCarten JR, Hemmy LS,
mx Butler M, Davila H, Ratner E, Calvert C, Barclay
4541 Am J Transl Res 2021;13(5):4535-4543Mefenamate improves cognitive impairment in prostate cancer patients
TR, Brasure M, Nelson VA and Kane RL. Phar- Delgado-Enciso I. Decreased biochemical pro-
macologic interventions to prevent cognitive gression in patients with castration-resistant
decline, mild cognitive impairment, and clini- prostate cancer using a novel mefenamic acid
cal Alzheimer-type dementia: a systematic re- anti-inflammatory therapy: a randomized con-
view. Ann Intern Med 2018; 168: 39. trolled trial. Oncol Lett 2020; 19: 4151-4160.
[12] Joo Y, Kim HS, Woo RS, Park CH, Shin KY, Lee [21] Lutz S, Berk L, Chang E, Chow E, Hahn C,
JP, Chang KA, Kim S and Suh YH. Mefenamic Hoskin P, Howell D, Konski A, Kachnic L, Lo S,
acid shows neuroprotective effects and im- Sahgal A, Silverman L, von Gunten C, Mendel
proves cognitive impairment in in vitro and in E, Vassil A, Bruner DW and Hartsell W. Pallia-
vivo Alzheimer’s disease models. Mol Pharma- tive radiotherapy for bone metastases: an AS-
col 2006; 69: 76-84. TRO evidence-based guideline. Int J Radiat
[13] Kern S, Skoog I, Östling S, Kern J and Börjes- Oncol Biol Phys 2011; 79: 965-976.
son-Hanson A. Does low-dose acetylsalicylic [22] Jones R and Cornford P. EAU and NICE guide-
acid prevent cognitive decline in women with lines for the diagnosis and management of
high cardiovascular risk? A 5-year follow-up of prostate cancer. How wide is the channel? J
a non-demented population-based cohort of Clin Urol 2018; 11: 149-153.
Swedish elderly women. BMJ Open 2012; 2: [23] Mokri H, Ávila-Funes JA, Meillon C, Gutiérrez
e001288. Robledo LM and Amieva H. Normative data for
[14] Imbimbo BP, Solfrizzi V and Panza F. Are the mini-mental state examination, the free
NSAIDs useful to treat Alzheimer’s disease or and cued selective reminding test and the
mild cognitive impairment? Front Ag Neurosci isaacs set test for an older adult Mexican pop-
2010; 2: 19. ulation: the coyoacán cohort study. Clin Neuro-
[15] Broe GA, Grayson DA, Creasey HM, Waite LM, psychol 2013; 27: 1004-1018.
Casey BJ, Bennett HP, Brooks WS and Halliday [24] Ferrari C, Lombardi G, Polito C, Lucidi G, Bag-
GM. Anti-inflammatory drugs protect against noli S, Piaceri I, Nacmias B, Berti V, Rizzuto D,
Alzheimer disease at low doses. Arch Neurol Fratiglioni L and Sorbi S. Alzheimer’s disease
2000; 57: 1586-1591. progression: factors influencing cognitive de-
[16] Sanz-Blasco S, Calvo-Rodríguez M, Caballero cline. JAD 2017; 61: 785-791.
E, Garcia-Durillo M, Nunez L and Villalobos C. [25] Halliwell RF, Thomas P, Patten D, James CH,
Is it all said for NSAIDs in Alzheimer’s disease? Martinez-Torres A, Miledi R and Smart TG. Sub-
Role of mitochondrial calcium uptake. CAR unit-selective modulation of GABA A receptors
2018; 15: 504-510. by the non-steroidal anti-inflammatory agent,
[17] Daniels MJD, Rivers-Auty J, Schilling T, Spencer mefenamic acid: fenamate anti-inflammatory
NG, Watremez W, Fasolino V, Booth SJ, White agents and GABA A receptors. Eur J Neurosci
CS, Baldwin AG, Freeman S, Wong R, Latta C, 1999; 11: 2897-2905.
Yu S, Jackson J, Fischer N, Koziel V, Pillot T, Ba- [26] Lerma J and Martín del Río R. Chloride trans-
gnall J, Allan SM, Paszek P, Galea J, Harte MK, port blockers prevent N-methyl-D-aspartate
Eder C, Lawrence CB and Brough D. Fenamate receptor-channel complex activation. Mol
NSAIDs inhibit the NLRP3 inflammasome and Pharmacol 1992; 41: 217-222.
protect against Alzheimer’s disease in rodent [27] Partridge LD and Valenzuela CF. Block of hip-
models. Nat Commun 2016; 7: 12504. pocampal CAN channels by flufenamate. Brain
[18] Rajesh V, Mridhulmohan M, Jayaseelan S, Siv- Res 2000; 867: 143-148.
akumar P and Ganesan V. Mefenamic acid at- [28] de Mello NR, Baracat EC, Tomaz G, Bedone AJ,
tenuates chronic alcohol induced cognitive Camargos A, Barbosa IC, de Souza RN, Rumi
impairment in Zebrafish: possible role of cho- DO, Martinez Alcala FO, Velasco JA and Cortes
linergic pathway. Neurochem Res 2018; 43: RJ. Double-blind study to evaluate efficacy and
1392-1404. safety of meloxicam 7.5 mg and 15 mg versus
[19] Asanuma M, Nishibayashi-Asanuma S, Miyaza- mefenamic acid 1500 mg in the treatment of
ki I, Kohno M and Ogawa N. Neuroprotective primary dysmenorrhea: treatment of primary
effects of non-steroidal anti-inflammatory dysmenorrhea. Acta Obstet Gynecol Scand
drugs by direct scavenging of nitric oxide radi- 2004; 83: 667-673.
cals: Non-steroidal anti-inflammatory drugs on [29] Gligore V and Bolosiu HD. Mefenamic acid in
NO. J Neurochem 2001; 76: 1895-1904. the treatment of rheumatoid arthritis and re-
[20] Guzman-Esquivel J, Mendoza-Hernandez M, lated diseases. J Int Med Res 1974; 2: 153-
Tiburcio-Jimenez D, Avila-Zamora O, Delgado- 155.
Enciso J, De-Leon-Zaragoza L, Casarez-Price J, [30] Kamour A, Crichton S, Cooper G, Lupton DJ,
Rodriguez-Sanchez I, Martinez-Fierro M, Meza- Eddleston M, Vale JA, Thompson JP and Thom-
Robles C, Barocio-Acosta A, Baltazar-Rodriguez as SH. Central nervous system toxicity of mef-
L, Zaizar-Fregoso S, Plata-Florenzano J and enamic acid overdose compared with other
4542 Am J Transl Res 2021;13(5):4535-4543Mefenamate improves cognitive impairment in prostate cancer patients NSAIDs: an analysis of cases reported to the [31] Yaxley J and Litfin T. Non-steroidal anti-inflam- United Kingdom National poisons information matories and the development of analgesic service. Br J Clin Pharmacol 2017; 83: 855- nephropathy: a systematic review. Renal Fail- 862. ure 2016; 38: 1328-1334. 4543 Am J Transl Res 2021;13(5):4535-4543
You can also read