Oseltamivir pharmacokinetics in morbid obesity (OPTIMO trial)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
J Antimicrob Chemother 2011; 66: 2083 – 2091
doi:10.1093/jac/dkr257 Advance Access publication 23 June 2011
Oseltamivir pharmacokinetics in morbid obesity (OPTIMO trial)
L. M. Thorne-Humphrey1,2*†, K. B. Goralski1,3†, K. L. Slayter1,2,4,5, T. F. Hatchette2,4,6, B. L. Johnston2,4
and S. A. McNeil2,4,5,7 (The 2009 OPTIMO Study Group)
1
College of Pharmacy, Dalhousie University, Halifax, Nova Scotia, Canada B3H 4R2; 2Capital District Health Authority Halifax Infirmary,
Pharmacy Department, Halifax, Nova Scotia, Canada B3H 3A7; 3Department of Pharmacology, Dalhousie University, Halifax, Nova Scotia,
Canada B3H 4R2; 4Department of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada B3H 4R2; 5Canadian Centre for
Vaccinology, Halifax, Nova Scotia, Canada B3K 6R8; 6Department of Pathology, Dalhousie University, Halifax, Nova Scotia,
Canada B3H 4R2; 7IWK Health Centre, Halifax, Nova Scotia, Canada B3K 6R8
*Corresponding author. Tel: +1-902-488-6999; Fax: +1-902-473-3904; E-mail: lucas@dal.ca
†L. M. T.-H. and K. B. G. were entirely responsible for the data analysis and pharmacokinetic modelling. They wish to be acknowledged
as co-first authors as they have contributed equally to writing the manuscript.
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
Received 1 November 2010; returned 16 December 2010; revised 26 May 2011; accepted 29 May 2011
Background: Detailed pharmacokinetics to guide oseltamivir (Tamifluw) dosing in morbidly obese patients is
lacking.
Methods: The OPTIMO trial was a single-centre, non-randomized, open-label pharmacokinetic study of single-
dose and steady-state oral oseltamivir phosphate and its carboxylate metabolite in healthy, morbidly obese
[body mass index (BMI).40)] and healthy, non-obese (BMI, 30) subjects.
Results: In the morbidly obese versus control subjects, respectively, the single-dose median oseltamivir oral
clearance (CL/F) [840 (range 720– 1640) L/h versus 580 (470–1800) L/h] was higher, the area under the
curve from time zero to infinity (AUC0 – 1) [89 (46 –104) ng.h/mL versus 132 (42– 160) ng.h/mL] was lower
and the volume of distribution (V/F) [2320 (900 –8210) L versus 1670 (700 –7290) L] was unchanged. In the
morbidly obese versus control subjects, respectively, the single-dose median oseltamivir carboxylate CL/F
[22 (17 –40) L/h versus 23 (12 –33) L/h], AUC0 – 1 [3100 (1700 –4100) ng.h/mL versus 3000 (2100– 5900)
ng.h/mL] and V/F [200 (130– 370) L versus 260 (150–430) L] were similar. Similar results for oseltamivir and
oseltamivir carboxylate CL/F, AUC0 – 12 and V/F values were observed in the multiple-dose study.
Conclusions: With single and multiple dosing, the systemic exposure to oseltamivir is decreased but that of
oseltamivir carboxylate is largely unchanged. Based on these pharmacokinetic data, an oseltamivir dose
adjustment for body weight would not be needed in morbidly obese individuals.
Keywords: body mass index, obese, PK, body weight
Introduction morbid obesity (BMI .40) as a risk factor for increased morbidity
and mortality in severely ill patients.7 – 9 Obesity had not been
Oseltamivir (Tamifluw), an orally administered antiviral ester identified as a risk factor for excess morbidity and mortality
prodrug, is rapidly converted by hepatic esterases to an active during previous influenza seasons, and the mechanistic factors
metabolite, oseltamivir carboxylate, that blocks viral replication have not been fully elucidated. Several theories have been pro-
by inhibition of viral neuraminidase enzyme activity.1 Oseltamivir posed to explain the reported association between obesity and
is used for seasonal influenza treatment and outbreak preven- the poor outcomes with pH1N1 infection seen in hospitalized
tion, and has been employed for the treatment of pandemic patients.9 It is plausible that oseltamivir may be under-dosed
H1N1 influenza (pH1N1) since its emergence in the spring of in critically ill morbidly obese patients with influenza. Specifically,
2009.2,3 Despite sporadic case reports of resistance, pH1N1 is a reduction in the circulating drug concentration could arise
considered susceptible to oseltamivir and, thus, oseltamivir is a through an expanded volume of distribution (V) for lipid-soluble
first-line antiviral treatment for severely ill individuals and drugs (e.g. oseltamivir), which distribute into fat tissue, and, to
those with risk factors for poor outcomes.4 – 6 a lesser extent, water-soluble drugs (e.g. oseltamivir carboxy-
During the recent H1N1 influenza pandemic, several surveil- late), which distribute into lean tissue. Further, obesity may
lance reports identified obesity [body mass index (BMI).30] or increase or decrease drug clearance (CL), depending on the
# The Author 2011. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved.
For Permissions, please e-mail: journals.permissions@oup.com
2083Thorne-Humphrey et al.
specific pathways of elimination for the drug in question.10 – 13 safety of the participants and utility of the results. All participants were
Depending on the degree of changes in V and CL, respectively, required to sign a written informed consent form, and undergo a com-
adjustments in loading and maintenance doses may be required plete medical history and physical examination. Subjects were compen-
in order to initiate and maintain therapeutic drug levels during sated monetarily for their participation in the study.
multiple-dose therapy. Detailed pharmacokinetics information All study subjects were required to keep a diary to be reviewed by one
of the study investigators at each study visit. The subject’s diary included
to guide oseltamivir dosing for the morbidly obese patient is
a record of drug administration and all side effects experienced through-
lacking.5 The objectives of the OPTIMO study were to: (i) charac-
out the study. All study medication was accounted for and packaged in
terize the single-dose and steady-state pharmacokinetics of accordance with local and national standards.
oseltamivir and its active carboxylate metabolite in healthy, On the first day of the subject’s study participation, a 75 mg capsule
morbidly obese subjects (BMI .40) and non-obese controls of oseltamivir phosphate was administered by mouth after the subject
(BMI,30); and (ii) develop a dosing strategy for morbidly confirmed that he/she had consumed a meal either provided by study
obese patients if the disposition of oseltamivir was significantly staff or taken independently within the previous hour. Blood samples
different from that observed in non-obese patients. (7– 10 mL) were collected into EDTA tubes from a peripheral intravenous
catheter just prior to the first oseltamivir dose (0 h) and at 0.5, 1, 1.5, 2, 3,
4, 5, 6, 7, 8, 10, 12 and 24 h following the first dose. Plasma was separ-
Methods ated by centrifugation and immediately stored at 2208C until analysed.
Beginning on day 2, participants were instructed to take a single 75 mg
Clinical trial approval capsule of oseltamivir phosphate twice daily for 5 consecutive days. On
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
The OPTIMO trial was approved by institutional ethics review boards at day 7 (steady-state), subjects returned to the unit where they were admi-
the IWK Health Centre and Capital District Health Authority in Halifax, nistered a final 75 mg capsule of oseltamivir phosphate in the morning.
Nova Scotia. The study, which is in accordance with the declaration of Blood samples (7– 10 mL) were collected as above, just prior to adminis-
Helsinki, was registered with the Clinical Trials Registry (Clinicaltrials.gov tering the final oseltamivir dose (C12 trough concentration from dose 10)
identifier: NCT01002729) before enrolment began. and at 0.5, 1, 1.5, 2, 3, 4, 5, 6, 7, 8, 10, 12 and 24 h after the final dose.
The collected plasma samples were shipped on dry ice to PRA Inter-
national Bioanalytical Laboratory in the Netherlands. An established
Study design high-performance liquid chromatography– tandem mass spectrometric
OPTIMO was a single-centre, non-randomized, open-label pharmacoki- detection method was used to determine the concentrations of oselta-
netic study of single-dose and steady-state oral administration of oselta- mivir and its biologically active metabolite, oseltamivir carboxylate, in
mivir phosphate. The study was carried out at the Human Vaccine all samples.16,17 The lower limit of quantification (LLQ) was 1 ng/mL for
Challenge Unit, IWK Health Centre, Halifax, Nova Scotia, Canada. oseltamivir and 10 ng/mL for oseltamivir carboxylate. The performance
of the assay was satisfactory throughout the study. The interassay pre-
cision (coefficient of variation) of quality-control samples ranged
Study subjects between 4.8% and 6.7% for oseltamivir and between 8.4% and 13.5%
for oseltamivir carboxylate. There was no marked inaccuracy in the
Subjects were recruited through local poster advertisements and broad-
results from these quality-control samples [mean accuracy; 94.7%
cast communications to clinicians and local healthcare institutions. Par-
(n ¼18) to 102.5% (n ¼18) for oseltamivir and 94.1% (n¼14) to 97.7%
ticipants (male and female) were considered eligible for the study if
(n ¼14) for oseltamivir carboxylate].
they had a BMI of ,30 (non-obese) or .40 (morbidly obese) and were
aged 18–55 years. Subjects were ineligible if they had an allergy to osel-
tamivir, donated blood within 3 months before the subject’s date of first
drug administration, were anaemic, had an estimated glomerular fil- Pharmacokinetic analysis
tration rate ,60 mL/min, as calculated using the Cockcroft– Gault For each study subject, the maximum oseltamivir and oseltamivir carbox-
equation,14 or were taking any concomitant medications thought to ylate concentrations achieved after a single dose (Cmax) and at
interact with the pharmacokinetics of oseltamivir, such as probenecid.15 steady-state (Css max), the time to reach Cmax and Css max (Tmax), and
Ideal body weight (IBW) and obese dosing weight (ODW) were calculated the trough concentrations obtained 12 h after the initial (C12) and final
and used only to determine estimated glomerular filtration rates in the (C12 ss) oseltamivir phosphate doses were recorded directly from the
non-obese and morbidly obese arms to exclude subjects with compro- plasma drug concentration versus time datasets. For determination of
mised renal function. The following formula was used to determine an oseltamivir C12 or C12 ss, any of the t¼12 h samples that were below
ODW for use in the Cockcroft–Gault formula in morbidly obese subjects LLQ were assumed to be zero. The linear trapezoidal rule was used to cal-
[ODW¼ IBW +0.4(actual body weight 2IBW)]. Subjects were also culate the single-dose area under the curve from t¼0 to infinity (AUC0 – 1)
excluded if they had had any surgeries involving the gastrointestinal and the steady-state AUC0 – 12. For the AUC0 – 1 analysis, the levels of the
tract that had the potential to interfere with drug absorption, such as parent drug and metabolite were assumed to be zero at t¼0 and in any
gastrectomies and enterectomies, or were judged unable to consume samples that were below LLQ prior to the sampling time at which oselta-
the study mediation for any reason. Those with a laboratory abnormality mivir and oseltamivir carboxylate were first measurable above the LLQ.
detected on screening blood work were excluded if the abnormality was For all other samples in which oseltamivir or oseltamivir carboxylate
judged clinically significant by one of the study investigators. Those with a was below the LLQ, no assumptions were made regarding concen-
clinically significant cardiac conduction abnormality, influenza-like illness trations, and these samples were omitted from the single-dose and
in the previous 7 days of enrolment or, for female subjects, a positive steady-state AUC analyses. The oral clearance (CL/F) was determined
urine pregnancy test just prior to the first dose were also ineligible. by non-compartmental pharmacokinetic analysis using the relationship
CL/F¼Dose/AUC. The elimination rate constant (l) was determined by
least-squares linear regression of the terminal elimination phases of
Study procedures the semi-log10-transformed concentration versus time curves. The half-
Research personnel were responsible for an initial telephone interview of life of elimination (t12) was calculated using the equation t12 ¼0.693/l.
all potential subjects and coordination of their baseline tests to ensure The oral volume of distribution (V/F) was calculated from the relationship
2084OPTIMO trial JAC
V/F¼CL/(F×l). The observed accumulation of oseltamivir carboxylate at common in the morbidly obese group included acid reflux
steady-state was calculated as the ratio of Cmax steady-state/Cmax single (n¼ 4), muscle skeletal/joint pain (n¼ 3), hypertension (n¼ 2),
dose. The predicted steady-state to single-dose relative accumulation type 2 diabetes (n¼2), high cholesterol (n¼ 2), anxiety (n¼ 2),
(Rac) of oseltamivir carboxylate was calculated using the formula depression (n¼ 2) and asthma (n¼ 2). Additionally, three controls
Rac ¼(1/12elt), where l ¼the single-dose elimination rate constant and and one morbidly obese subject were taking contraceptive
t¼the dose interval (12 h). PK Solutions 2.0 (Summit Research Services,
agents at the time of the study.
Montrose, CO, USA) software was used for the non-compartmental
Two hundred and thirty-nine of a total 240 doses were
pharmacokinetic data analysis.
confirmed taken by the study participants. One patient in the
non-obese arm missed one dose of oseltamivir phosphate at
Statistical analysis the midpoint of the steady-state study and returned the
unused capsule to staff. During the study, the only medication-
All results are expressed as the median (range). The median values for
subject characteristics, and the median single-dose and steady-state
related adverse effects were nausea, vomiting, abdominal dis-
pharmacokinetic parameters for oseltamivir and oseltamivir carboxylate comfort and headache. One subject with previous history of
in the BMI, 30 versus BMI.40 subjects were compared using a migraine headaches experienced nausea and headache, which
non-parametric Mann–Whitney test. Linear regression analysis was was suspected by the patient and study staff as migraine in
performed to determine the dependence of CL/F and V/F on total nature, on the last day of drug administration. The patient was
body weight (TBW) or lean body weight (LBW), calculated from the given pain-relieving medication and the headache completely
formulae LBWmales ¼[9270×TBW (kg)]/[6680 +216×BMI (kg/m2)] and
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
resolved. One subject experienced sore joints and another
LBWfemales ¼[9270×TBW (kg)]/[8870+244×BMI (kg/m2)].18,19 For all reported fatigue, which both subjects felt to be unrelated to
statistical analyses, a P value ≤0.05 was considered significant. GraphPad the study medication due to their previous occurrence and
Prism (version 5.0b) software was used for all graphical and statistical benign nature.
analyses. Oseltamivir and oseltamivir carboxylate were below the LLQ in
99/276 and 42/276 (single-dose study), and 38/276 and 0/276
Results (multiple-dose study) measured plasma samples, respectively.
This included all t¼ 0 samples in the single-dose study. The
Patient characteristics, oseltamivir dosing, safety, majority of the remaining samples in which oseltamivir was
adverse effects and concomitant medications below the LLQ coincided with the latter portions of the dosing
interval (i.e. after 10 h), reflecting its rapid elimination. The
Ten subjects for each group were recruited to participate in the
majority of the remaining samples in which oseltamivir carboxy-
study. All subjects met the eligibility requirements and com-
late was below the LLQ coincided with t¼0.5 h, which reflects
pleted the study. No subjects were excluded according to our
the lag time for absorption and conversion of the parent drug
predetermined exclusion criteria. The baseline characteristics of
to the active metabolite. Four of 280 scheduled blood draws
the morbidly obese and non-obese controls are shown in
were missed in each study phase; these misses resulted from
Table 1. Each group had two males and eight females. The
temporary loss of patient intravenous access, occurred in
median BMI and TBW were approximately 2-fold higher in the
isolation and were distributed in both groups.
obese group compared with the control group. Both groups
had a similar median age, serum creatinine and creatinine clear-
ance (CLCR). The obese group was taking significantly more medi-
cations and had more co-morbidities than the non-obese group. Oseltamivir and oseltamivir carboxylate
At the time of study, the pre-existing medicated conditions most pharmacokinetics in morbidly obese versus
common in the control subjects were headache (n¼ 2), anxiety non-obese subjects
(n¼ 2) and allergies (n¼ 3). The medicated conditions most
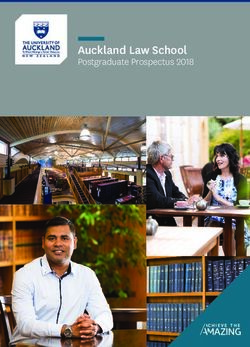
The individual and mean single-dose and steady-state oseltami-
vir and oseltamivir carboxylate concentration versus time profiles
Table 1. Baseline subject characteristics are shown in Figure 1. The plasma-concentration time curves
generally illustrate a lower systemic oseltamivir exposure in the
Morbidly obese Non-obese morbidly obese group compared with the non-obese group
Characteristic (BMI.40) (BMI, 30) P after the initial dose of oseltamivir phosphate (Figure 1a–c)
and at steady-state (Figure 1d– f). This is reflected by the phar-
Age (years)a 39 (31 – 46) 29 (23 –52) 0.075 macokinetic analysis (Tables 2 and 3), which found that the
BMI (kg/m2)a 46.0 (40.2– 82.0) 24.0 (21.0–29.0)Thorne-Humphrey et al.
(a) 75 mg single dose, BMI < 30 (b) 75 mg single dose, BMI > 40 (c) 75 mg single dose
200 200 150
BMI < 30
Oseltamivir (ng/mL)
Oseltamivir (ng/mL)
Oseltamivir (ng/mL)
125
150 150 BMI > 40
100
100 100 75
50
50 50
25
0 0 0
0 3 6 9 12 0 3 6 9 12 0 3 6 9 12
Time (h) Time (h) Time (h)
(d) 75 mg twice daily for 5 days, BMI < 30 (e) 75 mg twice daily for 5 days, BMI > 40 (f) 75 mg twice daily for 5 days
200 200 150
BMI < 30
Oseltamivir (ng/mL)
Oseltamivir (ng/mL)
Oseltamivir (ng/mL)
125
150 150 BMI > 40
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
100
100 100 75
50
50 50
25
0 0 0
0 3 6 9 12 0 3 6 9 12 0 3 6 9 12
Time (h) Time (h) Time (h)
(g) (h) (i)
Oseltamivir carboxylate (ng/mL)
Oseltamivir carboxylate (ng/mL)
Oseltamivir carboxylate (ng/mL)
75 mg single dose, BMI < 30 75 mg single dose, BMI > 40 75 mg single dose
800 800 600
700 700 500 BMI < 30
600 600 BMI > 40
400
500 500
400 400 300
300 300 200
200 200
100
100 100
0 0 0
0 3 6 9 12 15 18 21 24 0 3 6 9 12 15 18 21 24 0 4 8 12 16 20 24
Time (h) Time (h) Time (h)
(j) (k) (l)
Oseltamivir carboxylate (ng/mL)
Oseltamivir carboxylate (ng/mL)
Oseltamivir carboxylate (ng/mL)
75 mg twice daily for 5 days, BMI < 30 75 mg twice daily for 5 days, BMI > 40 75 mg twice daily for 5 days
800 800 600
700 700 BMI < 30
500
600 600 BMI > 40
400
500 500
400 400 300
300 300 200
200 200
100
100 100
0 0 0
0 3 6 9 12 15 18 21 24 0 3 6 9 12 15 18 21 24 0 4 8 12 16 20 24
Time (h) Time (h) Time (h)
Figure 1. Oseltamivir and oseltamivir carboxylate plasma concentrations versus time profiles in control (BMI,30) and morbidly obese (BMI. 40)
subjects. The individual plasma oseltamivir (a, b, d and e) and oseltamivir carboxylate (g, h, j and k) concentrations versus time after a single
75 mg dose of oseltamivir phosphate and after 5 days of twice-daily administration of 75 mg of oseltamivir phosphate are shown on linear
scales. Each line represents an individual patient. The corresponding mean+SD plasma oseltamivir (c and f) and oseltamivir carboxylate (i and l)
concentrations are shown on the right.
2086OPTIMO trial JAC
Table 2. Summary of oseltamivir pharmacokinetics
Single dose Steady-state
Parameter BMI,30 BMI.40 P BMI,30 BMI.40 P
Cmax (ng/mL) 71 (14– 171) 38 (7 –79) 0.089 68 (30 –177) 33 (15 –83) 0.009
C12 (ng/mL) 0 (0–1.6) 0 (0 –0) NA 1.2 (0– 2.4) 0 (0– 1.2) 0.024
Tmax (h) 1.0 (0.5–2) 1.5 (0.5 –4.0) 0.183 1.0 (0.5 –2.0) 1.3 (0.5 –3.0) 0.293
AUC0 – 1 (ng.h/mL) 132 (42– 160) 89 (46 – 104) 0.002 — — —
AUC0 – 12 (ng.h/mL) — — — 134 (92 –196) 85 (49 –128) 0.001
CL/F (L/h) 580 (470–1800) 840 (720 –1640) 0.002 560 (380– 810) 880 (590– 1530) 0.001
CL/F/TBW (L/h/kg) 8.6 (5.7–26.6) 6.8 (6.2 –10.3) 0.059 7.7 (5.5 –10.9) 6.4 (5.0 –9.6) 0.089
V/F (L) 1670 (700–7290) 2320 (900 –8210) 0.190 2110 (930– 4050) 3430 (1260–4800) 0.353
V/F/TBW (L/kg) 26.7 (8.3–108) 20.7 (7.5 –31.4) 0.280 30.2 (13.3– 54.0) 19.0 (10.4– 45.4) 0.101
t12 (h) 1.8 (1.0–3.4) 2.0 (0.8 –3.5) 0.853 2.4 (1.6 –5.5) 1.9 (1.1 –4.0) 0.199
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
Cmax, maximum concentration; C12, concentration 12 h after dose (i.e. trough); Tmax, time to maximum concentration; t12, half-life of elimination;
AUC0 – 1, area under the curve from time 0 to infinity; AUC0 – 12, area under the curve from time 0 h to 12 h; CL/F, oral clearance; V/F, oral volume
of distribution; TBW, total body weight.
Each value represents the median (range) of 10 subjects per group.
P≤ 0.05 (bold) indicates a significant difference in the median values between the low and high BMI groups.
Table 3. Summary of oseltamivir carboxylate pharmacokinetics
Single dose Steady-state
Parameter BMI,30 BMI. 40 P BMI,30 BMI. 40 P
Cmax (ng/mL) 250 (129 –470) 270 (130 –360) 0.796 430 (280– 700) 370 (230 –630) 0.123
C12 (ng/mL) 94 (0– 160) 91 (0 –180) 0.969 170 (140– 260) 130 (86 – 190) 0.094
Tmax (h) 3.0 (2.0 –7.0) 4.0 (3.0 –8.0) 0.043 4.0 (2.0 –5.0) 4.0 (3.0 –5.0) 0.284
AUC0 – 1 (ng.h/mL) 3000 (2100– 5900) 3100 (1700– 4100) 1.00 — — —
AUC0 – 12 (ng.h/mL) — — — 3600 (2600–5700) 2800 (2100– 4900) 0.075
CL/F (L/h) 23 (12 –33) 22 (17 – 40) 0.853 19 (12 –26) 25 (14 – 32) 0.075
CL/F/TBW (L/h/kg) 0.35 (0.18– 0.51) 0.17 (0.13– 0.27) 0.001 0.26 (0.18– 0.39) 0.18 (0.12– 0.28) 0.003
V/F (L) 260 (150 –430) 200 (130 –370) 0.528 210 (160– 360) 270 (140 –300) 0.315
V/F/TBW (L/kg) 3.6 (1.9 –6.3) 1.6 (0.8 –3.4) 0.002 3.2 (2.1 –5.3) 1.8 (1.0 –2.8) 0.002
t12 (h) 7.4 (4.9 –11.3) 6.9 (4.4 –7.5) 0.141 8.3 (6.4 –9.9) 6.9 (5.8 –10.1) 0.041
Cmax, maximum concentration; C12, concentration 12 h after dose (i.e. trough); Tmax, time to maximum concentration; t12, half-life of elimination;
AUC0 – 1, area under the curve from time 0 to infinity; AUC0 – 12, area under the curve from time 0 h to 12 h; CL/F, oral clearance; V/F, oral volume
of distribution; TBW, total body weight.
Each value represents the median (range) of 10 subjects per group.
P≤ 0.05 (bold) indicates a significant difference in the median values between the low and high BMI groups.
appeared similar in the obese versus non-obese subjects after versus lean group (Table 3). However, the median Cmax, C12,
the single dose of oseltamivir phosphate (Figure 1g –i). Represen- Tmax, AUC0 – 12, absolute CL/F and absolute V/F did not differ
tative of this, no significant differences were observed for the between groups. In both the single-dose and steady-state
single-dose metabolite pharmacokinetic parameters, with the studies, the TBW-normalized oseltamivir carboxylate CL/F and
exception of Tmax, which was slightly longer in the obese group V/F were lower in the obese group versus the non-obese group.
(Table 3). The concentrations of oseltamivir carboxylate at In the single-dose study, the median (range) metabolite/
steady-state appeared modestly lower in the obese versus non- parent drug AUC0 – 1 ratio was 23 (20 –50) in the control group
obese subjects (Figure 1j –l). The observed median (range) and significantly higher 34 (24 –72) in the obese group
steady-state accumulations of oseltamivir carboxylate in the (P ≤ 0.05). Similarly, in the steady-state study, the metabolite/
control [1.5 (1.2 –1.9)] and obese [1.4 (1.2 –1.5)] groups were parent drug AUC0 – 12 ratio was 26 (17 –43) in the control group
consistent with the accumulations [1.6 (1.2 –3.1) and 1.5 and significantly higher 35 (23 –54) in the obese group (P ≤ 0.05).
(0.95 –2.3)] predicted from the single-dose elimination rate con- As a secondary analysis, we examined the correlation
stant and the dosage interval. The median steady-state oselta- between the calculated oseltamivir and oseltamivir carboxylate
mivir carboxylate t12 was significantly shorter in the obese CL/F and V/F with TBW or LBW. After the single oseltamivir
2087Thorne-Humphrey et al.
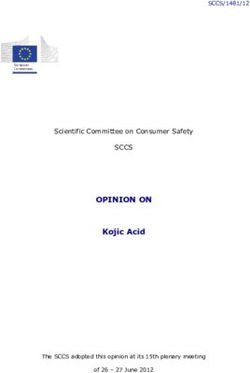
Single dose dose and at steady-state, oseltamivir CL/F correlated with TBW
(a) Oseltamivir CL/F versus TBW (Figure 2a and b) and to a lesser extent with LBW (single dose,
2000 r 2 ¼ 0.241, P ¼ 0.028 and steady-state, r 2 ¼ 0.583, P ¼0.001). In
comparison, the steady-state but not the single-dose oseltamivir
1500 carboxylate CL/F correlated weakly with TBW (Figure 2c and d) or
LBW (single dose, r 2 ¼ 0.144, P ¼ 0.099 and steady-state,
CL/F (L/h)
1000 r 2 ¼ 0.370, P ¼ 0.004). Oseltamivir V/F correlated weakly with
TBW (r 2 ¼ 0.297, P ¼0.013) but not with LBW (r 2 ¼0.162,
P ¼ 0.069) after a single dose of oseltamivir phosphate. TBW or
500
r2 = 0.375 LBW was not observed to have a significant linear correlation
P = 0.004 with steady-state oseltamivir V/F, and single-dose and
0 steady-state oseltamivir carboxylate V/F (data not shown).
0 50 100 150 200 250 300
During the analysis, one morbidly obese subject was identified
TBW (kg)
as an outlier (open squares, Figure 2), because of an extremely
Steady-state high body weight (.262 kg) and BMI (.80). One non-obese
subject was identified as an outlier with respect to oseltamivir
Oseltamivir CL/F versus TBW
(b) 2000 V/F and CL/F (open circles, Figure 2). When these subjects are
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
excluded, the correlation between oseltamivir CL/F with TBW
1500 (single dose, r 2 ¼ 0.659, P ¼ 0.004 and steady-state, r 2 ¼ 0.580,
P ¼ 0.001) and LBW (single dose, r 2 ¼ 0.337, P ¼ 0.014 and
CL/F (L/h)
1000
steady-state, r 2 ¼0.403, P ¼ 0.004) changed somewhat but
remained significant. In comparison, the single-dose oseltamivir
V/F no longer correlated with TBW (r 2 ¼ 0.182, P¼ 0.078). The
500 r2 = 0.690 steady-state correlation between oseltamivir carboxylate CL/F
P = 0.001 with TBW (r 2 ¼ 0.284, P ¼ 0.019) and LBW (r 2 ¼ 0.226, P¼ 0.040)
0 weakened but remained significant.
0 50 100 150 200 250 300
TBW (kg)
Single dose
Discussion
(c) Oseltamivir carboxylate CL/F versus TBW
50 In North America, the prevalence of obesity is on the rise. Par-
ticularly concerning is the dramatic rise in severe obesity,
40
which now stands at 2.2% and 1.3% of American and Canadian
adults, respectively.20,21 The increased prevalence of morbid
CL/F (L/h)
30
obesity is a concern for drug dosing, as increased total body
20 mass can significantly affect circulating and/or target tissue
drug concentrations.11,13,22 While the explanation for the
10 r2 = 0.149 observed association between morbid obesity and poorer out-
P = 0.093 comes in hospitalized patients with pH1N1 infection has not
0 yet been elucidated,7,9 pharmacokinetic differences for oseltami-
0 50 100 150 200 250 300 vir and/or oseltamivir carboxylate in obesity are distinct possibi-
TBW (kg) lities. Thus, our study was designed to specifically test the
effect of morbid obesity on the pharmacokinetics of oseltamivir
Steady-state
and its active metabolite.
(d) Oseltamivir carboxylate CL/F versus TBW
50
Figure 2. Linear correlations of oseltamivir and oseltamivir carboxylate
40
CL/F parameters with TBW. The single-dose and steady-state
oseltamivir (a and b) and oseltamivir carboxylate (c and d) CL/F were
CL/F (L/h)
30
plotted versus TBW, and the line of best fit through the points was
determined by linear regression. The corresponding r 2 and P values are
20
listed within each figure. Individuals in the BMI,30 group are
r2 = 0.412 represented by circles and those in the BMI. 40 group by squares. The
10
P = 0.370 open circles represent the CL/F values of a BMI, 30 subject who was
deemed an outlier with respect to oseltamivir CL/F and V/F in the
0
single-dose study. The open squares represent the CL/F values for a
0 50 100 150 200 250 300
morbidly obese individual who was deemed an outlier with respect to
TBW (kg) extremely high body weight (262 kg).
2088OPTIMO trial JAC
Orally administered oseltamivir is rapidly absorbed from the subjects and controls whereas TBW-normalized oseltamivir car-
gastrointestinal tract, followed by rapid conversion in the liver boxylate CL/F was significantly reduced in morbidly obese individ-
to oseltamivir carboxylate by carboxylesterase 1 (HCE1), resulting uals also indicates minimal dependence of these metabolite
in an overall bioavailability of 80% of the active metabolite.3,23 – 28 pharmacokinetic parameters on body weight. While we did
The reduction in oseltamivir single-dose AUC0 – 1 and observe a moderate linear correlation between oseltamivir car-
steady-state AUC0 – 12 and Cmax ss combined with an elevated boxylate CL and TBW at steady-state, the interpretation of the
oseltamivir CL/F and unchanging terminal elimination t12 could result should tempered by the fact that it was strongly influ-
indicate that the parent drug undergoes less absorption and/or enced by an outlier in the morbidly obese group. We did
a higher rate of first-pass metabolism to oseltamivir carboxylate observe that oseltamivir carboxylate t12 was significantly shorter
in obese versus non-obese individuals. The fact that the reduced in the obese subjects at steady-state. This result suggests an
AUC of the parent drug did not translate to an equivalent obesity-related increase in oseltamivir carboxylate elimination
reduction in the metabolite AUC argues against a major that becomes apparent as the metabolite accumulates to
reduction in oseltamivir absorption in morbidly obese individuals. higher levels. In theory, this could arise due to a combination
The latter possibility (increased first-pass metabolism) is sup- of enhanced renal tubule secretion and filtration elimination,
ported by the increase in the metabolite/parent drug AUC ratios which are the primary pathways of oseltamivir carboxylate elim-
in the morbidly obese versus control subjects. Some studies ination.26 However, we did not measure urinary levels of the
have reported increased activity of specific hepatic cytochrome metabolite and are unable to confirm this directly.
P450 enzymes in obesity.29,30 Therefore, an intriguing possibility
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
The perceived clinical significance of our overall findings is
to explain the lower oseltamivir Cmax ss and AUC values is that that the standard 75 mg twice-daily oseltamivir dose is sufficient
HCE1 activity is increased in the obese group. to provide adequate systemic levels of oseltamivir carboxylate in
The choice of size descriptor for drug dosing in obese individ- the majority of morbidly obese subjects. One could counter that
uals is still a matter of debate and there is no single valid method although not statistically significant, a 15% – 25% reduction in
to relate V or CL to the degree of obesity.11 Some have argued for oseltamivir carboxylate Cmax ss, C12 ss and AUC0 – 12 is potentially
the use of the semi-mechanistic model for LBW as an ideal meaningful in terms of reduced antiviral efficacy. However, at
metric to quantify the influence of body composition on drug steady-state in the morbidly obese and non-obese subjects,
CL and for adjusting chronic dosing in the obese.19 Others have respectively, the trough levels of oseltamivir carboxylate in our
also reported that the incorporation of the LBW formula does study exceeded the effective range of in vitro pH1N1 IC50
not lead to substantially improved relationships with CL com- (0.08 –0.40 mg/L) concentrations by 325 –1625- and 425 –
pared with TBW.31 In the case of oseltamivir, our results would 2125-fold.33 Thus, we conclude the minor reductions in oselta-
indicate TBW, rather than the semi-mechanistically calculated mivir carboxylate concentrations in morbidly obese individuals
LBW, as the more appropriate maintenance-dosing scalar. The are not likely to be clinically relevant. This interpretation is
observation that oseltamivir CL/F becomes similar in obese and consistent with that of Ariano et al.,25 who concluded that an
control groups when normalized to TBW is consistent with oseltamivir dose adjustment in morbid obesity is likely unnecess-
the correlative data and supports that oseltamivir clearance ary, given that the plasma levels still exceeded IC50 for the
changes in proportion to TBW. pH1N1 influenza strain.
The observed relationship between oseltamivir CL/F and TBW There are a number of important limitations with respect to
conflicts with a study presented by Ariano et al.,25 which showed our conclusion. First, the ability to extrapolate from oseltamivir
no correlations between oseltamivir or oseltamivir carboxylate CL carboxylate IC50 for inhibition of viral neuraminidase in vitro to
with TBW in critically ill patients after the enteric administration patient oseltamivir carboxylate plasma levels and clinical out-
of oseltamivir phosphate. The discrepancy could be due to the comes is not clear. There are in vitro data using a highly patho-
substantially different subjects in our respective studies. The genic H5N1 and mouse model that suggest that the in vivo
OPTIMO subjects were healthy and, other than body weight, efficacy of oseltamivir cannot be predicted by susceptibility
they were relatively homogeneous with respect to baseline testing.34 In addition, there are reports of patients with pH1N1
characteristics, including renal function. In comparison, the sub- who failed therapy because of the development of resistant
jects in the study by Ariano et al. had varying degrees of renal viruses through the selection of the H275Y mutation in the neur-
impairment. In addition, other confounding factors, such as aminidase gene. These viruses had a .200–1400-fold increase
short gut syndrome, time to steady-state and drug interactions, in the IC50 compared with the sensitive precursor viruses.35 – 37
were not controlled for and may have interfered with detecting a Given that the peak concentrations of the active metabolite at
relationship between oseltamivir and oseltamivir carboxylate steady-state in this study were 370 and 430 mg/L for morbidly
CL/F and TBW. It is also possible that in the critically ill, infected obese and non-obese groups, respectively, we expect that both
patient factors other than body weight, such as cytokine-drug would be insufficient to inhibit viral replication of resistant
disposition interactions or reduced renal function, become rate- strains. Studies that correlate clinical outcomes with plasma con-
limiting in their impact on oseltamivir and oseltamivir carboxy- centrations and viral susceptibility are needed to clarify this
late pharmacokinetics.32 issue. Second, we do not know whether plasma levels of oselta-
While the plasma concentrations of oseltamivir were signifi- mivir and its metabolite reflect lung concentrations in humans.
cantly lower in morbidly obese subjects receiving a single-dose Eisenberg et al.38 examined concentrations of oseltamivir phos-
or the 5 day twice-daily oseltamivir dosing regimen, this did phate and carboxylate in bronchial alveolar lavage fluid of rats,
not translate to an equivalent reduction in the systemic exposure and found that the parent drug and metabolite concentrations
to the active metabolite. The observation that absolute oseltami- were similar to those in plasma. This would suggest that
vir carboxylate CL/F and V/F were similar in morbidly obese plasma oseltamivir carboxylate concentration is a good
2089Thorne-Humphrey et al.
surrogate marker of the metabolite concentration at the site of
infection in the lung, assuming that the distribution is similar in Transparency declarations
humans and rats. However, we cannot conclude this with cer- The study investigators and authors received no remuneration for their
tainty, as bronchial lavage was not performed in our study of work on the OPTIMO trial. The study investigators/authors declare no
individuals with morbid obesity. Third, debate exists in how to conflicts of interest. All study authors had input into the design of
best estimate renal function in obese patients; measures such study and the intellectual material found in the manuscript. L. M. T.-H.,
as calculating the ODW are often used clinically to grossly deter- K. L. S. and S. A. M. were directly involved in conducting the clinical
mine an estimated glomerular filtration rate when IBW calcu- phase of the research. Hoffman-La Roche, the makers of Tamifluw, had
no role in the design of the trial, access to the data or its publication.
lations are thought to underestimate the renal CL of drugs in
obese patients. Others have proposed using LBW.18 Regardless
of the body weight estimate used, all obese subjects had
calculated CLCRs that were above our conservative cut point of References
60 mL/min and rightfully included in the study. Fourth, as we 1 Doucette KE, Aoki FY. Oseltamivir: a clinical and pharmacological
have shown, in a small study, outliers can influence the results perspective. Expert Opin Pharmacother 2001; 2: 1671–83.
of correlation analyses. Additionally, our small study size may 2 Jefferson T, Jones M, Doshi P et al. Neuraminidase inhibitors for
have insufficient power to detect small, yet clinically important, preventing and treating influenza in healthy adults: systematic review
differences between the two study groups. Fifth, our subjects and meta-analysis. BMJ 2009; 339: b5106.
3 Hoffman-La Roche Tamifluw (Oseltamivir Phosphate Capsule) Product
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
were all otherwise well and influenza free, and lung secretions
were not sampled for drug levels. Thus, our results may not be Monograph. 2009.
generalizable to morbidly obese, sick patients with influenza 4 CDC. Updated Interim Recommendations for the Use of Antiviral
pneumonia. Finally, no meal standardization for study subjects Medications in the Treatment and Prevention of Influenza for the 2009–
was conducted and, as a result, theoretical food–drug inter- 2010 Season. http://www.cdc.gov/h1n1flu/recommendations.htm (2
actions were conceivable, although deemed by investigators to May 2011, date last accessed).
be unlikely. 5 Writing Committee of the WHO Consultation on Clinical Aspects of
In conclusion, we report that systemic exposure to oseltamivir Pandemic (H1N1) 2009 Influenza. Clinical aspects of pandemic 2009
is decreased in morbidly obese subjects, whereas that of the influenza A (H1N1) virus infection. N Engl J Med 2010; 362: 1708– 19.
active metabolite is largely unchanged. Thus, an oseltamivir 6 WHO. Weekly Update On Oseltamivir Resistance To Pandemic Influenza
dose adjustment would not be needed in morbidly obese individ- A (H1N1) 2009 Viruses. http://www.who.int/csr/disease/swineflu/
uals. Based on our data, a possible exception are those of oseltamivirresistant20100611.pdf (2 May 2011, date last accessed).
extreme body weight (.250 kg), who could potentially be under- 7 Napolitano LM, Park PK, Sihler KC et al. Intensive-care patients with
exposed to the active metabolite following a standard 75 mg severe novel influenza A (H1N1) virus infection - Michigan, June 2009.
twice-daily regimen. In such cases, a TBW-based approach to MMWR Morb Mortal Wkly Rep 2009; 58: 749–52.
oseltamivir maintenance dosing could be considered if the goal 8 Jain S, Kamimoto L, Bramley AM et al. Hospitalized patients with 2009
is to achieve plasma oseltamivir and oseltamivir carboxylate H1N1 influenza in the United States, April– June 2009. N Engl J Med 2009;
levels more similar to those in patients who are non-obese. 361: 1935– 44.
9 Louie JK, Acosta M, Winter K et al. Factors associated with death or
hospitalization due to pandemic 2009 influenza A (H1N1) infection in
California. JAMA 2009; 302: 1896– 902.
Acknowledgements 10 Pai MP, Bearden DT. Antimicrobial dosing considerations in obese
Preliminary results of the OPTIMO trial have been presented at: the adult patients. Pharmacotherapy 2007; 27: 1081– 91.
Canadian Centre for Vaccinology—Annual Symposium, Halifax, Nova 11 Hanley MJ, Abernethy DR, Greenblatt DJ. Effect of obesity on the
Scotia, 2010 (poster and abstract); the Capital District Health Authority pharmacokinetics of drugs in humans. Clin Pharmacokinet 2010; 49:
Division of Infectious Diseases Annual Research Day, Halifax, Nova 71– 87.
Scotia, 2010 (poster); the Association of Medical Microbiology and 12 Bearden DT, Rodvold KA. Dosage adjustments for antibacterials in
Infectious Disease Canada—Canadian Association for Clinical obese patients: applying clinical pharmacokinetics. Clin Pharmacokinet
Microbiology and Infectious Diseases Annual Conference, Edmonton, 2000; 38: 415–26.
Alberta, 2010 (poster and abstract); and the Canadian Society of
13 Cheymol G. Effects of obesity on pharmacokinetics implications for
Pharmacology and Therapeutics Annual Conference, Toronto, Ontario,
drug therapy. Clin Pharmacokinet 2000; 39: 215–31.
2010 (oral presentation and abstract).
A special thank you to Cathy Brown, Sarah DeCoutere, Ying Wat, Petra 14 Cockcroft DW, Gault MH. Prediction of creatinine clearance from
Rykers, Annette Morris, Kim Slaney, Lisa Duncan, Anna Maria Brown, Gina serum creatinine. Nephron 1976; 16: 31– 41.
Dickie, Diana Lawlor and Kara Thompson, who all contributed 15 Hill G, Cihlar T, Oo C et al. The anti-influenza drug oseltamivir exhibits
significantly to the clinical phase of this study. low potential to induce pharmacokinetic drug interactions via renal
secretion—correlation of in vivo and in vitro studies. Drug Metab Dispos
2002; 30: 13– 9.
16 Heinig K, Bucheli F. Sensitive determination of oseltamivir and
Funding oseltamivir carboxylate in plasma, urine, cerebrospinal fluid and brain
This work was supported by the Canadian Centre for Vaccinology and an by liquid chromatography-tandem mass spectrometry. J Chromatogr B
unrestricted grant from Hoffman La-Roche Pharmaceuticals. All OPTIMO Analyt Technol Biomed Life Sci 2008; 876: 129–36.
investigators donated their time through in-kind donations or as part of 17 Wiltshire H, Wiltshire B, Citron A et al. Development of a
their employment at respective institutions. high-performance liquid chromatographic-mass spectrometric assay for
2090OPTIMO trial JAC
the specific and sensitive quantification of Ro 64–0802, an anti-influenza 28 Taylor WR, Thinh BN, Anh GT et al. Oseltamivir is adequately absorbed
drug, and its pro-drug, oseltamivir, in human and animal plasma and following nasogastric administration to adult patients with severe H5N1
urine. J Chromatogr B Biomed Sci Appl 2000; 745: 373– 88. influenza. PLoS One 2008; 3: e3410.
18 Janmahasatian S, Duffull SB, Ash S et al. Quantification of lean 29 Emery MG, Fisher JM, Chien JY et al. CYP2E1 activity before and after
bodyweight. Clin Pharmacokinet 2005; 44: 1051– 65. weight loss in morbidly obese subjects with nonalcoholic fatty liver
19 Han PY, Duffull SB, Kirkpatrick CM et al. Dosing in obesity: a simple disease. Hepatology 2003; 38: 428–35.
solution to a big problem. Clin Pharmacol Ther 2007; 82: 505– 8. 30 de la Maza MP, Hirsch S, Petermann M et al. Changes in microsomal
20 Freedman DS, Khan LK, Serdula MK et al. Trends and correlates of activity in alcoholism and obesity. Alcohol Clin Exp Res 2000; 24: 605–10.
class 3 obesity in the United States from 1990 through 2000. JAMA 31 Mathijssen RH, Sparreboom A. Influence of lean body weight on
2002; 288: 1758– 61. anticancer drug clearance. Clin Pharmacol Ther 2009; 85: 23; author reply 4.
21 Katzmarzyk PT, Mason C. Prevalence of class I, II and III obesity in 32 Renton KW. Regulation of drug metabolism and disposition during
Canada. CMAJ 2006; 174: 156–7. inflammation and infection. Expert Opin Drug Metab Toxicol 2005; 1:
22 Poggesi I, Benedetti MS, Whomsley R et al. Pharmacokinetics in 629–40.
special populations. Drug Metab Rev 2009; 41: 422–54. 33 Update: drug susceptibility of swine-origin influenza A (H1N1) viruses,
23 Davies BE. Pharmacokinetics of oseltamivir: an oral antiviral for April 2009. MMWR Morb Mortal Wkly Rep 2009; 58: 433–5.
the treatment and prophylaxis of influenza in diverse populations. 34 Govorkova EA, Ilyushina NA, McClaren JL et al. Susceptibility of highly
J Antimicrob Chemother 2010; 65 Suppl 2: ii5–10. pathogenic H5N1 influenza viruses to the neuraminidase inhibitor
Downloaded from http://jac.oxfordjournals.org/ by guest on February 3, 2015
24 Shi D, Yang J, Yang D et al. Anti-influenza prodrug oseltamivir is oseltamivir differs in vitro and in a mouse model. Antimicrob Agents
activated by carboxylesterase human carboxylesterase 1, and the Chemother 2009; 53: 3088 –96.
activation is inhibited by antiplatelet agent clopidogrel. J Pharmacol Exp 35 Baz M, Abed Y, Papenburg J et al. Emergence of oseltamivir-resistant
Ther 2006; 319: 1477– 84. pandemic H1N1 virus during prophylaxis. N Engl J Med 2009; 361: 2296– 7.
25 Ariano RE, Sitar DS, Zelenitsky SA et al. Enteric absorption and 36 Memoli MJ, Hrabal RJ, Hassantoufighi A et al. Rapid selection of
pharmacokinetics of oseltamivir in critically ill patients with pandemic oseltamivir- and peramivir-resistant pandemic H1N1 virus during therapy
(H1N1) influenza. CMAJ 2010; 182: 357–63. in 2 immunocompromised hosts. Clin Infect Dis 2010; 50: 1252 –5.
26 He G, Massarella J, Ward P. Clinical pharmacokinetics of the prodrug 37 Speers DJ, Williams SH, Pinder M et al. Oseltamivir-resistant pandemic
oseltamivir and its active metabolite Ro 64-0802. Clin Pharmacokinet (H1N1) 2009 influenza in a severely ill patient: the first Australian case.
1999; 37: 471–84. Med J Aust 2010; 192: 166– 8.
27 Massarella JW, He GZ, Dorr A et al. The pharmacokinetics and 38 Eisenberg EJ, Bidgood A, Cundy KC. Penetration of GS4071, a novel
tolerability of the oral neuraminidase inhibitor oseltamivir (Ro 64-0796/ influenza neuraminidase inhibitor, into rat bronchoalveolar lining fluid
GS4104) in healthy adult and elderly volunteers. J Clin Pharmacol 2000; following oral administration of the prodrug GS4104. Antimicrob Agents
40: 836–43. Chemother 1997; 41: 1949 –52.
2091You can also read