Prone restraint cardiac arrest: A comprehensive review of the scientific literature and an explanation of the physiology - Charly D. Miller
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review article
Medicine, Science and the Law
0(0) 1–12
Prone restraint cardiac arrest: ! The Author(s) 2021
Article reuse guidelines:
A comprehensive review of the sagepub.com/journals-permissions
DOI: 10.1177/0025802420988370
scientific literature and an explanation journals.sagepub.com/home/msl
of the physiology
Alon Steinberg
Abstract
Deaths occurring among agitated or violent individuals subjected to physical restraint have been attributed to positional
asphyxia. Restraint in the prone position has been shown to alter respiratory and cardiac physiology, although this is
thought not to be to the degree that would cause asphyxia in a healthy, adult individual. This comprehensive review
identifies and summarizes the current scientific literature on prone position and restraint, including experiments that
assess physiology on individuals restrained in a prone position. Some of these experimental approaches have attempted
to replicate situations in which prone restraint would be used. Overall, most findings revealed that individuals subjected
to physical prone restraint experienced a decrease in ventilation and/or cardiac output (CO) in prone restraint.
Metabolic acidosis is noted with increased physical activity, in restraint-associated cardiac arrest and simulated encoun-
ters. A decrease in ventilation and CO can significantly worsen acidosis and hemodynamics. Given these findings, deaths
associated with prone physical restraint are not the direct result of asphyxia but are due to cardiac arrest secondary to
metabolic acidosis compounded by inadequate ventilation and reduced CO. As such, the cause of death in these
circumstances would be more aptly referred to as “prone restraint cardiac arrest” as opposed to “restraint asphyxia”
or “positional asphyxia.”
Keywords
Forensic medicine, medical law, prone restraint, cardiac arrest, restraint asphyxia, restraint physiology, prone asphyxia,
cardiac output, metabolic acidosis and police custody death
Introduction
(i.e., cellular exchange of oxygen and carbon diox-
Physical restraint is used by law enforcement officers ide).14 In cases of compression asphyxia, the physical
(LEOs) and health-care workers when dealing with act of ventilation is impaired or prevented by compres-
people who are aggressive, uncooperative, or violent. sion due to an external force on the chest and/or abdo-
Deaths have been reported during physical restraint of men.15 The definition of death from positional
agitated individuals held in the prone (facedown) posi- asphyxia involves three specific criteria: (a) evidence
tion, as detailed in case reports, case series, and that the individual’s body position interfered with or
inquests.1–13 However, the actual physiologic cause of prevented ventilation or normal gas exchange, (b) evi-
death in these circumstances remains uncertain. There dence that the individual was unable to move to anoth-
is currently controversy regarding the role of positional er position, and (c) clear exclusion of other causes of
asphyxia as the primary factor underlying restraint- death based on finding from autopsy.2
associated mortality.
Asphyxia is defined as a state of impaired oxygen
intake and the accumulation of excess carbon dioxide Community Memorial Hospital, USA
that results in loss of unconsciousness and often leads
Corresponding author:
to death. Asphyxia typically results from physical inter- Alon Steinberg, Cardiology Associates Medical Group, 168 North Brent
ference with the mechanics of breathing (i.e., inhala- St Suite 503, Ventura, CA 93003, USA.
tion, exhalation, and ventilation) and/or respiration Email: aloncardio@gmail.com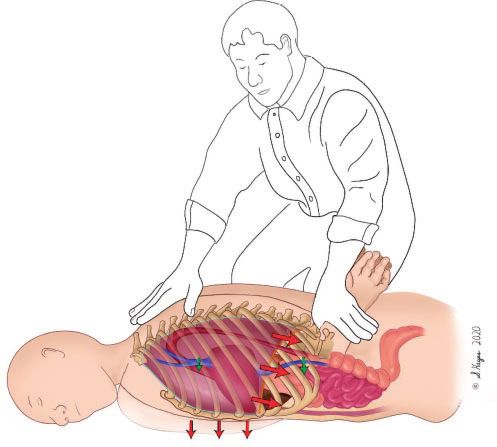
2 Medicine, Science and the Law 0(0)
Restraint procedures currently in use include Methods
“hogtie restraint” in which the subject’s wrists are
A literature search of PubMed, Medline, and Google
handcuffed behind their back with ankles strapped
Scholar was performed to identify all English language
(hobbled), also known as the prone maximal restraint
manuscripts published between 1980 and August 2020.
position (PMRP).16 Other physical restraint procedures
Keywords used included positional asphyxia, postural
include (a) physically restraining the extremities while
asphyxia, restraint asphyxia, sudden death custody,
an individual is held in a prone position, and (b) plac-
sudden death restraint, excited delirium, acute behav-
ing downward pressure on a subject’s back (a weight ioral disorder, physiological restraint death, and prone
force (WF)) while in the prone position. Individuals position adverse effects. Publications included were
who expired while held in these restraint positions those that focused on both medical science and clinical
meet the previously defined criteria for positional aspects associated with deaths related to prone
asphyxia and their postmortem diagnosis can be restraint with particular reference to positional or
referred to as restraint asphyxia.5,16 restraint asphyxia. Citation lists within these publica-
Epidemiological studies have revealed that deaths tions were searched and reviewed for additional source
due to prone restraint are rare, and occur approximate- material. This information was used to build and to
ly two to three times a year in regions that include Los expand on an earlier review of the adverse effects of
Angeles,6 Ontario in Canada,17 and England and physical restraint by Barnett et al.22 and also included
Wales.18 Other studies, including one carried out over studies that focused on metabolic acidosis and the
a seven-year period in western Canada19 and another impact of physical prone restraint on circulatory
one-year study that involved 11 agencies across the physiology.
USA,20 reported no deaths, despite the frequent use
of prone restraint in cases involving police custody.
These two studies led the authors to conclude that Ventilation
prone restraint was associated with no clinically signif-
Basic physiology
icant effects19 and that this method was safe.20 Indeed,
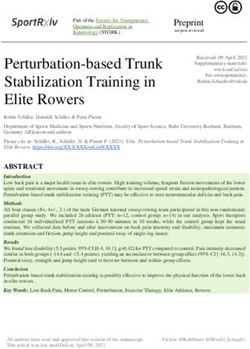
the authors of three independent textbooks stated Contraction of the diaphragm is responsible for about
clearly that there is no significant physiologic evidence two thirds of the air that enters the lungs during relaxed
indicating that force used on subjects held in the prone breathing (Figure 1).23 During deep inspiration, the
position results in significant respiratory compromise diaphragm can descend by as much as 10 cm.23
that could lead to asphyxia and death.16,21,63 Individuals in a prone position can experience an
The precise role of physical restraints and their increase in intra-abdominal pressure, which limits the
impact on respiratory physiology and cardiac output space available for movement of the diaphragm and
(CO) remain unclear. While many experimental set- expansion of the chest cavity, thereby decreasing ven-
tings have attempted to reproduce the impact of tilation.22,24–27 The prone position also restricts expan-
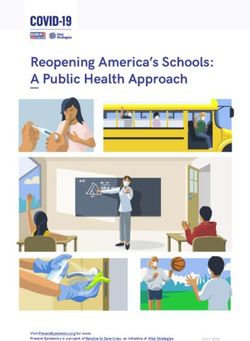
prone restraint and PMRP, these experiments were typ- sion of the ribs and external intercostal muscles,
ically performed on healthy volunteers. By contrast, likewise limiting the expansion of the chest cavity
agitated individuals may be in a state of preexisting (Figure 2).3,4,6,25
metabolic acidosis. Restraint in the prone position Several studies published in the medicolegal litera-
may exacerbate this state via inadequate ventilation ture have focused on attempts to replicate prone
and a decrease in CO. These physiologic derangements restraint situations to assess an individual’s capacity
can lead to pulseless electrical activity (PEA) and asys- for ventilation under these conditions (Table 1).24–31
tolic cardiac arrest. These experimental models are limited by their inability
In this review, the results of several published studies to replicate real-world conditions and the chaotic sit-
that report the effects of prone restraint on respiratory uations in which prone restraint would ordinarily be
physiology and CO are reviewed. The review also applied. Most subjects in these experiments were
focuses on the physiology of physical activity and sec- healthy and not in a “fight-or-flight” or a fearful
ondary metabolic acidosis that has been reported in state that would most likely prevail during a confron-
tation with an LEO or health-care worker.
individuals with acute behavioral disturbances.
Several alternative theories that may explain the
cause of death in individuals subjected to prone Pulmonary function tests
restraint are also presented. Taken together, this con- Pulmonary function tests (PFTs) are a set of clinical
sideration of the published literature explores the evaluations that document how well the lungs are func-
hypothesis that prone restraints may not be universally tioning at a given moment in time. Forced vital capac-
safe, and supports efforts to limit their use. ity (FVC) is the amount of air an individual can exhale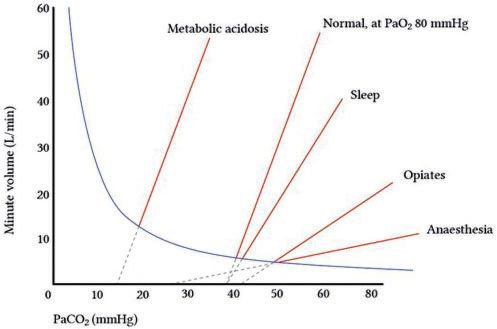
Steinberg 3
Figure 1. Normal breathing. Diaphragm expanding into abdomen and rib expansion are important components. (Illustrations by
Suzanne Hayes.)
minute. Individuals undergoing MVV testing are
instructed to breathe rapidly and deeply for 12–30 sec-
onds; the volume is then measured in liters per
minute.35 MVV can be used to estimate breathing
reserve during maximal exercise and can provide an
estimate of respiratory muscle endurance and fatigue.35
Research studies from the University of California,
San Diego
One research group at the University of California San
Diego (UCSD) has published several studies that
assessed ventilatory capacity in prone
patients.24–26,28,29 Changes in PFTs were detected,
although these findings were deemed as not clinically
significant by the authors. The first study enrolled 15
Figure 2. Prone restraint leads to an increase in intrathoracic
pressure, thus reducing venous return. Decreased rib expansion healthy volunteers who were evaluated with PFTs
also reduces ventilation. Prone restraint also increases intra- while sitting, supine, prone, and in the PMRP after
abdominal pressure, which compresses the low pressure inferior four minutes of exercise on a bicycle. The authors
vena cava, thereby decreasing venous return. Lastly, intraabdo- reported a 13% drop in baseline FVC, a 14% drop in
minal compression also limits diaphragm expansion and
baseline FEV1, and a 21% drop in MVV in partici-
decreases ventilation.
pants in the PMRP when compared to responses
from the same individuals evaluated while in a sitting
in a single breath. Forced expiratory volume (FEV1) is position.28 A second study from this group measured
the amount of air an individual can exhale rapidly in PFTs in the sitting, supine, and prone positions in 20
the first second of exhalation.23,34,35 Maximum volun- healthy men. The authors reported statistically signifi-
tary ventilation (MVV) measures the largest volume of cant reductions in PFT results, including an 8% reduc-
air that can be moved by voluntary effort in one tion in FVC, a 10% reduction in FEV1, and a 16%4 Medicine, Science and the Law 0(0)
Table 1. Ventilatory capacity in prone and restrained prone subjects.
Study No. of Subjects BMI (kg/m2) Restraint conditions Percent change vs. sitting
FVC FEV1 MVV
Chan et al., 199728 15 35 kg/m2.26 Prior UCSD studies had only
or 50 lb weights placed on the subject’s back). PFTs included subjects with a BMISteinberg 5
However, no significant change in end-tidal CO2 was and FEV1 were reduced to 11% and 10%, respectively,
noted when comparing outcomes between these three in what was described as a “supported prone” position
positions—a finding that would be expected with no that reduced pressure on the anterior chest.33
apparent change in MVV. Kroll et al. estimated that the application of a 260 kg
(570 lb) weight will result in a flail chest, which is a
Other published trials major cause of acute fatal compression asphyxia.36
This initial observation was followed by an evaluation
Several published trials from other groups identified
of WF applied to prone mannequins by an LEO with
significant decreases in lung capacity among partici-
three different single-knee techniques and one double-
pants held in a prone position and the PMRP.27,30,31
knee technique.37 This group reported that the
Roeggia et al. placed six healthy young males in a
application of a single knee creates an average WF of
prone restraint position for three minutes and found
23.7–32.9 kg, independent of the weight of the LEO.
that their FVCs and FEV1s dropped by 40% and
The double-knee technique created a WF that was
42%, respectively, from initial measurements; this
23.3 kg plus 24% of the weight of the LEO. As such,
decrease was described as “dramatic.”27 These authors
the authors concluded that force typically applied by
also reported that end-tidal CO2 increased by 14.7%
LEOs on subjects held in a prone position was safe and
among participants held in a prone restraint position.
did not support the concept of restraint asphyxia.
Likewise, Cary et al. evaluated the responses of 12
Ventilation studies with individuals held in the
healthy subjects of unknown weight.30 Subjects exer-
PMRP both with and without added weights revealed
cised by cycling until they reached 85% of their age-
no significant changes in blood oxygenation.24,25,27,30
predicted maximal heart rate. Subjects were then tested
At rest, the ratio of alveolar ventilation to pulmonary
during the post-exercise period while seated, in prone
blood flow (the V/Q ratio) is normally 0.84. During
positions, and in the prone position with a 75 kg (165
intense physical activity, alveolar ventilation increases
lb) added weight burden placed across each subject’s
disproportionately to blood flow; the V/Q ratio may
back. Among their findings, the participants’ FVCs
ultimately exceed 5.0 to ensure adequate aeration and
dropped by 12% while in the prone position and by
oxygenation of blood.38 As such, the decrease in ven-
31% while in the prone position with the added 75 kg
tilation noted in the aforementioned studies would be
weight burden, while FEV1s dropped 14% and 35%,
unlikely to result in hypoxia.
respectively. MVVs did not change significantly among
participants in the prone position but dropped by 33%
among participants in the prone position with the
Prone positioning and mechanical ventilation
added 75 kg weight burden. The authors concluded The recent coronavirus disease pandemic has resulted
that these findings represented “marked reductions” in increased awareness of prone positioning with
in ventilatory capacity.22,30 Parkes reported an average respect to the treatment of patients who require
25% drop in FVC and a 28% drop in FEV1 in a cohort mechanical ventilation for acute respiratory distress
of 14 healthy volunteers positioned in prone restraint. syndrome (ARDS). Prone positioning has been
These findings were described as “significant.” One shown to improve oxygenation in patients with severe
participant in this study experienced a 57% drop in hypoxemia. As such, this intervention is likely to
FEV1.31 reduce mortality among patients with severe ARDS
Other published studies include that of Meredith when it is applied for at least 12 hours a day.39 Prone
et al., who examined PFTs in eight individuals (ages positioning may improve oxygenation in this patient
45–80 years) with chronic obstructive pulmonary dis- cohort and prevent ventilator-induced lung injury by
ease who were in prone the position and PMRP. Three reducing overinflation while promoting alveolar
of the eight participants were unable to tolerate the recruitment. As such, prone positioning would serve
prone position due to clinical symptoms and deteriora- to normalize the distribution of stress and strain
tion. No statistically significant changes in FVC or within the lungs.40 While undergoing mechanical ven-
FEV1 were identified among the five participants tilation, these patients are anesthetized and provided
who completed the study protocol. The authors con- with a fixed volume (i.e., no decrease in the prone posi-
cluded that response to the prone position and PMRP tion) together with positive end-expiratory pressure
varied on a case-by-case basis.32 In another study, (PEEP). In these cases, the diaphragm acts as a passive
Barnett et al. reported that the prone position imposed membrane.41 The positive effects of prone positioning
pressure on the anterior chest and thereby restricted on regional blood flow and ventilation are substantially
lung function. The participants in this study experi- greater in patients under general anesthesia and those
enced a 16% decrease in FVC and a 16% decrease in provided with PEEP than they are in patients who
FEV1 while in the prone position. Decreases in FEV remain awake and capable of breathing6 Medicine, Science and the Law 0(0)
spontaneously.42 In other words, while prone position- experience a 45% reduction in CO in response to exer-
ing may serve to improve oxygenation of mechanically cise compared to normal controls.45 One recent publi-
ventilated ARDS patients, these findings are not rele- cation reported the case of a patient who developed
vant to healthy unsedated subjects placed in prone shock secondary to acute IVC occlusion.46
restraint.
Research studies
Cardiac output A study from the UCSD group enrolled 25 healthy
subjects that were placed in five positions: supine,
Basic physiology prone, PMRP, PMRP with an additional 50 lb of
CO is the volume of blood pumped by the heart per weight placed on the back, and PMRP with an addi-
unit time and is the product of heart rate and stroke tional 100 lb of weight placed on the back. No PFTs
volume.38 The cardiac index (CI) is the CO divided by were performed. Vital signs, CO, and CI were deter-
the body surface area. CO has a direct impact on mined by echocardiography, and IVC diameters were
oxygen and CO2 transport to and from the muscles measured. No statistically significant changes in these
during physical activity. The amount of oxygen that parameters were noted, except the CI underwent a 16%
the body utilizes is the product of the CO and oxygen drop upon addition of the 50 lb weight, and the IVC
extraction (i.e., the arteriovenous oxygen difference).38 diameter dropped by 19% in response to the addition
A decrease in CO will result in decreased oxygen deliv- of the 100 lb weight (Table 2).47
ery to the muscles, including the heart and the lungs, By contrast, results from studies carried out by other
and will reduce the amount of oxygen that can be uti- groups revealed significant decreases in CO and IVC
lized. A decrease in CO will also reduce the rate and diameter under similar conditions. For example,
amount of CO2 delivery to the lungs and result in Roeggia et al. reported a 37% drop in CO in patients
diminished pulmonary blood flow and perfusion. held in prone restraint. The observed decrease in CO
was attributed to reduced venous return through the
IVC to the heart.27 Likewise, in a study involving 14
CO and prone position healthy volunteers, Pump et al. reported an 18%
The prone position generates an increase in intratho- decrease in stroke volume and an 11% decrease in
racic pressure, thereby decreasing venous return CO among participants in an unrestrained prone posi-
(Figure 2) to the heart and thus decreasing CO.38 The tion.48 Furthermore, Ho et al. evaluated IVC diameters
prone position can also lead to abdominal restriction in 25 healthy subjects during standing, prone, prone
and obstructed blood flow in the compliant inferior restraint with an additional 45 kg (100 lb) placed on
vena cava (IVC), thereby reducing preload and CO. each participant’s back, and prone with an additional
IVC flow in the resting supine position represents 67 kg (147 lb) placed on each participant’s back.49
20–30% of total CO.43 This value increases to Compared to standing, prone with the addition of the
45% of total CO during supine leg exercise.44 45 kg weight resulted in significant reductions of 42%
Patients who have undergone an IVC ligation and 68% in the minimal longitudinal and transverse
Table 2. Cardiac output and IVC diameter changes in restrained prone subjects.
Researchers Prone type CO/CI IVC
Yokoyama et al., 199153 Prone anesthesia –18%
Backofen et al., 198551 Prone anesthesia –21%
Sudheer et al., 200652 Prone with propofol –20%
Prone anesthesia –27%
Roeggla et al., 199929 PMRP –37%
Pump et al., 200248 Prone position –11%
Krauskopf et al., 200850 Prone with 15 kg –11% –45%
Prone with 25 kg –16% –58%
Ho et al., 201149 Prone with 45 kg –31% to 68%
Prone with 67 kg –57% to 77%
Savaser et al., 201347 PMRP –10%* 8%*
PMRP with 50 lb –16% 12%*
PMRP with 100 lb –12%* 19%
*Not statistically significant.
IVC: inferior vena cava; CO: cardiac output; CI: cardiac indexSteinberg 7
diameters, respectively, while the maximal diameters 20- to 25-fold to 150 L/min during short periods of
were reduced by 31% and 35%, respectively. The addi- maximal exercise.23 Likewise, respiratory rates can
tion of the 67 kg weight also resulted in significant 77% increase from 16–20 to 40–50 breaths per minute.
and 74% reductions in minimal longitudinal and trans- Ventilation and CO both increase linearly with
verse diameters, respectively, with maximal diameters oxygen consumption during exercise. The increases in
reduced by 57% and 45%, respectively.49 No CO ventilation develop more rapidly to maintain physio-
values were reported. Finally, Krauskopf et al. studied logic pH under conditions that promote the production
responses to weights applied to the lower torsos of six and release of lactic acid. CO does not increase to the
healthy, non-obese volunteers, five of whom were same extent as ventilation and can undergo maximal
noted to be athletic. Application of 15 lb to the lower increases of four- to sixfold over the resting CO
torsos of each subject when in the prone position level.23,34 The increase in venous return observed in
resulted in a 45% reduction in IVC diameter, a 69% response to deeper inspiratory efforts and extravascu-
reduction in maximal IVC blood flow, and an 11% lar compression by muscles used during exercise
decrease in CO. Application of 25 lb to the lower together with a decrease in venous capacitance all con-
torso resulted in a 58% reduction in IVC diameter, tribute to an increased stroke volume. Oxygen con-
an 80% reduction in maximal IVC blood flow, and a sumption (VO2) is the product of CO and the oxygen
16% reduction in CO. The results of this study revealed arteriovenous oxygen difference. Although increased
significant IVC compression and decreased CO among oxygen use and extraction result in a significant drop
participants placed in the prone position with added in venous oxygen levels, arterial oxygen levels are
weights.50 maintained.
CO during surgical procedures Conditions associated with metabolic acidosis
Surgeons often perform procedures on patients placed Psychotic or agitated behavior secondary to a psychi-
in a prone position. This position has been evaluated in atric condition or illicit stimulant abuse may incite a
publications focused on anesthesia, and revealed state in which an individual may be unable to cooper-
decreases in CO that ranged from 17% to 26%.51–53 ate with LEOs or health-care workers. Individuals in
Diminished CO has been attributed to reduced these altered states are less likely to cease exertion due
venous return, direct effects on arterial filling, and to fatigue and may resist and struggle while in restraint.
reduced left ventricular compliance secondary to These activities can result in a high-output state requir-
increased thoracic pressure. IVC compression is a rec- ing significant increases in ventilation, CO, and oxygen
ognized complication that can occur in patients placed extraction.
in a prone position during surgery and has been Metabolic acidosis can occur during intense exercise
reported to be exacerbated by abdominal and can result from an increased reliance on non-
compression.54 mitochondrial ATP turnover.56 Blood pH levels as
low as 6.8 have been reported in association with
exhausting exercise.33 In a study of 12 subjects designed
Physical activity and metabolic acidosis to simulate physical resistance to an LEO, Ho et al.
found that just 45 seconds of heavy bag physical resis-
Basic physiology
tance exercise resulted in a reduction of blood pH from
Physical activity increases the metabolic rate in work- 7.36 (physiologic) to 7.04, together with a significant
ing muscles, increases ventilation, and augments CO. increase in epinephrine, norepinephrine, dopamine,
Oxygen consumption is measured in units of metabolic and total catecholamine levels.57 Interestingly, blood
equivalents of task (METs), which defines the rate of pH remained low (at 7.06) at 10 minutes post exercise.
oxygen consumption per minute.55 For example, skip- Hick et al. described five individuals who sustained
ping rope at 84 times a minute, rowing a distance of cardiac arrest while in the custody of LEOs and were
8 km/h, or ambulating at a rate of 3.4 mph with a 14% found to have severe acidosis (pH range 6.25–6.81).58
grade consume oxygen at 10 times the baseline rate Individuals in psychotic or delirious states may have
(i.e., 10 METs). The relative maximum intensity and altered sensation, and as such, they may continue to
energy that can be used, a value known as the VO2 exert themselves beyond normal physiologic limits.
max, reflects the absolute intensity of METs.38 While in this state, metabolic acidosis signals a signif-
During physical activity, ventilation, oxygen extrac- icant compensatory increase in ventilation, thus result-
tion, and CO all increase to meet the acute demand for ing in a secondary respiratory alkalosis. Hick et al.
oxygen consumption. In normal adults, the resting theorized that prone placement and restraint may
minute ventilation of 5–6 L/min can be increased impede the development of the critical compensatory8 Medicine, Science and the Law 0(0)
respiratory alkalosis—a problem that may ensue in specific mechanisms connect ventilation and pH via
response to a mere 20% reduction in ventilatory the partial pressure of CO2 (pCO2). The first relation-
capacity.58 ship is based on the fact that PaCO2 (arterial partial
During heavy physical activity, ventilation is no pressure of CO2) is directly proportional to VCO2
longer linked as tightly to oxygen demand. Instead, ((CO2 production))/Va (alveolar ventilation)).23,34 If
ventilation is connected directly to CO2, hydrogen ion one assumes that CO2 production is constant, a
(Hþ), and lactate anion concentrations that stimulate decrease in ventilation will result in a net increase in
and regulate respiratory function and ventilation.38 arterial CO2. For example, a 20% decrease in ventila-
tion will generate a 25% increase in PaCO2. The second
Post-exercise syncope relationship is based on the equilibrium between acids
and bases as defined by the Henderson–Hasselbalch
Muscle contraction during exercise is a critical factor
equation (below) and the fact that acidity or pH is
that promotes venous return to the heart.38 An individ-
directly related to pCO2:
ual who is held in restraint may result in a significant
decrease in venous return, with pooling of blood in the
pH ¼ pKa þ log ½ðHCO3 Þ=ð0:03 pCO2 Þ
extremities, resulting in reduced CO. Post-exercise syn-
cope or loss of consciousness is a condition thought to
be due to a sudden reduction in muscle activity result- Given this relationship, a 25% increase in arterial
ing in decreased venous return. This may initiate a pCO2 would (as per the Henderson–Hasselbalch equa-
neurocardiogenic response and a drop in systemic tion) result in a decrease in pH by 0.1.23,34 As such,
blood pressure.59,60 This paradoxical response may decreased ventilation in a person who may have
contribute to deaths observed in individuals who have already be in a state of severe metabolic acidosis can
developed severe metabolic acidosis. However, there have a catastrophic outcome. Reduced ventilation will
were no reports of a significant drop in blood pressure serve to exacerbate the acidosis and thereby promote
or syncope among any of the individuals who partici- autonomic instability with secondary PEA or
pated in studies involving exercise with prone asystole.61
restraint.24,28,30 Reduced CO in an individual with preexisting severe
metabolic acidosis may also result in severe negative
outcomes due to decreased delivery of CO2 to the
Effects of prone restraint on the lungs. A decrease in CO will also reduce oxygen flow
physiology of an individual with metabolic to the muscle tissue during a situation that requires
acidosis significant oxygen demand and extraction. Given
Prone restraint has been shown to limit ventilation due these observations, the decrease in CO observed
to a decrease in pulmonary volumes in a restrictive among individuals held in prone restraint may be suf-
pattern.24,27–31,33 As stated previously, decreased venti- ficient to cause death.
lation has no significant impact on arterial oxygen
level. However, CO2 has a direct effect on this response Reconsideration of current terminology
to ventilation (Figure 3).23 The process of the respira- The terms “restraint asphyxia” and “prone asphyxia”
tory system responding to pH changes in peripheral do not provide a correct description of this condition
circulation is known as respiratory regulation. Two because positional and/or restraint-associated limita-
tions on breathing and gas exchange represent only
part of the problem. This condition should be renamed
“prone restraint cardiac arrest.” Cardiac arrest in this
setting is due to a combination of factors, including a
state of high oxygen demand, a need for increased CO2
removal, and significant metabolic acidosis, along with
the significant decrease in both ventilation and CO.
Indeed, restraint in the prone position added to preex-
isting metabolic acidosis represents a potential physio-
logic catastrophe.
Alternative theories
Figure 3. Direct relationship of minute volume ventilation to Alternative theories have been postulated to explain
PaCO. (From Levitsky.23) deaths occurring in individuals held in prone restraint.Steinberg 9
While many of these theories focus on cardiac condi- Discussion
tions, there is usually no evidence of significant cardiac
Asystole and PEA are the primary arrhythmias associ-
pathology reported on autopsy.1,3,5,6,8 Individuals with
ated with the “4Hs and 4Ts,” including hypoxia, hypo-/
normal cardiac structural anatomy do at times experi-
hyperkalemia, hydrogen ion (acidosis), hypo-/hyper-
ence sudden cardiac death (SCD) during or immediate-
thermia, hypovolemia, tension pneumothorax, cardiac
ly after a stressful event.64 These events have been
tamponade, thrombosis (coronary and pulmonary),
linked to various cardiac disorders.62,65,66 Among
and toxins (poisoning).69 These conditions have revers-
these disorders, channelopathies are a group of condi-
ible causes and require specific treatments. Asystole
tions associated with the dysfunction of ion channels
and PEA are commonly observed in cardiac arrests
located in the cardiac cell membranes, including pro-
associated with asphyxia and metabolic acidosis.61
longed QT interval, catecholaminergic ventricular
Even with the application of cardiopulmonary resusci-
tachycardia, and arrhythmogenic right ventricular dys-
tation, advanced cardiovascular life support, and treat-
plasia. Increased activity of catecholamines and adre-
ment of reversible causes, the probability of survival
nergic receptors that will occur during an altercation
after asystole or a PEA-associated cardiac arrest is
may provoke ventricular arrhythmias in these individ-
extremely low (currently estimated at 4.4%).70 Lower
uals. Stress-induced Takotsubo cardiomyopathy, a pH values detected post-cardiac arrest have been asso-
condition characterized by catecholamine-induced ciated with comparatively lower rates of survival.71 As
myocardial stunning and weakening of the heart such, the best management practices focus on both pre-
muscle, may also predispose an affected individual to vention and treatment of the “4Hs and 4Ts” in an
ventricular arrhythmias. Coronary artery spasm may effort to avoid cardiac arrest. Put plainly, it is impor-
lead to ventricular arrhythmias and subsequent death tant to identify potentially vulnerable subjects who
in individuals with structurally normal hearts. Some might present with metabolic acidosis and to refrain
SCD events have been linked to psychiatric drugs, as from the use of prone restraint. Multiple studies
the use of these medications can lead to a prolonged reviewed in this article revealed that the prone restraint
QT interval and ventricular arrhythmias called torsades position can decrease ventilation and CO, which
de pointes. Sudden death has been associated with left together can lead to death in a subject who is at risk.
ventricular hypertrophy on autopsy—a condition Physical restraint has been identified as a powerful
known to give a predisposition to ventricular arrhyth- contributor to death in subjects who are agitated and in
mias. As a group, these potential underlying causes of excited states.72 A recent article reviewed 38 sudden
SCD have been associated primarily with the induction deaths during restraint by Dutch police over a 12-
of ventricular tachycardia or ventricular fibrillation year period. The causes of death in these cases were
and not with PEA or asystole, which are most often deemed as multifactorial. However, 94.7% of subjects
identified in cases of restraint cardiac arrest. Taken were noted in the prone body position, and 76.3% of
together, results from several case series revealed that subjects received thoracic pressure.73 The clear associ-10 Medicine, Science and the Law 0(0)
most likely due to metabolic acidosis exacerbated by 11. Judiciary. Regulation 28: prevention of future deaths
inadequate ventilation and a decrease in CO. These report: Michael James Sweeney, www.judiciary.uk/wp-
physiologic derangements can lead to a PEA or asys- content/uploads/2016/03/Sweeney-2013-0236.pdf
tolic cardiac arrest. These deaths have been tradition- (September 2013, accessed 21 January 2021).
12. Judiciary. Regulation 28: prevention of future deaths
ally attributed to “positional asphyxia.” However,
report: Duncan Tomlin, www.judiciary.uk/wp-content/
given the associated metabolic and physiologic
uploads/2019/06/Duncan-TOMLIN-2019-0135_
changes, the findings reviewed here lead to the conclu- Redacted.pdf (December 2019, accessed 21 January
sion that death in this setting might be more aptly 2021).
described as “prone restraint cardiac arrest.” 13. Meng A-Y. Ormrod Lecture October 2019: police
Sedation, de-escalation, ensuring minimal time in restraint – causes of death. Med Sci Law 2020; 60:
restraint, and overall avoidance of the prone position 227–233.
in cases of acute behavioral disturbances may serve to 14. Shkrum MJ and Ramsay DA. Asphyxia. In: Forensic
prevent prone restraint cardiac arrest in highly vulner- pathology of trauma: common problems for the patholo-
able subjects. gist. Totowa: Humana Press, 2007, pp.65–66.
15. Tumran NK, Ambade VN and Dixit PG. Compression
asphyxia in upright suspended position. Am J Forensic
Declaration of conflicting interests
Med Pathol 2014; 35: 80–82.
The author has been a paid medicolegal consultant and 16. Savaser D and Chan TC. Positional and restraint
expert witness in cases of prone restraint cardiac death. No asphyxia. In: Ross D and Vilke G (eds) Guidelines
other relevant potential financial conflicts of interest. for investigating officer-involved shootings, arrest-related
deaths, and deaths in custody. New York and
Funding London: Routledge, Taylor & Francis Group, 2017, pp.
The author received no financial support for the research, 149–162.
authorship and/or publication of this article. 17. Michaud A. Restraint related deaths and excited delirium
syndrome in Ontario (2004–2011). J Forensic Leg Med
ORCID iD 2016; 41: 30–35.
18. Independent Advisory Panel on Deaths in Custody.
Alon Steinberg https://orcid.org/0000-0001-8705-2599
Report of the cross-sector restraint workshop held in
May 2010.
References 19. Hall C, Votova K, Heyd C, et al. Restraint in police use
1. Reay DT, Fligner CL, Stilwell AD, et al. Positional of force events: examining sudden in custody death for
asphyxia during law enforcement transport. Am J prone and not-prone positions. J Forensic Leg Med 2015;
Forensic Med Pathol 1992; 13: 90–97. 31: 29–35.
2. Bell MD, Rao VJ, Wetli CV, et al. Positional asphyxia- 20. Ross DL and Hazlett MA. A prospective analysis of the
tion in adults. Am J Forensic Med Pathol 1992; 13: outcomes of violent prone restraint incidents in policing.
101–107. Forensic Res Criminol Int J 2016; 2: 16–24.
3. Belviso M, De Donno A, Vitale L, et al. Positional 21. Di Maio TG and Maio VJ. Excited delirium syndrome
asphyxia. Am J Forensic Med Pathol 2003; 24: 292–297. cause of death and prevention. 1st ed. Boca Raton, FL:
4. OʼHalloran RL and Lewman LV. Restraint asphyxiation Taylor & Francis, 2006, pp.7–31, 35–37.
in excited delirium. Am J Forensic Med Pathol 1993; 14: 22. Barnett R, Stirling C and Pandyan AD. A review of the
289–295. scientific literature related to the adverse impact of phys-
5. O’Halloran RL and Frank JG. Asphyxial death during ical restraint: gaining a clearer understanding of the phys-
prone restraint revisited. Am J Forensic Med Pathol 2000; iological factors involved in cases of restraint-related
21: 39–52. death. Med Sci Law 2012; 52: 137–142.
6. Stratton SJ, Rogers C, Brickett K, et al. Factors associ- 23. Levitsky M. Pulmonary physiology. 4th ed. New
ated with sudden death of individuals requiring restraint York: McGraw Hill, 1995. pp.14–17, 44–45, 163–182,
for excited delirium. Am J Emerg Med 2001; 19: 187–191. 226–232.
7. Pollanen MS, Chiasson DA, Cairns JT, et al. Unexpected 24. Chan TC, Neuman T, Clausen J, et al. Weight force
death related to restraint for excited delirium: a retro- during prone restraint and respiratory function. Am J
spective study of deaths in police custody and in the com- Forensic Med Pathol 2004; 25: 185–189.
munity. CMAJ 1998; 158: 1603–1607 25. Michalewicz BA, Chan TC, Vilke GM, et al. Ventilatory
8. Kunz S, Pordardottir S and Runarsdottir R. Restraint- and metabolic demands during aggressive physical
related asphyxia on the basis of a drug-induced excited restraint in healthy adults. J Forensic Sci 2007; 52:
delirium. Forensic Sci Int 2018; 288: e5–e9. 171–175.
9. Aiken F, Duxbury J and Dale C. Deaths in custody: role 26. Sloane C, Chan TC, Kolkhorst F, et al. Evaluation of the
of restraint. Learn Disabil Q 2011; 2: 178–190. ventilatory effects of the prone maximum restraint
10. Huether J. The inquest into the death of Stephanie Jobin. (PMR) position on obese human subjects. Forensic Sci
OACAS J 2003; 47. Int 2014; 237: 86–89.Steinberg 11
27. Roeggla G, Roeggla H, Moser B, et al. Cardiorespiratory 45. Varat M, Fowler N and Adolph RJ. Cardiac output
consequences of the hobble restraint. Acad Emerg Med response to exercise in patients with inferior vena caval
1999; 6: 1076–1077. ligation. Circulation 1970; 42: 445–453.
28. Chan TC, Vilke GM, Neuman T, et al. Restraint position 46. Higashi H, Yoshii T, Inaba S, et al. Life-threatening
and positional asphyxia. Ann Emerg Med 1997; 30: shock due to inferior vena cava filter thrombosis. Hear
578–586. lung Vessel 2015; 7: 263–265.
29. Vilke GM, Chan TC, Neuman T, et al. Spirometry in 47. Savaser DJ, Campbell C, Castillo EM, et al. The effect of
normal subjects in sitting, prone and supine positions. the prone maximal restraint position with and without
Respir Care 2000; 45: 407–410. weight force on cardiac output and other hemodynamic
30. Cary NRB, Roberts CA, Cummin ARC, et al. The effect measures. J Forensic Leg Med 2013; 20: 991–995.
of simulated restraint in the prone position on cardiore- 48. Pump B, Talleruphuus U, Christensen NJ, et al. Effects
spiratory function following exercise in humans. of supine, prone, and lateral positions on cardiovascular
J Physiol 2000; 525: 30P–31P. and renal variables in humans. Am J Physiol Integr Comp
31. Parkes J. Sudden death during restraint: do some posi- Physiol 2002; 283: R174–R180.
tions affect lung function? Med Sci Law 2008; 48: 49. Ho JD, Dawes DM, Moore JC, et al. Effect of position
137–141. and weight force on inferior vena cava diameter – impli-
32. Meredith C, Taslaq S, Kon OM, et al. The cardiopulmo- cations for arrest-related death. Forensic Sci Int 2011;
nary effects of physical restraint in subjects with chronic 212: 256–259.
obstructive pulmonary disease. J Clin Forensic Med 2005; 50. Krauskopf A, Mayerhoefer M, Oberndorfer F, et al.
12: 133–136. Does weight force application to the lower torso have
33. Barnett R, Hanson P, Stirling C, et al. The physiological an influence on inferior vena cava and cardiovascular
impact of upper limb position in prone restraint. Med Sci parameters? Am J Emerg Med 2008; 26: 603–607.
Law 2013; 53: 161–165. 51. Backofen JE. Hemodynamic changes with prone position
34. West JB and Luks A. Respiratory physiology: the essen- during general anesthesia. Anesth Analg 1985; 64:
tials. 10th ed. Philadelphia: Wolters Kluwer Health, 2016, 194–194.
pp.132, 98–100, 162–164. 52. Sudheer PS, Logan SW, Ateleanu B, et al.
35. Bruscasco V, Crapo R, Virgo G, et al. ATS/ERS Task Haemodynamic effects of the prone position: a compar-
Force: standardization of lung function Testing. Eur ison of propofol total intravenous and inhalation anaes-
Respir J 2005; 26: 720–735. thesia. Anaesthesia 2006; 61: 138–141.
36. Kroll MW, Still GK, Neuman TS, et al. Acute forces 53. Yokoyama M, Ueda W, Hirakawa M, et al.
required for fatal compression asphyxia: a biomechanical Hemodynamic effect of the prone position during anes-
model and historical comparisons. Med Sci Law 2017; 57: thesia. Acta Anaesthesiol Scand 1991; 35: 741–744.
61–68. 54. Edgcombe H, Carter K and Yarrow S. Anaesthesia in the
37. Knoll MW, Brave MA, Kleist SR, et al. Applied force prone position. Br J Anaesth 2008; 100: 165–183.
during prone restraint. Is officer weight a factor? Am H 55. Jette M, Sidney K and Blümchen G. Metabolic equiva-
Forensic Med Pathol 2019; 40: 1–7. lents (METS) in exercise testing, exercise prescription,
38. McArdle WD, Katch FI and Katch VL. Exercise physi- and evaluation of functional capacity. Clin Cardiol
ology: nutrition, energy, and human performance. 1990; 13: 555–565.
Baltimore: Wolters Kluwer Health, 2015, pp.200, 264, 56. Robergs RA, Ghiasvand F and Parker D. Biochemistry
286–301, 337. of exercise-induced metabolic acidosis. Am J Physiol
39. Munshi L, Del Sorbo L, Adhikari NKJ. Prone Integr Comp Physiol 2004; 287: R502–R516.
position for acute respiratory distress syndrome. A sys- 57. Ho JD, Dawes DM, Nelson RS, et al. Acidosis and cat-
tematic review and meta-analysis. Ann Am Thorac Soc echolamine evaluation following simulated law enforce-
2017; 14. ment ‘use of force’ encounters. Acad Emerg Med 2010;
40. Guerin C, Reignier J, Richard J-C, et al. Prone position- 17: e60–e68.
ing in severe acute respiratory distress syndrome. N Engl 58. Hick JL, Smith SW and Lynch MT. Metabolic acidosis in
J Med 2013; 368: 2159–2168. restraint-associated cardiac arrest. A case series. Acad
41. Gattinoni L and Caironi P. Prone positioning beyond Emerg Med 1999; 6: 239–243.
physiology. Anesthesiology 2010; 113: 1262–1264. 59. Halliwill JR, Sieck DC, Romero SA, et al. Blood pressure
42. Petersson J, Ax M, Frey J, et al. Positive end-expiratory regulation X: what happens when the muscle pump is
pressure redistributes regional blood flow and ventilation lost? Post-exercise hypotension and syncope. Eur J Appl
differently in supine and prone humans. Anesthesiology Physiol 2014; 114: 561–578.
2010; 113: 1361–1369. 60. Van Hooren B and Peake JM. Do we need a cool-down
43. Ross J and Braunwald E. Studies on Starling’s law of the after exercise? A narrative review of the psychophysiolog-
heart. Circulation 1964; 30: 719–727. ical effects and the effects on performance, injuries and
44. Sackner MA, Schnabel TG and Lewis DH. Effect of the long-term adaptive response. Sports Med 2018; 48:
restriction of venous return on the hemodynamics of 1575–1595.
normal persons and patients with congestive heart fail- 61. Neumar RW, Otto CW, Link MS, et al. American Heart
ure. Am J Cardiol 1964; 13: 782–789. Association guidelines for cardiopulmonary resuscitation12 Medicine, Science and the Law 0(0)
and emergency cardiovascular care. Part 8: Adult 70. Chan PS, McNally B, Tang F, et al. Recent trends in
advanced cardiovascular life support. Circulation 2010; survival from out-of-hospital cardiac arrest in the
122: S729–767. United States. Circulation 2014; 130: 1876–1882.
62. Fabre A, Shepard MN. Sudden adult death syndrome 71. Nolan JP, Laver SR, Welch CA, et al. Outcome following
and other non-ischaemic causes of sudden cardiac admission to UK intensive care units after cardiac arrest:
death. Heart 2006 Mar; 92(3):316–320 a secondary analysis of the ICNARC Case Mix
63. Neuman T. Positional and restraint asphyxia. In: Ross Programme Database. Anaesthesia 2007; 62: 1207–1216.
DL and Chan TC (eds) Sudden deaths in custody.1st ed. 72. Strommer EM, Leith W and Zeegers MP The role of
Totowa: Humana Press, 2006, pp.39–57. restraint in fatal excited delirium: a research synthesis
64. Krexi L, Georgiou R, Krexi D, et al. Sudden cardiac and pooled analysis. Forensic Sci Med Pathol 2020; 16:
death with stress and restraint: the association with 680–692.
sudden adult death syndrome, cardiomyopathy and cor- 73. Dijkhuizen LG, Kubat B and Duijst WL. Sudden death
onary artery disease. Med Sci Law 2016; 56: 85–90. during physical restraint by the Dutch police. J Forensic
65. Otahbachi M, Cevik C and Baghure S. Excited delirium, Leg Med 2020; 72: 101966.
restraints, and unexpected death. A review of pathogen- 74. The Royal College of Emergency Medicine Best Practice
esis. Am J Forensic Med Pathol 2010; 31: 107–112. Guideline. Guidelines for the management of excited
66. Fabre A and Sheppard MN. Sudden adult death syn- delirium/acute behavioural disturbance (ABD), https://
drome and other non-ischaemic causes of sudden cardiac www.rcem.ac.uk/docs/College%20Guidelines/5p.%
death. Heart 2006; 92: 316–320. 20RCEM%20guidelines%20for%20management%20of
67. Behr ER, Dalageorgou C, Christiansen M, et al. Sudden %20Acute%20Behavioural%20Disturbance%20(May%
arrhythmic death syndrome: familial evaluation identifies 202016).pdf (May 2016, accessed 21 January 2021).
inheritable heart disease in the majority of families. Eur 75. College of Paramedics. Position statement – management
Heart J 2008; 29: 1670–1680. of acute behavioural disturbance, https://www.collegeof
68. Kroll MW, Walcott GP and Ideker RE. The stability of paramedics.co.uk/COP/News/Statements%20and%
electrically induced ventricular fibrillation. In: 34th 20Consultations/COP/News/Statements_and_consulta
Annual International Conference of IEEE EMBS, San tions.aspx (October 2018, accessed 21 January 2021).
Diego, CA, 28 August–1 September 2012. New York: 76. Dame Elish Angiolini DBE QC. Report of the indepen-
IEEE Press, 2012. dent review of deaths and serious incidents in police cus-
69. Truhlar A, Deakin CD, Soar J, et al. European tody, https://assets.publishing.service.gov.uk/
Resuscitation Council guidelines for resuscitation 2015: government/uploads/system/uploads/attachment_data/
Section 4. Cardiac arrest in special circumstances. file/655401/Report_of_Angiolini_Review_ISBN_
Resuscitation 2015; 95: 147–200. Accessible.pdf (January 2017, accessed 21 January 2021).You can also read