R4R: Mental Health Awareness Training: Spotlight on Schizophrenia - Janssen ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
R4R: Mental Health
Awareness Training:
Spotlight on Schizophrenia
Static
Adverse events should be reported. Reporting forms and information can be found
at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google
Play or Apple App Store. Adverse events should also be reported to Janssen-Cilag
Limited on 01494 567447 or at dsafety@its.jnj.com.
This programme has been organised
Item code: PHGB/MEDed/0418/0020b and funded by Janssen.
Date of preparation: June 2018
Welcome to Module 3: Side Effect Observation and Management
Online Training Module
This series of modules on mental health awareness with a spotlight on schizophrenia have
been specifically developed for primary care nurses. This module aims to educate nurses on
the possible side effects of antipsychotic medication and enables them to recognise, manage
and monitor these.
This module has been sponsored and developed by Janssen-Cilag Limited, and has been
designed to benefit you, your team and your patients. The content has been written by Louise
Saxton RMN, Mental Health Clinical Nurse Specialist and Mednet Ltd.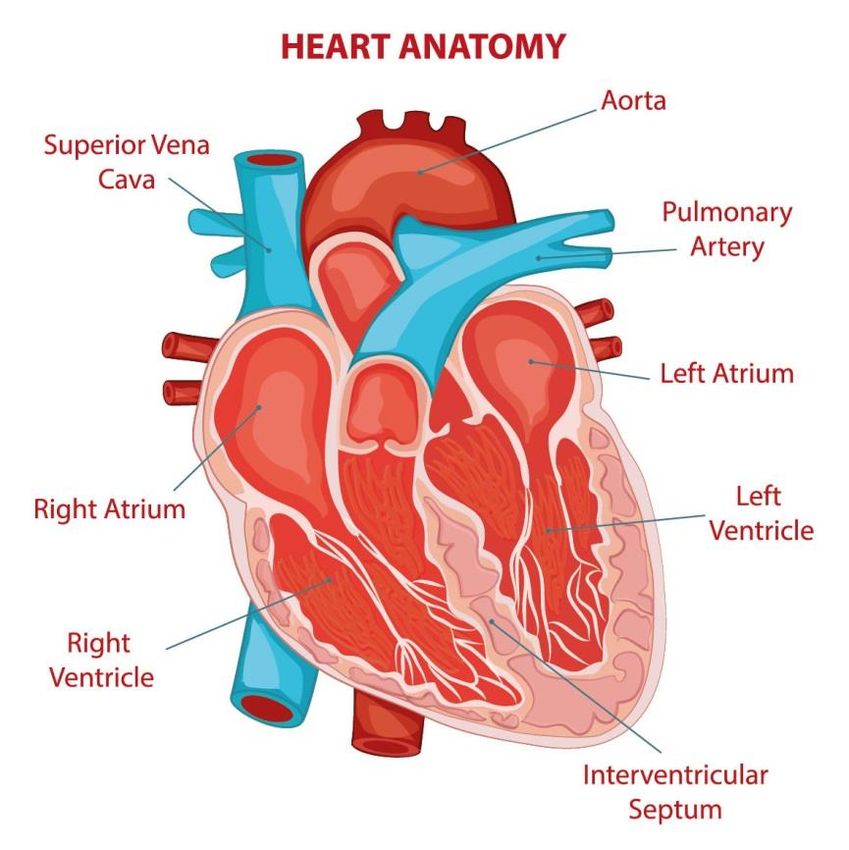
Module 3: Side Effect Observation and Management

Module aims
By the end of this module, you will:
• Have increased your awareness of commonly available first generation and second generation
antipsychotic medication.
• Be able to define key antipsychotic drug side effects and describe the impact that these may have on
patients affected by them.
• Have developed a working knowledge of the drug specific side effect indications of commonly
available antipsychotic medication.
• Understand the importance of monitoring physical health for patients receiving treatment for
schizophrenia.
• Be able to identify and apply key assessment tools for side effect management in patients receiving
treatment for schizophrenia.
Which antipsychotic medications and side effects are you aware of?

Commonly available antipsychotic medication
FIRST GENERATION SECOND GENERATION
Chlorpromazine Hydrochloride Amisulpride
Flupentixol Decanoate Aripiprazole
Fluphenazine Decanoate Aripiprazole Long Acting Injection
Haloperidol Clozapine
Haloperidol Decanoate Lurasidone Hydrochloride
Pimozide Olanzapine
Prochlorperazine Olanzapine Pamoate
Sulpiride Paliperidone Palmitate
Trifluoperazine Hydrochloride Paliperidone Palmitate 3-monthly
Zuclopenthixol Decanoate Quetiapine
Zuclopenthixol Acetate Risperidone
Risperidone Long Acting Injection
National Institute for Health and Care Excellence (2018) British National Formulary: Psychoses and related disorders. Advice of Royal College of Psychiatrists on doses of
antipsychotic drugs above BNF upper limit. [Internet] Available from: https://bnf.nice.org.uk/treatment-summary/psychoses-and-related-disorders.html [Accessed May 2018].
Extrapyramidal side effects
• The first antipsychotic drug was discovered
serendipitously in the early 1950s (first generation drugs).
It was soon realised that, as well as antipsychotic actions,
such drugs produce motor side effects reminiscent of
Parkinson’s disease.1
• In the 1960s, it started to be understood that these
medications act by blocking receptors for the neuro-
transmitter dopamine.1
• Common understanding assumed a single receptor type –
the dopamine D2 receptor - was responsible for both the
antipsychotic main effect, and the motor side effects.1
• However, there are indications that first generation drugs
act indirectly, with dopamine D1 receptors (and others)
as possible ultimate targets.1
1. Miller R. (2009) Mechanisms of action of antipsychotic drugs of different classes, refractoriness to therapeutic effects of classical neuroleptics, and individual variation in sensitivity
to their actions: Part 1. Current Neuropharmacology. 11(7); 3012-314.
Dystonia (uncontrolled muscular spasms)
Muscle spasm in any part of the body,
e.g.
• Eyes rolling upwards (oculogyric crisis)
• Head and neck twisted to the side View this video here:
(torticollis)
https://www.youtube.com/watch?v=Gjiy1rDZpp8
• The patient may be unable to swallow
or speak clearly
• In extreme cases the back may arch or
the jaw may dislocate
• Acute dystonia can be both painful and
very frightening.1
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg91.
2. Psychiatry Teacher (2009) Acute dystonia [Internet]. Available at: https://www.youtube.com/watch?v=Gjiy1rDZpp8 [Accessed June 2018].
Pseudoparkinsonism
• Tremor and/or rigidity
• Bradykinesia (decreased facial
expression, flat monotone voice, slow
body movements, inability to initiate
movement) View this video here:
• Bradyphrenia (slowed thinking) https://www.youtube.com/watch?v=bC6SR-qn90A
• Salivation
• Pseudoparkinsonism can be mistaken
for depression or the negative symptoms
of schizophrenia.1
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg91.
2. Amin, O.S.M. & Shwani, S.S. (2011) Drug-induced Parkinsonism Osama SM Amin FACP & Sa'ad S Shwani MD, [Internet]. Available from:
https://www.youtube.com/watch?v=bC6SR-qn90A [Accessed June 2018].
Akathisia
A subjectively unpleasant state of inner restlessness where there is a strong desire or compulsion to move
e.g.:
• Foot stamping when seated
• Constantly crossing/uncrossing legs
• Rocking from foot to foot View this video here:
• Constantly pacing up and down https://www.youtube.com/watch?v=DKNtv1LPSEM
• Akathisia can be mistaken for psychotic
agitation and has been linked with suicidal
ideation and aggression towards others.1
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg91.
2. PsychScene Hub (2018) Antipsychotic Medication Induced Akathisia - EPSE. [Internet] Available from: https://www.youtube.com/watch?v=DKNtv1LPSEM [Accessed August
2018].Tardive dyskinesia
A wide variety of movements can occur
such as:
• Lip smacking or chewing
• Tongue protrusion (fly catching)
• Choreiform hand movements (pill rolling
or piano playing) View this video here:
• Pelvic thrusting https://www.youtube.com/watch?v=Qf3I6t8fuA8
• Severe orofacial movements can lead to
difficulty speaking, eating or breathing
• Movements are worse when under
stress.1
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg91.
2. Minkecantrell45 (2012) Tardive Dyskinesia [Internet] Available from: https://www.youtube.com/watch?v=Qf3I6t8fuA8 [Accessed June 2018].Cardiac problems
ECG changes: QTc prolongation
Many psychotropic drugs are associated with ECG changes and some are causally linked to serious
ventricular arrhythmia and sudden cardiac death.1 Specifically they are linked to prolongation of the
cardiac QT interval (QTc), a risk factor for ventricular arrhythmia, which is often fatal.1
Table 1: Effects of antipsychotics on QTc1
No effect Low effect Moderate effect High effect Unknown effect
Brexpiprazole* Aripiprazole† Prochlorperazine Amisulpride§ Any intravenous antipsychotic Pipothiazine
Cariprazine* Asenapine Olanzapine‡ Chlorpromazine Pimozide Trifluoperazine
Lurasidone Clozapine Paliperidone Haloperidol Sertindole Zuclopenthixol
Flupentixol Risperidone Iloperidone Any drug or combination of
Fluphenazine Sulpiride Levomepromazine drugs used in doses exceeding
Loxapine Melperone recommended maximum
Perphenazine Quetiapine
Ziprasidone
* Limited clinical experience (association with QT prolongation may emerge). † One case of torsades de pointes (TDP) reported, two cases
of QT prolongation and an association TDP found in database study. Recent data suggest aripiprazole causes QTc prolongation of around
8ms. Aripiprazole may increase QT dispersion. ‡ Isolated cases of QTc prolongation and has effects on cardiac ion channel, Ikr, other data
suggest no effect on QTc. § TDP common in overdose; strong association with TDP in clinical doses.
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg.112.
Table 1: Adapted from Table 1.24, p.114, Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell.Sedation
Sedation
Key Drug Sedation incidence
+++ High incidence/ Amisulpride -
severity
++ moderate
Aripiprazole -
+ low Clozapine +++
- very low Flupentixol +
Fluphenazine +
Haloperidol +
Lurasidone +
Olanzapine ++
Paliperidone +
Quetiapine ++
Risperidone +
Zuclopenthixol ++
Adapted from Table 1.8, p.39, Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell.Weight gain
Weight gain
• The mechanisms underlying weight gain and other adverse metabolic events in patients
receiving antipsychotics for psychosis remain unclear.1
• For instance, the weight gain induced by second generation drugs is often centrally
distributed, and presents itself most obviously as an increase in waist circumference
measurement.1
• This central obesity is closely associated with insulin resistance and metabolic
syndrome, which increases the risk of developing cardiovascular disease among other
serious health conditions.1
• Aripiprazole is associated with the lowest increases of metabolic risk factors, whilst
olanzapine and clozapine are associated with the highest.1
1. Richards, D.B. & Bressington, D. (2015) Understanding antipsychotic-induced weight gain and other metabolic issues. British Journal of Mental Health Nursing. 4(4); 157-166.Drugs that contribute to weight gain
High risk of weight gain Clozapine
Olanzapine
Moderate risk of weight gain Chlorpromazine
Quetiapine
Risperidone
Paliperidone
Low risk of weight gain Amisulpride
Aripiprazole
Haloperidol
Loxapine
Sulpiride
Trifluoperazine
Zuclopenthixol
Adapted from Table 1.8, p.39, Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell.Metabolic syndrome Adapted from Table 2, p.81 Han, T.S. & Lean, M.E.J. (2015) Metabolic syndrome. Medicine. 43(2); 80-87.
Metabolic syndrome
• The prevalence of metabolic syndrome varies across countries and psychiatric
populations, and its development can be very rapid.1
• The prevalence among patients diagnosed with schizophrenia is around 40% and
around 32% for patients diagnosed with bipolar disorder.2
• Women tend to present with increased rates compared with men, and some ethnic
groups, such as black Africans and Hispanics show a possible predisposition to the
condition.1
• Most authors emphasise the importance of extrinsic factors (antipsychotic medication,
increased calorie intake, sedentary lifestyle) in its development, however the concept of
intrinsic factors being implicated (genetic links between schizophrenia and diabetes) is
also supported.1
1. Papanastasiou, E. (2013) The prevalence and mechanisms of metabolic syndrome in schizophrenia: a review. Therapeutic Advances in Psychopharmacology. 3(1); 33-51.
2. Malhotra, N., et al. (2013) A prospective, longitudinal study of metabolic syndrome in patients with bipolar disorder and schizophrenia. Journal of Affective Disorders. 150(2);
653-658.Diabetes
Diabetes
• Schizophrenia is associated with relatively high rates of insulin resistance and diabetes,
an observation that predates the discovery and widespread use of antipsychotics.1
• The mechanisms involved in the development of antipsychotic-related diabetes are
unclear, but may include 5-HT2A/ 5-HT2C antagonism, increased plasma lipids, weight
gain and leptin resistance.1
• Insulin resistance may occur in the absence of weight gain.1
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg.123Hyperprolactinaemia
Hyperprolactinaemia
• Dopamine inhibits prolactin release and so dopamine antagonists can be expected to increase
prolactin plasma levels. The degree of prolactin elevation is probably dose-related, and for
antipsychotic medications the threshold activity (D₂ occupancy) for increased prolactin is very close
to that of therapeutic efficacy.1
• Hyperprolactinaemia is often superficially asymptomatic. Nonetheless, persistent elevation of plasma
prolactin is associated with following symptoms: sexual dysfunction, menstrual disturbances, breast
growth and galactorrhoea and may include delusions of pregnancy. Long-term adverse
consequences are reductions in bone mineral density and a possible increase in the risk of breast
cancer.1
• Prolactin-elevating drugs with high risk should, if possible, be avoided in the following patient
groups:
- Patients under 25 years of age (i.e. before peak bone mass)
- Patients with osteoporosis
- Patients with a history of hormone-dependent breast cancer
- Young women1
1. Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell. pg.137Effects of antipsychotic medication on prolactin concentration
Prolactin-sparing Prolactin-elevating Prolactin-elevating
(prolactin increase very rare) (low risk; minor changes only) (high risk; major changes)
Aripiprazole Lurasidone Amisulpride
Asenapine Olanzapine Paliperidone
Brexpiprazole* Ziprasidone Risperidone
Cariprazine* Sulpiride
Clozapine FGAs (e.g. haloperidol and
chlorpromazine)
Iloperidone*
Quetiapine
*Not available in the EU at the time of writing.
FGA, first-generation antipsychotic.
Adapted from Table 1.33, p.137, Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed. Chichester: Wiley Blackwell.Comparing side effects of antipsychotic medication
Comparing side effects of antipsychotic medication
Drug Akathisia Weight gain Sedation Anti Hypo- Prolactin
cholinergic tension elevation
Aripiprazole + - - - - -
Flupentixol ++ ++ + ++ + +++
Fluphenazine ++ + + ++ + +++
Haloperidol +++ + + + + ++
Olanzapine - +++ ++ + + +
Paliperidone + ++ + + ++ +++
Risperidone + ++ + + ++ +++
Zuclopenthixol ++ ++ ++ ++ + +++
Key
+++ High incidence/
severity
++ Moderate
+ Low
Adapted from Table 1.8, p.39, Taylor, D., Barnes, M. & Young, A. (2018) The Maudsley Prescribing Guidelines in Psychiatry. 13th Ed.
- Very low Chichester: Wiley Blackwell.Physical health awareness
Side effects and physical health awareness
• Life expectancy for people with severe mental illnesses can be up to 15 years less for men and 13
years less for women compared to the general population.1
• The additional deaths were historically attributed to suicide and accidents, but these, in actuality,
account for only a small part of the excess mortality. 1 Most of the excess comes from comorbid
physical illness.1
• Nevertheless, the message is not that medication is bad: antipsychotics, used thoughtfully to
effectively treat mental health and ‘keeping the body in mind’, could be seen as part of mortality
reduction strategies.1
• Given that antipsychotics, other than clozapine, show little difference in efficacy but can vary
markedly in side effect profile, choice will often be governed by side effects.2
• RCTs often report “dropouts” due to side effects, but lack of knowledge, skills, or management
strategies to cope with side effects may be most relevant in dictating adherence behaviours.2
• Systematic physical health monitoring is necessary to ensure prevention of and early intervention
for physical comorbidities.1
• Awareness of modifiable risk factors, effective and mindful treatment of psychosis and earlier
detection of physical illness all play a role in reducing morbidity and mortality.1
1. Moore, S., et al. (2015) Promoting physical health for people with schizophrenia by reducing disparities in medical and dental care. Acta Psychiatrica Scandinavica. 132(2); 109-121.
2. Haddad, P., Brain, C. & Scott, J. (2014) Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Related Outcome Measures.
5; 43-62.‘No mental health without physical health as well’1
• NICE guidelines recommend that adults with psychosis or schizophrenia should have a regular
health check (at least once a year) that includes taking weight, waist, pulse and blood pressure
measurements and blood tests.1
• The WHO has suggested a change to its original statement of ‘no health without mental health’ to ‘no
mental health without physical health as well’, with a particular focus on improving services for
physical health in people with schizophrenia.2
• The WHO Comprehensive Mental Health Action Plan advises the development of policy to improve
the physical and mental health of people with mental illnesses, with a particular focus on improving
access to good quality physical healthcare services.2,3
• A freely available independent website called choice and medication www.choiceandmedication.org
has been devised to ensure people with mental illness have access to information regarding the
advantages and disadvantages of any treatment options available.
1. National Institute of Health and Care Excellence (2014) Psychosis and schizophrenia in adults: prevention and management. NICE clinical guideline [CG178] [Internet] Available from:
https://www.nice.org.uk/guidance/cg178 [Accessed June 2018].
2. Moore, S., et al. (2015) Promoting physical health for people with schizophrenia by reducing disparities in medical and dental care. Acta Psychiatrica Scandinavica. 132(2); 109-121.
3. World Health Organization (2013) Mental health action plan 2013–2020. [Internet] Available from:
http://apps.who.int/iris/bitstream/handle/10665/89966/9789241506021_eng.pdf;jsessionid=6DEF54B5797073D5AAAADEF4F474BCC7?sequence=1 [Accessed June 2018].Assessing and monitoring side effects
• Managing side effects that emerge during treatment
depends on their detection at review appointments.1
• If patients have a good therapeutic alliance with the
clinical team, particularly the prescriber, then they
are more likely to volunteer side effects.1
• The use of a simple checklist can also aid the
detection of side effects.1
1. Haddad, P., Brain, C. & Scott, J. (2014) Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Related Outcome
Measures. 5; 43-62.Monitoring side effects
• The Simpson Angus Scale (SAS)
• Barnes Akathisia Rating Scale (BARS)
Extrapyramidal Side Effects
• Abnormal Involuntary Movement Scale
(EPS)
(AIMS)
Tardive Dyskinesia (TD)
• The Liverpool University Neuroleptic Side
Effect Rating Scale (LUNSERS)
Side effect
• BMI & Waist Measurement
monitoring Weight Gain
• Abnormal Lipids
LUNSERS/
• Electrocardiogram (ECG)
GASS*
Cardiac • Blood Pressure (BP)
• Total Protein Test (TP)
Diabetes
• Fasting Blood Glucose Test (FBG)
Glucose Intolerance
Hyperprolactinaemia • Serum Prolactin Level
* Liverpool University Neuroleptic Side Effects Scale (LUNSERS); Glasgow Antipsychotic Side‐effect Scale (GASS)Assessment tools
Liverpool University Neuroleptic Side Effects Scale (LUNSERS)
• The test consists of 41 self-report, tick box questions with a predefined scale from "not at
all" to "very much”.1
Glasgow Antipsychotic Side effects Scale (GASS)
A self-report scale which can aid systematic clinical assessment, particularly in view of its
brevity and user-friendly language.2
https://www.janssenmedicalcloud.co.uk/sites/www.janssenmedicalcloud.co.uk/files/gass-
file.pdf
Simpson and Angus Scale (SAS)
• A parkinsonism scale with a high degree of validity and straightforward for multi-
disciplinary staff to perform.3
http://keltymentalhealth.ca/sites/default/files/SAS.pdf
1. Day J.C. et al. (1995) A self-rating scale for measuring neuroleptic side-effects. Validation in a group of schizophrenic patients. British Journal of Psychiatry.166; 650-653.
2. Waddell, L. & Taylor, M. (2008) A new self-rating scale for detecting atypical or second-generation antipsychotic side effects. Journal of Psychopharmacology. 22(3); 238-243.
3. Knol W. et al. (2009) Validity and reliability of the Simpson-Angus Scale (SAS) in drug induced parkinsonism in the elderly. International Journal of Geriatric psychiatry. 24(2); 183-189.Assessment tools
Barnes Akathisia Scale (BARS)
• A physician administered rating tool used to assess the severity of drug induced
akathisia.1
https://outcometracker.org/library/BAS.pdf
Abnormal Involuntary Movement Scale (AIMS)
• A reliable and valid scale used to evaluate dyskinesia, this scale is of increased
importance given the correlation between abnormal involuntary movement and
increased adolescent risk of psychosis.2
http://www.cqaimh.org/pdf/tool_aims.pdf
Serum Prolactin Level
• A test used to determine the presence of abnormally high levels of prolactin in the blood.
Normal levels are less than 25 ng/mL for women, and less than 15 ng/mL for men.3
1. Barnes, T. R. (1989) A Rating Scale for Drug-Induced Akathisia. British Journal of Psychiatry. 154; 672-676.
2. Kindler, J., et al. (2016) Abnormal involuntary movements are linked to psychosis-risk in children and adolescents: Results of a population-based study. Schizophrenia Research. 174
(1-3); 58-64.
3. Goldberg, J. and Jewell, T. (2016) Prolactin Level Test: Normal Results [Internet] Available from: http://www.healthline.com/health/prolactin#Overview1 [Accessed June 2018].You can also read