Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal on Ageing in Developing Countries, 2020, 5 (2): 130-145
Reliability and factor structure of the mini-
mental state examination (MMSE) among
older adults in Jamaica
Kenneth James1, Camelia Thompson2, Desmalee Holder
Nevins3, Cameal Chin-Bailey4, Douladel Willie-Tyndale5,
Julian McKoy Davis6, and Denise Eldemire-Shearer7
Abstract. The Mini-Mental Status Examination is the most commonly used and widely applied
test for assessment of cognitive impairment and memory problems. This paper examines
reliability-related characteristics and factor structure of the MMSE tool in older persons (age 60
years and over) in a Caribbean country, Jamaica. In 2012, a nationally represented sample of 2943
persons aged ≥60 years were selected using a two-stage cluster sampling technique. MMSE
screening tool was administered to eligible participants (2742) to assess cognitive function.
Reliability analysis was performed generating inter-item, item-total correlations and
standardized Cronbach’s alpha values. Exploratory factor analysis elucidated the factor structure
of the MMSE instrument. The variation of factor score (composite sub-test scores) with MMSE
score was also examined. The Cronbach’s alpha coefficient of the MMSE instrument was 0.742,
and item-total correlations varied from 0.2 to 0.5. On factor analysis, three factors (‘executive
functioning,’ ‘memory’ and ‘attention’) were extracted, which accounted for 32.9% of the total
variance in MMSE scores. The variation of factor scores with total MMSE score revealed pattern
suggesting that sensitivity of the instrument pivots around MMSE score 18. The MMSE is
considered as a reliable instrument for this study and has a three-factor structure. The 3-factor
structure parallels recognized dimensions of neurocognitive ability. The established factor
structure provides context and understanding, which can aid clinicians and researchers in
interpreting data obtained from the use of the MMSE.
Keywords: reliability, factor analysis, Jamaica.
1 Department of Community Health and Psychiatry, The University of the West Indies, Mona, Jamaica
2 Department of Community Health and Psychiatry, The University of the West Indies, Mona, Jamaica
(camelia.thompson@uwimona.edu.jm)
3 Department of Community Health and Psychiatry, The University of the West Indies, Mona, Jamaica
4 Department of Community Health and Psychiatry, The University of the West Indies, Mona, Jamaica
5 Mona Ageing and Wellness Centre, The University of the West Indies, Mona, Jamaica
6 Mona Ageing and Wellness Centre, The University of the West Indies, Mona, Jamaica
7 Mona Ageing and Wellness Centre, The University of the West Indies, Mona, Jamaica
130Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
Abstracto. El Examen del Estado Mini-Mental (EEMM) es la prueba más común y
ampliamente utilizada para evaluar el deterioro cognitivo y los problemas de memoria.
Este documento examina las características relacionadas con la confiabilidad y la
estructura de factores de la herramienta EEMM en personas mayores (de 60 años o más)
en el país caribeño, Jamaica. En 2012, se seleccionó una muestra representada a nivel
nacional de 2943 personas más de 60 años utilizando una técnica de muestreo
conglomerada en dos etapas. La herramienta de detección EEMM fue administrado a
los participantes elegibles (2742) para evaluar la función cognitiva. El análisis de
confiabilidad se realizó generando correlaciones entre ítems, ítems totales y valores alfa
estandarizados de Cronbach. El análisis factorial exploratorio dilucidó la estructura
factorial del instrumento EEMM. También se examinó la variación del puntaje del factor
(puntajes compuestos de subprueba) con el puntaje EEMM. El coeficiente alfa de
Cronbach del instrumento EEMM fue de 0.742, y las correlaciones ítem-totales variaron
de 0.2 a 0.5. En el análisis factorial, se extrajeron tres factores ("funcionamiento
ejecutivo", "memoria" y "atención"), que representaron el 32,9% de la varianza total en
las puntuaciones EEMM. La variación de las puntuaciones de los factores con la
puntuación EEMM total, reveló un patrón que sugiere que la sensibilidad del
instrumento gira alrededor de la puntuación EEMM 18. El EEMM es un instrumento
confiable para usar en nuestro entorno de estudio y tiene una estructura de tres factores.
La estructura de 3 factores es paralela a las dimensiones reconocidas de la capacidad
neurocognitiva. La estructura de factores establecida proporciona contexto y
comprensión, lo cual pueda ayudar a los médicos e investigadores a interpretar los
datos obtenidos del uso del EEMM.
Palabras claves: Fiabilidad, análisis factorial, Jamaica.
Introduction
The Mini-Mental Status Examination (MMSE) is the most commonly used and widely applied
test for assessment of cognitive impairment and memory problems in clinical medicine and
geriatrics (Bour, Rasquin, Boreas, Limburg, & Verhey, 2010; Elhan et al., 2005). There has
however been debate and criticisms about its broad applicability in multifarious cultural
settings and in linguistically disparate patients. There have also been questions concerning its
performance among people of low education status and its ability to identify persons with
very mild cognitive difficulties (Carnero-Pardo, 2014).
The MMSE is a brief 11-item screening tool that provides a quantitative assessment of
cognitive impairment (Folstein, Folstein, & McHugh, 1975). The tool evaluates performance
related to orientation to time and place, immediate recall, short-term verbal memory,
calculation, language, and construct ability. The score is the number of correct items, with a
maximum total score of 30. The component domain scores with regard to items are:
Orientation (total points = 10), Registration (total points = 3), Attention and calculation (total
points = 5), Recall (total points = 3), and Language (total points = 9). Generally, a score of 23
or less is deemed indicative of the presence of cognitive impairment (Ruchinskas & Curyto,
2003).
131James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
An updated scheme for interpreting scores with regard to level of impairment has been
outlined by Folstein, Folstein and Fanjiang (2001) as : ≥ 27, none; 21-26, mild; 11-20, moderate;
≤10, severe. A refinement of an earlier rubric by Tombaugh & McIntyre (1992) where the
categories 24-30, none; 18-23, mild; and 0-17, severe, were stipulated. However, the trust
placed in the results obtained and their subsequent interpretation is inter alia dependent on
reliability of the instrument; reliability being the degree to which an assessment tool produces
stable and consistent results (Leech, Barrett, & Morgan, 2015). Internal consistency reliability
is a measure of reliability used to evaluate the degree to which different test items that probe
the same construct produce similar results (ibid.). If an assessment tool is reliable, one can be
confident that repeated or equivalent assessments will provide consistent results (ibid.).
Attention to reliability issues is especially important when using the results of an assessment
to make decisions about clinical and social care.
Studies indicate variations in the reliability of the MMSE screening tool as reflected by
Cronbach’s alpha, a commonly recognized measure of the internal consistency (reliability) of
scale or tool items (Creavin et al., 2016; Hopp, Dixon, Grut, & Bäckman, 1997; Jorm et al., 1988;
Kabátová, Puteková, Martinková, & Súkenníková, 2016). Possible values of Cronbach’s alpha
generally range between 0 (‘no reliability’) and 1 (‘perfect reliability’), but if items on a scale
or tool are in systematic disagreement, negative values may be obtained ( Leech, Barrett, &
Morgan, 2015). Values above 0.7 are generally considered acceptable with greater reliability
as values increase (George & Mallery, 2003). Low values for Cronbach’s alpha have been cited
for the MMSE instrument; 0.54 among educated (> 8th grade) (Jorm et al., 1988). In a study
among adults without dementia who were over the age of 75 years, Hopp, Dixon, Grut, &
Backman (1997), reported Cronbach’s alpha to vary between 0.31 and 0.52. On the other hand,
higher and more desirable values such as 0.75 (Elhan et al., 2005), 0.78 (Kabátová et al., 2016),
0.82 (Ong et al., 2016) and 0.96 (Foreman, 1987) have been documented. These latter studies
were conducted respectively in Turkey among acute brain injury patients, Slovakia among
geriatric patients, China among patients with schizoaffective disorders, and the USA in
hospitalized medical-surgical patients age 65 years and over. Overall, these observations point
to the need to establish reliability of the MMSE for the local populations and specific contexts
in which the instrument is used. Furthermore, performance of the tool may be affected by
variables such as age, education, gender, socioeconomic status, culture, language and
ethnicity and test location (for example, home versus hospital) (Li, Jia, Yang, & Moreau, 2016;
Norris, Clark, & Shipley, 2016; Ridha & Rossor, 2005).
It is therefore useful to evaluate various aspects of the psychometric properties of the MMSE
tool in any population in which it is being used. Although the performance of the MMSE
screening tool among older persons in Jamaica with respect to sensitivity, specificity and
receiver operating characteristics (ROC) parameters has been recently reported (James et al.,
2019), a search of peer-reviewed literature found no published reports or details on attributes
related to reliability/internal consistency of the tool in Jamaica or the Anglophone Caribbean.
Given projected increases in cognitive impairment and dementia in the region (ADI/Bupa,
2013), with the likelihood of greater dementia and cognitive impairment screening, coupled
132Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica with rapid population ageing (Quashie, 2017), it is imperative that reliability of this widely used tool is be established. This paper examines reliability related characteristics of the MMSE tool in older persons (age 60 years and over) in a Caribbean country, Jamaica. It specifically reports Cronbach’s alpha and item-total correlations in the aforementioned population for the MMSE tool. The factor structure of the instrument when administered in the local population is also explored for comparison with previously reported and established domains. Method In 2012, 2943 persons aged 60 years and above in Jamaica constituting a nationally representative sample were surveyed. Data collected during the study pertained to health, lifestyle, and socio-economic aspects of older adults in Jamaica. The study employed a two- stage cluster sample with a probability proportional to size (PPS) to obtain participants for the survey. Parish enumeration districts and households were first- and second-stage cluster units respectively with subsequent selection of eligible participants age 60 years and older. Details of methodological approach and procedures have been published elsewhere (Mitchell-Fearon et al., 2014). Face-to-face interviews were conducted with study participants. A structured and pre-coded questionnaire elicited socio-demographic information, and the MMSE screening tool was administered to assess cognitive function. From the sample of 2943, 161 persons (approximately 5%) were unable to do the test due to severe illness or physically debilitation or known neurological disease (e.g., severe Parkinson’s disease). Mini-Mental Status Examination scores were determined for the remaining 2782 persons. The MMSE data for the 11 questions of the instrument were entered into a SPSS database (Statistical Package for the Social Sciences, version 19). Reliability analysis was performed generating Cronbach’s alpha values as well as inter-item and item-total correlations. Overall Cronbach’s alpha based on standardized items was preferentially reported as recommended by Gliem & Gliem, (2003) and Santos, (1999) as the 11 individual items are not scaled the same. For example, the ‘Read and Obey’ item has - possible scores of 0-1 while the ‘Serial 7’s’ item has possible scores of 0-5. Given that there are 11 items on the MMSE instrument, an inter-item correlation matrix produces multiple (55 distinct) correlation coefficients; each attempting to capture the relationship between each possible pair of the 11 different items. The data from items on the MMSE tool was subject to principal axis factor analysis (PA) using Varimax rotation; allowing for the aforementioned large amount of information generated to be distilled into a few components that succinctly capture and convey the main constructs which underlie these items in our local context. Values for the determinant (0.178), Keiser-Meyer-Olkin test of sampling adequacy (0.81), Bartlett’s test of Sphericity (p
James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
Exploratory factor analysis was done to identify and generate composite scores for factors
underlying the MMSE instrument used. Factors with primary factor loading or cross-loadings
of 0.4 were used to elucidate the simple factor structure of the MMSE instrument: items being
clustered into groups defined by their highest factor loadings.
A scree plot was also used to identify the number of factor components that should be retained
in the emergent simple factor structure by identification of the pattern of eigenvalue decline.
Consistent with convention, only components with eigenvalues one or greater were retained
(Field, 2005; C. H. James, David, & Vida, 2004).
For each respondent, a factor score was generated by summing the score obtained for the
items that constitute the factor. The variation of factor score with MMSE score was
subsequently examined for factors identified and retained.
Results
There was a total of 2782 participants in the study, with the majority (51.6%) being females.
Almost 44% of participants were between the ages of 60-69 years, those in the age categories
70-79, 80-89 and ≥ 90 years accounted for 33.7% (n=936), 18.7% (n=519) and 3.3% (n=93)
respectively. The majority (77.6%, n=2144) of participants had primary level education or
below, while 12.4% had secondary level education. The remaining portion (10%, n=275) had
post-secondary or tertiary level education. Approximately 76% of respondents had one or
more doctor-diagnosed chronic disease.
Descriptive statistics for the individual items (subtests) of the MMSE instrument administered
to the sample are displayed in Table 1. Respondents generally were able to complete most
subtests successfully as highlighted by the relatively high means. Exceptions were those tasks
related to attention and calculation, copying design/drawing and recall of three words.
134Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
Table 1: Mean score and standard deviation for MMSE items (n=2782)
Items (Subtests) Possible Score Range Mean Std. Deviation
Orientation – time 0–5 4.265 1.194
Orientation – place 0–5 4.693 0.815
Registration - 3 words 0–3 2.895 0.456
Attention and calculation 0–5 2.424 2.112
Recall of 3 words 0–3 1.325 1.102
Naming of objects 0–2 1.912 0.370
Repetition 0–1 0.890 0.313
Following/effecting three-
0–3 2.692 0.814
stage command
Read and obey 0-1 0.753 0.432
Write a sentence 0-1 0.694 0.461
Copy design/drawing 0-1 0.539 0.499
The Cronbach’s alpha coefficient of the MMSE instrument based on standardized items was
0.742, and item-total correlations varied approximately from 0.2 to 0.5 (Table 2). Of these item-
total correlations (standardized or not) 72.7% were approximately 0.4 and above (rounded to
one decimal place). Lower item-total correlations were observed for the items pertaining to
‘recall of three words’, ‘naming of objects’ and comprehending/effecting ‘the three-stage
command’. Each individual item would result in lower or approximately the same
Cronbach’s alpha if it was deleted, suggesting that all items should be kept as part of the scale.
135James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
Table 2: Item-Total correlations of the MMSE tool in persons 60 years and over, Jamaica
Item-Total Cronbach’s Alpha
Item-Total correlation if Item deleted
Item
correlation (standardized) (standardized)
Orientation- Time 0.500 0.493 0.708
Orientation -Place 0.426 0.458 0.713
Registration- 3 words 0.369 0.395 0.722
Attention and calculation
(serial ‘7s’) 0.430 0.420 0.719
Recall of 3 words 0.253 0.214 0.746
Naming of objects 0.275 0.316 0.733
Repetition 0.353 0.383 0.724
Follow/effect three-stage
0.229 0.293 0.736
command
Read and obey 0.407 0.446 0.715
Write a sentence 0.408 0.445 0.715
Copy design/drawing 0.394 0.406 0.720
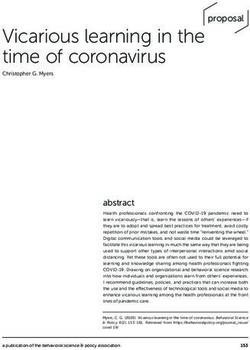
On factor analysis, three factors were extracted. These three factors had eigenvalues (an
indicator of explained variance) greater than 1 suggesting that they explain more information
than just what a single item would have explained. The scree plot below (Figure 1)
corroborates this observation showing that after these three factors, the curve flattens, and
differences between eigenvalues diminish and values are less than 1.
136Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
Figure 1: Scree plot for the MMSE among community dwelling older adults, Jamaica
The three identified factors explain approximately 32.9% of the total variance in MMSE score.
The first (Factor I), the second (Factor II) and the third (Factor III) account for 12.3%, 11.5%
and 9.1% of variance respectively. The factors and their loadings are presented in Table 3.
Factor loadings > 0.4 are marked in bold. Table 3 also displays the communalities which
ranged from 0.175 – 0.503 and reflect the proportion of variance in each item that can be
explained by the three retained factors.
137James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
Table 3: Varimax Rotation Factor Matrix for the factor structure of the 11 item MMSE instrument
for older adults, Jamaica
Factor Communality
I II III
Item
Write a sentence .680 .140 .144 .503
Copy design/drawing .582 .103 .174 .379
Read and Obey .554 .255 .100 .382
Orientation –Place .064 .545 .365 .434
Following/effecting 3-stage command .183 .456 -.074 .247
Registration- 3 words .058 .455 .281 .289
Naming of Objects .160 .434 .012 .214
Repetition .111 .401 .245 .234
Orientation – Time .191 .302 .579 .463
Recall of 3 words .085 .000 .410 .175
Attention and calculation (serial ‘7s’) .342 .124 .402 .294
Factor I, comprises three items which relate to psychomotor and sequencing aspects of
cognition and reflect the ability to plan and execute a goal. This is now labelled ‘Executive
functioning’. Factor II includes five items which appear to relate to short term and immediate
memory. This factor is now labelled ‘Memory’. Factor III is composed of three items which
predominantly pertain to attention and concentration. This is now labelled ‘Attention’. For
each of the three factors identified, the variation of factor scores with total MMSE score is
shown in Figure 2. Accompanying 95% confidence intervals for each factor score is also
displayed. For Factor I, scores generally remained flat with a slight increase after MMSE score
of 18. For Factor II, there was a positive correlation between Factor II scores and total MMSE
score. There was a notable increase in Factor II scores as MMSE scores increased up to MMSE
score of 18, after which, the scores generally remained constant. With regard to Factor III, there
was a marginal change in scores as MMSE increased up to MMSE score of 18, after which,
there was a sustained increase in factor scores. For all three factors, 95% confidence intervals
were relatively narrow and precise, except for MMSE score five as only two participants had
a score of five.
138Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
Figure 2: Variation of factor score with total MMSE score
139James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
Discussion
Establishing reliability is an acknowledged critical step for instruments used in research. For
the MMSE in our studied population, Cronbach’s alpha was 0.742. This, according to the
popularly used scale by George and Mallery (2003) implies an acceptable reliability and
moderate internal consistency of the MMSE tool (George & Mallery, 2003). Previous studies
have reported comparable Cronbach’s alpha values of 0.75, 0.74 and 0.80 respectively (Awan
et al., 2015; Elhan et al., 2005; Iatraki et al., 2017); the latter two from Pakistan (a developing
country) and from a rural population of relatively low educational status in Greece
respectively. Moderate internal consistency of the MMSE tool in our study is corroborated by
the fact that 72.7% of the item total correlations was above 0.4. De Vaus (2013) recommend
item total correlation values of 0.40 and above (De Vaus, 2013) and Carmines & Zeller (1974)
advocate having at least 50% of the item total scores being in the range of 0.30 to 0.70
(Carmines & Zeller, 1974).
Factor analysis of the present study resulted in three factors which we designate ‘Executive
functioning’, ‘Memory’ and ‘Attention’. The three factor solution parallels results of other
studies such as Shyu & Yip (2001) and Shigemori, Ohgi, Okuyama, Shimura, & Schneider
(2010) which had similar structure. For example, compared with Shyu and Yip (2001) our
Factor I ‘Executive functioning’ mirrored the ‘Complex processing’ factor in that study and
included the items (subtests) ‘Write a sentence’, ‘Read and Obey’ and ‘Copy design/drawing’.
The Factor II ‘Memory’ was analogous to their ‘Simple processing’ which included naming,
command, repetition and registration, and reflects processes related to short term memory,
storage and simultaneous processing. The Factor III ‘Attention’ was equivalent to their
Attention/Memory factor and consequently is concerned with items such as spelling,
arithmetic and attention to calculation. Orientation in time also loaded on Factor III. It may
appear counterintuitive, however, it is known that orientation in time is associated with
140Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
functions in the pre-frontal cortex (Gozlan, 2013; Rao, Mayer, & Harrington, 2001), a region
which regulates attention (Arnsten, 2009).
The triple factor structure was deemed optimal because of: evident leveling off of eigenvalues
below one after three factors and because the three-factor grouping facilitated represented a
simple structure that facilitated logical interpretation and characterization of the factors; the
primary purpose of factor analysis. Approximately one third of the variance in MMSE subtests
was explained by these three factors. Other studies with three factor extractions have reported
percentage of total variance explained ranging from 44.6% - 85% (Brugnolo et al., 2009;
Fillenbaum, Heyman, & Haynes, 1987; Shigemori, Ohgi, Okuyama, Shimura, & Schneider,
2010). The wide variation in variance explained across studies and the contrast with our study
could be due to a number of factors. The differences in clinical profile of the populations
studied and second, differences in educational level. In this study, subjects were community
dwelling older persons from the general population compared to other studies (Brugnolo et
al., 2009; Fillenbaum et al., 1987; Shigemori et al., 2010) which were confined to groups with
specific morbidities for example, Alzheimer’s disease, hospitalized stroke patients and
patients with mild cognitive impairment (MCI). Self-care ability influences ‘attention’ and
‘simple processing’ (memory) (Shyu & Yip, 2001). Education level can impact the responses
obtained on the MMSE and the percentage of total variance explained. Educational level has
been associated with complex processing ability (akin to ‘executive processing’ in our study)
accounting for as much as 88% of its variance (Shyu & Yip, 2001).
This study’s elucidation of a three-factor structure may have implications for existing and
future shortened versions of screening tests for cognitive impairment, example the Mini-Cog©
test. Shortened tests ought to reflect these three factors or domains in their construction. The
Mini-Cog© test would arguably be very useful in our local setting as its three constituent items
are aligned to elements from each of our three factors: three item registration (Factor II), three-
word recall (Factor III) and clock drawing (Factor I). The World Health Organization (2008)
‘Age Friendly Primary Health Care Centres Toolkit’ is a ten-minute comprehensive screening
tool developed to work in a number of countries including Jamaica (World Health
Organization, 2008) This tool utilizes registration and recall of three words for preliminary
rapid screening of memory function with subsequent detailed screening using the MMSE, as
necessary. Registration and recall of three words are related to Factors II and III of this study
respectively. Future efforts for improving this instrument may involve including an item from
our Factor I domain.
The pattern of variation of factor scores with total MMSE scores provides additional insight
on the way its constituent items (sub-test) collectively influence MMSE scores and subsequent
screening results. The pattern for Factor I with total MMSE scores shows a subtle but evident
decline from higher scores, until MMSE score of 18 and was generally flat for the lower scores
thereafter. This factor appears to be useful for detecting early decline. Factor II remained
relatively constant at scores above MMSE score of 18, but displayed a sharp linear decline
with scores below MMSE score 18. Factor II and its constituent sub-tests appear to be relatively
insensitive to early cognitive decline and mild impairment, but effectively identifies
141James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
deterioration in MMSE scores and cognitive function subsequently. Previous authors have
noted that the items which comprise Factor II are concerned with verbal skills that arise from
entrenched knowledge, and these are conserved in early dementia and cognitive decline,
explaining the relative insensitivity at higher MMSE scores (Brugnolo et al., 2009; Feher et al.,
1992). Factor III was highly sensitive to decline in higher MMSE scores and thus may be useful
in efforts to identify early or mild cognitive impairment.
Each factor maximizes sensitivity across different ranges of scores. Taken collectively, they
constitute a robust instrument and the MMSE as a tool is likely to be useful in our, and similar
settings. In this study, changes in patterns seem to pivot around MMSE score of 18. Previously
published findings utilizing data derived from the same sample of participants in this study
has noted that the MMSE score cut-point which maximizes sensitivity and specificity was
18/19 (K. James et al., 2019). Graphical analysis of the relation between factor score and total
MMSE score appears to indicate and corroborate optimal cut-points.
It was recognize that education level may influence emergent factor structure and item
performance (Vissoci et al., 2019). In this study, participants predominantly had low
educational level, with 78% achieving primary level education and below as their highest level
of schooling; consequently, effects of education level could not be substantively addressed.
Nevertheless, this study proposed many strengths. A nationally representative sample was
used, and the sample size was large. The study provides new information on factor structure
and reliability of the MMSE in the Caribbean region - the second most rapidly ageing region
of the world. Furthermore, it adds to the global body of literature being one of the few studies
that have examined and reported on the variation and relationship of factor scores and overall
MMSE scores.
Conclusion
The MMSE is a reliable instrument for use in our study setting and optimally has a three-
factor structure (‘executive functioning,’ ‘memory’ and ‘attention’). The 3-factor structure
parallels recognized dimensions of neurocognitive ability. There is variation in the
relationship of individual factors across total MMSE scores. The established reliability and
factor structure provides greater contextual understanding of the psychometric attributes of
the MMSE, which can aid clinicians and researchers in interpreting data derived from its use.
References
ADI/Bupa. (2013). Dementia in the Americas: Current and future cost and prevalence of
Alzheimer’s disease and other dementias.
https://www.alz.co.uk/sites/default/files/pdfs/dementia-in-the-americas-ENGLISH.pdf
Arnsten, A. F. T. (2009). The emerging neurobiology of attention deficit hyperactivity
disorder: The key role of the prefrontal association cortex. The Journal of Pediatrics,
154(5), I-S43. https://doi.org/10.1016/j.jpeds.2009.01.018
142Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
Awan, S., et al. (2015). Validation study of the mini-mental state examination in Urdu
language for Pakistani population. The Open Neurology Journal, 9, 53–58.
https://doi.org/10.2174/1874205X01509010053
Bour, A., Rasquin, S., Boreas, A., Limburg, M., & Verhey, F. (2010). How predictive is the
MMSE for cognitive performance after stroke? Journal of Neurology, 257(4), 630–637.
https://doi.org/10.1007/s00415-009-5387-9
Brugnolo, A., et al. (2009). The factorial structure of the mini mental state examination
(MMSE) in Alzheimer’s disease. Archives of Gerontology and Geriatrics, 49(1), 180–185.
https://doi.org/https://doi.org/10.1016/j.archger.2008.07.005
Carmines, E. G., & Zeller, R. A. (1974). On establishing the empirical dimensionality of
theoretical terms: An analytical example. Political Methodology, 1(4), 75–96.
http://www.jstor.org/stable/25791395
Carnero-Pardo, C. (2014). Should the mini-mental state examination be retired? Neurologia,
29(8), 473–481. https://doi.org/10.1016/j.nrl.2013.07.003
Creavin, S. T., et al. (2016). Mini-Mental State Examination (MMSE) for the detection of
dementia in clinically unevaluated people aged 65 and over in community and
primary care populations. Cochrane Database of Systematic Reviews, 13(1), CD011145.
https://doi.org/10.1002/14651858.CD011145.pub2
De Vaus, D. (2013). Surveys In Social Research (6th ed.). New York: Routledge
Elhan, A. H., et al. (2005). Psychometric properties of the mini-mental state examination in
patients with acquired brain injury in Turkey. Journal of Rehabilitation Medicine, 37(5),
306–311. https://doi.org/10.1080/16501970510037573
Feher, E. P., et al. (1992). Establishing the limits of the mini-mental state examination of
“subtests.” Archives of Neurology, 49(1), 87–92.
https://doi.org/10.1001/archneur.1992.00530250091022
Field, A. (2005). Factor analysis using SPSS. Unpublished manuscript, University of Sussex.
http://users.sussex.ac.uk/~andyf/factor.pdf
Fillenbaum, G. G., Heyman, A., & Haynes, C. S. (1987). Comparison of two screening tests in
Alzheimer’s disease: The correlation and reliability of the mini-mental state
examination and the modified blessed test. Archives of Neurology, 44, 924–927.
https://doi.org/10.1001/archneur.1987.00520210026014
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state. A practical method
for grading the cognitive state of patients for the clinician. Journal of Psychiatric
Research, 12(3), 189–198. https://doi.org/10.1016/0022-3956(75)90026-6
Foreman, M. D. (1987). Reliability and validity of mental status questionnaires in elderly
hospitalized patients. Nursing Research, 36(4), 216–220.
https://doi.org/10.1097/00006199-198707000-00004
George, D. & Mallery, P. (2003). SPSS for Windows Step by Step: A Simple Guide and Reference.
11.0 update (4th ed.). Allyn & Bacon
Gliem, J. A, & Gliem, R. R. (2003). Calculating, interpreting, and reporting cronbach’s alpha
reliability coefficient for likert-type scales. Midwest Research to Practice Conference in
Adult, Continuing, and Community Education, 82–88.
https://doi.org/10.1109/PROC.1975.9792
Gozlan, M. (2013, January 1). A stopwatch on the brain’s perception of time. The Guardian
143James Kenneth, Thompson Camelia, Holder Nevins Desmalee, Chin-Bailey Cameal, Willie-Tyndale Douladel, McKoy Davis
Julian & Eldemire-Shearer Denise
https://www.theguardian.com/science/2013/jan/01/psychology-time-perception-
awareness-research
Hopp, G. A., Dixon, R. A., Grut, M., & Bäckman, L. (1997). Longitudinal and psychometric
profiles of two cognitive status tests in very old adults. Journal of Clinical Psychology,
53(7), 673–686. https://doi.org/10.1002/(SICI)1097-4679(199711)53:73.0.CO;2-J
Iatraki, E., et al. (2017). Cognitive screening tools for primary care settings: Examining the
“test your memory” and “general practitioner assessment of cognition” tools in a rural
aging population in Greece. The European Journal of General Practice, 23(1), 171–178.
https://doi.org/10.1080/13814788.2017.1324845
James, C. H., David, G. A., & Vida, S. (2004). Factor retention decisions in exploratory factor
analysis: A tutorial on parallel analysis. Organizational Research Methods, 7(2), 191–205.
James, K., et al. (2019). Performance and receiver operating characteristics of the mini-mental
state examination instrument in detecting dementia in a rapidly aging developing
country (Jamaica). Journal of Geriatric Psychiatry and Neurology, 32(4), 195–204.
https://doi.org/10.1177/0891988719841722
Jorm, A. F., et al. (1988). Educational level differences on the mini-mental state: The role of
test bias. Psychological Medicine, 18(3), 727–731.
https://doi.org/10.1017/S0033291700008424
Kabátová, O., Puteková, S., Martinková, J., & Súkenníková, M. (2016). Analysis of
psychometric features of the mini-mental state examination and the montreal cognitive
assessment methods. Clinical Social Work and Health Intervention, 7(2), 62–69.
https://doi.org/10.22359/cswhi_7_2_08
Leech, N. L., Barrett, K. C., & Morgan, G. A. (2015). IBM SPSS for intermediate statistics: Use
and interpretation (5th ed.). New York: Routledge.
Li, H., Jia, J., Yang, Z., & Moreau, N. (2016). Mini-mental state examination in elderly
Chinese: A population-based normative study. Journal of Alzheimer’s Disease, 53(2),
487–496. https://doi.org/10.3233/JAD-160119
Mitchell-Fearon, K., et al. (2014). Hypertension and diabetes prevalence in older persons in
Jamaica, 2012. West Indian Medical Journal, 63(5), 416–423.
https://doi.org/10.7727/wimj.2014.065
Norris, D. R., Clark, M. S., & Shipley, S. (2016). The mental status examination. American
Family Physician, 94(8), 635–641. https://doi.org/10.4324/9780429040191-5
Ong, H. L., et al. (2016). Performance of Mini-Mental State Examination (MMSE) in long-stay
patients with schizophrenia or schizoaffective disorders in a psychiatric institute.
Psychiatry Research, 241, 256–262. https://doi.org/10.1016/j.psychres.2016.04.116
Quashie, N. (2017). Ageing and health in the Caribbean. Innovation in Aging, 1(Suppl 1),
1258. https://doi.org/10.1093/geroni/igx004.4576
Rao, S. M., Mayer, A. R., & Harrington, D. L. (2001). The evolution of brain activation during
temporal processing. Nature Neuroscience, 4(3), 317–323. https://doi.org/10.1038/85191
Ridha, B., & Rossor, M. (2005). The mini mental state examination. Practical Neurology, 5(5),
298–303. https://doi.org/10.1111/j.1474-7766.2005.00333.x
Ruchinskas, R. A., & Curyto, K. J. (2003). Cognitive screening in geriatric rehabilitation.
144Reliability and factor structure of the mini-mental state examination (MMSE) among older adults in Jamaica
Rehabilitation Psychology, 48(1), 14–22. https://doi.org/10.1037/0090-5550.48.1.14
Santos, J. R. A. (1999). Cronbach’s alpha: A tool for assessing the reliability of scales. Journal
of Extension, 37(2), 1–5.
Shigemori, K., Ohgi, S., Okuyama, E., Shimura, T., & Schneider, E. (2010). The factorial
structure of the mini-mental state examination (MMSE) in Japanese dementia patients.
BMC Geriatrics, 10, 36. https://doi.org/10.1186/1471-2318-10-36
Shyu, Y. I. L., & Yip, P. K. (2001). Factor structure and explanatory variables of the mini-
mental state examination (MMSE) for elderly persons in Taiwan. Journal of the
Formosan Medical Association, 100(10), 676–683.
Vissoci, J. R. N., et al. (2019). Cross-cultural adaptation and psychometric properties of the
MMSE and MoCA questionnaires in Tanzanian Swahili for a traumatic brain injury
population. BMC Neurology, 19(1), 57. https://doi.org/10.1186/s12883-019-1283-9
World Health Organization. (WHO) (2008). Age-friendly primary health care centres toolkit.
Geneva: World Health Organization.
https://apps.who.int/iris/bitstream/handle/10665/43860/9789241596480_eng.pdf;jsessio
nid=53E95753803FCBCCD154D084F1CB2412?sequence=1
145You can also read