Rheumatoid Arthritis of the Cervical Spine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
136 Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48
Rheumatoid Arthritis of the Cervical Spine
Clinical Considerations
Bradley R. Wasserman, M.D., Ronald Moskovich, M.D., F.R.C.S., and Afshin E. Razi, M.D.
Abstract Early initiation of pharmacotherapy may slow progression
Rheumatoid arthritis (RA) is a chronic, systemic inflam- of rheumatoid cervical disease. Operative intervention be-
matory disorder affecting multiple organ systems, joints, fore the onset of advanced myelopathy results in improved
ligaments, and bones and commonly involves the cervical outcomes compared to the surgical stabilization of patients
spine. Chronic synovitis may result in bony erosion and whose conditions are more advanced. A multidisciplinary
ligamentous laxity that result in instability and sublux- approach involving rheumatology, surgery, and rehabilita-
ation. Anterior atlantoaxial subluxation (AAS) is the most tion is beneficial to optimize outcomes.
frequently occurring deformity, due to laxity of the primary
R
and secondary ligamentous restraints. Additional manifesta- heumatoid arthritis (RA) is a chronic, systemic
tions of RA include cranial settling, subaxial subluxation, inflammatory disorder affecting multiple organ
or a combination of these. Although clinical findings can systems, joints, ligaments, and bones. The extra-
be confounded by the severity of multifocal joint and sys- articular involvement may involve the skin, the eye, the
temic involvement, a careful history is critical to identify larynx, and the pulmonary, cardiovascular, hematologic,
symptoms of cervical disease; serial physical examination renal, neurologic, and lymphatic systems. Although there
is the best noninvasive diagnostic tool. Thorough physical are periods when RA flares and times when it is quiescent,
and neurologic examinations should be performed in all it frequently results in a proliferative and erosive synovitis
patients and serial functional assessments charted. Radio- that progresses to destruction of articular cartilage. RA
graphs of the cervical spine with lateral flexion-extension is the most common inflammatory disorder affecting
dynamic views should be obtained periodically and used to the cervical spine, an involvement that is second only to
“clear” the cervical spine before elective surgery requiring RA in the metatarsophalangeal joints. The course of the
general anesthesia. Advanced imaging, such as magnetic disease is unpredictable. For some patients, it manifests as
resonance imaging (MRI) or myelography and computed a benign process, while in others, a progressive pattern of
tomography (CT), may be necessary to evaluate the neuraxis. instability develops. In 1890, Garrod reported involvement
of the cervical spine in 178 (36%) of 500 patients with
Bradley R. Wasserman, M.D., was a Chief Resident, Department RA.1 In 1951, Davis and Markley2 were the first to describe
of Orthopaedic Surgery, and is currently a fellow in the Depart- medullary compression from atlantoaxial subluxation. In
ment of Sports Medicine, University of Pittsburgh Medical Center, 1952, Kornblum and colleagues3 were the first to recognize
Pennsylvania. Ronald Moskovich, M.D., F.R.C.S., is Assistant the relationship between RA and cervical spine instability,
Professor, New York University School of Medicine, and within the knowledge of which has deepened our understanding
the Division of Spine Surgery, Department of Orthopaedic Surgery.
of the effects of RA on the cervical spine. More recent
Afshin E. Razi, M.D., is Clinical Assistant Professor, NYU School
literature has documented involvement of the cervical spine
of Medicine, and within the Division of Spine Surgery, Department
of Orthopaedic Surgery, NYU Hospital for Joint Diseases, NYU early in the course of RA,4 often within the first 2 years after
Langone Medical Center, New York, New York. diagnosis.4,5 Craniocervical complications arise in 30% to
Correspondence: Ronald Moskovich, M.D., NYU Hospital for 50% of patients who have had RA more than 7 years, while
Joint Diseases, 301 East 17th Street, New York, New York 10003; atlantoaxial subluxation with myelopathy develops in 2.5
ronald.moskovich@nyumc.org. percent of those with RA for more than 14 years.6
Wasserman BR, Moskovich R, Razi AE. Rheumatoid arthritis of the cervical spine: clinical considerations. Bull NYU Hosp Jt Dis. 2011;69(2):136-48.Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 137
Although the exact etiology is uncertain, RA is 50% of all cervical spine rotation. The dynamic forces on
multifactorial and currently believed to be triggered by the cervical spine are increased by its range of motion and
exposure of an immunogenetically susceptible host to an its location between the stiffer thoracic spine and the weight
arthritogenic microbial antigen. It is an immunologically of the head.
mediated disorder that can affect the articular and non- The stability of the atlantoaxial complex depends
articular organ systems. The articular involvement is a primarily on the integrity of the transverse ligament. The
symmetrical peripheral joint disease affecting large and alar ligament is a secondary stabilizer located between the
small joints and axial involvement predominantly of the odontoid process and the occiput. The apical ligaments
upper cervical spine. provide additional support for the occiput-atlanto-axial
Following the expression of the new antigen, these synovial articulation. Because the C1-C2 facets are primarily ori-
cells stimulate the body to produce immunoglobulins (IgM) ented in the axial plane, compared to the lower cervical
against autologous IgG, the so-called rheumatoid factor. spine, there is no bony structure interlocking the atlas
An inflammatory response is initiated by the activated and axis to prevent subluxation.8 Fielding and coworkers
CD4+ helper T cells, stimulating the release of monocytes, demonstrated that the integrity of the transverse ligament
macrophages, and synovial fibroblasts to produce the is an important factor in preventing anterior subluxation
proinflammatory cytokines interleukin-1, interleukin-6, and of the atlas, especially during neck flexion.7,8 In RA, the
TNF-α and to secrete matrix metalloproteinases through cell- transverse ligament is frequently targeted and becomes
surface signaling by means of CD69 and CD11, as well as incompetent, due to involvement or spread of inflamma-
through the release of soluble mediators such as interferon-γ tion from the synovial articulation of the dens. Complete
and interleukin-17; this ultimately results in synovitis and rupture of the transverse ligament allows only 4 to 5 mm of
pannus formation. The sequelae of this process can lead anterior subluxation of the atlas if the secondary stabilizers
to destruction or incompetence of the involved ligaments, are intact. Involvement of the secondary stabilizers in RA
bones, or joints, or any combination thereof. Early initiation results in progressive loss of stability of the atlantoaxial
of pharmacotherapy using disease modifying anti-rheumatic joint. The synovial inflammation at the base of the dens
drugs (DMARDS) in combination with the introduction of can result in erosion of the odontoid process, further com-
newer immunological mediators, such as TNF-α blockers, promising stability. The lack of osteophyte formation in
slows progression of the disease. Initiation of aggressive the face of hypermobility, a unique characteristic of RA,
therapy prior to cartilage destruction may actually prevent fails to provide compensatory stability. The dynamic forces
or significantly mitigate joint damage, usually caused by generated by the weight of the head and relative stability of
rheumatoid pannus. It is also important to identify patients the thoracic spine exacerbate the situation and may result
who are at risk of developing irreversible neurologic deficit in incompetence of the ligamentous stabilizers or fracture
and to intervene surgically before neurologic deterioration of the weakened dens, or a combination of the two. The
compromises their already limited functional ability. lower medulla is approximately 11 mm in AP diameter. At
the foramen magnum, the spinal diameter is 10 mm and
Anatomy distally 8 to 10 mm. The space available for cord (SAC)
The anatomy and the dynamic forces exerted on the cervi- is 14 mm at the foramen magnum, 14 mm at C2, and 12
cal spine make it especially vulnerable to the effects of RA. to 14.5 mm in the subaxial spine.6
There are numerous synovial joints, including the atlanto-
occipital, atlantoaxial, and facet (apophyseal) joints. The Pathophysiology
neurocentral joints of Luschka and the intervertebral disks The role of mediators of inflammation, such as cytokines,
are also functional components of the subaxial motion seg- growth factors, and metalloproteinases has been described
ments. The occiput-C1 and C1-C2 articulations are the only in the progression of RA. These factors attract and activate
segments in the spine without intervertebral disks. These two cells from the peripheral blood and enhance proliferation and
segments consist exclusively of synovial joints and, thus, do activation of synoviocytes. The proteases can then invade
not benefit from the protection afforded by the more stable and destroy articular cartilage, subchondral bone, tendons,
cartilaginous intervertebral joints. Even the transverse liga- and ligaments. The histologic picture of a joint affected by
ment of the atlas (C1) articulates with the posterior aspect RA typically consists of a hypervascular layer of synovium
of the dens via a synovial joint.7 The unique characteristics infiltrated with giant cells and other inflammatory cells.
of the atlas and axis permit increased motion of the cervical There is a high population of lymphocytes in the acute phase.
spine. The atlas lacks a vertebral body and supports the head Fibrin is seen as a sheet within the joint cavity. The hyaline
by lateral articulations with the occipital condyles, result- cartilage is damaged, and reactive bone formation is seen
ing in greater than 50% of the total cervical spine flexion in the subchondral regions. The ligaments are also involved
and extension at the occiput-C1 articulation. The odontoid via disruption of collagen, multiple micro-tears, and fibrous
process of the axis articulates with the atlas-transverse liga- tissue repair. This destructive synovitis progresses to bone
ments. This unique articulation accounts for approximately erosion and ligamentous laxity, ultimately leading to instabil-138 Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48
ity and subluxation of the cervical spine. The most common ligaments playing the predominant role in early RA.
presentations of cervical spine involvement include: atlan- Autopsy reports of patients with RA most likely underes-
toaxial subluxation (65%), cranial settling (20%), subaxial timate the true frequency of death due to rheumatoid cervical
subluxation (15%), or a combination thereof. changes and spinal cord compression.2,20,29 Mikulowski and
Anterior atlantoaxial subluxation (AAS) is the most colleagues30 found that of 104 autopsies of RA patients, 11
common deformity and results from laxity of the primary had AAS with cord compression; seven of these 11 patients
and secondary ligamentous restraints, as described. Anterior had died suddenly. This study revealed a 10% rate of fatal
subluxation greater than 10 to 12 mm implies destruction cord compression in patients dying with RA.
of the entire ligamentous complex. The SAC decreases In a postmortem study of nine patients with RA and
as the anterior atlantodental interval (AADI) increases myelopathy, Henderson and coworkers31 noted that the cord
and the posterior atlantodental interval (PADI) decreases. pathology occurred mostly in the dorsal white matter of the
Rheumatoid pannus, formed by granulation tissue within spinal cord and was characterized by axonal degeneration,
the synovium due to collagenases and proteolytic enzymes central chromatolysis, and axonal retraction. The cord pa-
that destroy other ligaments, cartilage, tendons, and bones, thology usually included subaxial degeneration, indicating
has a propensity for the periodontoid region. The pannus diffuse injury throughout the cervical spine. Their results
itself may further decrease the PADI, resulting in additional concluded that the effects of compression, stretch, and
injury to the cord. Subluxation may ultimately lead to cord movement were the likely causes of myelopathy, rather
compression, resulting in myelopathy. than ischemia. However, in another autopsy study of 11
Posterior atlantoaxial subluxation occurs less frequently patients with paralysis secondary to RA, Delamarter and
than anterior AAS, accounting for approximately 7% of Bohlman32 suggested that the paralysis could be due to
cases. Posterior subluxation is usually due to erosion or either mechanical neural compression or vascular impair-
fracture of the dens, and it may carry a higher risk of cord ment, or both.
compression than AAS.9,10 Lateral subluxation usually oc- The fibers in the pyramidal decussation to the upper limbs
curs with rotational deformity and is seen in as many as 20% are more superior and ventral and more medial than the
of cases.11,12 lower limb fibers, which are located inferior and laterally at
Cranial settling results from occipito-atlanto-axial ero- the cervicomedullary junction.33,34 Atlanto-axial subluxation
sion that usually follows atlantoaxial subluxation. Other may result in cruciate paralysis, which is a symmetric upper
terms describing this deformity include basilar invagination, extremity paralysis with less lower extremity involvement.
translocation of the dens, atlantoaxial impaction, superior
migration of the odontoid, and vertical settling.13-15 However, Epidemiology and Natural History
“basilar invagination” and “basilar impression” are terms Complete understanding of the natural history of rheumatoid
usually used to describe actual deformity of the skull base, cervical spine remains deficient, due in part to therapeutic
such as occurs in osteogenesis imperfecta. El-Khoury and intervention. Reports of the prevalence of cervical spine
associates16 observed that symmetrical rheumatoid destruc- abnormality associated with RA (17% to 88%) and neu-
tion of the occipito-atlanto and atlantoaxial joints allows rologic complications (11% to 70%)8,12,35,36 vary widely in
the cranium to settle on the cervical spine and for the dens the literature. According to one study, approximately 1%
to enter the foramen magnum. However, another investiga- of adults in Europe and the United States (2.2 million) are
tion observed that if only one lateral mass is involved, fixed affected by RA, 220,000 (10%) of whom have cervical
rotational tilt of the head may result. Superior migration of spine involvement; 62,700 individuals would benefit from
the dens can lead to brain stem compression.17 Cranial set- surgical stabilization.28
tling often results in reduction of the atlantoaxial interval There is a wide variation in the prevalence of AAS in
due to the conical shape of the dens and reduced motion, RA patients, depending on the length of follow-up. The
giving a false impression of anatomic improvement known variations reported in different studies may be due to
as “pseudostabilization.”11,14,18,19 different populations studied and different criteria (i.e.,
Subaxial cervical subluxation occurs secondary to com- neurologic or radiographic evaluation or both). Sharp
bined destruction of the discovertebral and the facet joints. and Purser37 performed a large general population survey,
Subluxation can appear as an isolated deformity or can affect reviewing 1,478 single lateral cervical films; 78 (5.3%)
multiple spinal levels, producing a “staircase” deformity.20-26 patients had clinical evidence of RA and, of those, 6.4%
Kudo and Iwano27 have described anterior soft tissue masses, (5/78) displayed atlantoaxial subluxation. Of another 79
posterior ligamentous thickening, and bony subluxation. RA patients admitted to the hospital, 14 (18%) were noted
These changes may cause osteophyte formation, ankylosis, to have atlantoaxial subluxation. Among 241 patients with
bone collapse, and kyphosis. Crockard28 further postulated RA, Riise and associates38 documented a mean observa-
that laxity of the atlantoaxial ligaments and subaxial post- tion time from the diagnosis of RA to AAS of 3.9 years.
inflammatory ankylosis are the two main deforming factors The prevalence of AAS has been reported to be as high as
in RA of the cervical spine, with the laxity of the atlantoaxial 12% within 2 years after the onset of RA.5 Pellici and col-Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 139
leagues39 reported on the outpatient records of 106 patients while one passed away from cardiac disease. All seven
from a comprehensive arthritis program at one institution. patients treated nonoperatively died within 4 years, five
They reported that 46 (43%) of their patients already had (71%) from cord compression; three died within 1 month
radiographic evidence of rheumatoid involvement of the from the onset of paralysis. Forty-eight percent (35/73)
cervical spine at the start of their study. Of these 46, AAS had operative treatment; 71% (25/35) of those treated op-
was observed in 28 (61%), AAS combined with subaxial eratively for paralysis had neurologic improvement, while
subluxation in 9 (20%), and subaxial subluxation alone in only two of these patients (6%) worsened one neurological
5 (11%). Two years later, Winfield and coworkers26 con- level. They also noted that the initial neurological class was
cluded that cervical subluxation was more likely to occur related to neurological recovery. Rana46 reviewed a series
in patients with erosions of the hands and feet, which had a of 41 patients with AAS during a 12-year period. Radio-
propensity to deteriorate progressively over time. They also graphically, 12% improved, 61% were unchanged, and
noted that the timing and severity of cervical subluxation 27% had progression of instability. With disease progres-
coincided with the progression of peripheral erosive disease sion, the occipitoatlantal complex involvement becomes
in 26 (76.5%) of the 34 patients in their case series. significant and cranial settling develops. The prevalence
The consequences of the development of AAS can be of cranial settling has been reported to be between 5% and
dire. In 1997, Sunahara and associates40 published their 38%21,37,46,47 and progresses in 35% to 50% of patients.19
follow-up on 21 patients with RA and myelopathy second- Subaxial subluxation develops in 10% to 20% of patients
ary to AAS. All patients were recommended for surgery but with late stage RA.21,25,37 It may also develop in patients who
refused. No patient showed any sign of improvement, while were treated with an arthrodesis. In 1991, Kraus and associ-
16 (76%) had evidence of deterioration during follow-up. ates14 reported on a series of 79 patients with generalized
All patients became bedridden within 3 years of the onset RA and prior occipito-cervical fusions. Thirty-six percent
of myelopathy. The cumulative probability of survival was developed subaxial subluxation an average of 2.6 years fol-
0% 7 years following the onset of myelopathy. In 2001, lowing their fusion; however, only 5.5% of patients treated
Riise and colleagues38 reported that patients with AAS had with an atlantoaxial fusion developed subaxial subluxation
a mortality rate eight-times that of patients without AAS. an average of 9 years after their fusion. This case series sug-
Untreated AAS can have very poor outcomes. Once gests that monosegmental atlantoaxial (C1-C2) arthrodesis
myelopathy has occurred, death is a common sequela. is preferable to occiput-C2 fusion, if possible, and also that
Even with all of the literature that is available on rheuma- consideration be given to extending fusion levels in patients
toid cervical spine, it is still impossible to predict which with early subaxial subluxation and to monitoring patients
patient will progress radiographically or which patient will with occipitocervical fusion for development of subsequent
experience neurologic deficits. Hence, the best results of subaxial subluxation.
operative stabilization have been reported in patients who
were treated before any myelopathic signs were present. Clinical Manifestations
There have been several reports stating that the severity of A careful history is critical in identifying symptoms of
cervical spine involvement in RA correlates to the severity cervical disease. Neurologic findings are difficult to define,
of extant peripheral joint disease, rheumatoid nodules, high because of multifocal involvement associated with muscle
seropositivity, vasculitis, high-dose steroid therapy, and male wasting, joint arthropathy, decreased range of motion, joint
gender.9,35,36,38,41-44 pain, and neuropathy. Many patients may be asymptomatic,
Boden and coworkers45 investigated the radiographic and even with severe instability, due to the silent nature of this
clinical course of 73 patients with rheumatoid involvement condition. Marks and colleagues48 showed a 31-week delay
of the cervical spine over an average of 7.1 years; 58% in diagnosis from the first signs of cervical myelopathy. Once
(42/73) became paralyzed. Seven patients with paralysis myelopathy has occurred, progression is almost a certainty.
were treated nonoperatively. None of these individuals A thorough physical examination should be performed
improved, and six patients had worsening of their neuro- in all patients, even though findings can be confounded
logic deficits. Three of the patients died within 1 month by the severity of multifocal involvement. Serial physical
after the onset of paralysis, two from compression of the examinations are the best noninvasive diagnostic tool.
spinal cord. The other four patients died within 4 years of Certain findings should arouse suspicion for further
the diagnosis; three died secondary to cord compression, work-up, including but not limited to an increase in
Table 1 Ranawat Grading System
Class I No neural deficit
Class II Subjective weakness with hyperreflexia and dysesthesia
Class III Objective weakness and long tract signs
Class IIIA Ambulatory
Class IIIB Nonambulatory140 Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 Table 2 Classification of Functional Capacity in Rheumatoid Arthritis Class I Complete ability to carry on all usual duties without handicaps Class II Adequate for normal activities, despite handicap of discomfort or limited motion at one or more joints Class III Limited to little or none of the duties of usual occupation or self-care Class IV Incapacitated, largely or wholly bedridden, or confined to wheelchair, little or no self-care pain or weakness, spasticity of the extremities, a change tigators also noted myelopathy in 36/45 patients (80%) with in ambulatory status, bowel or bladder disturbance (or cranial settling. Brain stem dysfunction was also higher in both), Babinski’s sign, loss of proprioception, and hy- patients with cranial settling. The cranial nerve involvement perreflexia. Plantar reflexes may be difficult to elicit or included the glossopharyngeal, hypoglossal, and trigeminal interpret in patients with forefoot deformities or after foot nerves. surgery. Entrapment neuropathies, which are associated Urinary retention and later incontinence or rectal dis- with RA, can adversely affect the sensory examination turbances, or both, are symptoms of more severe disease of the upper extremity. and occur late in the progression. A patient who has been Traditional grading and classification systems for neuro- using crutches or a walker for ambulation and progresses logic deficits of RA patients are difficult to apply because of to the use of a wheelchair should raise the suspicion of cer- the comorbidities expressed and the multiple joint deficien- vical pathology. Other clinical manifestations reported in cies that occur. By nature of the disease itself, disability is the literature include amnestic episodes, brain stem signs, multifactorial (with a combination of arthropathy, deformity, and lower cranial nerve palsies, as well as signs consistent compressive neuropathy, and radiculopathies, as well as with Brown-Sequard syndrome.17,46,54 However, a study by myelopathy), as previously discussed. Any one of these Rogers and associates55 suggested that cranial nerve palsies, variables may adversely affect grading. The Ranawat grad- nystagmus, and other select brain stem dysfunctions are ing system, used commonly in the literature, is a valuable more accurately attributed to the co-morbidities associ- method for evaluating patients’ baseline neurologic function, ated with RA, rather than the direct mechanical effects of planning surgery, and examining postoperative outcome rheumatoid craniocervical deformities. These investiga- (Table 1).49 Other common classifications are that of the tors reported a low incidence of such problems in 235 RA American Rheumatological Association, which is the func- patients with craniocervical involvement. tional equivalent of the Steinbrocker classification (Table 2).50 Other grading scales in the literature are described but Diagnostic Evaluation have not been frequently applied.28,32,51,52 Plain Films Neck pain is the most common complaint, present Radiographic evaluation of the cervical spine in patients in 40% to 80% of patients,53 and located mostly at the with RA should be performed routinely, as well as preopera- craniocervical junction. It is usually associated with oc- tively, even in asymptomatic patients.56 This should include cipital headaches. Occipital neuralgia, facial pain, and ear lateral, anteroposterior (AP), open-mouth odontoid views, pain can occur from compression of the greater occipital and lateral flexion-extension dynamic views. Radiographic nerve (C2), the nucleus of the spinal trigeminal tract, changes representing early cervical involvement include and the greater auricular nerve, respectively. Pain in the odontoid erosion, disc narrowing, and atlantoaxial and sub- suboccipital region can also occur due to irritation of the axial subluxation. Precise evaluation of plain radiographs lesser occipital nerve (C1). Patients may describe a feel- is often difficult, due to osteopenia, anatomic variation, ing of their head falling forward with flexion and with a bony overlap, and most commonly, odontoid erosions. In a clunking sensation. They may also describe myelopathic retrospective review of 113 RA patients undergoing elective symptoms with cord and medullary compression, as well total hip or knee replacement, Collins and colleagues41 noted as upper or lower motor neuron signs, or both. Patients 69 individuals (61%) had evidence of cervical abnormalities may report weakness, loss of endurance, loss of dexter- on preoperative cervical radiographs. These abnormalities ity, gait disturbance, and paresthesias. Neck motion, included AAS, cranial settling, and subaxial subluxation. especially flexion, may cause electric shock sensation They also noted that 35/69 (50%) of patients with abnormal of the torso and extremities (Lhermitte’s sign), or either radiographs were asymptomatic. alone. Symptoms of tinnitus, vertigo, visual disturbances, loss of equilibrium, diplopia, and dysphagia can occur Cervical Instability due to either vertebrobasilar insufficiency or mechanical As discussed, the four common patterns of cervical insta- compression of the cervicomedullary junction. bility in rheumatoid disease are 1. isolated AAS; 2. cranial Occipital pain with radiation to the vertex is one of the settling associated with AAS; 3. subaxial subluxation; and most common symptoms in patients with cranial settling. 4. a combination of AAS, cranial settling, and subaxial Menezes and coworkers17 documented 100% prevalence in subluxation, or a combination of AAS with cranial settling 45 patients evaluated with RA and cranial settling. The inves- or subaxial subluxation. One should attempt to identify
Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 141
magnum), clivus, hard palate, atlas, pedicle of axis, and tip
of the odontoid process.
The AADI or ADI is measured from the posterior aspect
of the ring of atlas to the anterior aspect of the odontoid
process, as measured along the transverse axis of the ring
of the atlas. The normal value in an adult is less than 3 mm.
AAS is defined as a pre-odontoid interval greater than 3
mm and not fixed in dynamic flexion and extension views.8
Typically, the AADI is inversely related to the PADI or SAC
and is used because of the ease and reliability of measure-
ment. Commonly, the AADI has been utilized in following
patients with RA, and many studies have recommended
surgical intervention based on measures above 8, 9, or 10
mm.12,46,57 However, more recent studies have questioned the
utility of AADI and have shown that AADI is not a reliable
parameter in distinguishing patients with neurologic deficit
from those who are neurologically intact.41,45,58 With progres-
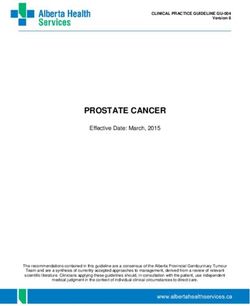
Figure 1 Midsagittal MRI of a 67-year-old female with long-
standing RA. The image demonstrates marked vertical subluxation sion of instability, the odontoid process migrates superiorly
of the dens. The tip of the dens impinges on the medulla and sig- within the ring of the atlas. With continued cranial settling,
nificantly reduces the functional cervicomedullary angle (normal the AADI may paradoxically decrease, and even become
range: 135° to 175°). The ADI paradoxically decreases and may fixed, resulting in pseudostabilization (Fig. 1), as previously
fall into the “normal” range. described.18,59 More recently, the PADI has been reported as
a more reliable predictor of neurologic compromise. The
critical landmarks on the lateral cervical plain radiograph PADI is measured from the posterior aspect of the odon-
to facilitate serial diagnostic and prognostic measurements. toid process to the anterior edge of the posterior ring of the
These include the opisthion (the dorsal border of the fora- atlas (as measured along the transverse axis of the ring of
men magnum), basion (the ventral border of the foramen the atlas). In a recent study by Boden and coworkers,45 they
Table 3 Indices of Cranial Settling
Description
Measurement Line is Drawn From-To Diagnostic Criteria
McGregor’s line62 Posterior tip of the hard palate to the most caudal Cranial settling is diagnosed when the apex of
(lowest) cortical margin of the occiput. the dens rises more than 4.5 mm above this line.
McRae’s line63 Foramen magnum, from the basion to the Protrusion of the tip of the dens above this line
opisthion (posterior rim of foramen magnum). indicates cranial settling.
Chamberlain’s line60 Posterior aspect of the hard palate to the Protrusion of the tip of the dens more than 3 mm
opisthion. above this line indicates cranial settling.
Wackenheim’s line64 Drawn along the superior surface of the clivus. Protrusion of the dens posterior to the projection
of this line indicates settling.
Fischgold-Metzger’s Drawn between the tips of mastoid processes on Protrusion of the tip of the dens above this line
line61 the anteroposterior open-mouth odontoid view. indicates cranial settling.
Ranawat index49 Center of the C2 pedicle to the transverse axis of (Normal range: Males: 17 ± 2 mm; Females: 15
the atlas. ± 2 mm.)
Measurement decreases as C1-C2 vertical
subluxation occurs.
Redlund-Johnell McGregor’s line to the midpoint of the caudal (Normal: Males ≥ 34 mm; Females ≥ 29 mm).
measurement24 margin of the C2 body. Measurement decreases as C1-C2 vertical
subluxation occurs.
Clark and colleagues57 Dividing the odontoid process into three equal Station I: Anterior ring of atlas is level with
(Simplest method, parts, or stations, from superior to inferior. superior third of odontoid process (normal).
relationships do not Assess which station of the odontoid process is Station II: The anterior ring of atlas is adjacent to
change in flexion, adjacent to the anterior ring of the atlas. the middle third of the dens (mild).
extension, or neutral Station III: The anterior ring of atlas is adjacent
views) to the caudal third of the dens (severe).142 Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48
Figure 2 A, Lateral cervical ra-
diograph of a 68-year-old female
with RA erosion of the dens. B,
Lateral flexion view demonstrat-
ing anterior atlantoaxial sublux-
ation (AAS). The ADI cannot be
directly measured, as the dens is
not visible radiographically. Note
A B the break in the spinolaminar line
between C1 and C2.
noted 60% (19/32) of patients who had AAS and paralysis Cranial Settling and AAS
had an AADI that was less than 9 mm. This weak correlation Cranial settling can be evaluated with a variety of measure-
between AADI and paralysis may be due to variations in the ments on plain films, such as the relationship of the tip of
diameter of the atlas as well as in pannus formation behind the dens to McGregor’s line, McRae’s line, and Chamber-
the odontoid process. Ninety-six percent (23/24) of patients lain’s line, among others (Table 3).60-64 Measurements may
with AAS and a Ranawat class III neurological deficit had a be difficult to obtain when there is erosion of the dens and
PADI of less than or equal to 13 mm; patients in their series the overlying mastoid air cells degrade the view of the dens
who had a Ranawat class II (n = 11) or a class I rating (n on a lateral radiograph (Figs. 2A and 2B), or either of these
= 31) had mean PADIs of 13 and 15 mm, respectively. A situations exist singly. Two common measurements are the
PADI of 14 mm or less yielded 97% sensitivity and 52% Ranawat index49 and the Redlund-Johnell values (Table 3).24
specificity for detecting patients with paralysis, compared to The anatomic landmarks used for these measurements are
an AADI of greater than 8 mm with a 59% sensitivity, 58% usually clearly seen on lateral films (Figs. 3 and 4). The
specificity, and 56% negative predictive value; patients with abnormal Ranawat index most likely represents a settling
a PADI of greater than 14 mm had no neurologic deficits. at the C1-C2 level and the Redlund-Johnell value reflects
Figure 3 Commonly drawn lines and measurements to assess Figure 4 Commonly drawn lines and measurements to assess
occipito-C1-C2 relationships. The lines in this figure are somewhat occipito-C1-C2 relationships. These lines are based on clearly
arbitrary, as the center of the various landmarks must be estimated. defined cortical landmarks.Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 143
negative measurements for cranial settling after reviewing
plain radiographs.
Subaxial Subluxation and AAS
Lower, or subaxial, cervical spine lesions occur with changes
in apophyseal joints, the joints of Luschka, interspinous
ligaments, and intervertebral discs. As per White and co-
workers,66 the criterion for diagnosing subaxial subluxation
is 3.5 mm or more of motion. Boden and associates45 noted
that subluxation with a SAC of 14 mm or less represents
a more accurate measurement for risk of neurologic dys-
function, as well as postoperative recovery. Yonezawa and
colleagues67 evaluated 58 RA patients neurologically and
radiographically after 5 to 10 years of follow-up. Progres-
sion of myelopathy correlated with anterior subluxation (>
2 mm) and axial shortening, accompanied by progression
of disc collapse, apophyseal joint erosion, and spinous
Figure 5 Clark’s stations. process destruction. These parameters progressed in 50%
of patients. One-fourth to one-third of patients who had
occiput-C2 changes. In 1989, Clark and associates57 de- radiographic progression had a potential for myelopathic
scribed a method by defining three equidistant stations of the changes. Progression of radiographic lesions and deteriora-
odontoid process of the axis (Fig. 5). Normally, the superior tion of myelopathy was mainly correlated with a higher dose
third of the odontoid is level with or adjacent to the anterior of corticosteroids, higher stage (or class) of RA, younger
ring of the atlas. With mild cranial settling, the middle third patients, and those with longer duration of disease. The
of the odontoid process is level with the anterior ring of the findings of this study were also correlated with the results
atlas (station II). With severe cranial settling, the inferior of a study done by Klein and coworkers.68
third of the odontoid process is level with the anterior ring
of the atlas (station III). Advanced Imaging
In 2001, Riew and colleagues 65 published a review Advanced radiographic imaging technology is utilized to
of 131 patients with rheumatoid cervical spine. They evaluate the presence of cord compression, to determine the
evaluated the interobserver and intraobserver reliabilities, presence of multilevel disease, and to help predict impending
sensitivity, specificity, and negative and positive predictive paralysis. Tomograms are particularly useful in determin-
values for several measurements used to diagnose cranial ing the amount of cranial settling and to measure SAC or
settling. The most easily identified landmarks were the hard AADI values. Cervical myelography, polytomography, and
palate, “definitely visible” on 93% (62/67) of radiographs, computed tomography (CT) with intrathecal contrast have all
and the atlas, which was “definitely seen” on 88% (59/67) been used to evaluate rheumatoid cervical spine pathologies.
of radiographs. The tip of the odontoid process was the least Magnetic resonance imaging (MRI) and CT scans, providing
clearly identifiable landmark, having been “definitely seen” both sagittal and coronal views, have largely replaced these
on only 34% (22/67) of radiographs, and was completely studies. CT scans can contribute detailed osseous informa-
unidentifiable in 19% (13/67). Of the remaining 31 radio- tion and have been shown to have a higher correlation with
graphs (46%), the tip of the dens could only be “guessed.” neurologic deficits than that of AADI assessment. Raskin
No single test had a sensitivity or negative predictive value and associates69 noted a significant increase in the AADI in
greater than 90% or a reasonable specificity or positive 19 patients; however, CT scan showed cord compression
predictive value. However, the combination of Clark’s sta- in 11, and an absence of compression in the other eight pa-
tions, the Ranawat index, and the Redlund-Johnell value tients. These investigators also noted that absent superficial
was superior when compared to any single criterion by abdominal reflexes and a history of bladder dysfunction cor-
itself. The combined value had a sensitivity of 94% and related highly with cord compression on CT. Furthermore,
a negative predictive value of 91% for diagnosing cranial CT myelography is useful in patients who have contraindica-
settling if any of the three were positive. Consequently, only tions to MRI scanning.
6% of patients with cranial settling were improperly diag- MRI provides explicit information of soft tissue lesions,
nosed as not having this manifestation. The investigators the neuraxis, and epidural tissues and continues to be the
recommended that if any of these values are suggestive of imaging modality of choice in determining neural compres-
cranial settling, a tomograph or MRI should be performed, sion. The main advantage of an MRI over other imaging
or, alternatively, whenever there is clinical suspicion of procedures is that anatomic structures can be visualized in
cervicomedullary or brainstem dysfunction in the setting of all planes, without bone artifact or beam hardening effects.70144 Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48
statistically significant subarachnoid space narrowing rela-
tive to the neutral position at the atlantoaxial level and below
C2. This narrowing significantly affected cord compression
at the atlantoaxial level if there was some encroachment on
neutral MRI images. Other studies have also highlighted
the usefulness and clinical application of dynamic flexion-
extension MRI scanning in evaluating RA involvement of
the cervical spine.71,76 Allmann and colleagues77 performed
dynamic MR imaging of the cervical spine and observed
12% of patients with subarachnoid encroachment in flex-
ion that was not evident on neutral MRI. In a more recent
prospective study, Reijnierse and coworkers78 observed a
five-fold increased risk of neurologic dysfunction when MRI
revealed atlas erosion and cranial settling, as evidenced by a
decreased distance of the dens to McRae’s line. Furthermore,
subarachnoid space encroachment was associated with a
12-fold increased risk of neurologic dysfunction. They also
associated muscle weakness with a 10-fold increased risk
of neurologic dysfunction.
Electrophysiologic Modalities
Evaluation of neurologic signs and symptoms may be dif-
ficult in patients with advanced rheumatoid deformities or
following surgical treatment. Electrophysiologic modali-
ties can serve as additional adjunctive tests in diagnosing
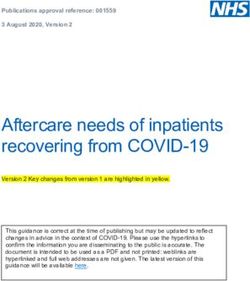
Figure 6 Sagittal T1-weighted MRI demonstrating advanced
pannus formation eroding the dens. and following myelopathy in this patient population. They
also can differentiate between radicular and spinal cord
An MRI should be obtained in any patient with a neurologic involvement. Toolanen and colleagues79 observed abnormal
deficit or abnormalities on plain films. A strong correlation somatosensory evoked potentials (SSEPs) in 22% (4/18)
has been found between MRI and myelography, with respect of patients with subluxation. Lachiewicz and coworkers80
to the diagnosis of compressive cervical spine and clinical demonstrated that all patients with reducible atlantoaxial
evidence of cervical myelopathy in RA patients.70-72 MRI can or subaxial subluxation had normal SSEPs. However, 58%
demonstrate cord compression due to bone as well as soft tis- (7/12) of those with irreducible AAS or cranial settling, or
sue mass, such as the peri-odontoid pannus (Fig. 6). Dvorak both, had abnormal SSEPs. In another study, SSEPs have
and colleagues73 reported two-thirds of patients (22/34) with been shown to have a sensitivity of 58% and a specificity
AAS had more than 3 mm of pannus; furthermore, a cord of 90% in detecting AAS in patients with RA.81 Motor
diameter of 6 mm in flexion was highly consistent with neu- evoked potentials also have been used to evaluate cervical
rological deficits. Bundschuh and coworkers74 described the spine disease; 67% of 55 patients with RA had an abnormal
cervicomedullary angle as the angle between a line drawn delay in the latency of the central motor evoked potentials
along the anterior aspects of the cervical cord and another consistent with neural element compression.82
line along the medulla. The normal angle is between 135° In summary, the radiographic predictors of paralysis are
and 175° (Fig. 1). Patients with a cervicomedullary angle as follows: a PADI of less than 14 mm, any combination
of less than 135° had cranial settling and clinical signs of of AAS with cranial settling, a subaxial canal diameter of
C2 root pain, neural compression, or myelopathy. Reijnierse less than 14 mm, MRI findings of either a cervicomedullary
and associates75 evaluated 42 patients with RA to assess the angle of less than 135°, a cord diameter in flexion of less
changes in radiologic measurements between neutral and than 6 mm, or a SAC measure of less than 13 mm. Other
flexion MRI views. They reported that the cervicomedullary recent predictors of paralysis noted in the literature include
angle changed from 126° to 165° (median, 145°) in neutral subaxial anterior subluxation (> 2 mm) and axial shorten-
position to 118° to 165° (median, 140°) in the flexed position. ing, accompanied by progressive disc collapse, apophyseal
However, there was no significant change in compression joint erosion, spinous process destruction, and subarachnoid
of the brainstem between images obtained in the flexed and narrowing on MRI.
neutral positions. They suggested that the distance of the
dens to McRae’s line and the amount of pannus were inde- Predictors of Neurologic Recovery
pendent determinants of the cervicomedullary angle. These As discussed earlier, Pellicci and colleagues39 reviewed
investigators also found that flexion MRI can demonstrate 106 patients followed over a 5-year period, with 46 (43%)Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 145
having cervical spine involvement at the start of the study.
Eighty percent had radiographic, while 36% had neurologic
progression (most by one grade). Mortality rate was 17%,
compared to 9% for the same age group without RA. In
1987, Santavirta and coworkers83 noted in their review of
34 patients with rheumatoid cervical spine that only one of
16 patients treated nonoperatively had an improvement in
pain. Neurologic function diminished in all patients treated
nonoperatively. Marks and Sharp48 reviewed 31 patients with
RA and cervical myelopathy. They noted that 19/31 patients
died, with 15 deaths (48%) occurring within 6 months. They
also reported that all nonoperatively treated patients and half
of those treated with collars died. In this historical paper,
four patients were treated with occipitocervical fusion and
the three who developed successful fusions survived and
had excellent outcomes. These results were similar to that of
Meijers and associates,43 who reported that 9 patients with
myelopathy who were treated nonoperatively all died within
1 year, with four deaths arising from cord compression.
Certain clinical and radiographic parameters factors
have been shown to be associated with a poor neurologic
recovery after operative stabilization with or without de-
compression: 1. patients with a more severe preoperative
neurologic dysfunction have less chance of an uneventful
postoperative recovery84; 2. the location of pathology, e.g.,
cranial settling, especially in combination with AAS, has a Figure 7 Lateral cervical radiograph of a 55-year-old female with a
significantly worse prognosis than isolated atlantoaxial or C1-C2 fusion. The arthrodesis was performed for rheumatoid atlan-
subaxial subluxation45,58,59,85; and 3. the Ranawat grading sys- toaxial subluxation 9 years prior. There is no radiographic evidence
of occipitocervical pathology nor signs of subaxial involvement.
tem provides a rough estimate of neurological recovery, with
a progressively worsening prognosis in patients with stage III
compared to stage II, and IIIb compared to IIIa.45,84-87 Casey 15 patients had worsening or recurrence of their neurologic
and colleagues84 evaluated 134 patients who underwent sur- findings; thirteen (86.7%) were caused by later subaxial
gery for rheumatoid involvement of the cervical spine after subluxation.
development of objective signs of myelopathy. Fifty-eight Several studies have demonstrated that preoperative SAC
percent of the ambulatory patients (IIIA) attained Ranawat and postoperative subaxial canal diameter are important
neurological grades I or II as compared with only 20% of the specific predictors of neurologic recovery. Patients with
nonambulatory patients (IIIB). They also observed that those isolated AAS and a PADI of more than 14 mm have a better
patients with Ranawat index IIIB also fared worse in regard chance of recovery. However, those with a PADI of less than
to postoperative complication rate, length of hospital stay, 10 mm prior to surgery have a poor prognosis for functional
functional outcome, and ultimately survival when compared recovery. Furthermore, patients with combined AAS and
to patients with Ranawat IIIA. Peppelman and coworkers85 cranial settling are expected to have a better neurologic
reviewed the results of 90 patients with rheumatoid deformi- recovery if their PADIs are at least 13 mm. Patients suffer-
ties of the cervical spine with objective neurologic deficits ing from subaxial subluxation with a postoperative canal
and who were surgically treated. Seventy-eight (86.7%) had diameter less than 14 mm will have less neurologic recovery
improvement of at least one Ranawat class postoperatively. after surgical intervention.45 However, patients with a spinal
Fifty-eight patients had objective signs of paresis before cord area of 44 mm or greater have been shown to have a
surgery (IIIA, IIIB); 49 (84.4%) of these individuals obtained good prognosis postoperatively.85 Patient factors that do not
resolution of the paresis after surgery. Among the patients appear to correlate with neurologic recovery after operative
with AAS and neurologic findings without cranial settling, treatment for rheumatoid cervical spine include gender, age,
94.8% of patients in their series improved at least one class. duration of disease and paralysis before surgery, percent of
Seventy-six percent of patients with neurologic deficits in preoperative subaxial vertebral subluxation, and preoperative
the setting of AAS and cranial settling improved one class, anterior atlantoaxial interval.87
whereas 71% of patients with neurologic findings with The manifold rationale for performing C1-C2 fusions
combined AAS, cranial settling, and subaxial subluxation (Fig. 7) when significant anterior instability is identified are:
improved at least one class. Furthermore, in their cohort, 1. earlier performance of a monosegmental atlantoaxial fu-146 Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48
sion can decrease the development of superior migration of 7. Bland JH. Rheumatoid arthritis of the cervical spine. Bull
the odontoid; 2. the increase in stress on the subaxial spine Rheum Dis. 1967;18:471-6.
will also be reduced compared to having an occiput-to-C2 8. Fielding JW, Cochran GB, Lawsing JF, 3rd, Hohl M. Tears
fusion, that would be indicated to manage more advanced of the transverse ligament of the atlas. A clinical and biome-
chanical study. J Bone Joint Surg Am. 1974;56:1683-91.
vertical atlantoaxial subluxation; and 3. surgical intervention
9. Lipson SJ. Cervical myelopathy and posterior atlanto-axial
in patients with Ranawat class IIIA findings may also aid in
subluxation in patients with rheumatoid arthritis. J Bone Joint
preventing subsequent irreversible cord damage. Surg Am. 1985;67:593-7.
10. Santavirta S, Slatis P, Kankaanpaa U, et al. Treatment of the
Conclusion cervical spine in rheumatoid arthritis. J Bone Joint Surg Am.
RA is a chronic, systemic inflammatory disorder of unknown 1988;70(5):658-67.
etiology. It is an immunologically mediated disorder that can 11. Halla JT, Fallahi S, Hardin JG. Nonreducible rotational head
affect the articular and non-articular organ systems. Axial tilt and lateral mass collapse. A prospective study of frequency,
involvement predominantly affects the upper cervical spine. radiographic findings, and clinical features in patients with
The morbidity of the disorder can have profound effects on rheumatoid arthritis. Arthritis Rheum. 1982;25(11):1316-24.
an individual’s activities of daily living as a consequence of 12. Weissman BN, Aliabadi P, Weinfeld MS, et al. Prognostic
features of atlantoaxial subluxation in rheumatoid arthritis
deformity, pain, and neurological dysfunction. Early initia-
patients. Radiology 1982;144(4):745-51
tion of pharmacotherapy using DMARDS in combination
13. Agarwal AK, Peppelman WC, Kraus DR, et al. Recurrence
with newer immunological mediators reduces the inflam- of cervical spine instability in rheumatoid arthritis following
matory components of RA. Indeed, initiation of aggressive previous fusion: can disease progression be prevented by early
therapy prior to cartilage destruction may actually prevent surgery? J Rheumatol. 1992;19(9):1364-70.
or significantly mitigate destabilizing cervical joint damage 14. Kraus DR, Peppelman WC, Agarwal AK, et al. Incidence of
and reduce the need for surgical intervention. Radiographs of subaxial subluxation in patients with generalized rheumatoid
the cervical spine should be performed initially and within arthritis who have had previous occipital cervical fusions.
2 years after diagnosis of RA, and periodically thereafter. Spine 1991;16(10 Suppl):S486-9.
Dynamic cervical images should be taken prior to any elec- 15. Reijnierse M, Bloem JL, Dijkmans BA, et al. The cervical
tive operation to rule out instability. Operative intervention spine in rheumatoid arthritis: relationship between neurologic
signs and morphology of MR imaging and radiographs. Skel-
before the onset of advanced myelopathy results in improved
etal Radiol. 1996;25(2):113-8.
outcomes, compared to the stabilization of patients whose
16. El-Khoury GY, Wener MH, Menezes AH, et al. Cranial settling
conditions are more advanced. A multidisciplinary approach in rheumatoid arthritis. Radiology. 1980;137:637-42.
involving medical, surgical, and rehabilitation disciplines is 17. Menezes AH, VanGilder JC, Clark CR, el-Khoury G. Odontoid
necessary to optimize outcomes. upward migration in rheumatoid arthritis. An analysis of 45
patients with “cranial settling.” J Neurosurg. 1985;63(1):500-
Disclosure Statement
9.
None of the authors have financial or proprietary interest 18. Casey AT, Crockard HA, Geddes JF, Stevens J. Vertical trans-
in the subject matter or materials discussed, including, but location: the enigma of the disappearing atlantodens interval
not limited to, employment, consultancies, stock ownership, in patients with myelopathy and rheumatoid arthritis. Part
honoraria, and paid expert testimony. I. Clinical, radiological, and neuropathological features. J
Neurosurg. 1997;87:856-62.
References 19. Mathews JA. Atlanto-axial subluxation in rheumatoid arthritis.
1. Garrod, AE. A Treatise on Rheumatism and Rheumatoid A 5-year follow-up study. Ann Rheum Dis. 1974;33(6):526-
Arthritis. London: Griffins Medical Series. Charles Grif- 31.
fin & Co., 1890. Available at: http://books.google.com/ 20. Ball J. Pathology of the rheumatoid cervical spine. [Abstract]
bkshp?hl=en. Accessed July 11, 2011. Ann Rheum Dis. 1958;17:121.
2. Davis FW, Jr, Markley HE. Rheumatoid arthritis with death 21. Bland JH. Rheumatoid arthritis of the cervical spine. J Rheu-
from medullary compression. Ann Intern Med. 1951;35:451-4. matol. 1974;1:319-42.
3. Kornblum D, Clayton ML, Nash HH. Non-traumatic cervi- 22. Lipson SJ. Rheumatoid arthritis in the cervical spine. Clin
cal dislocations in rheumatoid spondylitis. J Am Med Assoc. Orthop Relat Res. 1989(239):121-7.
1952;149:431-5. 23. Martel W. Pathogenesis of cervical discovertebral destruction
4. Paimela L, Laasonen L, Kankaanpää E, Leirisalo-Repo M. in rheumatoid arthritis. Arthritis Rheum. 1977;20(6):1217-25.
Progression of cervical spine changes in patients with early 24. Redlund-Johnell I, Pettersson H. Radiographic measurements
rheumatoid arthritis. J Rheumatol. 1997;24(7):1280-4. of the cranio-vertebral region. Designed for evaluation of
5. Moskovich, R. Inflammatory arthritis of the cervical spine. In: abnormalities in rheumatoid arthritis. Acta Radiol Diagn
Spivak JM, Di Cesare PE, Feldman DS, et al. (eds): Ortho- (Stockh). 1984;25(1):23-8.
apedics: A Study Guide. New York: McGraw-Hill, pp. 373-80. 25. Santavirta S, Konttinen YT, Sandelin J, Slatis P. Opera-
6. Moskovich R, Shott S, Zhang ZH. Does the cervical canal tions for the unstable cervical spine in rheumatoid arthritis.
to body ratio predict spinal stenosis? Bull Hosp Jt Dis. Sixteen cases of subaxial subluxation. Acta Orthop Scand.
1996;55:61-71. 1990;61(2):106-10.Bulletin of the NYU Hospital for Joint Diseases 2011;69(2):136-48 147
26. Winfield J, Young A, Williams P, Corbett M. Prospective study toid arthritis of the cervical spine. A long-term analysis with
of the radiological changes in hands, feet, and cervical spine in predictors of paralysis and recovery. J Bone Joint Surg Am.
adult rheumatoid disease. Ann Rheum Dis. 1983;42(6):613-8. 1993;75:1282-97.
27. Kudo H, Iwano K. Surgical treatment of subaxial cervical 46. Rana NA. Natural history of atlanto-axial subluxation in
myelopathy in rheumatoid arthritis. J Bone Joint Surg Br. rheumatoid arthritis. Spine. 1989;14:1054-6.
1991;73(3):474-80. 47. Santavirta S, Konttinen YT, Laasonen E, et al. Ten-year results
28. Crockard HA. Surgical management of cervical rheumatoid of operations for rheumatoid cervical spine disorders. J Bone
problems. Spine. 1995;20:2584-90. Joint Surg Br. 1991;73:116-20.
29. Webb FW, Hickman JA, Brew DS. Death from verte- 48. Marks JS, Sharp J. Rheumatoid cervical myelopathy. Q J Med
bral artery thrombosis in rheumatoid arthritis. Br Med J. 1981;50:307-19.
1968;2(5604):537-8. 49. Ranawat CS, O’Leary P, Pellicci P, et al. Cervical spine fusion
30. Mikulowski P, Wollheim FA, Rotmil P, Olsen I. Sudden death in rheumatoid arthritis. J Bone Joint Surg Am. 1979;61:1003-
in rheumatoid arthritis with atlanto-axial dislocation. Acta 10.
Med Scand. 1975;198(6):445-51. 50. Steinbrocker O, Traeger CH, Batterman RC. Therapeutic
31. Henderson FC, Geddes JF, Crockard HA. Neuropathology of criteria in rheumatoid arthritis. JAMA. 1949;140:659-62.
the brainstem and spinal cord in end stage rheumatoid arthritis: 51. Hirabayashi K, Watanabe K, Wakano K, et al. Expansive open-
implications for treatment. Ann Rheum Dis. 1993;52(9):629- door laminoplasty for cervical spinal stenotic myelopathy.
37. Spine. 1983;8:693-9.
32. Delamarter RB, Bohlman HH. Postmortem osseous and 52. Nurick S. The pathogenesis of the spinal cord disorder associ-
neuropathologic analysis of the rheumatoid cervical spine. ated with cervical spondylosis. Brain. 1972;95(1):87-100.
Spine. 1994;19:2267-74. 53. Rawlins BA, Girardi FP, Boachie-Adjei O. Rheumatoid
33. Bell HS. Paralysis of both arms from injury of the upper arthritis of the cervical spine. Rheum Dis Clin North Am.
portion of the pyramidal decussation: “cruciate paralysis.” J 1998;24:55-65.
Neurosurg. 1970;33:376-80. 54. Rana NA, Hancock DO, Taylor AR, Hill AG. Upward trans-
34. Zeidman SM, Ducker TB. Rheumatoid arthritis. Neu- location of the dens in rheumatoid arthritis. J Bone Joint Surg
roanatomy, compression, and grading of deficits. Spine. Br. 1973 Aug;55(3):471-7.
1994;19:2259-66. 55. Rogers MA, Crockard HA, Moskovich R, et al. Nystagmus
35. Agarwal AK, Peppelman WC, Jr, Kraus DR, Eisenbeis and joint position sensation: their importance in poste-
CH, Jr. The cervical spine in rheumatoid arthritis. BMJ. rior occipitocervical fusion in rheumatoid arthritis. Spine.
1993;306(6870):79-80. 1994;19:16-20.
36. Halla JT, Hardin JG, Vitek J, Alarcon GS. Involvement of 56. Kwek TK, Lew TW, Thoo FL. The role of preoperative cer-
the cervical spine in rheumatoid arthritis. Arthritis Rheum. vical spine X-rays in rheumatoid arthritis. Anaesth Intensive
1989;32:652-9. Care. 1998 Dec;26(6):636-41.
37. Sharp J, Purser DW. Spontaneous atlanto-axial dislocation in 57. Clark CR, Goetz DD, Menezes AH. Arthrodesis of the cer-
ankylosing spondylitis and rheumatoid arthritis. Ann Rheum vical spine in rheumatoid arthritis. J Bone Joint Surg Am.
Dis. 1961 Mar;20(1):47-77. 1989;71:381-92.
38. Riise T, Jacobsen BK, Gran JT. High mortality in patients 58. Boden SD. Rheumatoid arthritis of the cervical spine. Surgical
with rheumatoid arthritis and atlantoaxial subluxation. J decision making based on predictors of paralysis and recovery.
Rheumatol. 2001;28:2425-9. Spine. 1994;19:2275-80.
39. Pellicci PM, Ranawat CS, Tsairis P, Bryan WJ. A prospective 59. Casey AT, Crockard HA, Stevens J. Vertical translocation. Part
study of the progression of rheumatoid arthritis of the cervical II. Outcomes after surgical treatment of rheumatoid cervical
spine. J Bone Joint Surg Am. 1981;63:342-50. myelopathy. J Neurosurg. 1997;87:863-9.
40. Sunahara N, Matsunaga S, Mori T, et al. Clinical course of 60. Chamberlain WE. Basilar impression (platybasia): a bizarre
conservatively managed rheumatoid arthritis patients with developmental anomaly of the occipital bone and upper cervi-
myelopathy. Spine. 1997;22:2603-7; discussion 8. cal spine with striking and misleading neurologic manifesta-
41. Collins DN, Barnes CL, FitzRandolph RL. Cervical spine tions. Yale J Biol Med. May 1939;11:487-96.
instability in rheumatoid patients having total hip or knee 61. Fischgold H, Metzger J. Etude radiotomographique
arthroplasty. Clin Orthop Relat Res. 1991:127-35. de l’impression basilaire. Rev Rheum Mal Osteoartic.
42. Kauppi M, Konttinen YT, Honkanen V, et al. A multivariate 1952;19:261-8. [French].
analysis of risk factors for anterior atlantoaxial subluxation 62. McGregor M. The significance of certain measurements of
and an evaluation of the effect of glucocorticoid treatment the skull in the diagnosis of basilar impression. Br J Radiol.
on the upper rheumatoid cervical spine. Clin Rheumatol. 1948;21:171-81.
1991;10:413-8. 63. McRae DL, Barnum AS. Occipitalization of the atlas. Am J
43. Meijers KA, Cats A, Kremer HP, et al. Cervical myelopathy Roentgenol Radium Ther Nucl Med. 1953;70:23-46.
in rheumatoid arthritis. Clin Exp Rheumatol. 1984;2:239-45. 64. Wackenheim A. Disostosi chiro-lombare. Disostosi stenotica
44. Rasker JJ, Cosh JA. Radiological study of cervical spine and del canale vertebrale e brachichiria. Radiologia Medica.
hand in patients with rheumatoid arthritis of 15 years’ dura- 1979;65:21-6. [Italian]
tion: an assessment of the effects of corticosteroid treatment. 65. Riew KD, Hilibrand AS, Palumbo MA, et al. Diagnosing basi-
Ann Rheum Dis. 1978;37:529-35. lar invagination in the rheumatoid patient. The reliability of
45. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheuma- radiographic criteria. J Bone Joint Surg Am. 2001;83(2):194-You can also read