The Revised FIGO Staging System for Uterine Malig-nancies: Implications for MR Imaging1
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Note: This copy is for your personal non-commercial use only. To order presentation-ready
copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
PELVIC MALIGNANCY 1805
The Revised FIGO Staging
System for Uterine Malig-
nancies: Implications for
MR Imaging1
Susan J. Freeman, MRCP, FRCR • Ahmed M. Aly, PhD • Masako Y.
ONLINE-ONLY
CME Kataoka, MD, PhD • Helen C. Addley, MRCP, FRCR • Caroline Reinhold,
See www.rsna
MD, MSc • Evis Sala, MD, PhD, FRCR
.org/education
/search/RG Cancers of the uterine corpus and cervix are the most common gyneco-
logic malignancies worldwide. The International Federation of Gynecol-
LEARNING ogy and Obstetrics (FIGO) staging system was first established in 1958,
OBJECTIVES when it was recognized that the recurrence rate and patient outcomes
After completing this were directly related to the degree of tumor spread at the patient’s initial
journal-based CME
activity, participants presentation. Changes in understanding of tumor biology led to a recent
will be able to: update in the FIGO staging system that reflects the variation in treat-
■■Listthe revised
FIGO stages for
ment strategies between endometrial and cervical cancer. Patients with
both cervical and endometrial cancer are primarily treated with hysterectomy; thus, stag-
endometrial car-
cinoma and their
ing is done at surgery and histologic analysis. Magnetic resonance (MR)
respective manage- imaging may accurately depict the extent of endometrial cancer at diag-
ment implications.
nosis and, in conjunction with the tumor grade and histologic subtype,
■■Discuss the op-
timal MR imaging help stratify risk, which determines the therapeutic course. Cervical
sequences and pro- carcinoma is staged at clinical examination because many tumors are
tocols for staging
uterine malignancies. inoperable at the time of patient presentation. Preoperative MR imaging
■■Describe the ap- criteria are not formally included in the revised FIGO staging system
pearances of the because cervical carcinoma is most prevalent in developing countries,
different stages of
uterine malignancy where imaging resources are limited. However, MR imaging is highly
at MR imaging. sensitive and specific for depicting important prognostic factors and,
when available, is recommended as an adjunct to clinical examination.
The MR imaging findings of uterine carcinoma should be discussed in
a multidisciplinary setting in conjunction with clinical and histologic
findings, an approach that provides accurate staging and risk stratifica-
tion and allows for individualized treatment.
©
RSNA, 2012 • radiographics.rsna.org
Abbreviations: ADC = apparent diffusion coefficient, DWI = diffusion-weighted imaging, ESUR = European Society of Urogenital Radiology,
FIGO = International Federation of Gynecology and Obstetrics, NCCN = National Comprehensive Cancer Network
RadioGraphics 2012; 32:1805–1827 • Published online 10.1148/rg.326125519 • Content Codes:
1
From the Department of Radiology, Box 218, Addenbrooke’s Hospital, Cambridge University Hospitals Trust, Hills Rd, Cambridge, CB2 0QQ,
England (S.J.F., H.C.A., E.S.); Department of Radiology, National Cancer Institute, Cairo University, Cairo, Egypt (A.M.A.); Department of Diagnostic
Radiology, Kyoto University Hospital, Kyoto, Japan (M.Y.K.); and Department of Radiology, McGill University Health Centre, Montreal, Quebec, Canada
(C.R.). Received April 10, 2012; revision requested May 7 and received June 1; accepted June 20. For this journal-based CME activity, the authors, editor,
and reviewers have no relevant relationships to disclose. Address correspondence to S.J.F. (e-mail: sue.freeman@addenbrookes.nhs.uk).
©
RSNA, 20121806 October Special Issue 2012 radiographics.rsna.org
Introduction be depicted at MR imaging and used as a road
Endometrial and cervical carcinomas are the map for sampling at surgery. MR imaging fea-
most common gynecologic malignancies world- tures of abnormal lymph nodes include clusters
wide: Endometrial cancer is the most common of multiple small lymph nodes, necrosis, and sig-
gynecologic cancer in industrialized countries, nal intensity similar to that of the primary tumor.
whereas cervical cancer is most common in de- MR imaging findings are reviewed in conjunction
veloping countries. The International Federation with the tumor grade determined on the basis of
of Gynecology and Obstetrics (FIGO) staging endometrial biopsy and histologic findings at the
system is the most widely accepted method for multidisciplinary team meeting or tumor board
staging endometrial and cervical cancers (1). The conference. This meeting provides an accurate
first FIGO staging system was created in 1958. risk stratification, which determines the progno-
It was updated in 1988 and was most recently sis and management strategy, including whether
revised in 2009. Cancer staging is fundamen- lymph node dissection is necessary (6). In the
tally important in treating patients with cancer United Kingdom and other countries, risk strati-
and must be reliable, reproducible, and practi- fication determines whether patients are treated
cal. Unified criteria must be established to en- at a local center (those with low and intermediate
able treatment planning, assess tumor response, risk) or a specialist gynecologic oncology center
predict prognosis, and allow information to be (those with high risk).
exchanged between different treatment centers MR imaging may also provide additional use-
(2). This process ensures that identical cases are ful information, including the size of the uterus,
accurately assigned a tumor stage, which leads to tumor volume, presence of ascites, and adnexal
consistent management decisions and is reflected pathologic characteristics, that may guide the
in similar clinical outcomes, and it provides a surgical approach (eg, transabdominal, trans-
major prognostic factor in predicting the rate of vaginal, or laparoscopic). Pelvic and paraaortic
recurrence and patient outcomes. Changes in our lymph node dissection is not routinely performed
understanding of tumor biology led to a recent in low- and intermediate-risk patients because
update in the FIGO staging system in June 2009. its clinical benefit remains uncertain (7–10).
Cancer classification systems must continue to However, if suspicious lymph nodes are seen
respond to changes in our knowledge of tumor preoperatively or in the presence of a high-grade,
etiology, pathogenesis, and predisposing genetic high-stage tumor at MR imaging, lymph node
factors because they affect prognosis. dissection may be considered (10). In medically
The FIGO staging system for endometrial and high-risk patients, MR imaging may be useful in
cervical cancers reflects their different clinical planning nonsurgical treatment options.
management strategies. Management of endo- In contrast, although cervical cancer is the
metrial carcinoma is primarily surgical, whereas third most common gynecologic malignancy in
that for cervical carcinoma depends on the FIGO the United States, it remains the most common
stage at the time of its manifestation. MR imag- gynecologic malignancy worldwide (11,12).
ing has an integral role in evaluating the extent of Cervical cancer screening programs and im-
disease and managing its pathway. provements in chemoradiotherapy have helped
The primary treatment for patients with en- reduce mortality in industrialized nations. Nev-
dometrial cancer is hysterectomy; for this reason, ertheless, cervical carcinoma remains a common
staging is done on the basis of surgical and his- cause of cancer-related death among women in
tologic findings. However, MR imaging has been developing countries. Given its epidemiologic
shown to accurately delineate the local extent of characteristics, the FIGO staging system must
disease and depict extrauterine tumor spread. reflect the available resources: Any system must
MR imaging accurately depicts the depth of myo- allow for uniform staging between different cen-
metrial invasion and cervical stromal invasion ters and countries and remain practical, acces-
and may depict metastatic spread, including peri- sible, and reliable (2). Because access to imaging
toneal deposits (1,3–5). Lymph node metastasis may be limited in developing countries, cervical
is the most common form of extrauterine disease carcinoma continues to be staged at clinical ex-
spread and is the strongest predictor for recur- amination under anesthesia and combined with
rence. Enlarged or abnormal lymph nodes may cystoscopy and sigmoidoscopy. However, the
revised FIGO staging system acknowledges the
benefits of staging on the basis of MR imaging
findings and encourages its use when available.RG • Volume 32 Number 6 Freeman et al 1807
Table 1
MR Imaging Techniques for Staging Cervical Carcinoma
T1-weighted T2-weighted Diffusion-weighted
Weighting Axial Upper Axial Axial
and Plane Axial Abdomen Axial Sagittal Oblique Sagittal Oblique
Pulse sequence SE SE FRFSE FRFSE FRFSE EP EP
Repetition time 700 700 4500 4500 4500 5000 5000
(msec)
Echo time (msec) Min full 14 85 85 85 Minimum Minimum
No. of signals ac- 2 2 4 4 4 6 6
quired
No. of dimensions 2 2 2 2 2 2 2
Section thickness 5 10 5 5 4 4.5 4.5
(mm)
Section gap (mm) 2.5 5 2.5 2.5 1 0 0
Matrix 320 × 256 256 × 192 384 × 256 384 × 256 384 × 256 128 × 128 128 × 128
Field of view (mm) 240 280 240 240 240 240 280
Bandwidth (kHz) 15.63 15.63 41.67 41.67 41.67 ... ...
No. of sections 20 20 20 24 26 21 26
b value (sec/mm2) ... ... ... ... ... 500 800
Acquisition time* 6 min, 10 5 min 4 min, 50 4 min, 50 4 min, 50 2 min, 10 4 min, 10
sec sec sec sec sec sec
Note.—EP = echoplanar, FRFSE = fast recovery fast spin-echo, Min full = minimum full echo train (equates to
about 14–16 msec), SE = spin echo.
*Varies depending on required coverage.
In particular, imaging provides accurate infor- patients must also void their bladder to reduce
mation about important prognostic factors, such movement and ghosting artifacts on T2-weighted
as tumor size, parametrial and pelvic sidewall images (16–18). MR images are acquired with
invasion, and lymphadenopathy (13,14). When patients lying supine and a surface array multi-
possible, MR imaging should be used as an channel coil to optimize image quality and reduce
adjunct to clinical assessment, which currently acquisition time (1,17,19). Endoluminal coils are
remains the reference standard. The role of im- not routinely used because of the reduced field of
aging is to distinguish early stage disease, which view, which limits depiction of extrauterine ex-
is treated with surgery, from early stage bulky tension to adjacent organs.
disease and locally advanced disease, which are
not treated with surgery and require chemora- MR Imaging
diotherapy. In this article, we discuss the added Sequences and Planes
value of MR imaging in staging endometrial and The basic gynecologic pelvic MR imaging
cervical carcinoma and the effect of MR imag- protocol includes acquiring axial, sagittal, and
ing findings on determining prognosis, treat- coronal T2-weighted images. Axial spin-echo
ment strategies, and treatment planning with T1- or T2-weighted images of the abdomen and
respect to the revised FIGO staging system. pelvis are used to depict enlarged lymph nodes,
hydronephrosis, and bone marrow abnormali-
MR Imaging Technique ties (20,21). The protocol is then tailored for
Optimal acquisition of MR images depends either cervical or endometrial cancer staging
on good patient preparation. Motion artifacts (Tables 1, 2). In patients with endometrial can-
caused by bowel peristalsis may be reduced by cer, high-resolution T2-weighted fast spin-echo
instructing patients to fast 4 hours before the ex- images are acquired in the axial oblique plane,
amination and by intravenously administering an
antiperistaltic agent (eg, hyoscine butyl bromide
or glucagon) (15). Immediately before imaging,Table 2
MR Imaging Techniques for Endometrial Carcinoma Staging
1808 October Special Issue 2012
Multiphase Dynamic
T1-weighted T2-weighted Diffusion-weighted Contrast-enhanced
Weighting Axial Upper Axial Axial Axial
and Plane Axial Abdomen Axial Sagittal Oblique Sagittal Oblique Sagittal Oblique
Sequence FSE SE FRFSE FRFSE FRFSE EP EP GRE GRE
Repetition time (msec) 470 700 4500 4500 4500 5000 5000 6.4 6.4
Echo time (msec) Min full 14 85 85 85 Minimum Minimum 2.1 2.1
No. of signals acquired 2 2 3 4 4 6 6 1 1
No. of dimensions 2 2 2 2 2 2 2 3 3
Section thickness (mm) 5 10 5 5 3 4.5 4.5 4 4.2
Section gap (mm) 2.5 5 2.5 2.5 0.5 0 0 ... ...
Matrix 448 × 288 256 × 192 384 × 256 384 × 256 384 × 256 128 × 128 128 × 128 288 × 192 288 × 192
Field of view (mm) 240 280 240 240 220 280 280 240 320
Bandwidth (kHz) 31.25 15.63 31.25 41.67 41.67 ... ... 83.33 83.33
No. of sections 20 20 20 21 26 21 26 32 per slab 24 per slab
b value (sec/mm2) ... ... ... ... ... 500 800 ... ...
Timing* ... ... ... ... ... ... ... Preinjection; Preinjection;
1 and 2 min 3 min after
after injection injection
Acquisition time† 4 min, 50 sec 5 min 3 min, 10 sec 3 min, 58 sec 4 min, 34 sec 2 min, 10 sec 4 min, 10 sec 18 sec 22 sec
Note.—EP = echoplanar, FRFSE = fast recovery fast spin-echo, FSE = fast spin-echo, GRE = gradient-recalled echo, Min full = minimum full echo train (equates to about
14–16 msec), SE = spin echo.
*Relative to administration of contrast medium.
†Varies depending on required coverage.
radiographics.rsna.orgRG • Volume 32 Number 6 Freeman et al 1809
perpendicular to the endometrium, allowing ac- axial oblique planes, perpendicular to the endo-
curate assessment of myometrial invasion (22). metrial cavity or cervical canal in patients with
High-resolution axial oblique T2-weighted fast endometrial and cervical carcinoma, respectively.
spin-echo images are also obtained in patients To distinguish between perfusion and diffusion,
with cervical cancer; however, they are obtained diffusion-weighted images are acquired with a
perpendicular to the cervical canal to accurately low b value (eg, 0 or 50 sec/mm2) followed by a
depict parametrial invasion (23). high b value (eg, 800 or 1000 sec/mm2). Com-
Dynamic multiphase contrast material–en- pared with adjacent tissues, tumor typically dem-
hanced imaging may be used to assess the local onstrates restricted diffusion, which is seen as an
extent of endometrial carcinoma. Before admin- area of high signal intensity on diffusion-weighted
istration of contrast material, T1-weighted gradi- images and an area of hypointensity on apparent
ent-echo MR images are acquired in the axial and diffusion coefficient (ADC) maps. In particular,
sagittal planes. One and 2 minutes after admin- DWI may accurately depict the depth of myome-
istration of contrast material, they are acquired trial invasion in patients with endometrial cancer.
in the sagittal plane, and 3 minutes after contrast It may be of particular use in patients with tumor
material administration, they are acquired in the extension to the cornua, myometrial compression
axial oblique plane. Many studies have reported from a polypoid tumor, poor tumor-to-myome-
the additional benefit of dynamic contrast en- trium contrast, leiomyomas, or adenomyosis,
hancement in evaluating myometrial invasion in as well as when intravenous contrast medium is
patients with endometrial carcinoma (5,24–31). contraindicated (43,44).
However, tumor extension into the cornua and ADC may be calculated with images with
loss of the junctional zone remain confounding different b values, providing a measurement in
factors in assessing the depth of myometrial inva- square millimeters per second. Coregistration of
sion at dynamic contrast-enhanced MR imaging. diffusion-weighted images with corresponding
Use of intravenous contrast medium does not T2-weighted images improves anatomic correla-
improve depiction of disease extent in patients tion. ADC maps should always be reviewed with
with cervical carcinoma because of the variable diffusion-weighted images to avoid pitfalls from
enhancement of cervical tumors; therefore, con- T2 shine-through and water restriction in normal
trast medium is not routinely used in cervical tissues or highly cellular benign tumors (41).
cancer staging protocols. The European Society
of Urogenital Radiology (ESUR) guidelines for Endometrial Carcinoma
staging cervical carcinomas recommend consid- Endometrial carcinoma is the most common gy-
ering the use of intravenous contrast medium necologic malignancy in industrialized nations.
or diffusion-weighted imaging in patients with The mean age at presentation is 63 years, and
small lesions, which are not well depicted on more than 90% of patients are women over the
T2-weighted images, and those who underwent age of 50 years (45). Postmenopausal women
treatment (20). Dynamic multiphase contrast- who present with vaginal bleeding should un-
enhanced T1-weighted gradient-echo imaging dergo transvaginal ultrasonography as the initial
may improve depiction and delineation of small imaging evaluation. If endometrial thickness of
cervical lesions that are 3 mm or larger with more than 4 mm is identified, endometrial biopsy
98% sensitivity, providing important informa- should be performed (46).
tion for surgical planning in patients being Endometrial carcinomas are divided into two
considered for trachelectomy (32,33). It is also histologic subtypes. Endometrioid adenocar-
useful in distinguishing between tumors with a cinoma (type 1), the most common histologic
cervical or endometrial uterine cancer origin in subtype, accounts for almost 90% of cases of
patients with biopsy-proved adenocarcinoma, endometrial cancer, which are further subdivided
especially when both the cervix and lower uter- according to the histologic grade of tumor dif-
ine segment are involved (34). ferentiation, from grade 1 (well differentiated)
Diffusion-weighted imaging (DWI) has an to grade 3 (poorly differentiated). Type 2 endo-
increasingly accepted role in routine cervical metrial carcinomas include serous papillary and
and endometrial carcinoma staging because it clear cell adenocarcinomas. Serous papillary,
increases tumor conspicuity and aids in image clear cell, and grade 3 endometrioid adenocar-
interpretation (35–40). DWI is a physiologic im- cinomas demonstrate more aggressive tumor
aging technique that provides information about biologic characteristics and have a 50% pretest
water mobility, tissue cellularity, and the integrity probability of locally advanced or distant disease
of cellular membranes (39,41,42). Diffusion- at manifestation.
weighted images are acquired in the sagittal and1810 October Special Issue 2012 radiographics.rsna.org
Staging on the basis of the revised FIGO sys- of the small biopsy sample, which often does not
tem for endometrial carcinoma remains surgical represent the whole tumor (4).
because the condition is predominantly treated When the extent of disease at MR imaging is
with surgery. Currently, the National Compre- combined with the histologic subtype and grade
hensive Cancer Network (NCCN) guidelines determined at endometrial biopsy, an accurate
only recommend that chest radiography be assessment of risk stratification and prognosis
performed preoperatively; MR imaging is only may be made. Stage I may be divided into the
recommended when gross cervical invasion is following three risk categories: (a) low risk,
suspected (47). However, the information pro- which includes stage IA, histologic subtype 1
vided by MR imaging has become invaluable in (endometrioid), grades 1 and 2; (b) intermediate
managing endometrial carcinoma. In response to risk, which includes stage IA, histologic subtype
growing evidence, the National Cancer Institute 1, grade 3 and stage IB, histologic subtype 1,
in France incorporated preoperative MR imag- grades 1 and 2; and (c) high risk, which includes
ing into its guidelines for managing endometrial stage IB, histologic subtype 1, grade 3 and all
carcinoma. MR imaging is also recommended stages with histologic subtype 2 (nonendometri-
by the ESUR for staging high-risk endometrial oid) (45).
carcinoma, including all histologic subtype 2 and Patients with a low- or intermediate-risk early
high-grade subtype 1 tumors (21,48). stage tumor have a good prognosis and, thus, may
MR imaging plays an important role in the be treated with simple hysterectomy and bilateral
treatment stratification of patients with endome- salpingo-oopherectomy. In the United Kingdom,
trial carcinoma. Accurate preoperative delinea- these patients may be treated in local centers.
tion of local disease extent and involved lymph Pelvic lymph node dissection may be considered
nodes is essential. When combined with tumor only if suspicious lymph nodes are identified at
histologic findings, this information may be used MR imaging. Furthermore, in patients with low
to guide the surgical approach. or intermediate risk and no myometrial invasion
who are ineligible for surgery, hormonal treat-
Effect of Imaging on Risk Strati- ment or brachytherapy may be considered.
fication and Disease Management In contrast, high-risk patients require hysterec-
The approach to preoperative staging on the ba- tomy; bilateral salpingo-oopherectomy; and para-
sis of MR imaging findings varies among differ- aortic, common iliac, and, possibly, pelvic lymph
ent countries and centers but may become more node dissection. These procedures are performed
established as the use of laparoscopic and robotic in a specialist gynecologic cancer center. There
surgery increases. The information obtained at is no consensus regarding routine systematic
preoperative MR imaging provides crucial infor- lymph node dissection because its clinical benefit
mation regarding local extent and distant spread remains uncertain (7–10). It may be associated
of endometrial tumors before surgery. The depth with substantial morbidity and have little effect
of myometrial and cervical stromal invasion may on the patient’s final outcome if performed rou-
be used as surrogate markers to determine pos- tinely, without preoperative imaging. MR imaging
sible lymphovascular space invasion and the risk enables assessment of the pelvic and paraaortic
for lymph node metastases (28,49). lymph nodes, and if a lymph node is suspicious
The tumor grade and histologic subtype, for tumor involvement, individual treatment deci-
determined on the basis of preoperative hyster- sions may be established regarding the need for
oscopy and biopsy or pipelle sampling findings, lymph node dissection.
are invaluable prognostic indicators. Grade 3 Endometrial carcinoma of stage II or higher,
endometrioid adenocarcinoma and all type 2 with any tumor grade or histologic subtype, ne-
tumors correlate with a poor prognosis because cessitates radical hysterectomy, bilateral salpingo-
more than 50% of patients present with stage IB oophorectomy, and pelvic lymph node dissection.
or higher. However, the histologic subtype and Paraaortic lymphadenectomy may be considered.
grade determined on the basis of biopsy findings In all patients with histologic subtype 2 disease,
often differ from the definitive histologic subtype omentectomy, pelvic and paraaortic lymphad-
and grade determined after hysterectomy, a result enectomy, peritoneal washing, and biopsy are
recommended (48). In addition, in patients with
stage III and IV disease, M fast track R imaging
is able to depict the extent of local tumor inva-
sion and the organs involved, providing a preop-
erative road map regarding resectability and theRG • Volume 32 Number 6 Freeman et al 1811
Table 3 Table 4
Pearls and Pitfalls of MR Imaging of Endome- FIGO Staging of Endometrial Carcinoma
trial Carcinoma
Stage Description
Pearls
Assessment of the depth of myometrial invasion is I Tumor confined to the uterus
optimized by using both the sagittal and oblique IA1812 October Special Issue 2012 radiographics.rsna.org
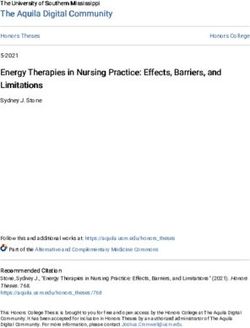
Figure 1. Stage IA endometrial carcinoma
(grade 3 endometrioid adenocarcinoma) in a 51-
year-old woman. (a) Sagittal T2-weighted MR
image shows an intermediate- to high-signal-in-
tensity endometrial tumor (arrows). It is difficult
to distinguish the extent of myometrial invasion
on T2-weighted images alone. (b) Sagittal T1-
weighted MR image obtained after administration
of intravenous gadolinium-based contrast mate-
rial shows the endometrial tumor (arrow), which
demonstrates relatively poor enhancement com-
pared with that of the myometrium, which avidly
enhances. (c) Corresponding diffusion-weighted
MR image shows an area of high signal intensity
within the endometrial tumor (arrow), a finding
indicative of restricted diffusion. The tumor is
seen to invade only the inner myometrium.
revised FIGO stage IA, eliminating the imag- IIIC was subdivided into pelvic and paraaortic
ing limitations of the previous FIGO stages by lymph node involvement, becoming stages IIIC1
no longer requiring radiologists to differentiate and IIIC2, respectively.
between tumors that are confined to the endome-
trium and those that invade the inner one-half of Stage I.—Because the previous stages IA and IB
the myometrium. This change reflects the similar were combined to form stage IA in the revised
prognosis associated with these two clinical sce- FIGO staging system, there is no need to dif-
narios. In the revised FIGO staging system, stage ferentiate between tumors that are confined to
IB now represents invasion of the outer one-half the endometrium and those that invade the in-
of the myometrium. (Before 2009, outer myome- ner myometrium. Stage IA reflects tumors that
trial invasion was classified as stage IC.) Second, involve less than 50% of the myometrial thickness
stage II no longer has subsets A and B. In the (Fig 1). Consequently, in the new FIGO staging
revised FIGO staging system, stage II represents system, stage IB represents tumor invasion into
invasion of the cervical stroma. Involvement of more than 50% of the myometrial thickness (Fig
only the endocervical glands and mucosa, with 2). It is important to distinguish between stages IA
sparing of the cervical stroma (previously IIA dis- and IB because they have different risk stratifica-
ease in the 1988 FIGO staging system), was re- tions when combined with the tumor grade and
classified as stage I. It is important to distinguish histologic subtype. The presence of lymphovas-
cervical stromal invasion because it is associated cular space invasion correlates strongly with the
with a higher risk for lymphovascular space inva-
sion and confers a poorer prognosis. Third, stageRG • Volume 32 Number 6 Freeman et al 1813 Figure 2. Stage IB endometrial carcinoma (grade 3 endometrioid adenocarcinoma) in a 67-year-old woman. (a) Sagittal T2-weighted MR image shows an intermediate- to high-signal-intensity endometrial tumor (arrows). (b) Dynamic contrast-enhanced MR image shows the endometrial tumor (arrowheads), which demonstrates poor enhancement compared with that of the myometrium. (c, d) Corresponding diffusion-weighted image (c) and ADC map (d) show restricted diffusion within the endometrial tumor (arrow), which extends into the outer one-half of the myometrium. The extent of myometrial invasion is clearly delineated on the dynamic contrast-enhanced image, diffusion-weighted image, and ADC map. presence of lymph node metastases and a higher sion vary between 69%–94% and 64%–100%, relapse rate. However, invasion of the lymphovas- respectively (5). The presence of fibroids and cular space may only be identified at pathologic adenomyosis reduce its accuracy, but their ef- analysis of the hysterectomy specimen; it cannot fect may potentially be reduced by performing be identified at preoperative imaging. The extent dynamic multiphase contrast-enhanced imaging of myometrial invasion may be used as a surro- and DWI (43). gate imaging marker for potential lymphovascular Debate remains regarding the value of dy- space invasion and, therefore, the likelihood of namic contrast-enhanced multiphase imaging in nodal metastases (28,49). The incidence of in- evaluating patients with endometrial carcinoma. volved lymph nodes among patients with endome- The presence of tumoral enhancement within trial carcinoma increases from 2.4% in those with the endometrial cavity enables differentiation low risk to 9% in those with intermediate risk and from blood products and debris, which demon- 24% in those with high risk (7,9). strate similar signal intensity on T2-weighted The sensitivity and specificity of MR imag- ing for depicting the depth of myometrial inva-
1814 October Special Issue 2012 radiographics.rsna.org
Figure 3. Stage II endometrial carcinoma (grade 3 endometrioid adenocarcinoma) in a 55-year-old
woman. (a) Sagittal T2-weighted MR image shows an intermediate- to high-signal-intensity endometrial
tumor (arrows) invading the normal, low-signal-intensity cervical stroma. (b) Axial oblique T2-weighted
MR image, obtained perpendicular to the endocervical canal, shows the tumor (arrows) invading
the cervical stroma but not the parametrium. (c, d) Sagittal diffusion-weighted image (c) and ADC
map (d) show restricted diffusion within the endometrial tumor (arrow), with invasion of the cervical
stroma and the outer one-half of the myometrium but not the serosa.
images. Peritumoral inflammation may cause dynamic contrast-enhanced imaging (5,24–31).
overestimation of myometrial invasion, a poten- The use of DWI may also improve accuracy of
tial pitfall. Some studies have reported that the tumor depiction, particularly when intravenous
pretest probability of myometrial invasion and contrast material is contraindicated. Accuracy
overall staging accuracy of T2-weighted imag- of DWI for depicting myometrial invasion is re-
ing increase from 55%–77% to 85%–91% with ported to be 62%–90% (38,52). In addition, the
the use of dynamic contrast-enhanced imaging use of DWI may improve staging accuracy when
(5,25–27,29–31,51). However, other studies tumor delineation is difficult because tumors
reported no additional benefit with the use of appear iso- or hyperintense relative to the myo-
metrium on T2-weighted images or demonstrate
marked peritumoral enhancement after adminis-
tration of contrast material, (43,44).RG • Volume 32 Number 6 Freeman et al 1815
Figure 4. Stage IIIA endometrial carcinoma
(grade 3 endometrioid adenocarcinoma) in
a 60-year-old woman. Sagittal T1-weighted
MR image obtained after intravenous admin-
istration of gadolinium-based contrast mate-
rial shows a bulky endometrial tumor with
relatively low signal intensity distending the
endometrial cavity and extending through the
avidly enhancing myometrium to the serosal
surface (arrow).
Figure 5. Stage IIIA endometrial carcinoma
(mixed high-grade serous papillary and grade
3 endometrioid adenocarcinoma) in a 71-year-
old woman. Coronal T2-weighted MR image
shows an endometrial tumor with intermediate
signal intensity within the endometrial cavity
(white arrow) and enlarged ovaries (black ar-
rows), which demonstrate abnormal heteroge-
neous signal intensity, a finding consistent with
ovarian metastases.
It is important to distinguish between stage I and
stage II disease because of their different progno-
ses. Invasion of the cervical stroma is associated
with a high risk for lymphovascular space inva-
sion, which directly correlates with the risk for
lymph node metastases.
Stage II.—In the revised FIGO staging system,
stage II represents stromal invasion of the cervix, Stage III.—Stage III reflects local or regional
a finding that is best depicted on sagittal and ax- tumor spread: that is, beyond the uterus but not
ial oblique T2-weighted images as an area of low outside the true pelvis. Stage IIIA tumors (those
signal intensity (the cervical stroma) disrupted by that invade the serosa) appear as an area of in-
the intermediate- or high-signal-intensity tumor termediate to high signal intensity that disrupts
(Fig 3). Stage II endometrial tumors must be the contour of the outer myometrium (Fig 4). In
differentiated from stage I tumors, which enter stage IIIA disease, the adnexa is also involved,
the endocervical canal and widen the internal os, particularly in high-grade or type 2 tumors (Fig
with preservation of the normal low-signal-inten- 5). The use of DWI improves depiction of extra-
sity cervical stroma (1). uterine metastatic deposits. In stage IIIB disease,
The use of dynamic imaging after administra- tumor extends into the parametrium, with vagi-
tion of intravenous contrast material helps dis- nal involvement by direct invasion or metastatic
tinguish between stromal invasion and polypoid spread, a finding indicated by segmental loss of
tumor protruding from the endometrial cavity low signal intensity in the vaginal wall on T2-
and into the endocervix (1). On delayed phase weighted images (Fig 6). Stage IIIC disease is
images (obtained 2–3 min after administration of characterized by lymph node involvement, which
contrast material), normal enhancement of the
cervical mucosa excludes stromal invasion (53).1816 October Special Issue 2012 radiographics.rsna.org
Figure 6. Stage IIIB endometrial carcinoma (high-grade serous papillary adenocarcinoma) in a 67-year-
old woman. (a) Axial T2-weighted MR image shows a tumor (*) with intermediate signal intensity in-
vading the cervical stroma and extending into the right parametrium (arrow). (b) Corresponding axial
diffusion-weighted image shows an area of restricted diffusion within the tumor extending into the right
parametrium (arrow).
Figures 7, 8. (7) Stage IIIC1 endometrial carcinoma (high-grade serous carcinoma) in a 75-year-old
woman. Axial T1-weighted fat-saturated MR image obtained after administration of intravenous gadolinium-
based contrast material shows the tumor (*), which demonstrates relatively poor enhancement compared
with the avidly enhancing myometrium. Bilateral enlarged external iliac lymph nodes (arrows) are also
seen. (8) Stage IIIC2 endometrial carcinoma (grade 3 endometrioid adenocarcinoma) in a 59-year-old
woman. Axial T2-weighted MR image shows an enlarged left paraaortic lymph node (arrow) and an en-
dometrial tumor that has spread to the right ovary (arrowheads), which is grossly enlarged and hetero-
geneous, a finding consistent with ovarian metastasis.
is further subdivided into pelvic (stage IIIC1) the revised FIGO staging system (Figs 7, 8). MR
and paraaortic (stage IIIC2) node involvement in imaging features that are considered suspicious
for lymph node involvement include a size larger
than 1 cm, multiplicity, an irregular contour,
necrosis, and abnormal signal intensity similar
to that of the primary tumor. The revised FIGO
staging system reflects the different prognoses as-
sociated with lymph node metastases in the pelvic
and paraaortic regions (3).RG • Volume 32 Number 6 Freeman et al 1817
Figure 9. Stage IVB endometrial carcinoma
(high-grade serous papillary adenocarcinoma)
in a 61-year-old woman. (a, b) Axial T2-weighted
(a) and diffusion-weighted (b) MR images show
peritoneal deposits (arrow), a finding typical for
serous papillary endometrial carcinoma. (c) Ax-
ial T2-weighted MR image shows omental cake
(arrowheads), a pattern of metastatic spread
similar to that of ovarian carcinoma.
metastatic spread similar to that of ovarian carci-
noma, with omental cake and serosal deposits (Fig
9). Liver, lung, and bone metastases are rare at the
time of manifestation.
Cervical Carcinoma
Although cervical carcinoma is the third most
common gynecologic malignancy in the United
States, it remains the most common gynecologic
Stage IV.—Stage IV disease represents direct inva- malignancy worldwide; an estimated 540,000
sion of the bladder or rectal mucosa (stage IVA) or women were diagnosed with cervical carcinoma
the presence of distant metastases (stage IVB). On in 2010 (11). The highest prevalence of cervi-
T2-weighted images, extension of tumor directly cal carcinoma is in Central and South America,
into the normally hyperintense vesical or rectal South Central Asia, and parts of Africa, with Asia
mucosa is indicative of endometrial tumor inva- accounting for approximately 80% of cervical
sion into the bladder or rectum. Bullous edema, carcinoma diagnoses (12). Whereas the intro-
which appears as thickening of the high-signal-in- duction of cervical cancer screening programs
tensity mucosal layer, is not indicative of mucosal and improved treatment strategies have caused a
invasion. Disruption of the hypointense muscularis reduction in mortality rates in industrialized na-
layer does not indicate stage IV disease because tions, there has been little change in developing
it cannot be visualized at subsequent cystoscopy countries, where tumors are usually detected at
or sigmoidoscopy. In stage IVB disease, distant an advanced stage. Because of its epidemiologic
metastases, including paraaortic lymphadenopa- characteristics, cervical carcinoma continues to
thy, occur above the renal vessels, and inguinal be staged at clinical examination, with anesthesia
lymph node metastases are seen (54). Malignant and often with cystoscopy and sigmoidoscopy,
ascites and peritoneal deposits are more common according to the FIGO classification system (55).
in type 2 endometrial tumors and high-grade type However, there are discrepancies between tumors
1 tumors. Type 2 (serous papillary and clear cell
adenocarcinoma) tumors demonstrate a pattern of1818 October Special Issue 2012 radiographics.rsna.org
that are staged at clinical examination according ing is optional in patients with tumors that are
to the FIGO staging system and those that are stage IB1 or lower. Chest radiography, CT, or
staged at surgery, with an error rate as high as positron emission tomography (PET)/CT may
32% in patients with stage IB disease and 65% in be considered in patients with distant disease
patients with stage III disease (13). In addition, spread. The NCCN guidelines also state that MR
clinical staging has been shown to be limited in imaging be used to exclude disease high in the
evaluating important prognostic factors such as endocervix (61). However, treatment of patients
parametrial and pelvic sidewall invasion, tumor with early stage disease (stages IIA1 and IB1)
size, and lymph node metastases (54,56). Stud- comprises surgery, including trachelectomy and
ies have reported discordance between findings radical hysterectomy. Therefore, it is crucial that
seen at clinical evaluation and MR imaging. In tumor extension beyond the cervix be identified
particular, endocervical lesions are often discrep- preoperatively. If parametrial invasion or lymph
ant, with underestimation of tumor size at clinical node metastases are detected at surgery, adjuvant
examination compared with that at MR imaging. chemoradiotherapy is necessary. In this context,
Overall, the accuracy of MR imaging for depict- patients will have undergone unnecessary surgery
ing tumor size is 93%, whereas that of clinical and have higher postoperative morbidity associ-
staging is less than 60% (57). Tumor size is clini- ated with chemoradiotherapy. Evaluation of para-
cally important for risk stratification because of metrial invasion is difficult at clinical examina-
its direct correlation with lymph node involve- tion, depending on the extent of tumor invasion,
ment, prognosis, and patient outcome (58,59). with studies reporting variable accuracy of 29%–
This relationship is reflected in the FIGO classi- 53% (62). In comparison, MR imaging is able to
fication system, in which tumor stages IB and IIA depict parametrial invasion with 88%–97% accu-
are subdivided according to size (smaller or larger racy and 93% specificity (1,63). Most important,
than 4 cm in the maximal dimension). MR imaging helps exclude parametrial invasion
with a negative predictive value of 94%–100%,
Effect of Imaging on Risk Strati- enabling identification of patients who are suit-
fication and Disease Management able for radical surgery, which is contraindicated
The revised FIGO staging system now recom- in patients with parametrial invasion (57,64,65).
mends performing computed tomography (CT) In addition, MR imaging assessment of patients’
or MR imaging when available. CT is of limited suitability to undergo trachelectomy is essential;
use in local staging, but it is able to depict ex- ideally, trachelectomy requires that tumors be
trauterine spread of disease, including enlarged smaller than 2 cm, the cervix be longer than 2
lymph nodes, fistulation into the bladder or cm, and the distance from the internal cervical os
rectum, and distant metastases. In contrast, MR be more than 1 cm (64,66).
imaging has exquisite soft-tissue contrast resolu- Bulky early stage disease includes stages IB2
tion and is able to clearly define the local extent and IIA2, with tumors measuring more than 4
of primary tumor and depict metastatic spread cm. The size of the primary tumor may be pre-
(59,60). It accurately depicts findings that are cisely determined at MR imaging with an accu-
important for prognosis, including tumor size, racy of 93%, stratifying patients into an appropri-
parametrial and pelvic sidewall invasion, bladder ate prognostic group and treatment regimen (57).
or rectal invasion, and lymph node metastases. Given the poorer prognosis of bulky tumors,
Accurate risk stratification of patients with cervi- patients undergo the same treatment pathway
cal carcinoma is used to determine the most ap- as those with locally advanced tumors (stage
propriate management pathway, which ensures IIB and above), including chemo- and radiation
the best clinical outcome. therapy. MR imaging also provides information
There is no role for MR imaging in patients for brachytherapy planning.
with stage IA disease because it is, by defini- MR imaging may exclude local invasion into
tion, microscopic and, therefore, not visible at the bladder and rectum with a negative predic-
MR imaging. NCCN guidelines state that imag- tive value of 100% (65–69). In comparison,
when FIGO staging is performed on the basis of
cystoscopy or sigmoidoscopy findings, bladderRG • Volume 32 Number 6 Freeman et al 1819
Therefore, lymph nodes that are enlarged or
Table 5
Pearls and Pitfalls of MR Imaging of Cervical
have other suspicious features at preoperative
Carcinoma MR imaging indicate the need for a two-stage
surgical procedure. Initially, laparoscopic lymph
Pearls
node sampling is performed before definitive
Preservation of an intact low-signal-intensity cervi-
surgery. If laparoscopy findings are negative for
cal stromal ring excludes parametrial invasion.
Multiphase contrast-enhanced imaging or DWI may tumor involvement, hysterectomy or trachelec-
improve delineation of small tumors (important tomy may be performed. Surgical lymph node
in patients being considered for trachelectomy). assessment remains the reference standard for
Use of dynamic intravenous contrast medium may detecting lymph node metastases, although it is
help distinguish between cervical and endo- associated with complications (73,74).
metrial tumors in patients with biopsy-proved
adenocarcinoma, especially when both the cervix Appearances at MR Imaging
and lower uterine segment are involved. The normal cervix demonstrates a trilaminar pat-
Pitfalls tern of signal intensity, with high-signal-intensity
Cervical stroma can be indistinct due to the pres- endocervical mucosal glands surrounded by low-
ence of stromal edema in patients with large signal-intensity stroma and a rim of intermediate-
tumors.
signal-intensity smooth muscle. On T2-weighted
High-signal-intensity thickening of the bladder
mucosa on T2-weighted images indicates bullous
images, cervical carcinoma appears as an inter-
edema and is not a sign of direct invasion.* mediate- to high-signal-intensity mass that re-
After hysterectomy, nodularity or fullness at the places the low-signal-intensity cervical stroma.
vaginal vault may be seen on T1-weighted images Enhancement of cervical cancer varies on
and should not be mistaken for a lesion. dynamic multiphase contrast-enhanced T1-
*One study has shown that the addition of dy-
weighted images, with small tumors enhancing
namic contrast-enhanced T1-weighted images may earlier than adjacent cervical stroma and larger
improve the accuracy of distinguishing edema from tumors demonstrating a variable degree of en-
bladder and rectal invasion (70). hancement. Depiction of poorly circumscribed
lesions may be aided by the use of DWI and
ADC mapping; tumors demonstrate high signal
intensity on diffusion-weighted images and low
or rectal invasion is identified in less than 5% of signal intensity on corresponding ADC maps,
patients. In view of this, the revised FIGO staging and the ADC value of cervical cancer is signifi-
system states that cystoscopy and sigmoidoscopy cantly lower than that of normal cervical tissue
are no longer mandatory. However, when MR (Table 5) (37,75,76).
imaging findings are equivocal or assessment is
difficult due to the presence of bullous edema, Revised FIGO Staging
endoscopy may be used to depict or exclude mu- The revised FIGO staging system for cervical car-
cosal invasion. Furthermore, distant metastases, cinoma was implemented on June 1, 2009 (Table
including liver and bone metastases, which are 6). In the new FIGO staging system, the following
not apparent at clinical assessment, may be de- three changes, which affect imaging and inter-
picted at MR imaging. pretation, were made: First, the use of diagnostic
The presence of involved pelvic lymph nodes imaging, including CT and MR imaging, to stage
does not alter the FIGO stage, but it is associ- cervical tumors is recommended but remains
ated with a poorer prognosis and alters the nonmandatory (55). CT is able to depict lymph
treatment in patients with cervical carcinoma. nodes, hydronephrosis, and distant metastases.
MR imaging is sensitive and specific for de- MR imaging has superb soft-tissue resolution and
picting lymph node metastases (see section on is able to delineate both the local extent of tumor
“Lymph Node Evaluation”) (71,72). In early and distant tumor spread.
stage disease, the presence of pelvic lymph node
metastases significantly causes survival rates to
decrease, from 85%–90% to 50%–55% (58).1820 October Special Issue 2012 radiographics.rsna.org
Table 6
FIGO Staging of Cervical Carcinoma
Stage Description
0 Tumor confined to the surface layer (the cell lining) of the cervix;
also called carcinoma in situ
I Extension deeper into the cervix with no spread beyond (extension
to the corpus is disregarded)
IA Invasive carcinoma; may only be diagnosed at microscopy
IA1 Stromal invasion £3.0 mm deep and extension £7.0 mm
IA2 Stromal invasion >3.0 mm and £5.0 mm with extension ≤7.0 mm
IB Clinically visible lesions limited to the cervix uteri or preclinical
cancers higher than stage IA
IB1 Clinically visible lesion £4.0 cm in greatest dimension
IB2 Clinically visible lesion >4.0 cm in greatest dimension
II Cervical carcinoma extends beyond the uterus but not to the pelvic
wall or the lower one-third of the vagina
IIA No parametrial invasion
IIA1 Clinically visible lesion £4.0 cm in greatest dimension
IIA2 Clinically visible lesion >4.0 cm in greatest dimension
IIB With obvious parametrial invasion
III Extension to the pelvic wall, involvement of lower one-third of the
vagina, or hydronephrosis or nonfunctioning kidney
IIIA Involvement of lower one-third of the vagina with no extension to
the pelvic wall
IIIB Extension to the pelvic wall, hydronephrosis, or nonfunctioning
kidney
IV Extension beyond the true pelvis or involvement of the bladder or
rectal mucosa (biopsy proved); bullous edema does not convey
stage IV disease
IVA Spread to adjacent organs
IVB Spread to distant organs
Second, stage II tumors extend beyond the optional and no longer mandatory, a change from
uterus but not to the pelvic sidewall or the lower the 1988 FIGO staging system (78). Before 2009,
one-third of the vagina. Stage IIA tumors involve such examinations were the primary method for
the upper two-thirds of the vagina, and stage IIB staging cervical cancer by assessing the fixation of
tumors demonstrate parametrial invasion. In the the tumor to the parametrium and pelvic sidewall.
revised FIGO staging system, stage IIA was also Proctoscopy and cystoscopy are still used to depict
subdivided according to size into stages IIA1 (tu- stage IVA disease, in which tumor invades rectal
mors 4 cm or smaller) and IIA2 (tumors larger and bladder mucosa. However, T2-weighted MR
than 4 cm), a reflection of recent prognostic data imaging accurately depicts bladder (sensitivity,
regarding the size of IIA tumors and patient out- 75%) and rectal (sensitivity, 71%) involvement
comes. In contrast, no such data support a subdi- (79). Moreover, T2-weighted MR imaging find-
vision of stage IIB (77). The presence of parame- ings may be used to confidently exclude bladder
trial invasion alone is a poor prognostic indicator, or rectal involvement with a negative predictive
with a high risk for recurrence. value of 100%, obviating the need for invasive pro-
Third, examinations performed with anesthe- cedures (67). It should be noted that T2-weighted
sia, including cystoscopy and proctoscopy, are imaging also has a high false-positive rate due to
the presence of bullous edema, which appears as
thickened, high-signal-intensity mucosa.RG • Volume 32 Number 6 Freeman et al 1821
Figure 10. Stage IB1 cervical carcinoma (squa-
mous cell carcinoma) in a 36-year-old woman.
(a, b) Sagittal (a) and axial oblique (b) T2-
weighted MR images show a mass (arrow in a)
with intermediate signal intensity within the endo-
cervical canal. The surrounding low-signal-in-
tensity cervical stroma is intact (arrowheads in b),
excluding parametrial invasion. It is difficult to de-
termine the exact size of the tumor on T2-weighted
images. (c) Sagittal diffusion-weighted MR image
shows an area of high signal intensity within the
small endocervical tumor (arrow), a finding indica-
tive of restricted diffusion. Tumors that arise en-
tirely within the endocervical canal are difficult
to accurately stage at clinical examination.
Stage I.—In stage I, tumors are confined to the tastases (63). Identification of these prognostic
cervix. Stage IA is defined as a microinvasive factors is crucial because their presence pre-
tumor that cannot be reliably depicted on T2- cludes surgery (72,80).
weighted images; thus, there is no established role
for MR imaging in evaluating patients with a stage Stage II.—In stage II, tumors extend beyond the
IA tumor. Stage IB tumors are further subdivided uterus and involve the upper two-thirds of the
by size: Stage IB1 tumors are smaller than 4 cm, vagina but do not extend to the pelvic sidewall
and stage IB2 tumors are 4 cm or larger (Fig 10). or the lower one-third of the vagina. Stage II
On T2-weighted images, stage IB tumors typically is further subdivided according to the absence
demonstrate intermediate to high signal intensity (stage IIA) or presence (stage IIB) of parametrial
compared with the cervical stroma, which demon- invasion. Involvement of the upper two-thirds of
strates low signal intensity. the vagina is seen on T2-weighted images as a
MR imaging is recommended in patients with high-signal-intensity lesion disrupting the low-
clinical stage IB disease or higher because of the signal-intensity vaginal wall. A large exophytic
importance of accurate measurement of tumor polypoid cervical tumor may widen the vaginal
size and identification of parametrial invasion,
lower vaginal involvement, and lymph node me-1822 October Special Issue 2012 radiographics.rsna.org
Figure 11. Stage IIB cervical carcinoma (adenocarcinoma) in a 48-year-old woman. (a) Sagittal T2-
weighted MR image shows a tumor (arrows) with intermediate signal intensity replacing the normal
low-signal-intensity cervical stroma. (b) Axial oblique T2-weighted MR image obtained perpendicular
to the endocervical canal shows interruption of the low-signal-intensity cervical stromal ring. Nodular
soft tissue extends bilaterally into the parametrium (arrows), a finding indicative of parametrial inva-
sion. Right hydrosalpinx (*) is also incidentally noted.
fornix, mimicking vaginal infiltration; however, in stromal rim is thicker than 3 mm, a finding known
these cases, the low-signal-intensity vaginal wall as the “hypointense rim” sign (62). MR imaging
remains intact. According to the FIGO annual has 97% specificity and 100% negative predictive
report database, the maximum tumor diameter value for depicting parametrial invasion (67).
affects the prognosis of patients with a stage IIA In large tumors, parametrial invasion may be
tumor. Hence, stage IIA is subdivided into stages overestimated on T2-weighted images due to the
IIA1 (those that are 4 cm or smaller) and IIA2 presence of stromal edema, which is caused by
(those that are larger than 4 cm) (77). compression of the tumor or inflammation (58).
In stage IIB, parametrial invasion is present but Studies have reported that MR imaging has 69%
does not extend to the pelvic sidewall (Fig 11). sensitivity and 93% specificity for depicting para-
Stage IIB is not subdivided by size because the metrial invasion (57,65). Its accuracy varies ac-
presence of parametrial invasion alone indicates cording to the size of the tumor, with 96% accu-
a poor prognosis, which is reflected in the FIGO racy in small tumors and 70% accuracy in large
staging system. Parametrial invasion is indicated tumors (71). Postbiopsy hemorrhage may cause
by disruption of the low-signal-intensity cervi- peristromal stranding, another pitfall of assessing
cal stromal ring, with nodular or irregular tumor parametrial invasion (58,62). In these cases, DWI
extending into the parametrium (59). Segmental and ADC mapping may help determine the true
disruption of the cervical stroma is highly indica- extent of tumor (43).
tive of parametrial invasion; however, additional
features, such as a spiculated tumor-parametrium Stage III.—In stage IIIA, tumors extend to the
interface, soft-tissue extension into the parame- lower one-third of the vagina but not the pelvic
trium, and encasement of the periuterine vessels, sidewall (Fig 12). Extension to the pelvic sidewall
improve confidence in diagnosing parametrial or involvement of the ureters, which causes hy-
invasion (58). Conversely, parametrial invasion dronephrosis, is classified as stage IIIB. Visualiza-
may be confidently excluded, with specificity as tion of tumor within 3 mm of the obturator inter-
high as 99%, if the low-signal-intensity cervical nus, levator ani, and piriform muscles or the iliac
vessels is considered highly suggestive of stage
IIIB disease (62).RG • Volume 32 Number 6 Freeman et al 1823 Figure 12. Stage IIIA cervical carcinoma (squamous cell carcinoma) in a 61-year-old woman. Sagittal (a) and axial (b) T2-weighted MR images show a bulky cervical tumor (* in a) with intermediate signal intensity extending into the lower one-third of the vagina (arrow). Figure 13. Stage IVA cervical carcinoma (adenocarcinoma) in a 76-year-old woman. Sagittal (a) and axial (b) T2-weighted MR images show a cervical tumor (* in a) with intermediate signal intensity and nodular local invasion into the bladder (arrow). Stage IV.—Stage IVA reflects local pelvic organ by the hyperintense tumor. The reported sensitiv- invasion, which is characterized by infiltration of ity and specificity of MR imaging for depicting the rectal mucosa or urinary bladder (Fig 13). bladder or rectal invasion are 71%–100% and Rectal invasion usually follows the path of the 88%–91%, respectively (67,68). Bullous edema uterosacral ligaments because the peritoneal re- within the bladder causes high-signal-intensity flection of the pouch of Douglas acts as a barrier thickening along the superficial internal surface for direct invasion from the posterior fornix and of the bladder, a finding that may mimic tumor into the rectum (62). On T2-weighted images, involvement (63). Conversely, bladder or rectal rectal invasion is indicated by segmental disrup- tion of the low-signal-intensity muscularis layer
1824 October Special Issue 2012 radiographics.rsna.org
involvement may be confidently excluded at MR and understanding of tumor biology improve,
imaging with a negative predictive value of 100%, staging systems must also improve in order to
making cystoscopy and sigmoidoscopy redun- identify significant prognostic factors, which will
dant (67). In stage IVB, tumors spread beyond inform treatment decisions. The FIGO staging
the pelvis, including the paraaortic and inguinal system provides a robust, uniform method of
lymph nodes, lung, liver, and bone. Although the describing tumor extent, enabling accurate ex-
presence of pelvic lymph node metastases does change of information between clinical centers
not change the FIGO stage, it guides the surgical and consistent treatment strategies. Ultimately, it
approach in patients with early stage tumors. provides high-quality data, including response to
treatment, survival, and mortality.
Lymph Node Evaluation In the revised FIGO staging system, endome-
In patients with endometrial and cervical cancer, trial carcinoma continues to be surgically staged.
the presence of lymph node metastases confers However, studies have shown that MR imaging is
a poor prognosis and adversely affects survival accurate in delineating local disease extent, and
(80,81). Therefore, identification of involved pelvic MR imaging findings in conjunction with tumor
and paraaortic lymph nodes alters the therapeu- grade and histologic subtype enable preopera-
tic approach. With accuracies of 83%–90% and tive risk stratification, which guides surgery and
86%–90%, respectively, MR imaging and CT have chemoradiotherapy. Studies have also shown that
comparable accuracies for depicting nodal involve- MR imaging has higher accuracy than clinical
ment (82–85). Both modalities rely on size criteria, examination and surgical staging in delineating
such as a short-axis diameter of up to 10 mm in local extent of cervical carcinoma. Consequently,
normal nodes, a characteristic that inevitably leads the revised FIGO staging system recommends
to low sensitivity due to the inability of CT and that, when available, imaging be used as an ad-
MR imaging to depict metastases in normal-sized junct to clinical assessment in staging cervical
lymph nodes (26,83,86,87). carcinoma. Thus, it is important that radiologists
Detection of lymph nodes increases with the familiarize themselves with the revised staging
use of DWI because of the conspicuous high signal classification of endometrial and cervical carci-
intensity of nodes, although correlation with T2- noma and understand their relevance to disease
weighted imaging is advised. However, differenti- management.
ating an involved lymph node from a benign one is
difficult because both may demonstrate high signal References
intensity at DWI (88). Lin et al (89) reported that 1. Sala E, Wakely S, Senior E, Lomas D. MRI of ma-
with MR images obtained at 3 T, it was possible to lignant neoplasms of the uterine corpus and cervix.
successfully differentiate between metastatic and AJR Am J Roentgenol 2007;188(6):1577–1587.
2. Odicino F, Pecorelli S, Zigliani L, Creasman WT.
benign lymph nodes by combining ADC, relative History of the FIGO cancer staging system. Int J
ADC, and size criteria. Further studies of 1.5-T Gynaecol Obstet 2008;101(2):205–210.
MR images reported conflicting results (90,91). 3. Creasman W. Revised FIGO staging for carcinoma
Other promising studies have shown that combin- of the endometrium. Int J Gynaecol Obstet 2009;
ing DWI with ultrasmall super paramagnetic iron 105(2):109.
4. Frei KA, Kinkel K. Staging endometrial cancer: role
oxide (USPIO)-enhanced MR imaging has a role of magnetic resonance imaging. J Magn Reson Im-
in preoperative planning (92). It has been demon- aging 2001;13(6):850–855.
strated that the use of lymph node–specific MR 5. Sironi S, Colombo E, Villa G, et al. Myometrial in-
imaging contrast agents, such as USPIO, improves vasion by endometrial carcinoma: assessment with
sensitivity for depicting lymph node metastases, plain and gadolinium-enhanced MR imaging. Radi-
ology 1992;185(1):207–212.
with sensitivity of 93% with the use of USPIO 6. Cohen P, Tan AL, Penman A. The multidisciplinary
criteria compared with 29% with the standard size tumor conference in gynecologic oncology: does it
criterion (>1 cm) (86). alter management? Int J Gynecol Cancer 2009;19
(9):1470–1472.
Conclusions 7. Benedetti Panici P, Basile S, Maneschi F, et al. Sys-
tematic pelvic lymphadenectomy vs. no lymphad-
The revised FIGO staging system has served to enectomy in early-stage endometrial carcinoma: ran-
improve risk stratification in patients with endo- domized clinical trial. J Natl Cancer Inst 2008;100
metrial or cervical carcinoma. As our knowledge (23):1707–1716.
8. Dowdy SC, Mariani A. Lymphadenectomy in en-
dometrial cancer: when, not if. Lancet 2010;375
(9721):1138–1140.You can also read