RMUS 2021 Abstract Submission Summary
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
RMUS 2021 Abstract Submission Summary Friday, Poster Session 1 Saturday: Poster Session 2 Moderators: Granville Lloyd, MD University of Colorado and Moderators: Frances Alba, MD, University of New Mexico and Julie Riley, MD, University of New Mexico Paul Maroni, MD, University of Colorado Alan Quach, University of Colorado Kseniya Anishchenko, University of Colorado VIDEO DEMONSTRATION OF 16 CM BUCCAL GRAFT HARVEST DIAGNOSTIC UTILITY OF RENAL MASS BIOPSY IN A VA COHORT Jordan Foreman, MD, University of New Mexico MAXIMIZING BUCCAL GRAFT HARVEST LENGTH Miguel Rodriguez-Homs, MD, University of Colorado USING THE V-MAXX TECHNIQUE INTENSITY OF CARE AND COSTS FOR NEOADJUVANT CHEMOTHERAPY IN BLADDER CANCER: RESULTS FROM Kirk Redger, MD, University of Colorado A LARGE PRIVATELY INSURED COHORT IN THE UNITED ROBOTIC BUCCAL MUCOSA GRAFT URETEROPLASTY FOR STATES BENIGN +URETERAL STRICTURE DISEASE: IS OMENTAL FLAP INTERPOSITION ALWAYS NECESSARY Anessa Sax-Bolder, University of Colorado ASSOCIATION OF HOSPITALAND PATIENT CHARACTERISTICS Bryn Launer, University of Colorado WITH SURGERY AND CHEMOTHfERAPY FOR UPPER TRACT LONG-TERM FOLLOW UP OF ILEAL URETERAL REPLACEMENT UROTHELIAL CARCINOMA FOR COMPLEX URETERAL STRICTURES: STINGLE INSTITUTION STUDY Miguel Rodriguez-Homs, MD, University of Colorado HEALTH CARE COSTS AND HOSPITAL READMISSIONS Alan Quach, University of Colorado FOR RADICAL CYSTECTOMY FOR BLADDER CANCER BY CREATION OF CONTINENT URINARY CHANNEL USING THE SURGICAL APPROACH AND DIVERSION SPIRAL MONTI TECHNIQUE Anessa Sax-Bolder, University of Colorado Anessa Sax-Bolder, University of Colorado NEUROFIBROMATOSIS 1 CAN HAVE PLEXIFORM SPINA BIFIDA ONLINE EDUCATION SERIES FOR NEUROFIBROMAS WITH DIFFUSE GANGLIONEUROMATOSIS TRANSITIONAL PATIENTS IN THE ERA OF COVID-19 INFILTRATING THE URINARY BLADDER CAUSING URINARY TRACT SYMPTOMS Gary Shahinyan, BA, University of Colorado MARKET TRENDS IN REGENERATIVE THERAPIES FOR Brett Wiesen, Children’s Hospital of Colorado ERECTILE DYSFUNCTION ACROSS MAJOR METROPOLITAN DOUBLE-BLIND PLACEBO-CONTROLLED RANDOMIZED CITIES CONTROLLED TRIAL OF NSAID PRIOR TO URETERAL STENT REMOVAL IN A PEDIATRIC POPULATION Alan Makedon, University of Colorado ICG ANGIOGRAPHY IN ROBOTIC MICROSURGICAL SPERMATIC Anessa Sax-Bolder, University of Colorado CORD DENERVATION (VIDEO) MULTIDISCIPLINARY SURGICAL MANAGEMENT OF PUBIC OSTEOMYELITIS Alan Makedon, University of Colorado IDENTIFICATION OF GENES ASSOCIATED WITH THE RISK OF Anessa Sax-Bolder, University of Colorado REQUIRING BPH SURGERY CONCORDANCE OF PRE- AND INTRA-OPERATIVE BIOPSY IN PUBIC OSTEOMYELITIS Kirk Redger, MD, University of Colorado ROBOTIC REPAIR OF ABDOMINAL WALL MESH BLADDER EROSION
Video Demonstration of 16 cm Buccal Graft Harvest Alan Quach, MS; Kirk D. Redger, MD; Brian J. Flynn, MD University of Colorado SOM, Division of Urology 12631 E 17th Ave, C-319 Denver, CO 80045 United States Title: Video Demonstration of 16 cm Buccal Graft Harvest Category: Reconstructive urology Abstract: Introduction and Objective: The buccal mucosa graft harvest was first described by Graham Humby in 1941 for urethroplasty. Our objective is to demonstrate our technique on harvesting a large buccal graft. Methods: This video will show how we obtain exposure of the harvest site, hydrodissect and defat the graft, and manage the harvest site. Results: The harvest sites were packed and did not require closure or cautery. The two separate patients demonstrated in the video had no complications post-operatively. Conclusions: The buccal graft’s versatility, overall high success rate, reliability and ability to be harvested by a single surgeon lends itself to widespread increase in adoption for surgical reconstruction, especially in our practice. Funding: none Video: https://drive.google.com/file/d/1t2yXzaYtUrxl3QghbOT3DSQk-bwcUH8P/view?usp=sharing 2 Back to Summary Page
Maximizing Buccal Graft Harvest Length Using the V-Maxx Technique Jordan Foreman MD, and Maxx Gallegos MD University of New Mexico Division of Urology Objectives: A hurdle encountered during urethral reconstruction of long length strictures is the amount of substitution graft needed. Often buccal mucosa, lingual, and/or contralateral buccal mucosal are used. The objective of this study is to describe a novel technique to harvest buccal mucosal graft currently used at our institution for long length urethral strictures. Methods: A retrospective review was performed looking at patients undergoing buccal substitution urethroplasty for long length urethral strictures using the V-Maxx technique for buccal harvest. The stretched length harvest was measured and comparable to the length of graft needed for urethroplasty. Results: A retrospective review was performed identifying 10 patients who the V-Maxx technique was used. The pre- incision stretched graft length using a classical linear harvest, the pre-incision stretched V-Maxx length, and the post harvest V-Maxx graft length were all measured. On average, patients had 30% longer pre incision stretched grafts able to be harvested with the V-Maxx technique. The average post harvest V-Maxx graft length was 10cm long. All graft harvest sites were able to be closed. Conclusions: This study describes a novel technique to harvest buccal mucosal graft allowing for use of a single side buccal graft for strictures up to 12cm in length. With this technique morbidity can be decreased with only a single site of harvest. Future studies will include patient/clinical outcomes after urethroplasty with V-Maxx buccal harvest. Financial Disclosure: None Back to Summary Page 3
Robotic buccal mucosa graft ureteroplasty for benign ureteral stricture disease: Is omental flap interposition always necessary Humberto Villarreal, MD1; David Koslov, MD1; Paul Maroni, MD1; Ty Higuchi, MD1; Alan Quach, BS1; Kirk D. Redger, MD1; Brian J. Flynn, MD1 University of Colorado SOM, Division of Urology 12631 E 17th Ave, C-319 Denver, CO 80045 United States Title: Robotic buccal mucosa graft ureteroplasty for benign ureteral stricture disease: Is omental flap interposition always necessary Category: Reconstructive urology Abstract: Introduction: Robotic buccal mucosal graft ureteroplasty was initially described in 2015 with increasing utilization over the past 4 years. In the literature, an omental flap is commonly used to secure the anastomosis and provide vascularity. Our institution has utilized buccal mucosa for the reconstruction of benign ureteral stricture disease since 2017. In this study, we review this experience and report on outcomes. Methods: A retrospective analysis was performed in patients undergoing robotic buccal mucosal graft ureteral reconstruction since 2017 at a single institution by two surgeons. Data including stricture etiology, location of injury, length of stricture, surgical management, length of follow-up, success rate, complications, and the need for secondary procedures was obtained. Results: Twelve patients underwent robotic buccal mucosal graft augmented ureteral reconstruction based on attending preference and stricture complexity, excluding patients with primary repair for UPJ obstruction or external traumatic injury. 10 patients (83%) were managed preoperatively with a stent or nephrostomy tube. 10 patients (83%) had undergone prior endoscopic intervention. Mean number of prior endoscopic treatments for ureteral stricture was 3 (range 0-6). Mechanism of injury included recurrent stricture after prior reconstruction (50%), stone disease (33%), and iatrogenic injury during pelvic surgery (17%). Location of injury was proximal (83%) and distal (17%). Average stricture length was 4 cm. The type of repair included ureteral reimplant with buccal mucosa augmentation (n=1), pyeloplasty with BMG augmentation (n=3), and BMG ureteroplasty (n=8). Mean operative time was 366 minutes. Mean length of stay was 4 days. At the time of this study, 9 patients had completed follow-up and their outcomes are as follows. At a mean follow-up of 5 months, primary success rate was 89%, with the one failure planning to undergo nephrectomy instead of additional reconstructive surgery. Time to failure was 120 days. There was one major complication (defined as a Clavien-Dindo grade 3 or higher) in a patient that suffered a post-op cryptogenic ischemic stroke. Conclusion: Robotic buccal mucosa graft ureteral reconstruction has been an important addition to our reconstructive treatment algorithm for benign ureteral strictures. Utilization of this minimally-invasive technique has decreased the need for ureteral reconstruction using bladder or omental flap-based repairs or ileal interposition. Funding: none Video: n/a 4 Back to Summary Page
Title: LONG-TERM FOLLOW UP OF ILEAL URETERAL REPLACEMENT FOR COMPLEX URETERAL STRICTURES: STINGLE INSTITUTION STUDY Bryn M. Launer* BA1, Kirk D. Redger MD2, David S. Koslov MD2, Anessa Sax-Bolder BA1, Ty T. Higuchi MD PhD2, Andrew P. Windsperger MD2, Brian J. Flynn MD2 1, University of Colorado School of Medicine, Aurora, CO. 2, Division of Urology, University of Colorado, Aurora, CO. Title: LONG-TERM FOLLOW UP OF ILEAL URETERAL REPLACEMENT FOR COMPLEX URETERAL STRICTURES: STINGLE INSTITUTION STUDY Category: Reconstructive Urology INTRODUCTION AND OBJECTIVES: Ureteral reconstruction continues to evolve to include less invasive techniques to successfully manage ureteral stricture. However, long, complex, obliterative and especially radiated ureteral strictures are not amenable to less invasive techniques and may require Ileal ureter interposition. We report our 16 year experience with ileal ureter interposition for complex ureteral stricture. METHODS: Retrospective review of a single institution’s ureteral reconstruction database was performed. Demographics, operative details , type of reconstruction, success rate, complication rate and length of follow-up were noted. Unilateral replacements utilized ileal ureteral interposition. Bilateral ileal ureters were performed using the “reverse 7” technique. Success rate was defined as no need for further open intervention. RESULTS: Between 2003 and 2019, 188 ureteral reconstructions were performed, of which 46 required ileal ureter interposition. Of these 46 patients, 10 required bilateral reconstruction. Average age was 53 years, 26 (57%) were female. The average stricture length was 9.1 cm. Stricture etiology included iatrogenic causes (n=24, 52%), radiation (n=12; 26%), vascular disease (n=3; 7%), and idiopathic retroperitoneal fibrosis (n=3; 7%). Forty-three surgeries were performed by open abdominal approach; 3 were performed robotically. The average length of operation was 412 minutes, blood loss = 417 mLs, LOS=10 days, 11 (24%) patients experiencing a major complication. At mean follow up of 4.4 years, overall success rate was 83%, with 17% (n=8) patients requiring subsequent major surgery (5 successful ureteral revision, 3 nephrectomy). CONCLUSIONS: In our long-term follow up of over 4 years, ileal ureteral interposition remains a successful option for complex ureteral strictures in properly selected patients. Funding: None Back to Summary Page 5
Creation of continent urinary channel using the spiral monti technique Alan Quach, MS; David S. Koslov, MD; Kirk D. Redger, MD; Ty T. Higuchi, MD; Brian J. Flynn, MD University of Colorado SOM, Division of Urology 12631 E 17th Ave, C-319 Denver, CO 80045 United States Title: Creation of continent urinary channel using the spiral monti technique Category: Reconstructive urology Abstract: Introduction and Objectives: For patients with neurogenic bladder dysfunction, the Mitrofanoff principle has been utilized for over 30 years to provide a reliable catheterizable urinary channel. However, in morbidly obese patients or patients without an appendix, an ileal segment may be used as an alternative to appendicovesicostomy. In some morbidly obese patients, a single Monti tube may not be able to reach the skin. Subsequently, Casale has described the Spiral Monti technique, which allows for longer catheterizable channels (up to 14cm) using a shorter piece of bowel. This video will demonstrate our technique with creation of a urinary channel in an adult using a single piece of bowel. Methods: This video illustrates a representative case of the Spiral Monti technique in a 67 year old female with neurogenic bladder due to stable multiple sclerosis. Results: At our institution we identified 20 women and 6 men with a mean age of 48 years (range, 25-80) and a follow-up of 64 months (range, 22-100) who underwent creation of a continent urinary channel. The mean body mass index (BMI) was 30.5 kg/m 2 (range, 20.1- 50.2). All patients had benign bladder disease, including 22 (85%) with known neurologic disease and 4 with a devastated bladder outlet. Creation of a continent urinary channel was performed using the single Monti tube in 1, double Monti tube in 7, and the Casale (Spiral Monti) in 18. Mean hospital stay was 10.5 days (range, 5-37). There were 5 (19%) bowel complications and 1 (4%) bladder perforation. The percentage of patients continuing to catheterize via the stoma with a BMI of 40 kg/m 2 was 89%, 50%, and 25%, respectively. Conclusions: The Monti and Casale procedures are effective in creating a long continent urinary channel for catheterization in the adult population with neurogenic bladder, regardless of BMI. Funding: none Video: https://drive.google.com/file/d/1QKYxSyG5eZNuQqaZgR5-T1LWXpe7v0_F/view?usp=sharing 6 Back to Summary Page
TITLE: SPINA BIFIDA ONLINE EDUCATION SERIES FOR TRANSITIONAL PATIENTS IN THE ERA OF COVID-19 Authors: Anessa Sax-Bolder BA*, Alan Quach BS, Cindy Buchanan PhD, Ty Higuchi MD PhD Division of Urology, University of Colorado Hospital; 1635 Aurora Court, Aurora, CO 80045 TITLE: SPINA BIFIDA ONLINE EDUCATION SERIES FOR TRANSITIONAL PATIENTS IN THE ERA OF COVID-19 CATEGORY: Pediatric Urology INTRODUCTION: Spina Bifida (SB) is a congenital spinal defect with multiple urologic manifestations requiring life-long urologic care. Transition to adult health care can be particularly difficult for patients with complex medical issues, especially during COVID-19. Our team created an online educational series for patients with SB to help provide education and community building. Herein, we describe our experience with a virtual SB Education Series and the results of survey-based patient experience through a virtual platform. METHODS: Patients with SB ages 16-24 and their caregivers were identified at a single tertiary academic medical center and were invited to the zoom education day series. Pre and post session surveys were collected, and data analyzed. RESULTS: There were a total of 68 registrations for 4 conferences held between 5/3/20- 12/9/20. 24, 24, 21,36 invitations were sent out before each session and 18,18, 11, 21 patients attended each education session, respectively. A total of 46% (31/68) participants completed the pre-survey and 19% (13/68) completed the post-survey. The survey results can be found in Table 1. Participants were comfortable using telehealth for medical visits (4.87), found them easy (4.69) and would use telehealth for future appointments (4.7). This did not increase significantly after the educational sessions. However, there was a significant increase in patients’ comfort of navigating non-emergent medical problems during the COVID-19 pandemic between pre and post-survey results (4.07 vs 5.17, p
Table 1: Pre and Post Survey Results Pre-Survey Post- P-Value (Unpaired (n=31) Survey t test results) (n=13) I feel comfortable using telehealth for medical visits. 4.87 4.52 0.344 (Disagree 1-6 Agree) It is easy to use telehealth for medical visits. 4.69 4.71 0.9737 (Disagree 1-6 Agree) I would use telehealth in the future for health 4.7 5.17 0.2447 services. (Disagree 1-6 Agree) How prepared do you feel to navigate a non 4.07 5.31 0.0018 emergent medical problem during COVID-19? (Disagree 1-6 Agree) I have little sense of togetherness with my peers 3.47 3.51 0.9447 (Disagree 1-6 Agree) I catch myself losing a sense of connectedness with 3.68 4.25 0.3118 society (Disagree 1-6 Agree) I am able to connect with other people (Disagree 1-6 4.45 4.89 0.2874 Agree) How likely are you to attend another education day in n/a 5.9 n/a future? 8 Back to Summary Page
MARKET TRENDS IN REGENERATIVE THERAPIES FOR ERECTILE DYSFUNCTION ACROSS MAJOR METROPOLITAN CITIES Gary Shahinyan*, BA, University of Colorado School of Medicine, Aurora, CO Robert Shahinyan, BA, UCLA, Los Angeles, CA Shangyang Christopher Yang, BS, UCLA, Los Angeles, CA James Weinberger MD, UCLA, Los Angeles, CA Jesse Mills, MD, UCLA, Los Angeles, CA Sriram Eleswarapu, MD PhD, UCLA, Los Angeles, CA MARKET TRENDS IN REGENERATIVE THERAPIES FOR ERECTILE DYSFUNCTION ACROSS MAJOR METROPOLITAN CITIES Category: Andrology Abstract: Introduction and Objective: A booming market focused on “regenerative” therapies has emerged to cater to men suffering from erectile dysfunction (ED). Despite a lack of scientific evidence, providers have begun to market platelet-rich plasma (PRP) and stem cell therapy directly to consumers. These treatments are not recommended beyond an investigational role by the AUA. In this study, we aimed to characterize the landscape of PRP and stem cell treatments for ED by evaluating trends in marketing and deployment of these therapies in large metropolitan areas. We sought to describe the cost of treatment, the variability in pricing, and the training and qualifications of providers. Methods: Utilizing Google’s search engine, we identified regenerative medicine treatment providers in seven large U.S. metropolitan areas. Search terms included: “PRP for ED in [city]”; “P shot in [city]”; “PRP for erectile dysfunction in [city]”; “Priapus shot in [city]”. Clinics were contacted by phone and data regarding providers, prices, and durations of treatment were collected. Results: A summary of results is shown in Table 1. Eighty-seven clinics provide PRP or stem cell treatments for ED in the metropolitan areas sampled. Comprehensive information was available for 68% of the clinics identified. 8% of providers had formal urology training. The average price of PRP injections was $1519 per injection (range $500- $2500). Stem cell therapy was offered by 10 providers, averaging $3620 per treatment (range $1000-$7000). Treatment courses ranged from one injection to indefinite injections based on patient circumstance. Conclusions: PRP and stem cell treatments suffer from exorbitant prices, substantial inconsistency and lack of standardization. Non-urologists predominate while costs and frequency of therapy appear to be market-driven and lack evidence. Advertised outcomes vary with some clinics suggesting a single injection will be sufficient for cure, while others recommend repeat injections indefinitely. The AUA and SMSNA classify these treatments as experimental and state explicitly that providers should not charge patients for these treatments. The need for urologists to play an active role in preventing the proliferation of these profitable yet experimental treatments is crucial along with advancing research on these treatments. Funding: None Table 1: Market trends in providers offering PRP and stem cell treatments for ED across seven large metropolitan cities. City % Urologists % Non-Physician PRP Average Price Stem Cell Average Price Providers Atlanta, GA 0% 0% $1561 ($600-1900) - Boston, MA 0% 27% $1566 ($500-2100) $2000 ($2000-2000) Dallas, TX 0% 22% $1483 ($600-1900) - Los Angeles, CA 15% 20% $1367 ($650-2500) $3816 ($2600-5000) New York, NY 22% 0% $1564 ($1100-1900) $4700 ($2200-5000) Philadelphia, PA 17% 8% $1505 ($900-1800) $4000 ($1000-7000) Washington D.C. 0% 18% $1589 ($1200-1900) $4000 ($4000-4000) Average % 14% $1519 $3620 Back to Summary Page 9
Title: ICG Angiography in Robotic Microsurgical Spermatic Cord Denervation Author 1 * • Alan Makedon, BA • University of Colorado School of Medicine • 11033 E 28th Pl, Denver, CO 80238 Author 2 • Granville L. Lloyd, MD • Associate Professor of Surgery/ Urology • Rocky Mountain Regional VA Hospital • 1700 Wheeling Street, Aurora CO 80045 ICG Angiography in Robotic Microsurgical Spermatic Cord Denervation Introduction: Chronic orchialgia continues to be a challenge for urologists to treat and for patients to live with. Currently, conservative treatment (rest, anti-inflammatory drugs, physical therapy, antidepressants) is the first line therapy for men struggling with chronic orchialgia. However, when these approaches fail, alternative therapies are required. Before resorting to orchiectomy, microsurgical spermatic cord denervation has been shown to significantly decrease pain with few side effects. Parekatill et al described the “trifecta nerve complex,” an anatomical basis for the success of microsurgical spermatic cord denervation. Accurate microsurgical technique and especially avoidance of arterial injury is critical, especially in novice surgeons as well as in cases with aberrant anatomy. In this video presentation, we describe the use of indocyanine green (ICG) angiography in correlation with Doppler during MSCD for the purpose of arterial localization and verification of preservation. Methods: Robotic MSCD was performed in 10 cases of chronic orchialgia following failed conservative approaches and after a successful anesthetic cord block in the office. The procedure consists of a few distinct steps: division of the cremasteric muscle, isolation of the vas deferens and division of the central adipose tissue. ICG was injected twice in each procedure: to identify the testicular artery during central dissection and to confirm preservation of the artery at conclusion. Micro-doppler was used adjunctly to identify the arteries. Results: In all 10 patients, ICG angiography successfully identified the location and course of the testicular artery, including in cases of aberrant and re-operative anatomy. Doppler assessment confirmed this. Conclusion: ICG RMSCD assists and confirms spermatic cord vasculature localization, particularly in cases of difficult anatomy. This represents a valuable adjunct to this procedure, especially for novice surgeons, as well as producing visual documentation of successful arterial preservation. 10 Back to Summary Page
Title: Identification of Genes Associated with The Risk of Requiring BPH Surgery Category: General Urology Author 1* • Alan M. Makedon, BA, MS1 • University of Colorado School of Medicine • 13001 E 17th Pl, Aurora, CO 80045 Author 2 • Samuel G. Antoine, MD • University of Colorado Division of Urology • 13001 E 17th Pl, Aurora, CO 80045 Author 3 • Granville L. Lloyd, MD • Associate Professor of Surgery/ Urology • Rocky Mountain Regional VA Hospital • 1700 Wheeling Street, Aurora CO 80045 Identification of Genes Associated with The Risk of Requiring BPH Surgery Introduction: Benign prostatic hyperplasia (BPH) and associated lower urinary tract symptoms (LUTS) have high prevalence and increasingly large societal burden. The pathogenesis of BPH remains unclear but heritable factors have been shown to significantly influence prostate volume and increase the chances of requiring surgery. This study aimed to assess the presence of genomic differences in men that require BPH surgery when compared to men that do not. Methods: We evaluated single-nucleotide polymorphism (SNP) based heritability of BPH and conducted a genome-wide association study (GWAS) of BPH surgery risk using cases and controls. Scrubbed data was obtained from the University of Colorado Biobank and exempt from IRB approval. Using SAIGE v0.39, 103,154 LD-pruned SNPs of MAF ≥ 0.01 across 33,864 samples were used to generate kinship estimations with relatedness cutoff of 0.0625. Significance of p = 10-5 was used to identify relevant SNPs. These then were used to identify associated genes using SeattleSeq (University of Washington). Results: 33,864 total patients were considered, and after selection for male gender and age 50 or greater, patients with any diagnosis of prostate or bladder cancer were excluded. Patients with only one visit were excluded. Patients were screened for presence or absence of BPH surgical or minimally invasive procedure, and men who had required a procedure (transurethral resection or laser vaporization; simple prostatectomy) were compared to men that did not. No thermal ablation or prostatic lift patients were present in this sample. 149 cases and 6,204 controls were analyzed. GWAS analysis revealed 131 SNPs (on/near 25 genes, p ≤ 10-5) that predicted need for BPH treatment. Genes associated with a p ≤ 10-6 include DOCK4, a cytokinesis gene; MRAP, a melanocortin receptor-interacting protein; and NCOA3, a hormone receptor coactivator (Table 1). Conclusion: We have identified genes significantly associated with severe LUTS/BPH requiring surgical treatment. These findings suggest a significant heritable component of LUTS/BPH. These genes may provide targets for future research, treatments or development of a polygenic risk score to identify those at risk for progression to medical/surgical treatment. Source of Funding: None Back to Summary Page 11
Table 1 12 Back to Summary Page
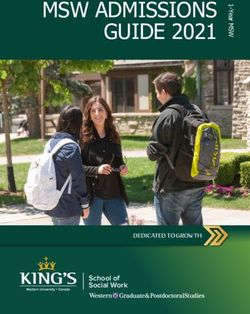
Cover Page HIGH RISK DISEASE AND POOR FOLLOWUP: THE ROLE OF RENAL MASS BIOPSY IN A COHORT OF VETERANS Kseniya Anishchenko, BA, MS21, Samuel Antoine, MD2, Rachel Lenzmeier, PA2, Simon Kim, MD2, Granville Lloyd, MD1,2 1 University of Colorado School of Medicine, 13001 E 17th Pl, Aurora, CO 80045 2 University of Colorado, Division of Urology, 13001 E 17th Pl, Aurora, CO 80045 HIGH RISK DISEASE AND POOR FOLLOWUP: THE ROLE OF RENAL MASS BIOPSY IN A COHORT OF VETERANS Category: Urologic Oncology Introduction and Objective: Renal mass biopsy (RMB) is increasingly used in the clinical management of renal masses, especially for masses ≤ 4 cm (T1a). In this study, we sought to review utility of this procedure for identification and management of small renal cell carcinoma (RCC) in the setting of the unique and comorbid population of our Veterans Affairs Hospital. Methods: From 136 renal mass biopsies performed between 06/2015 and 11/2020, 89 patients with T1a lesions were identified in this Quality Improvement analysis. Mass size, biopsy pathology, treatment, and imaging compliance were retrospectively analyzed. Surveillance compliance was compared to National Comprehensive Cancer Network (NCCN) guidelines for each treatment modality, which were recommended initially and reviewed at each patient visit. Results: The median age of our cohort at time of RMB was 66 years old. Biopsy of T1a renal masses yielded diagnostic results in 96.5% with a complication rate of 2%: one retroperitoneal bleed treated with observation and one hemorrhage requiring embolization (Clavien Grades 1 and 3). Findings of unexpectedly aggressive lesions (Fuhrman Grade 4, Type 2 papillary RCC or sarcomatoid features) were identified by biopsy in 8 (9%), with 28 (31.5%) identified as benign or indolent neoplastic processes including oncocytoma. 57 (64%) patients were treated with cryoablation or surgery and 32 (36%) patients elected active surveillance (AS) for their renal masses. 16 patients in the AS group (50%) had a neoplastic RMB finding (oncocytoma or RCC), while 52 patients in treatment group (91.2%) had a neoplastic result. At the second follow-up, compliance with NCCN-recommended imaging was 50% for surveillance, 47% among those undergoing cryoablation and 47% among those undergoing partial or radical nephrectomy. Conclusions: In this cohort, we found a significant incidence of high-risk lesions on RMB and saw poor compliance with follow-up imaging despite vigorous attempts to adhere to NCCN guidelines. Follow-up was incomplete or absent in a high percentage of patients at all time points. More aggressive biopsy protocols with high consideration of treatment may be appropriate to limit risk in those lost to follow-up. Given that 9% of our small renal masses were highly aggressive, a significant percentage may be at especially high risk in an active surveillance setting. Source of Funding: None. Back to Summary Page 13
14 Back to Summary Page
INTENSITY OF CARE AND COSTS FOR NEOADJUVANT CHEMOTHERAPY IN BLADDER CANCER: RESULTS FROM A LARGE PRIVATELY INSURED COHORT IN THE UNITED STATES Miguel Rodriguez-Homs, MD* University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, C-319, Room 5602 Aurora, CO 80045 Boris Gershman, MD Beth Israel Deaconess Medical Center Division of Urology 330 Brookline Avenue, Shapiro 3 Boston, MA 02215-5400 Badrinath Konety, MD, MBA Rush University Medical Center Department of Urology 1725 W Harrison St, Professional Building, Suite 970 Chicago, IL, 60612 Thomas Flaig, MD University of Colorado School of Medicine Department of Medical Oncology 12605 E 16th Ave Aurora, CO 80045 Michael R. Bronsert, PhD, MS University of Colorado School of Medicine 13199 East Montview Boulevard, Suite 300 Aurora, CO 80045 Jeffrey C. Morrison, MD University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, C-319, Room 5602 Aurora, CO 80045 Sarah P. Psutka, MD University of Washington Department of Urology Norm Maleng Building, 410 9th Ave. Seattle, WA 98104 Rodrigo Rodrigues Pessoa, MD, PhD University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, C-319, Room 5602 Aurora, CO 80045 Robert Abouassaly, MD Cleveland Clinic Department of Urology 11100 Euclid Ave Cleveland, OH 44106 Simon P. Kim, MD, MPH University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, Room: 6111 Aurora, CO 80045 Back to Summary Page 15
INTENSITY OF CARE AND COSTS FOR NEOADJUVANT CHEMOTHERAPY IN BLADDER CANCER: RESULTS FROM A LARGE PRIVATELY INSURED COHORT IN THE UNITED STATES CATEGORY: Urologic Oncology INTRODUCTION: Neoadjuvant chemotherapy (NAC) with gemcitabine and cisplatin (GC) or methotrexate, vinblastine, adriamycin and cisplatin (MVAC) represents the standard of care for clinical T2+Nx urothelial carcinoma of the bladder. However, the intensity of healthcare and financial costs attributable to GC versus MVAC remain poorly understood. Herein, we examined the intensity of care and costs associated with either regimen from the initiation of NAC to the postoperative period following radical cystectomy (RC). METHODS: Between 2010 to 2015, we identified all patients who received neoadjuvant GC or MVAC followed by RC in MarketScan. The primary outcomes were aggregate healthcare costs, all emergency visits, and hospital admissions from the initiation of NAC and up to 1-year following RC. We used a multivariable generalized estimating equation (GEE) model with assuming a negative binomial distribution to assess difference for each outcome by chemotherapy regimen adjusting for clinical characteristics. RESULTS: During the study interval, we identified 223 (29.5%) and 533 (70.5%) patients who received MVAC and GC, respectively. Overall, the mean age was 56.9 years (SD: 5.7) with a mean of 1.0 (SD: 1.2) emergency visits and 2.4 (SD: 1.7) hospital admissions, and $56,768.55 (SD: $106,064.17) from the initiation of NAC to 1-year following RC. On multivariable analysis, our results comparing GC to MVAC indicate similar risk adjusted averages for emergency room visits (1.1 [95% CI: 1.1 – 1.2] v. 0.7 [95% CI: 0.7 – 0.8]; p = 0.07), hospital admissions (2.4 [95% CI: 2.4 – 2.5] vs. 2.4 [95% CI: 2.3 – 2.5; p = 0.64) and aggregate health care costs ($157,789.9 [95% CI: 155,155.7 – 160,424.1] vs. $161,206.7 [95% CI: 157,175.2 – 165,238.1]; p = 0.51). CONCLUSIONS: Our results suggest similar intensity of care for emergency room visits, hospital admissions, and aggregate health care costs for GC and MVAC from the initiation of chemotherapy up to one-year after RC. Further research is needed to better ascertain treatment decisions about using GC or MVAC in a patient-centered manner. FUNDING: Schramm Foundation 16 Back to Summary Page
TITLE: ASSOCIATION OF HOSPITAL AND PATIENT CHARACTERISTICS WITH SURGERY AND CHEMOTHERAPY FOR UPPER TRACT UROTHELIAL CARCINOMA Jeffrey C. Morrison, MD1; Anessa Sax-Bolder, BA1*; Alexander Kutikov, MD2; Marc Smaldone, MD2; Robert Abouassaly, MD3; Rodrigo Rodrigues Pessoa, MD, PhD1; Simon P. Kim, MD, MPH1 1, Division of Urology, University of Colorado Hospital, 1635 Aurora Court, Aurora, CO 80045 2, Division of Urologic Oncology, Fox Chase Cancer Center, 333 Cottman Avenue, Philadelphia, PA 19111 3, Department of Urology, Cleveland Clinic, 18101 Lorain Avenue, Cleveland, OH 44111 TITLE: ASSOCIATION OF HOSPITAL AND PATIENT CHARACTERISTICS WITH SURGERY AND CHEMOTHERAPY FOR UPPER TRACT UROTHELIAL CARCINOMA CATEGORY: Urologic Oncology INTRODUCTION: Perioperative chemotherapy is increasingly recognized as the optimal treatment for high-grade upper tract urothelial carcinoma (UTUC) with radical nephroureterectomy (RNU). With the barriers to this treatment approach poorly understood, we sought to characterize patient and hospital characteristics associated with this multi-modal treatment strategy. METHODS: Using the National Cancer Database (NCDB), we identified all patients who presented with high grade UTUC (cTa-4Nx,1) from 2004 to 2013. We designated RNU and perioperative systemic chemotherapy as the primary outcome. Bivariate and multivariable analyses were used to identify patient and hospital characteristics associated with the primary outcome. RESULTS: Amongst the 14,566 patients in our analytic cohort 90.7% and 30.3% underwent RNU and received perioperative chemotherapy, respectively. There was a greater use of RNU and perioperative chemotherapy from 23.1% in 2004 to 32.5% in 2013 (p < 0.001 for trend). On multivariable analysis, lower use of RNU and perioperative chemotherapy was observed for black relative to white patients (OR: 0.75; p
HEALTH CARE COSTS AND HOSPITAL READMISSIONS FOR RADICAL CYSTECTOMY FOR BLADDER CANCER BY SURGICAL APPROACH AND DIVERSION Miguel Rodriguez-Homs, MD* University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, C-319, Room 5602 Aurora, CO 80045 Jeffrey C. Morrison, MD University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, C-319, Room 5602 Aurora, CO 80045 Badrinath Konety, MD, MBA Rush University Medical Center Department of Urology 1725 W Harrison St, Professional Building, Suite 970 Chicago, IL, 60612 Boris Gershman, MD Beth Israel Deaconess Medical Center Division of Urology 330 Brookline Avenue, Shapiro 3 Boston, MA 02215-5400 Michael R. Bronsert, PhD, MS University of Colorado 13199 East Montview Boulevard, Suite 300 Aurora, CO 80045 Alexander Kutikov, MD Fox Chase Cancer Center Division of Urology and Urologic Oncology 333 Cottman Ave Philadelphia, PA 19111 Janet B. Kukreja, MD University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, Room: 6111 Aurora, CO 80045 Rodrigo Rodrigues Pessoa, MD, PhD University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, C-319, Room 5602 Aurora, CO 80045 Simon P. Kim, MD, MPH University of Colorado School of Medicine Division of Urology 12631 East 17th Avenue, Room: 6111 Aurora, CO 80045 18 Back to Summary Page
HEALTH CARE COSTS AND HOSPITAL READMISSIONS FOR RADICAL
CYSTECTOMY FOR BLADDER CANCER BY SURGICAL APPROACH AND
DIVERSION
CATEGORY: Lap/robotic urology
INTRODUCTION: Radical cystectomy (RC) is associated with a high risk of
postoperative complications and higher health care costs. Although robotic surgery has
been initially shown to increase costs, readmission and health care costs attributable to
surgical approach (robotic versus open) and type of diversion (ileal conduit {IC} versus
neobladder {NB}) in the post-dissemination robotic era remain largely unknown. We
aimed to assess the comparative outcomes of a large privately insured cohort of
bladder cancer (BCa) patients by surgical approach and diversion.
METHODS: Using the MarketScan database, we identified all patients diagnosed with
BCa and underwent open or robotic RC and IC or NB from 2010 – 2015. The primary
outcomes were index length of stay (LOS), 90-day readmission, and total health care
costs. We used multivariable logistic regression and generalized estimating equations to
assess for 90-day readmission and health care costs, respectively, adjusting for age,
gender and Elixhauser comorbidity.
RESULTS: During the study interval, a majority of patients underwent open RC with IC
(56.7%; n = 1680) followed by open RC with NB (22.7%; n = 672), robotic RC with IC
(17.4%; n = 516), and robotic RC with NB (3.1%; n = 93). Patients had lower LOS when
undergoing robotic RC with IC (7.4; SD: 4.5) compared to open RC with IC (8.7 days,
SD: 7.0), open RC with NB (8.9 days; SD: 6.3), and robotic RC with NB (8.6 days; SD:
4.8). On multivariable analysis, patients had higher odds of 90-day readmission for open
RC with NB (OR: 1.5; 95% CI: 1.3 – 1.9), robotic RC with IC (OR: 1.3; 95% CI: 1.0 –
1.6), and robotic RC with NB (OR 1.8; 95% CI: 1.1 – 2.7) compared to open RC with IC.
Similarly, open RC with IC was associated with significantly lower 90-day adjusted costs
($65,761.2; 95% CI: $65,078.4 – $66,444.0) compared to robotic RC with IC
($71,671.4; 95% CI: $70,460.1 – $72,882.7), robotic RC with NB ($76,502.0; 95% CI:
$73,277.0 – $79,726.9), and open RC with NB ($76,252.6; 95% CI: $75,139.7 –
$77,365.5).
CONCLUSIONS: In this population-based cohort of privately insured patients
undergoing RC, neobladder diversion was associated with higher risk of readmission
and health care costs. Increased attention in reducing readmissions and perioperative
care for patients undergoing NB may substantially reduce costs.
FUNDING: Schramm Foundation
TABLE 1:
Open RC Open RC Robotic RC Robotic RC
with IC with NB with IC with NB
Number of patients 1680 672 516 93
Length of stay (days) 8.7 ± 7.0 8.9 ± 6.3 7.4 ± 4.5 8.6 ± 4.8
Odds of 90-day OR: 1.5 OR: 1.3 OR 1.8
readmission relative -- (95% CI: 1.3 (95% CI: 1.0- (95% CI: 1.1 –
to open RC with IC – 1.9) 1.6) 2.7)
65,761 76,252 71,671 76,502
90-day adjusted (95% CI: (95% CI: (95% CI: (95% CI:
health care costs ($) 65,078 - 75,139 - 70,460 - 73,277.0 -
66,444) 77,365) 72,882) 79,726.9)
Back to Summary Page 19TITLE: NEUROFIBROMATOSIS 1 CAN HAVE PLEXIFORM NEUROFIBROMAS WITH DIFFUSE GANGLIONEUROMATOSIS INFILTRATING THE URINARY BLADDER CAUSING URINARY TRACT SYMPTOMS Authors: Anessa Sax-Bolder BA1*, Katie Hall MD 2, Brian E. Moore MD,2 Francisco G. La Rosa MD2, Ty Higuchi MD PhD1 1, Division of Urology, University of Colorado Hospital; 1635 Aurora Court, Aurora, CO 80045 2, Department of Pathology, University of Colorado Hospital; 12605 E. 16th Ave, Aurora, CO 80045 TITLE: NEUROFIBROMATOSIS 1 CAN HAVE PLEXIFORM NEUROFIBROMAS WITH DIFFUSE GANGLIONEUROMATOSIS INFILTRATING THE URINARY BLADDER CAUSING URINARY TRACT SYMPTOMS CATEGORY: Reconstructive Urology INTRODUCTION: Neurofibromatosis 1 (NF1) is the most common inheritable neurologic disorder and recognized by characteristic manifestations such as café-au-lait macules, axillary freckling, multiple neurofibromas (NF) and lisch nodules. Urologists become familiar with NF1 while studying for their residency in-service examination due to association of NF1 with pheochromocytoma. In addition, NF can invade the bladder causing lower urinary tract symptoms. Plexiform neurofibromas (PNF) and Ganglioneuromas (GN) are rare forms of NF that can have malignant potential. Simultaneous presence of both lesions (PNF and GN) directly involving the urinary bladder of NF1 patients is extremely rare with only 5 cases reported in the literature. Herein, we present two NF1 patients with this very rare combination of PNF and GN lesions involving the urinary bladder. METHODS: We identified two patients with NF1 with concurrent PNF and GN lesions of the urinary bladder. Demographic data, surgical management and outcomes were collected. RESULTS: Patient A was a 26-year-old female and Patient B was a 22-year-old male. Both patients had a previous diagnosis of NF1 and both patients initially underwent medical management of their symptoms and surveillance of their upper tract. Eventually, both patients required surgical intervention for their urinary retention, hydronephrosis and recurrent infections. Patient A initially underwent Mitrofanoff, but due to non-compliance and recurrent UTI, underwent a cystectomy and ileal conduit. At the time of follow up eighteen months later she has not required additional surgical intervention and her renal function is stable. Patient B was initially treated with a transurethral resection of bladder neck tumor but required a Mitrofanoff with bilateral ureteral reimplantation one year later. At post-op month six he is tolerating catheterization through his Mitrofanoff. Clinical or radiologic concern for malignant transformation has not been reported at eighteen and six months follow up for both patients respectively. CONCLUSION: In patients with NF1, it is important to consider the presence of urinary bladder involvement when there are urinary tract symptoms and/or abnormal bladder imaging. If PNF and GN lesions are identified on pathology, the risk of malignant transformation must be factored into their follow-up. Due to the rarity of this condition, specific therapy or follow-up has not been established but urologists need to be aware of the association of NF1 with lower urinary tract symptoms and the risk of malignant transformation of patients with PNF and GN lesions on final pathology. FUNDING: NONE 20 Back to Summary Page
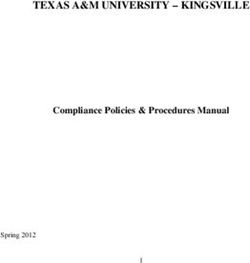
Double-blind, Placebo-controlled Randomized Controlled Trial of NSAID Prior to Ureteral Stent Removal in a Pediatric Population Brett M. Wiesen*1 N. Valeska Halstead MD, MPH1 Kyle O. Rove MD1 Alan R. Bielsky MD2 Jeffrey B. Campbell MD1 1 Children’s Hospital of Colorado, Department of Surgery, Division of Urology 2 Children’s Hospital of Colorado, Department of Anesthesiology, Division of Pediatric Anesthesiology Principle Investigators: Jeffrey Campbell, Kyle Rove Presenter: Brett Wiesen Category: Pediatric Urology BACKGROUND Ureteral spasm is a common complication with ureteral stents. This process is partially mediated by prostaglandins and may be suppressed by cyclooxygenase inhibitors like NSAIDs. Current practices vary widely for pain management in patients with ureteral stents, sometimes including opioids. OBJECTIVES We aimed to determine if NSAID given prior to stent removal would reduce postoperative pain. We hypothesized there would be at least a 75% reduction in postoperative severe pain in patients receiving ibuprofen compared to placebo. Severe pain was defined as a pain score ≥7. METHODS We performed a double-blind, placebo-controlled randomized controlled trial on pediatric urology patients with an indwelling ureteral stent undergoing removal in the operating room from 2014–2019. 20 patients in each arm were needed to achieve 80% power to detect a 75% reduction in the estimated 55% incidence of severe postoperative (α=0.05). Patients ≥4 years old who had a unilateral stent placed after treatment of urolithiasis or ureteropelvic junction obstruction were randomized to NSAID or placebo in a 1:1 ratio at least 15 minutes prior to scheduled stent removal. Patients estimated pain using Faces Pain Scale-Revised (FPS-R) or visual analogue scale (VAS) prior to and 24 hours after stent removal. RESULTS 254 patients undergoing stent removal were assessed for eligibility, and 44 randomized patients were analyzed using intention to treat analysis. The cohorts were demographically similar and received similar anesthesia treatment. There was no significant difference in maximum PACU pain score (p=0.540) or use of in-hospital opioids (p=0.626) between the two groups. No difference was seen in the incidence of severe post-operative pain (p=1.0), thus rejecting our hypothesis. Significant worsened postoperative pain (pain score increases of ≥2 between time points) decreased from 22.7% to 9.1% between placebo and NSAID, but this did not reach significance (p=0.410). CONCLUSION Back to Summary Page 21
There was no difference in postoperative pain for patients undergoing ureteral stent removal given preoperative NSAID versus placebo. SIGNIFICANCE The incidence of severe pain before and after stent removal was low, ranging from 4.5–9.1%. Our study may have been underpowered given the low incidence of severe pain. Research to minimize pain and stress of operations, even “minor” ones, should continue in order to optimize patient outcomes. Patients assessed for eligibility 254 patients Excluded 203 patients 103 – age < 4 years 61 – not UPJO nor stone Enrollment 48 – multiple procedures Patients enrolled 36 – prior kidney transplant 19 – not approached 51 patients 17 – bilateral stents 7 – developmental delay Withdrawn 4 – allergy to NSAIDs 4 – patient declined 2 patients 2 – history of asthma After hrs, unable to randomize 2 – CKD or receive study drug (n = 2) 0 – nasal polyps 0 – pregnant Patients randomized * patients could be excluded for multple reasons 49 patients Allocation Allocated to placebo Allocated to NSAID 25 patients 24 patients Received drug (n = 25) Received drug (n = 23) Did not receive drug (n = 0) Did not receive drug (n = 1) Follow up Lost to follow up Lost to follow up Incomplete surveys (n = 2) Incomplete surveys (n = 1) Analyzed Analyzed Analysis 22 patients 22 patients Excluded from analysis: Excluded from analysis: did not meet inclusion criteria (n = 1) misplaced consent (n = 1) Figure 1. CONSORT study flow diagram of patients assessed, enrolled, randomized, allocated, followed up, and ultimately analyzed. Intention to treat analysis was used. Reasons for exclusion at various stages are listed. One patient did not receive the drug in the NSAID arm secondary to ordering and pharmacy delays. This same patient had an incomplete survey and was thus lost to follow up. Two patients in the placebo arm had incomplete surveys and were categorized as lost to follow up. One patient from each arm was excluded from the final analysis for logistical reasons: one for improper enrollment and another for misplaced consent. In the case of the misplaced consent, family was contacted multiple times unsuccessfully and ultimately withdrawn at the request of the Institutional Review Board. 22 Back to Summary Page
Back to Summary Page 23
24 Back to Summary Page
TITLE: MULTIDISCIPLINARY SURGICAL MANAGEMENT OF PUBIC OSTEOMYELITIS Authors: Anessa Sax-Bolder BA1*, Eseosa Enabulele BDS MPH22, Ty Higuchi MD PhD1, Jason Stoneback MD3 1, Division of Urology, University of Colorado Hospital; 1635 Aurora Court, Aurora, CO 80045 2, Department of Orthopedics, University of Colorado Hospital; 12631 E 17th Ave #45, Aurora, CO 80045 TITLE: MULTIDISCIPLINARY SURGICAL MANAGEMENT OF PUBIC OSTEOMYELITIS CATEGORY: Reconstructive Urology INTRODUCTION: Pubic osteomyelitis (PO) is an uncommon yet potentially devastating diagnosis with increasing reports in the urologic literature. Patients present with recurrent UTI, pelvic pain, dystrophic calcification, urinary retention or pelvic sepsis. Patients commonly have a history of radiation therapy for pelvic malignancy and develop subsequent outlet obstruction requiring endoscopic treatment which leads to PO. PO can cause significant morbidity and mortality and few studies have described the optimal approach to the evaluation and treatment of these patients. We describe our experience with multidisciplinary management of PO. METHODS: Retrospective chart reviews were completed at a single tertiary academic medical center. Patients who underwent surgery for PO from 2013-2020 were included. Patients underwent evaluation with physical examination, CRP and MRI. Cases were reviewed by 2 surgeons and a musculoskeletal radiologist prior to intervention. Demographic data, surgical management and outcomes were collected. RESULTS: 17 patients met study criteria. Demographics and outcomes are described in Table 1. 70% (12/17) had a history of prostate cancer and radiation. Median time from last radiation dose to presentation of PO was 9 years (range 2-17). Prior to presentation to our institution, 76% (13/17) had a history of outlet obstruction managed endoscopically. At the time of presentation 88% (15/17) had pelvic pain and 76% (13/17) had difficulty walking. CRP was elevated in 94% (16/17) and MRI showed radiographic evidence of osteomyelitis in 100% (17/17) while only 94% (16/17) had a fistula. Surgical management of PO included cystectomy with/without prostatectomy with urinary diversion and omental flap with concomitant anterior pelvic resection that was guided by preoperative imaging. Positive bone and tissue cultures were identified in 76% (13/17) patients and all patients continued on 6 weeks of antibiotics. One patient died on POD105 from cardiac complications. At a median follow up time of 14 months (range 3-30) 76% (13/17) of patients had resolution of their pelvic pain and none of them had recurrence of their infection. CONCLUSION: PO is a devastating condition that can present with pelvic pain and difficulty walking. Preoperative evaluation with labs, MRI and review with a multidisciplinary team is pivotal in treatment planning. Treatment is often surgical with removal of urinary system in combination with pubic resection and long-term antibiotics. FUNDING: NONE Back to Summary Page 25
Table 1: Patient Demographics and Pubic Osteomyelitis Parameters Risk factors for pubic osteomyelitis Smoking (Current + Former) 47% (8/17) Diabetes 23% (4/17) Prostate Cancer 70% (12/17) Prostatectomy + Radiation (XRT) 16% (2/12) XRT alone 42% (5/12) XRT with adjuvant brachytherapy 33% (4/12) XRT with adjuvant cryotherapy 8% (1/12) Development of outlet obstruction 76% (13/17) Subsequent endoscopic procedure 76% (13/17) Median time from Radiation to presentation of PO 9 years (2-17) Presentation of Pubic Osteomyelitis Pelvic Pain 88% (15/17) Abscess 100% (12/12) Recurrent UTI 59% (10/17) Sepsis 82% (14/17) Difficulty Ambulating 76% (13/17) Initial Management of pubic osteomyelitis Antibiotics 94% (16/17) I&D 41% (7/17) Chronic Suppression 65% (11/17) Preoperative Diagnosis of Pubic Osteomyelitis Positive Urine Culture 76% (13/17) Elevated CRP 94% (16/17) Fistula to Urinary Tract 94% (16/17) MRI showing PO 100% (17/17) Pre Op CT-guided MSK biopsy 59% (10/17) Intraoperative Cultures Positive Bone Cultures 76% (13/17) Positive Tissue Cultures 76% (13/17) Postoperative Outcomes Pain Improvement 76% (13/17) Recurrence of Infection 0% (0/17) Currently on antibiotics 23% (4/17) 26 Back to Summary Page
TITLE: CONCORDANCE OF PRE- AND INTRA-OPERATIVE BIOPSY IN PUBIC OSTEOMYELITIS Authors: Anessa Sax-Bolder BA1*, Eseosa Enabulele BDS MPH2, Ty Higuchi MD PhD1, Jason Stoneback MD3 1, Division of Urology, University of Colorado Hospital; 1635 Aurora Court, Aurora, CO 80045 2, Department of Orthopedics, University of Colorado Hospital; 12631 E 17th Ave #45, Aurora, CO 80045 TITLE: CONCORDANCE OF PRE- AND INTRA-OPERATIVE BIOPSY IN PUBIC OSTEOMYELITIS CATEGORY: Reconstructive Urology INTRODUCTION: Pubic osteomyelitis (PO) is rare and devastating diagnosis with a variety of etiologies. There have been increasing reports of PO in the urologic literature. Historically, first line treatment for PO has been antibiotic treatment. More recently, a multidisciplinary surgical approach has been used, commonly including radical cystectomy with ileal conduit and omental flap with simultaneous anterior pelvic resection with intra-operative biopsies. Pre-operative CT-guided bone biopsies for pathology and culture data can be helpful in guiding therapy. Herein we report the concordance of pre and intra-operative biopsies in pubic osteomyelitis. METHODS: Retrospective chart reviews were completed at a single tertiary academic medical center. Patients that received surgery for PO from 2013-2020 were included. Demographic data, surgical management and outcomes were collected. RESULTS: A total of 17 patients were identified. 10 patients (59%) underwent a pre-operative CT-guided biopsy with 50% (5/10) yielding negative bone culture (BC) results. Of the negative BC results, 4 patients had positive intra-operative BCs. The remaining patient had a negative intra-operative BC but did have a positive intra-operative tissue culture. Of the 5 positive pre- operative BCs, 4 had intra-operative BCs that grew different organisms not found in the pre- operative biopsy. The final patient with a positive pre-operative BC had a negative intra- operative BC. Overall, of the 10 patients who underwent pre-operative BC, 90% (9/10) had discordance between their pre-operative CT-guided BC and their intra-operative BC. No patients had pre-operative biopsy showing cancer yet, and 24% (4/17) of patients had intra- operative frozen sections that were positive for cancer (prostatic adenocarcinoma, colorectal adenocarcinoma, urothelial cell carcinoma and squamous cell carcinoma). Importantly, all 4 patients had a history of radiation for prostate cancer and 3 had negative pre-operative bone biopsies. One recent patient not included in the study had a bone biopsy showing urothelial carcinoma, thus the success rate of bone biopsy in our series is 9% (1/11). CONCLUSION: Based on this single-center review, pre-operative BC was not concordant with intra-operative BC. Potential explanations include the limited sample obtained in pre-operative BC or subsequent antimicrobial treatment after pre-operative BC. This study suggests caution should be used when basing clinical decisions off pre-operative BC due to risk of misguiding antimicrobial treatments. Importantly pre-operative biopsy for pathology should be performed to rule out malignancy, however in our series this yielded low success rate and intraoperative frozen sections are vital. FUNDING: NONE Back to Summary Page 27
Robotic repair of abdominal wall mesh bladder erosion Alan Quach, MS; David Koslov, MD; Humberto Villarreal, MD; Brian J. Flynn, MD University of Colorado SOM, Division of Urology 12631 E 17th Ave, C-319 Denver, CO 80045 United States Title: Robotic repair of abdominal wall mesh bladder erosion Category: Reconstructive Urology Abstract: Erosion of bladder is a rare complication from a common procedure. Risks include intraoperative bladder injury or delayed migration presenting as hematuria. We discuss a case study on a 62 year old male with a history of bladder neck reconstruction as a child who underwent uncomplicated laparoscopic bilateral inguinal hernia repair with mesh. We demonstrated the value of robotic surgery in the removal of polypropylene mesh from the bladder. Diagnosis can be made with cystoscopy, with or without CT and robotic repair can be achieved with excellent outcomes. Funding: none Video: https://drive.google.com/file/d/1sf9UBcG1gW_1RPT77_E65mgKgO9pxrUo/view?usp=sharing 28 Back to Summary Page
You can also read