Scaling up newborn care in Afghanistan: opportunities and challenges for the health sector - Oxford Academic ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Health Policy and Planning, 33, 2018, 271–282
doi: 10.1093/heapol/czx136
Advance Access Publication Date: 27 November 2017
Review
Scaling up newborn care in Afghanistan:
opportunities and challenges for the
health sector
Malalai Naziri1, Ariel Higgins-Steele1,*, Zelaikha Anwari2,
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
Khaksar Yousufi1, Karla Fossand3, Sher Shah Amin3, David B Hipgrave1
and Sherin Varkey1
1
UNICEF Afghanistan, Health Section, UNOCA Jalalabad Road, Kabul, Afghanistan, 2Ministry of Public Health,
Reproductive, Maternal, Newborn, Child, and Adolescent Directorate, Kabul, Afghanistan and 3Health programme,
USAID, Kabul, Afghanistan
*Corresponding author. UNICEF Afghanistan, UNOCA Jalalabad Road, Kabul, Afghanistan. E-mail: ahiggins@unicef.org
Accepted on 12 September 2017
Abstract
Newborn health in Afghanistan is receiving increased attention, but reduction in newborn deaths
there has not kept pace with declines in maternal and child mortality. Using the continuum of care
and health systems building block frameworks, this article identifies, organizes and provides a syn-
thesis of the available evidence on and gaps in coverage of care and health systems, programmes,
policies and practices related to newborn health in Afghanistan. Newborn mortality in Afghanistan
is related to the nation’s weak health system, itself associated with decades of conflict, low and
uneven coverage of essential interventions, demand-side and cultural specificities, and compro-
mised quality. A majority of deliveries still take place at home. Birth asphyxia, low birth weight,
perinatal infections and poor post-natal care are responsible for many preventable newborn
deaths. Though the situation has improved, there remain many opportunities to accelerate
progress. Analyses conducted using the Lives Saved Tools suggest that an additional 10 405
newborn lives could be saved in Afghanistan in 5 years (2015–20), through reasonable increases
in coverage of these high-impact interventions. A long-term vision and strong leadership are
essential for the Ministry of Public Health to play an effective stewardship role in formulating
related policy and strategy, setting standards and monitoring maternal and newborn services.
Promotion of equitable access to health services, including health workforce planning, develop-
ment and management, and the coordination of much-needed donor support are also imperative.
Keywords: Afghanistan, neonatal health, maternal and child health, health systems
Introduction Health in 2010, and to its 2015 revision (UNSG 2010, 2014), which
As the proportion of young child deaths occurring in the newborn introduced a focus on adolescents and new mortality targets for
period (age 0–28 days) increases (Liu et al. 2015), more attention is women, young children and newborns. The country pledged—as
now being directed at improving newborn survival. Since 2002, part of A Promise Renewed—to take action to accelerate progress
Afghanistan, notwithstanding political, security and economic chal- on MNCH, and held a related national Call to Action meeting in
lenges, has made impressive improvements in young child health, Kabul in 2015. Afghanistan has also signed on to the global Every
with a substantive fall in under-5 mortality (UNICEF 2014; WHO Newborn Action Plan (ENAP) (WHO and UNICEF 2015).
et al. 2014). Bringing more political attention to maternal, newborn Newborn health, however, has received less attention, and the
and child health (MNCH), Afghanistan committed to implementing newborn mortality rate in Afghanistan has fallen more slowly,
the United Nations Global Strategy for Women’s and Children’s as observed in many low- and middle-income countries (LMICs)
C The Author 2017. Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine.
V
All rights reserved. For permissions, please e-mail: journals.permissions@oup.com 271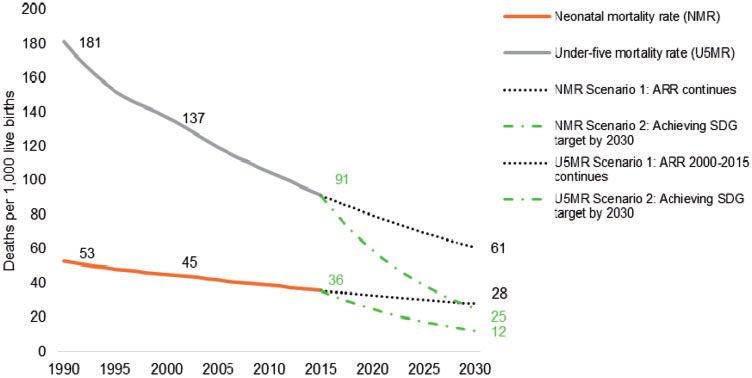
272 Health Policy and Planning, 2018, Vol. 33, No. 2
Key Messages
• Afghanistan’s health system has made impressive progress in the last decade; however, insecurity, complicated topog-
raphy, social norms and other factors contribute to persisting low coverage of life-saving neonatal interventions.
• Modest increases in essential neonatal care interventions can save thousands of newborn lives per year in Afghanistan.
• Accelerated progress for newborn survival in Afghanistan requires scaling up availability, accessibility and quality of
essential newborn care.
(Liu et al. 2015). Although under-5 child and infant mortality rates strengths and weaknesses of the local health system. A number of
fell 47.4 and 43% from 1990 to 2012, respectively, newborn conceptualizations of health systems have been developed, but the
mortality declined only 29%, to 36 deaths per 1000 live births, over one that has resonated most in recent years is the building blocks
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
the same period (WHO 2014). An estimated 37 000 newborns die framework developed by WHO (2007) (Shakarishvili et al. 2010;
annually, in Afghanistan (UNICEF 2014). The county’s high burden van Olmen et al. 2012).
of newborn death is also typical of nations experiencing recent We reviewed the available evidence on each of the six building
political instability and conflict (Lawn et al. 2012). blocks as they apply to newborn health in Afghanistan (Table 2), tak-
Since 2002, Afghanistan’s Ministry of Public Health (MoPH) ing a lead from the approaches outlined by global experts and repro-
has been establishing and expanding basic and life-saving health duced in Table 1. We also included an additional focus on community
interventions, especially in remote villages, where newborn, child ownership and participation, as a frequently perceived independent
and maternal mortality remain high. However, these areas remain influence on population health in LMIC (Musinguzi et al. 2017).
characterized by high rates of fertility, low levels of antenatal and
postnatal care and skilled birth attendance, young child malnutri- Collection of data and evidence
tion, and poor health service access, uptake and quality. Although
Available information on the influences on, and delivery of health
assessments have been done on health service delivery through
services affecting newborn health in Afghanistan was gathered, and
Afghanistan’s Basic Package of Health Services (Ameli and
categorized by four periods of the life-cycle: before conception, and
Newbrander 2008; Frost et al. 2016) and various surveys indicate
during antenatal, intrapartum and postnatal care, and according to
improvements, no systematic assessment of newborn healthcare has
the six building blocks and community-level influences. Searches
been undertaken in Afghanistan, to identify areas of related weak-
for peer-reviewed articles on newborn health in Afghanistan
ness or suggest viable strategies for scale-up.
were conducted using PubMed with the key search terms: (neonate
Using the continuum of care and WHO health systems building
block frameworks, this article identifies, organizes and provides a [All Fields] OR neonatal [All Fields] OR neonates [All Fields] OR
synthesis of the available evidence on, and opportunities for improv- newborn [All Fields] OR newborns [All Fields] AND afghanistan
ing newborn health in Afghanistan, focusing on coverage of care, AND health AND humans) (see Supplementary Web Appendix S1
health systems issues, programs, policies and practices. for flow diagram, and Supplementary Web Appendix S2 for final
articles included). Key word searches related to each phase of the
continuum of care and areas for scale-up, according to methods and
Methods standards established previously (Dickson et al. 2014) were con-
Frameworks ducted in GoogleScholar to supplement evidence on newborn health
extracted from the PubMed search. Gray literature including policy
We used two established frameworks to guide our analysis and the
and program documents was also captured by reviewing UNICEF
recommendations emanating.
Afghanistan’s internal documents on newborn health as well as
through a review of resources in the Afghanistan MoPH. Only
The continuum of care framework
papers published or written since the nation’s political reformation
Empirical evidence has established that high impact, low-cost inter-
in 2002 to April 2015 (date of searches) were included.
ventions reduce the three most common causes of newborn mortal-
Data on neonatal mortality, health status and coverage of inter-
ity in low-resource contexts: premature delivery, intrapartum
ventions was also extracted from national surveys and estimations
complications and infection (Darmstadt et al. 2005; PMNCH 2011;
that took place since 1990. Although data points were taken from a
Bhutta et al. 2014). These interventions may be delivered in the con-
text of integrated service delivery packages for maternal and new- longer period than the peer reviewed literature to underline the dire
born health (MNH) (Table 1), forming a continuum of care situation before 2002, more recent studies were preferred because of
spanning the period before conception to the end of the first month their improved methodological foundation.
of life. Three modes of delivery of these interventions have been sug- The studies and reports retained for analysis focused on newborn
gested: clinical care in health facilities, outreach or outpatient serv- survival and health and the health system in Afghanistan.
ices, and interventions that can be implemented at household or
community level (Kerber et al. 2007; Lawn et al. 2012). A contin- Data and additional analysis
uum of care framework underscores the importance of life-cycle For secondary data analysis, evidence was organized and analyzed
period and local context in considering the implementation and across the two frameworks selected. The impact of scaling up of
potential for implementation of these interventions. essential newborn care interventions was also estimated using the
Lives Saved Tool (LiST) (Boschi-Pinto et al. 2010; Winfrey et al.
Health systems building blocks 2011). In consultation with a technical committee led by the
Coverage of essential newborn health interventions across the life Afghanistan MoPH, targets for two dates—2020 and 2030—were
cycle is also associated with contextual factors, particularly the set, based on targets in existing commitments, frameworks andTable 1. Framework to scale-up newborn health strategies for countries with >30 neonatal deaths per 1000 live births (adapted from Dickson et al. 2014)
Focus of strategies for scaling up Equity, quality, supply and demand
Steps to scale-up Health-systems NMR more than 30 deaths per 1000 live births (‘strategies for this group of countries’)
building block
Step 1: Assess the situa- Community Leadership and • Increase the visibility of newborn issues in the context of reproductive, MNCH, engage stakeholders at all levels of care to raise awareness, ensure a
tion, determine prior- ownership governance coordinated convening group linked to the Ministry of Health, cultivate champions, strengthen the Neonatal Death Review Committee and closely
ities based on analyses, and follow up its action points
develop leadership partnership • Sharpen national plans and strategies, develop and promote evidence-based policies, and ensure adequate funding of key programmes
Step 2: Seize opportuni- Health financing • Increase government spending for health, allocate budget for newborn care, and seize opportunities to leverage additional resources for RMNCH initiatives
ties within the con- • Implement and expand pro-poor legislation and strategies (e.g. vouchers, community-based health insurance schemes, reimbursement of transport
straints of the existing costs) and remove user fees
health situation • Increase investment in family friendly care including infrastructure and technology in tertiary or specialized care centres
• Ensure financial protection for women and newborn babies needing emergency care
Health workforce • Strengthen the role of community providers and families to implement clean birth practices, appropriate hygiene, and basic newborn care
• Strengthen and support community providers through regular supervisory visits and strengthen linkages with health facilities
• Implement national human resources strategies that provide incentives to increase availability of providers, attract and retain skilled providers (con-
tinuous training, task shifting, compulsory service in rural areas, pay increases, etc.)
• Increase availability of nursing and midwifery skills and competencies for obstetric and newborn interventions [neonatal resuscitation, KMC, safe
oxygen management and breastfeeding support] through preservice and in-service
Health Policy and Planning, 2018, Vol. 33, No. 2
• Increase availability of specialists, e.g. obstetricians, neonatologists) in district and referral hospitals
• Establish learning centres at regional hospitals to improve quality and efficiency
• Increase efficiency and maintain skills and competencies of qualified health providers at all levels of care
Step 3: Systematically Health service • Address missed opportunities for facility births—improve emergency obstetric care (EmOC) and resuscitation
scale up care delivery • Educate and engage communities to increase early demand for quality skilled care
• Built partnerships to strengthen linkages and referral systems between communities and primary health care facilities to reduce access delays
• Implement strategies to increase quality of care, availability of standards in health facilities, ensuring supervision and mentoring of health workers,
maintaining patient-centered care and introducing maternal and perinatal audits
• Strengthen integrated management of newborn and childhood illness and routine postnatal care to ensure early detection of danger signs and improve
case management of neonatal infections by skilled providers
• Increase MNH outreach services including ANC coverage of TT1, integrated management of childhood illness (IMCI), routine postnatal care (includ-
ing extra care for small babies) and family planning
• Adapt KMC to the local context
• Address unhealthy birth practices, consider social marketing of clean birth kids
• Reach universal coverage of high-quality care for all newborn babies, including those who are preterm or ill, or both—use innovative approaches to
reach the most marginalized groups
• Improve follow-up mechanisms for newborn babies in need of long-term quality care
• Increase coverage of comprehensive EmOC and emergency neonatal care at least at referral level (then to district level)
• Establish neonatal intensive care unit (NICUs) to increase extra care of small and ill babies
• Strengthen newborn component within integrated community case management (iCCM)/IMCI to scale up CCM of neonatal sepsis in hard-to reach
areas with restricted access to health facilities
• Focus on quality ANC services to increase identification and treatment of women with pre-eclampsia and appropriate prevention of preterm labor
• Expand quality of care through perinatal audits
• Sustain long-term care and follow-up of premature babies with complications and early identification of impairment and disabilities
Essential medical • Strengthen procurement and supply chain for essential commodities
products and
technologies
Step 4: Monitor coverage, Health informa- • Improve data collection reporting, and use to improve service delivery
measure effect and tion systems • Improve birth registration, improve collation of cause of death data (in facilities and communities), institute surveillance for key newborn interven-
cost, improve data tions (e.g. survey modules for KMC)
gaps • Establish countrywide Maternal Neonatal Death Surveillance and Reporting system
273
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020274
Table 2. Integrated service delivery packages for MNCH (reproduced from Lawn et al. 2008)
Reproductive care Childbirth care Emergency newborn care
CLINICAL • Family planning • Skilled care and immediate • Extra care of pre-term babies including
• Management of STIs newborn care (hygiene, KMC
and HIV warmth, breastfeeding) and • Emergency care of sick newborns (con-
• Post-abortion care, resuscitation) text-specific e.g. CPAP)
TOP where legal • Antenatal steroids, antibiotics
for pPROM
• PMTCT of HIV
• EmOC if needed
ANC POSTNATAL CARE
OUTREACH • Family planning • Four-visit focused ANC • Promotion healthy behaviors, e.g.
• Prevention and man- package hygiene, breastfeeding, warmth
agement of STIs and • IPTp and bednets for malaria • Early detection of and referral for illness
HIV • Prevention and management • Extra care of at risk mothers and babies
• Peri-conceptual folic of STIs and HIV • PMTCT of HIV
acid
FAMILY/COMMUNITY • Adolescent and pre- • Counseling and preparation •
Where skilled care is Healthy home care including:
pregnancy nutrition for newborn care, breastfeed-
not available, consider • Promoting preventive care including
• Gender violence ing and emergency clean birth and imme- newborn care (hygiene, warmth),
• Education preparedness diate newborn care nutrition (exclusive breastfeeding, com-
• Prevention of STIs (hygiene, warmth, plementary feeding) and family planning
and HIV immediate • Seeking curative services for women,
breastfeeding) babies and children including ORS for
prevention of diarrhea and where
referral is not available, consider case
management for pneumonia, malaria
and neonatal sepsis
Intersectoral: Improved living and working conditions including housing, water and sanitation, and nutrition. Education and empowerment, especially for girls, folate fortification, safe and health work environ-
ment, especially for pregnant women.
Pre-pregnancy Pregnancy Birth Newborn/postnatal
Source: Lawn et al. (2012). Adapted from Kerber et al. (2008), revised by Kinney et al. (2010), and PMNCH (2011).
Abbreviations: ANC, antenatal care; CPAP, continuous positive airway pressure; HIV, human immunodeficiency virus; IPTI, intermittent preventive treatment in infants; IPTp, intermittent preventive treatment during preg-
nancy for malaria; ORS, oral rehydration solution; PMTCT, prevention of mother-to-child transmission of HIV; pPROM, prelabor rupture of membranes; STI, sexually transmitted infection; TOP, termination of pregnancy.
Health Policy and Planning, 2018, Vol. 33, No. 2
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020Health Policy and Planning, 2018, Vol. 33, No. 2 275
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
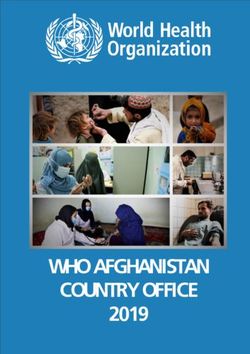
Figure 1. Trends in under-five child and newborn morality in Afghanistan with future projections (UNICEF analysis based on United Nations Inter-agency Group
for Child Mortality Estimation 2015)
mortality rate (NMR) of 12 by 2030 in Afghanistan, the desired/
expected average ARR is 5.2%, an average ARR of 11% is required
(Figure 1) (UNICEF 2014).
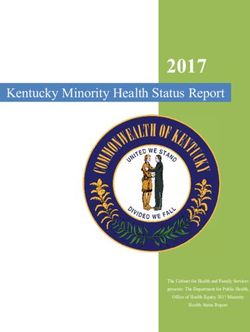
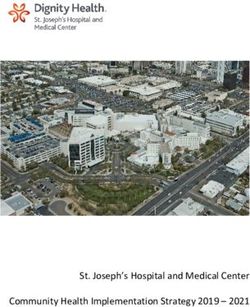
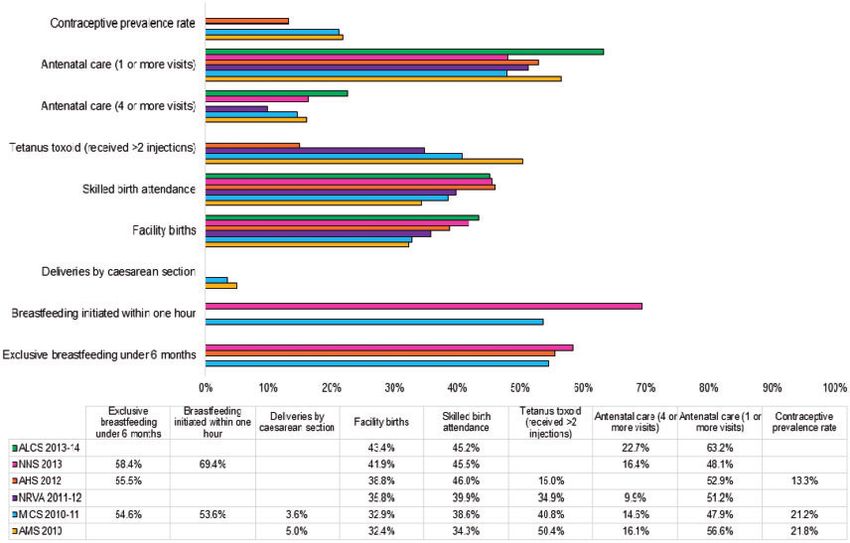
The causes of these newborn deaths are largely preventable, as
presented in Figure 2. Using data from a variety of sources, the low
coverage of many of the interventions proven to prevent the com-
monest causes of newborn death, including in Afghanistan, is pre-
sented in Figure 3. According to a secondary analysis of the 2010
Afghanistan Mortality Survey, predictors of newborn death include
birthweight, remoteness index, residence, wealth index, sanitation,
and duration of pregnancy (Adegboye and Kotze 2014).
Analyses conducted using LiST suggest that an additional 10 405
newborn lives could be saved in Afghanistan in 5 years (2015–20),
through reasonable increases in coverage of these high-impact inter-
ventions. The 21 LiST interventions related to saving additional
newborn lives are listed in descending order in Table 3. In terms of
Figure 2. Estimated causes of neonatal and child mortality for Afghanistan deaths prevented by intervention, seven1 are associated with skilled
(UNICEF 2015) birth attendance and institutional delivery, and account for 50%
of the deaths potentially prevented. Improved intrapartum care to
strategies. Two scenarios were modeled to estimate the impact of prevent asphyxia is a particular area of need. In addition to skilled
interventions: 2015–20, the timeframe of Afghanistan’s current birth attendance and institutional delivery, appropriate feeding,
Reproductive Health Strategy and National Health and Nutrition notably the promotion of early and exclusive breastfeeding, is also
Strategy and also the end date for Afghanistan’s unique Millennium predicted to make a contribution to saving additional newborn lives.
Development Goal targets (endorsed in 2004) (Afghanistan Ministry In this scenario analysis of scaled up interventions, newborn
of Economy 2013), and 2015–30, the timeframe established by the deaths by cause are still largely associated with intrapartum manage-
sustainable development goals. ment (Table 4). Asphyxia, a birth related cause, decreases over
the period by >3000 deaths but is still causing the largest overall
Expert review number of deaths in 2020, followed by prematurity and sepsis.
A committee in the Afghanistan MoPH, led by the Reproductive
Health Directorate, reviewed the analysis and provided substantive Review of the available evidence on newborn death in
guidance and inputs into this report. Afghanistan by life-cycle framework
The pre-conception period
The annual population growth rate in Afghanistan is estimated at
Results
2.7% associated with the high total fertility rate of 5.1 children per
Neonatal mortality in Afghanistan woman (Afghan Public Health Institute et al. 2011). High-fertility
Reduction of preventable neonatal mortality is one of several goals rates in Afghanistan are due in part to low contraceptive uptake
when improving the coverage rate of essential MNCH interventions (21.8% at the national level) with wide inter-provincial variation
across the continuum of care. Despite progress in reducing maternal (almost 50% in western Herat province but only 2% in Paktika, in
and child mortality rates in the past decade, reduction in the new- the southeast) (Afghan Public Health Institute et al. 2011). According
born mortality rate has been comparatively slower, with an annual to one predictive model, increasing contraceptive prevalence to 60%
rate of reduction (ARR) of only 0.1%. In order to achieve a neonatal could prevent almost 320 000 infant deaths in Afghanistan over276 Health Policy and Planning, 2018, Vol. 33, No. 2
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
Figure 3. Coverage of newborn interventions in Afghanistan from recent nationwide surveys
5 years (Rahmani et al. 2013). Family planning and reproductive ANC included the associated cost, distance and transportation
health services are not well integrated, a missed opportunity to raise problems, the perceived absence of need or a tradition of ANC, and
awareness and prevent unintended pregnancies (Singh et al. 2013), in the south, insecurity due to conflict (APHI 2011). Disrespectful
particularly since family planning is considered a primary prevention treatment was identified as another factor (Rahmani and Brekke
measure to reduce newborn and child death (Liu et al. 2015). 2013).
Misconceptions on the risks and dangers associated with contra- During ANC visits, 47.7% women received information and
ceptive use are prevalent in Afghanistan (Haider et al. 2009). Some counseling about nutrition, rest (42.3%) and exclusive breastfeeding
evidence indicates that contraceptive use increases rapidly in rural (15.5%). However, almost 21.9% reported receiving no relevant
Afghanistan when community health workers (CHWs) receive information during ANC visits (MoPH 2013; CSO 2014).
support and guidance (Huber et al. 2010).
Pre-conception nutrition is known to be associated with new- Intrapartum care
born outcomes (Mason et al. 2014). Anemia (hemoglobin < 2 g/dl), Although recent years have seen improvement in skilled birth attend-
most commonly secondary to iron deficiency, is prevalent among ance, rates remain very low in Afghanistan. Estimates range from
women of reproductive age (15–49 years) (40.4%) and adolescent 34.3 to 46% (Afghan Public Health Institute 2011; Johns Hopkins
girls (10–19 years) (29.9%) in Afghanistan MoPH (2013). University [JHU] 2012). However, even the higher estimates mean a
Additionally, knowledge of anemia is low, with under 40% of large proportion of women deliver at home with unskilled care,
women of reproductive age aware of the condition (MoPH 2013). including by traditional birth attendants (CSO 2012) with some high-
Given the empirical association between maternal anemia and low risk practices reported (Save the Children 2008). Coverage again
birthweight, premature delivery and newborn mortality (Rasmussen ranges widely from 68% in the central region to 21% in the south.
2001), control of anemia is a priority in Afghanistan, using estab- Women in Afghanistan deliver at home because of lack of transporta-
lished approaches before and during pregnancy. tion, economic problems, lack of awareness or low decision-making
power in the household. Afghan women must typically receive
Antenatal care permission from their husbands or mother-in-law to attend health
Recent surveys show low coverage of antenatal care (ANC) in facilities, even in emergency situations (Asia Foundation 2016).
Afghanistan. Only 48–59% of women had at least one assessment
during pregnancy by a doctor, nurse or midwife (Central Statistics Postnatal care
Organization [CSO] 2012; MoPH 2013; APHI 2011) and only As in most low-income countries, a large proportion of newborn
16.4–18% of women report the recommended four or more ANC deaths in Afghanistan occur during the first 24 h following delivery
visits during their last pregnancy (MoPH 2013). The timing of first (Lawn et al. 2005). Less than one-third (28%) of women received
attendance for ANC is usually late, with only 24.7% attending dur- postnatal care for their last birth (Afghan Public Health Institute
ing the first trimester (MoPH 2013). There are wide disparities in 2011). Only one in five women received postnatal care within 4 h of
ANC coverage, with the lowest level in the southern region (31%) delivery, more than one in five (22%) received care within the first
and highest in the central region (74%) (CSO 2012). ANC uptake is hours, and 2% of women are seen 2 days following delivery. Factors
higher in urban (78%) than rural areas (46%) (CSO 2014). preventing women and newborns from getting medical advice orHealth Policy and Planning, 2018, Vol. 33, No. 2 277
Table 3. Additional deaths prevented in children under 1 month of Reproductive Health Strategy 2012–16, with maternal and neonatal
age by intervention health as the first strategic component. In response to ENAP, the
MoPH has developed the National Newborn Care Comprehensive
Intervention Additional num-
ber of lives saved Operational Plan for Afghanistan, which aims to significantly
in the period reduce preventable newborn deaths. A national standard newborn
2015–20 toolkit was developed and a ‘Center of Excellence’ for newborn care
established in the major pediatric hospital in Kabul.
1 Labor and delivery management 2560
Despite progress in some areas and increased attention to new-
2 Antenatal corticosteroids for 1033
preterm labor born health, important policy gaps remain. Policies support the
3 Full supportive care for 891 international code on marketing of breastmilk substitutes and com-
prematurity munity treatment of pneumonia with antibiotics, and chlorhexidine
4 Promotion of breastfeeding 870 digluconate gel for cleaning the newborn umbilicus was recently
5 Neonatal resuscitation 703 added to the National Essential Drug List. The National Newborn
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
6 TT1 vaccination 638 Working Group is in the process of promoting its use by facility-
7 Clean postnatal practices 542
and community-based health workers. However, no policies exist
8 Chlorhexidine 527
9 Clean birth practices 480
for kangaroo mother care (KMC) of low-birthweight/premature
10 Full supportive care for sepsis/ 424 newborns, antenatal corticosteroids in management of preterm
pneumonia labor, or maternity protection (i.e. Convention 183) (Countdown
11 KMC 353 MNCH 2014).
12 Immediate assessment and 305 Many challenges exist for implementing existing and needed
stimulation policies at decentralized levels in Afghanistan. However, one study
13 Thermal care 221
found that consistent application of four ‘effective governing’
14 Antibiotics for pPRoM 219
practices (sub-committees to oversee financial transparency and
15 Oral antibiotics 153
16 Micronutrient supplementation 144 governance; collaboration with diverse stakeholders; sharper focus
(multiple micronutrients þ on community health needs, and more frequent presentation of serv-
iron folate) ice delivery data with increased use of data for decision-making)
17 Oral rehydration solution (ORS) 116 was associated with a 20% increase in ANC visits in pilot provinces
18 Injectable antibiotics 110 (Anwari et al. 2015).
19 Folic acid supplementation/ 87
fortification
20 Balanced energy supplementation 28 Financing
21 Syphilis detection and treatment 1 Health sector financing has risen substantially, with a rise from
Total 10 405 donors from $1.8 million in 2003 to $169 million in 2012 (Dalil
et al. 2014). Despite large increases in the MoPH budget, out-of-
pocket expenditures for health services are high, an estimated 73%
of total health expenditure (MoPH 2013). Health service clients
treatment during the postnatal period noted included lack of money make unofficial payments to government facilities, including those
(78%), distance and transportation to a health facility (70%), lack run by non-governmental organizations, adding to the cost of care
of medicines (30%) and security concerns (28%) (Afghan Public (Cockcroft et al. 2011).
Health Institute 2011). Households in Afghanistan spend an average of US$41/capita/
Appropriate rates of newborn feeding (early initiation and exclu- annum on health, in a nation with an average household size of 7.4
sive breastfeeding) have improved over the last few years but remain individuals (CSO 2014), and gross domestic product per capita of
low. All three recent surveys measuring exclusive breastfeeding in US$668 (UN Statistics Division 2014). Accordingly, such high
the first 6 months reported a rate below 60% (MoPH 2013; CSO expenses pose severe barriers to accessing care for individuals and
and UNICEF 2012; APHI et al. 2011). reinforces inequity in health service uptake, especially affecting the
Vaccination coverage is low in Afghanistan. According to a recent rural poor (MoPH 2013). Conditional cash transfer pilots in
immunization coverage survey, only 58.6% of mothers and their Afghanistan have shown promising results (Lin and Salehi 2013).
newborn children were protected against tetanus at the time of deliv-
ery by Tetanus Toxoid (TT1) vaccine (MoPH and UNICEF 2013). Health workforce
Afghanistan has a shortage of skilled health workers, with 22
Review of the available evidence on newborn health in (including 7.4 volunteer CHWs) per 10 000 head of population
Afghanistan by WHO building block framework (MoPH 2011); this is far below the WHO recommended minimum
Leadership and governance of 23 doctors, nurses and midwives per 10 000. Regional disparities
Improving newborn health is already among the priorities of mean there were only 16.7 public health workers (including unquali-
Afghanistan’s government: article 52 of the Constitution of fied support staff) per 10 000 in rural areas, where a majority (71%)
Afghanistan stipulates that health is a fundamental human right and of Afghanistan’s population resides (CSO 2014; Witter et al. 2015).
the Afghanistan National Development Strategy and National Afghanistan’s National Health Workforce Plan 2012–16 estab-
Action Plan for Women of Afghanistan recognize MNH as priority lished goals for increasing qualified and gender-balanced health
areas. The Government reiterated its political commitment to reduce workers from 22 to 39 per 10 000, and (within this number) doc-
maternal and newborn mortality at the 2014 World Health tors/nurses/midwives from 7 to 13. It planned an almost doubling of
Assembly through endorsement of the ENAP and the National the number of 119 951 public health staff.278 Health Policy and Planning, 2018, Vol. 33, No. 2
Table 4. Cause-specific deaths in children under one month of age by 2020 with scaling of essential interventions, as modeled by the LiST
2015 2016 2017 2018 2019 2020
Neonatal asphyxia 10 228 9918 9623 9343 7436 7056
Neonatal prematurity 10 035 9394 8796 8237 7177 6669
Neonatal sepsis 6912 6330 5796 5304 4733 4315
Neonatal other 2435 2429 2426 2426 2427 2430
Neonatal congenital anomalies 2064 2042 2022 2005 1988 1973
Neonatal pneumonia 2232 2110 1996 1888 1785 1688
Neonatal tetanus 1201 1038 885 741 591 465
Neonatal diarrhea 542 498 456 417 379 344
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
A clear plan is needed to deliver basic essential newborn care in absenteeism and service providers’ attitudes towards health seekers
the facilities that do not presently have skilled birth attendants. can be major deterrents.
However, there have been improvements in the availability of skilled As the health sector looks to expand coverage and demand for
birth attendants due to investment in community midwifery MNCH services, quality of care is central to attracting clients and
(Mohmand 2013). Between 2003 and 2012, the number of grad- for improved health outcomes (Montgomery et al. 2014). However,
uated midwives in Afghanistan increased from 467 to 3001 (MoPH by way of example, the cesarean section rate is low in Afghanistan
[undated]). Two studies have emphasized the competency of these (1.1% of births) due to lack of related skills and equipment (Jhpiego
midwives (Partamin et al. 2012; Kim et al. 2013), and another noted 2010). A high percentage of intrapartum stillbirths of normal
that community selection of trainees significantly elevated the pres- birthweight also suggest a need for improved labor monitoring
ence of trained midwives in high-risk rural communities, without and surgical obstetric practices, and use of facility-based perinatal
compromising skills (Mansoor et al. 2011). However, another surveillance and audit to guide quality assurance initiatives
study found that lack of equipment and training for such staff (Kandasamy et al. 2009).
compromise intrapartum care, affecting newborn outcomes The working environment at health facilities and hospitals
(Guidotti et al. 2009). directly affects care provided. A recent Kabul hospital study revealed
Competency-based pre- and in-service training, complemented heavy workloads, a high proportion of complicated cases and poor
staff organization affecting the quality of care, and that cultural
by supportive supervision, can build providers’ capacity, including
values, social and family pressures influenced the motivation and
for newborn resuscitation and other signal functions (Kim et al.
priorities of healthcare providers (Arnold et al. 2015). Moreover,
2013; Gabrysch et al. 2012) but remains a neglected area in
nepotism and cronyism affected clinical training, undermined the
Afghanistan. Each year universities and health institutions graduate
authority of management to improve standards of care and created
doctors and allied health workers with poor competencies.
an atmosphere of vulnerability for those without influential backers.
In Afghanistan, CHWs introduced in 2002 are volunteer village-
In contrast, an approach piloted in Kunduz and Balkh provinces and
based health workers supported by the MoPH to provide basic
in Kabul showed that measurable improvements in patient care can
health education and simple medical treatment to community mem-
be improved while systematically building the capacity of the health
bers. More than 28 000 CHWs have been trained and deployed in
system, through national leadership and policy making (Rahimzai
>11 000 health posts in all 34 provinces, especially in rural areas
et al. 2014). Afghanistan’s ongoing conflict and its unpredictability
where a majority (71%) of Afghanistan’s population resides
in some areas of the country also affects health service delivery,
(CSO 2014). A qualitative study on the national CHW program in
particularly for women accessing care during labor. The impact of
Afghanistan (Najafizada et al. 2014) found that female CHWs
insecurity on service continuity is most likely underreported in
accomplished their tasks vis-à-vis MNCH with greater ease than
Afghanistan (Rubenstein and Bittle 2010).
male CHWs, as societal gender dynamics influenced task allocation. Outreach services in Afghanistan’s so-called ‘white areas’ with
It noted that while volunteerism helps to deploy a larger number of no access to fixed facilities are conducted by several cadres of health
CHWs, it also makes retention difficult. workers, including community midwives and members of mobile
Finally, continuous work is needed to attract and retain skilled health teams. An evaluation in 11 provinces of mobile health
female health workers. Insecurity and traditional attitudes to gender teams covering locations geographically far from health facilities
in Afghanistan require a multisectoral response and innovative concluded positive impacts in almost all the primary care indicators
strategies to reduce their impact. Within the health sector, midwife monitored in Afghanistan MoPH (2011). These included consulta-
career advancement also impacts retention and requires attention tions, maternal health and immunization.
(Wood et al. 2013). In another small study using direct clinical observation, all time
intervals with the exception of ‘decision to skin incision’ were longer
Health service delivery in the record reviews than in observed cases. It was also found that
Although overall access to MNCH services has improved in recent prior cesarean was the most common primary indication for all
years, and some studies suggest pro-poor distribution of health cases. Among newborns there were two stillbirths (7%) in observed
care (Steinhardt et al. 2008), the urban-rural differential remains a births and seven (21%) in the record reviews (Evans et al. 2014).
problem in Afghanistan, and equity-focused strategies are required.
In particular, it is difficult for women in rural areas to access ANC Logistics, and essential medical products and technologies
and skilled maternity care, as described already (Afghan Public General deficiencies exist in Afghanistan’s pharmaceutical sub-
Health Institute 2011). Perceived poor quality of services, sector, in terms of implementation of policy, regulation andHealth Policy and Planning, 2018, Vol. 33, No. 2 279
management. In general, the accessibility, affordability and avail- symptoms of obstetric complications and the associated urgency
ability of quality medicines varies widely by province (Harper and (Hirose et al. 2015).
Strote 2012; Kohler et al. 2012) and Afghanistan is considered a Demand side barriers at community level remain significant
chaotic and unregulated market (Paterson and Karimi 2005). As a obstacles to improved newborn health. There is limited understand-
consequence, the pharmaceutical market and supply system are ing of the importance of ANC and a lack of family support, funds
flooded with substandard, counterfeit, and diverted medicines which and transportation lead to underuse of available care, especially by
affect all population groups, particularly vulnerable newborns. poorly educated rural women (Rahmani and Brekke 2013).
Work is ongoing for greater regulation and to develop local produc- Financial barriers and social norms are the most frequently men-
tion (MoPH 2014); however, interim measures, especially to tioned; relative wealth is the most important determinant in seeking
increase the availability and affordability of essential drugs are care outside the home, and in choice of provider (Mayhew et al.
needed. 2008; Steinhardt et al. 2008). The husband’s social network influ-
Gaps were present in the availability of several essential drugs spe- enced delays in care-seeking during labor in one study of women
cific to newborn care at the time of a nation-wide needs assessment who give birth at health facilities (Hirose et al. 2015). Several
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
(Jhpiego 2010). The most common cause of delay in the delivery of community-level factors and perceptions have been found to
supplies overall was reported as administrative difficulties (27%) and increase the number of institutional deliveries, including intensive
inadequate transport (21%). community mobilization, provision of free services and transport
facilities at night, maintaining privacy in the delivery room and the
Health information systems quality of services (Hadi et al. 2007). Fee removal appeared to be an
Major investments have supported the development of Afghanistan’s influential factor to increase demand (Steinhardt et al. 2011).
Health Management Information System (HMIS) in which a sub-set Community participation facilitated the tasks of CHWs, but also
of indicators is collected for newborn health (MoPH 2015). posed challenges, such as traditional leaders influencing the recruit-
Strengthening of monitoring systems and a culture of data use ment of CHWs who may not be the most appropriate candidate for
through HMIS at community, facility and district levels is a critical community health promotion (Najafizada et al. 2014). The MoPH
need for improving the quality of care. Options being considered is introducing a new community-based package for newborn care
include real-time monitoring of results and establishing accountabil- that emphasizes the importance of home visits for mothers and new-
ity mechanisms for health facilities and provincial health depart- borns to promote healthy behaviors and identify danger signs.
ments. RMNCH Scorecards were launched mid-2015, and include
indicators relevant to newborn care such as skilled birth attendance,
low birth weight etc. (MoPH 2015). The Scorecards monitor district, Discussion
provincial and national progress and performance by quarter, and Despite ongoing insecurity, Afghanistan is making progress in some
preliminary results show they are effective tool in identifying areas areas of newborn care; for this progress to be reflected in improved
(geographic and programmatic) requiring more attention, and for health outcomes for newborns, it is necessary to examine and address
proxy measurements on quality of care. The Scorecards and other bottlenecks to newborn care and implement strategies for scaling up.
routine monitoring can improve awareness of standardized norms Using the bottleneck analysis for newborn care to accelerate scale-up
and practices, and identify the magnitude and nature of bottlenecks (Dickson et al. 2014) initially introduced in Afghanistan in 2013, the
to newborn health (Singh et al. 2013). following areas should be prioritized to improve newborn health
A ‘balanced scorecard’ approach is being used to assess and outcomes and reduce mortality in Afghanistan.
improve health service capacity and service delivery using perform- To improve proximity to health facilities, especially in rural
ance benchmarking in Afghanistan. According to a study reviewing areas of Afghanistan, a recent study indicates a need to re-examine
performance over 5 years, reconfigurations are needed to integrate criteria for selecting and positioning basic and emergency obstetric
effectiveness and efficiency measures and accommodate changes in and newborn care services at appropriate levels of the healthcare
health systems policy and strategy architecture, though it is unclear system, connected by appropriate communication and functional
how performance was rated for newborn health (Edward et al. referral mechanisms (Kim et al. 2012).
2011). More recently, the MoPH has instituted a third party moni- Policy, implementation and oversight mechanisms must be
toring mechanism to verify implementation of basic health services strengthened to eliminate unofficial payments and reduce of out-of-
across the country, including maternity services and newborn care pocket expenditures for improved neonatal health outcomes.
(MoPH 2015). Strengthening governance closer to delivery of health services could
have positive implications not only for better use of resources but
Community ownership and participation also for improved community perceptions.
Although not one of WHO’s six health system building blocks, this Improvements in quality of neonatal care are also directly linked
is a critical aspect of health system functioning, especially in low- to improving supervision. Supportive supervision systems in the
income countries where access is a major limiting factor in health health system in Afghanistan can help to ensure that providers pos-
sector performance. sess the knowledge, skills, and attitudes required to provide quality
In Afghanistan, community-level influences exist on the demand EmONC services (Kim et al. 2012). For midwives, in-service train-
for maternity and newborn services. Newborn and infant mortality ing and job rotation could help skilled birth attendants retain their
rates are higher among the poorest quintile, and cultural restrictions skills, especially in managing common high-risk emergencies
on the mobility and decision-making capacity of women are signifi- (Partamin et al. 2012; Turkmani et al. 2015).
cant constraints to them accessing maternity care. The practice of Notwithstanding, midwives’ contribution in Afghanistan ranges
purdah, or seclusion of women, makes it difficult for them to obtain from increased newborn care to changing community perceptions of
social and health services including MNH (Mansoor et al. 2011). women’s education and professional independence, which must con-
Rural and poor populations have low awareness of the signs and tinue to be reinforced (Turkmani et al. 2013). Advocacy to280 Health Policy and Planning, 2018, Vol. 33, No. 2
encourage family and community support for midwives working in Acknowledgements
rural facilities and providing benefits such as housing, education for The authors would like to specially thank Alyssa Sharkey and Deepika
their children, and employment for the accompanying male family Attygalle (UNICEF Regional Office for South Asia) and Karen Edmond
member are measures likely to improve midwife retention in (UNICEF Afghanistan), for their valuable inputs, as well as Danzhen You and
Afghanistan (Mansoor et al. 2013). Lucia Hug (UNICEF Headquarters, Division of Data, Research and Policy)
Mortality associated with cesarean section may be partly due to for guidance and support on mortality estimates and reduction rates. The
women coming late for obstetric care; however, increasing availabil- authors would like to also thank colleagues and collaborators in the Ministry
of Public Health, UNICEF and other UN agencies, USAID and all develop-
ity and utilization of cesarean section requires focus on quality, such
ment partners working on the issue of newborn health in Afghanistan.
as encouraging use of partographs and improving decision-making
and documentation around cesarean section deliveries (Kim et al. Conflict of interest statement. None declared.
2012). A high percentage of intrapartum stillbirths among normal
birth weight fetuses suggests a need for improved labor monitoring
References
and surgical obstetric practices. A study concluded that the use of a
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
facility-based perinatal surveillance system is critical in guiding such Adegboye, OA. Danelle, K. 2014. Causes and patterns of morbidity and mor-
tality in Afghanistan: joint estimation of multiple causes in the neonatal
quality assurance initiatives (Kandasamy et al. 2009).
period. Canadian Studies in Population 41:165–79.
To link postnatal counseling to family planning, currently a
Afghan Public Health I. Ministry of Public Health, Central Statistics
weak area, one study underscored the importance of providing pri- Organization, ICF Macro, Indian Institute of Health Management Research,
vate spaces for postpartum family planning (counseling, along with and World Health Organization Regional Office for the Eastern
involving husbands and mothers-in-law in counseling). Private Mediterranean (WHO/EMRO). 2011. Afghanistan Mortality Survey 2010.
spaces can increase the percentage of women receiving this counsel- Calverton, MD: APHI/MoPH, CSO, ICF Macro, IIHMR and WHO/EMRO.
ing and, importantly, their preferred contraceptive method before Afghanistan Ministry of Economy. Islamic Republic of Afghanistan
discharge (Tawfik et al. 2014). Millennium Development Goals Report 2013.
Afghanistan Ministry of Public Health. [undated]. National Reproductive
Though the situation has improved, there are many urgent oppor-
Health Strategy (2012–2016). Kabul: Ministry of Public Health.
tunities for reducing the number of newborn deaths in Afghanistan.
Afghanistan Ministry of Public Health. 2011. Report on Evaluation of Mobile
Newborn mortality is related to complex factors; a weak health sys- Health Teams in Afghanistan. Kabul: Ministry of Public Health.
tem associated with decades of conflict, low and uneven coverage of Afghanistan Ministry of Public Health. 2013. Afghanistan National Health
essential interventions, demand-side and cultural specificities, and Accounts with Subaccounts for Reproductive Health 2011-2012. Kabul:
compromised quality. With a majority of deliveries still taking place Ministry of Public Health.
at home, birth asphyxia, low birth weight, perinatal disorders and Afghanistan Ministry of Public Health. 2014. Economic Evaluation of the
Potential for Local Pharmaceutical Production in Afghanistan. Kabul:
infections are causing many preventable newborn deaths.
Ministry of Public Health.
A long-term vision and strong leadership are essential for the
Afghanistan Ministry of Public Health. 2015. Health Information
MoPH to play an effective stewardship role in formulating policy, Management System (HMIS) Newsletter. Kabul: Ministry of Public Health.
strategy and setting standards to regulate and monitor MNCH serv- http://moph.gov.af/Content/Media/Documents/HMISNewsletter61220141
ices and promotion of equitable access, including through health 0427582553325325.pdf.
workforce planning, development and management. To achieve Afghanistan Ministry of Public Health. 2015. Correspondence with Director
these aims, the MoPH must build on and upgrade existing systems of Reproductive Health, Ministry of Public Health.
for health service delivery and performance monitoring, as well as Afghanistan Ministry of Public Health. National Human Resources for Health
(HRH) Consultative Forum Secretariat 2011. Afghanistan National Health
further leverage global initiatives and partnerships for technical and
Workforce Plan 2012-16.
financial resources. Afghanistan Ministry of Public Health, Aga Khan University, United Nations
Particular attention is required to strengthening access to and use Children’s Emergency Fund (UNICEF). 2013. National Nutrition Survey.
of intrapartum services and comprehensive newborn care. A shift is Kabul: Ministry of Public Health.
required from the traditional facility-based health service delivery Afghanistan Ministry of Public Health, United Nations Children’s Emergency
model to a demand-driven model that includes community-level Fund (UNICEF). 2013. National Immunization Coverage Evaluation
care, awareness-raising, risk sensitization and women’s empower- Survey. Kabul: Ministry of Public Health.
Afghanistan Ministry of Public Health, United Nations Children’s Emergency
ment for decision-making.
Fund (UNICEF), USAID. 2015. Reproductive, Maternal, Newborn and
Attention must also be paid to cross-sectoral areas such as sani-
Child Health ScorecardQ3 1393. Kabul: Ministry of Public Health.
tation and girls’ education, to improve rates of health-promoting Ameli O, Newbrander W. 2008. Contracting for health services: effects of uti-
behaviors and practices and address root causes of maternal and lization and quality on the costs of the Basic Package of Health Services in
child mortality and morbidity. Afghanistan. Bulletin World Health Organisation 86: 920.
Anwari Z, Shukla M, Maseed BA. et al. 2015. Implementing people-centred
health systems governance in 3 provinces and 11 districts of Afghanistan: a
Supplementary data case study. Conflict and Health 9: 2.
Arnold R, van Teijlingen E, Ryan K, Holloway I. 2015. Understanding Afghan
Supplementary data are available at Health Policy and Planning online. healthcare providers: a qualitative study of the culture of care in a Kabul
maternity hospital. Bjog 122: 260–7.
Note Asia Foundation. 2016. A Survey of the Afghan People: Afghanistan in 2016.
http://asiafoundation.org/wp-content/uploads/2016/12/2016_Survey-of-
1. These interventions include: labor and delivery management,
the-Afghan-People_full-survey.Jan2017.pdf.
full supportive care for prematurity, clean postnatal practices, Bhutta Z, Das JK, Bahl R. et al. 2014. Can available interventions end prevent-
clean birth practices, chlorhexidine, immediate assessment and able deaths in mothers, newborn babies, and stillbirths, and at what cost?
stimulation and thermal care. The Lancet 384: 9940.Health Policy and Planning, 2018, Vol. 33, No. 2 281
Boschi-Pinto C, Young M, Black RE. 2010. The child health epidemiology Kohler JC, Pavignani E, Michael M. et al. 2012. An examination of pharma-
reference group reviews of the effectiveness of interventions to reduce mater- ceutical systems in severely disrupted countries. BMC International Health
nal, neonatal and child mortality. International Journal of Epidemiology and Human Rights 12: 34.
39: i3–6. Kim YM, Ansari N, Kols A. et al. 2013. Assessing the capacity for newborn
C. Statistics Organisation (CSO). 2014. National Risk and Vulnerability resuscitation and factors associated with providers’ knowledge and skills: a
Assessment 2011-12. Afghanistan Living Conditions Survey. Kabul: CSO. cross-sectional study in Afghanistan. BMC Pediatrics 13: 140.
C. Statistics Organisation (CSO), United Nations Children’s Emergency Fund Kim Y-M, Tappis H, Zainullah P. et al. 2012. Quality of caesarean delivery
(UNICEF). 2012. Afghanistan Multiple Indicator Cluster Survey 2010-11. services and documentation in first-line referral facilities in Afghanistan: a
Kabul: CSO and UNICEF. chart review. BMC Pregnancy and Childbirth 12: 14.
Cockcroft A, Khan A, Ansari NM. 2011. Does contracting of health care in Kim YM, Zainullah P, Mungia J. et al. 2012. Availability and quality of emer-
Afghanistan work? Public and service users’ perceptions and experience. gency obstetric and neonatal care services in Afghanistan. International
BMC Health Services Research 11: S11. Journal of Gynecology and Obstetrics 116: 192–6.
Countdown for Maternal, Newborn and Child Health (MNCH). 2014. Knippenberg R, Lawn JE, Darmstadt GL. et al. 2005. Systematic scaling up of
Fulfilling the Health Agenda for Women and Children: Afghanistan Profile neonatal care in countries. The Lancet 365: e1087–98.
2014 Report. http://www.countdown2015mnch.org/documents/2014Report/ Lawn JE, Cousens S, Zupan J. 2005. 4 million neonatal deaths: When?
Downloaded from https://academic.oup.com/heapol/article/33/2/271/4668760 by guest on 04 November 2020
Afghanistan_Country_Profile_2014.pdf. Where? Why? The Lancet 365: 891–900.
Darmstadt GL, Bhutta ZA, Cousens S. et al. 2005. Evidence-based, Lawn JE, Kinney MV, Black RE. et al. 2012. Newborn survival: a
cost-effective interventions: how many newborn babies can we save? The multi-country analysis of a decade of change. Health Policy and Planning
Lancet 365: 977–88. 27(Suppl 3): iii6–28.
Dalil S, Newbrander W, Loevinsohn B. et al. 2014. Aid effectiveness in rebuild- Lin A, Salehi AS. 2013. Stimulating demand: effects of a conditional cash
ing the Afghan health system: a reflection. Global Public Health 9: S124–36. transfer programme on increasing maternal and child health-service utilisa-
Dickson KD, Simen Kapeu A, Kinney MV. et al. 2014. Every newborn: tion in Afghanistan, a quasi-experimental study. Lancet 381: S84.
health-systems bottlenecks and strategies to accelerate scale-up in countries. Liu L, Oza S, Hogan D, Perin J. et al. 2015. 2015. Global, regional, and
national causes of child mortality in 2000–13, with projections to inform
The Lancet 384: 438–54.
post-2015 priorities: an updated systematic analysis. Lancet 385: 430–40.
Edward A, Kumar B, Kakar F. et al. 2011. Configuring balanced scorecards
Mansoor GF, Hashemy P, Gohar F. et al. 2013. Midwifery retention and cov-
for measuring health system performance: evidence from 5 years’ evaluation
erage and impact on service utilisation in Afghanistan. Midwifery 29:
in Afghanistan. PloS Medicine 8: e1001066.
1088–94.
Evans, CL Kim, YM Yari, K Ansari, N Tappis, H. 2014. Using direct clinical
Mansoor GF, Hill PS, Barss P. 2011. Midwifery training in post-conflict
observation to assess the quality of cesarean delivery in Afghanistan: an
Afghanistan: tensions between educational standards and rural community
exploratory study. BMC Pregnancy and Childbirth 14: 176.
needs. Health Policy and Planning 27: 60–8.
Frost A, Wilkinson M, Boyle P, Patel P, Sullivan R. 2016. An assessment of the
Mason E, McDougall L, Lawn JE. et al. 2014. From evidence to action to
barriers to accessing the Basic Package of Health Services (BPHS) in
deliver a healthy start for the next generation. The Lancet 384: 455–67.
Afghanistan: was the BPHS a success? Globalization and Health 12: 71.
Mayhew M, Hansen PM, Peters DH. et al. 2008. Determinants of skilled birth
Gabrysch S, Civitelli G, Edmond KM. et al. 2012. New signal functions to
attendant utilization in Afghanistan: a cross-sectional study. American
measure the ability of health facilities to provide routine and emergency
Journal of Public Health 98: 1849–56.
newborn care. PLoS Medicine 9: e1001340.
Mohmand KA. 2013. Community Midwifery Education Program in
Guidotti RJ, Kandasamy T, Betrán AP. et al. 2009. Monitoring perinatal out-
Afghanistan. Washington, DC: World Bank.
comes in hospitals in Kabul, Afghanistan: The first step of a quality assurance
Montgomery AL, Fadel S, Kumar R, Bondy S, Moineddin R, Jha P. 2014. The
process. The Journal of Maternal-Fetal and Neonatal Medicine 22: 285–292.
effect of health facility admission and skilled birth attendant coverage on
Hadi A, Rahman T, Khuram D, Ahmed D, Alam A. 2007. A. Raising institu-
maternal survival in India: a case-control analysis. PLOS One 9: e95696.
tional delivery in war-torn communities: experience of BRAC in
Musinguzi LK, Turinawe EB, Rwemisisi JT. et al. 2017. Linking communities
Afghanistan. Asia Pacific Journal of Family Medicine 6: 1.
to formal health care providers through village health teams in rural Uganda:
Hirose A, Borchert M, Cox J. et al. 2015. Determinants of delays in travelling
lessons from linking social capital. Human Resources for Health 15: 4.
to an emergency obstetric care facility in Herat, Afghanistan: an analysis of Najafizada SAM, Labonté R, Bourgeault IL. 2014. Community health workers
cross-sectional survey data and spatial modelling. BMC Pregnancy and of Afghanistan: a qualitative study of a national program. Conflict and
Childbirth 15: 14. Health 8: 26.
Haidari AM, Zaidi S, Gul R. 2014. Prospects for the sustainability of deliver- Oestergaard MZ, Inoue M, Yoshida S. et al. 2011. Neonatal mortality levels
ing the Basic Package of Health Services in Afghanistan: a stakeholder anal- for 193 countries in 2009 with trends since 1990: a systematic analysis of
ysis. Eastern Mediterranean Health Journal 20: 5. progress, projections, and priorities. PLoS Medicine 8: e1001080.
Haider S, Todd C, Ahmadzai M. et al. 2009. Childbearing and contraceptive Partamin Kim YM, Mungia J. et al. 2012. Patterns in training, knowledge, and
decision making amongst afghan men and women: a qualitative analysis. performance of skilled birth attendants providing emergency obstetric and
Health Care for Women International 30: 935–53. newborn care in Afghanistan. International Journal of Gynecology and
Harper J, Strote G. 2011. Afghanistan pharmaceutical sector development: Obstetrics 119: 125–29.
problems and prospects. Southern Med Review 4: 29–39. Partnership for Maternal, Newborn and Maternal Health (PMNCH). 2011. A
Huber D, Saeedi N, Samadi AK. 2010. Achieving success with family planning Global Review of the Key Interventions Related to Reproductive, Maternal,
in rural Afghanistan. Bulletin World Health Organisation 88: 227. Newborn and Child Health (RMNCH). Geneva: The Partnership for
Jhpiego, Afghanistan Ministry of Public Health, United Nations Children’s Maternal, Newborn & Child Health.
Emergency Fund (UNICEF). 2010. Emergency Obstetric and Neonatal Paterson A, Karimi A. 2005. Understanding Markets in Afghanistan: A Study of the
Care (EmONC) Needs Assessment. Kabul: Jhpiego. Market for Pharmaceuticals. Kabul: Afghanistan Research and Evaluation Unit.
John Hopkins University (JHU), Indian Institute of Health Management Rahimzai M, Naeem AJ, Holschneider S, Hekmati AK. 2014. Engaging front-
Research (IIHMR). 2012. Afghanistan Health Survey. line health providers in improving the quality of health care using
Kandasamy T, Merialdi M, Guidotti RJ. et al. 2009. Cesarean delivery surveil- facility-based improvement collaboratives in Afghanistan: case study.
lance system at a maternity hospital in Kabul, Afghanistan. International Conflict and Health 8: 21.
Journal of Gynecology and Obstetrics 104: 14–7. Rahmani AM, Wade B, Riley W. 2013. Evaluating the impact a proposed fam-
Kerber K, de Graft-Johnson JE, Bhutta ZA. et al. 2007. Continuum of care for ily planning model would have on maternal and infant mortality in
maternal, newborn, and child health: from slogan to service delivery. The Afghanistan. The International Journal of Health Planning and
Lancet 370: 1358–69. Management 30: 71–85.You can also read