SENTICOL III International validation study of sentinel node biopsy in early cervical cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

SENTICOL III
International validation study of sentinel node biopsy
in early cervical cancer
INVESTIGATORS MEETING_FRANCE
17th MAY 2019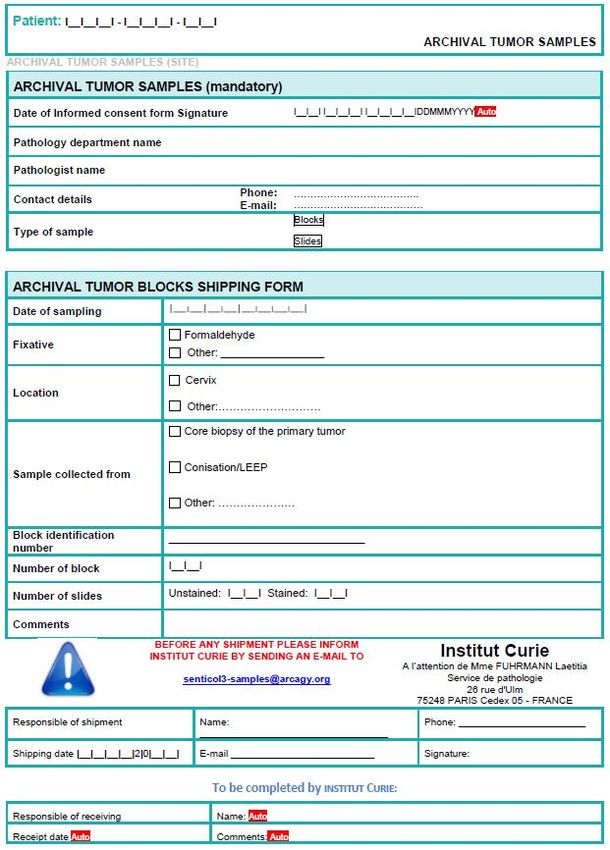
SENTICOL III
ID-RCB: 2017-A00945-48
Sponsor: Centre Hospitalier Universitaire de Besançon
2 place Saint-Jacques 25030 Besançon Cedex
FRANCE
Pr Fabrice LECURU
Hôpital Européen Georges Pompidou
COORDINATING INVESTIGATOR
Phone: +33 (0)1 56 09 35 84
Email: fabrice.lecuru@aphp.fr
Dr Amélie ANOTA
STUDY BIOSTATISTICIANS CHU de Besançon
Phone: +33 (0)3 70 63 21 72
Email: aanota@chu-besancon.fr
Marie-Aude LE FRERE BELDA
PATHOLOGIST Hôpital Européen Georges Pompidou
Phone: +33 (0)1 56 09 35 84
Email: marie-aude.le-frere-belda@aphp.fr
Rachida MAMA ABDOU (international project manager)
Sandra MABALUKIDI (CTA)
TRIAL MANAGEMENT COORDINATING CENTER
ARCAGY-GINECO
AND PHARMACOVIGILANCE
Phone: +33 (0)1 84 85 20 20
E-mail: senticol3-study@arcagy.org
Pharmacovigilance: pharmacovigilance@arcagy.org
Kristina MOUYABI (project manager)
Aude Le Breton(CRA) / Caroline CARETTE (CRA)
MONITORING CHU de Besançon
AND CONTRACTS FEES Phone: + 33 (0)3 81 21 83 56
E-mail: kmouyabi@chu-besancon.fr
a1lebreton@chu-besancon.fr/ ccarette@chu-besancon.fr
2
AGENDA
ITEMS WHO
Standard of care and rationale Pr Lecuru
SLN and nSLN (mapping and biopy) Pr Lecuru
Protocol overview Pr Lecuru and Rachida
Translational research Pr Lecuru
Communication and Timelines Rachida
Study tools and monitoring Rachida and Kristina
3 ARCAGY - GINECO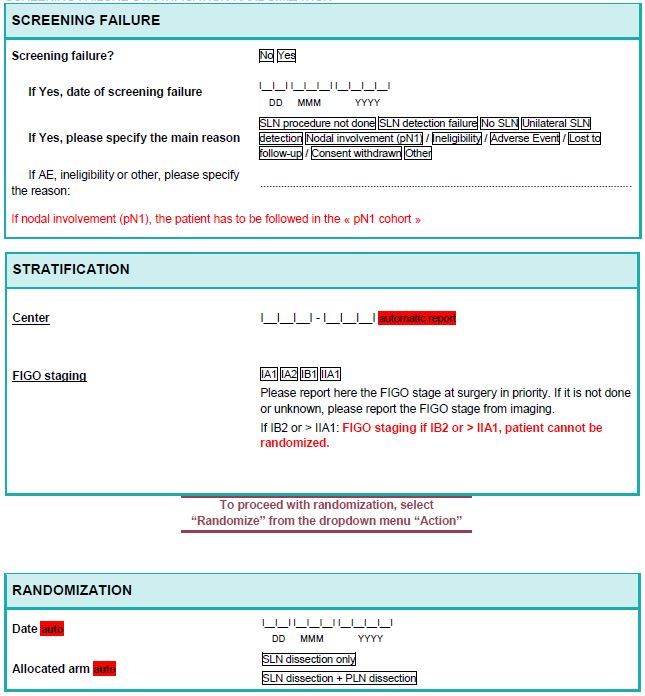
STANDARD OF CARE AND RATIONALE
4 ARCAGY - GINECO
STUDY RATIONALE (1/2)
❖ Cervical cancer: 2nd cause of cancer death in women worldwide. Incidence:
527600/year, mortality: 265700/year.
❖ Prognosis of early stage cervical cancers relatively good, especially in patients
without risk-factors and in the absence of nodal disease. FIGO 2009 meeting: 5
years OS > 97 % for stage Ia2 and > 91% for stage Ib1.
❖ Standard of care to assess nodal involvement in early stage cervical cancer is
lymphadenectomy. However:
➢ A minority of patient presents with nodal metastasis at this stage,
➢ The number of involved nodes is small in case of nodal spread,
➢ Tumor deposits’ size small
➢ Per and post operative complications of nodal dissection reported in 0 to 58 % of cases:
bleeding and injuries during surgery, lymphocysts, lymphedema….
5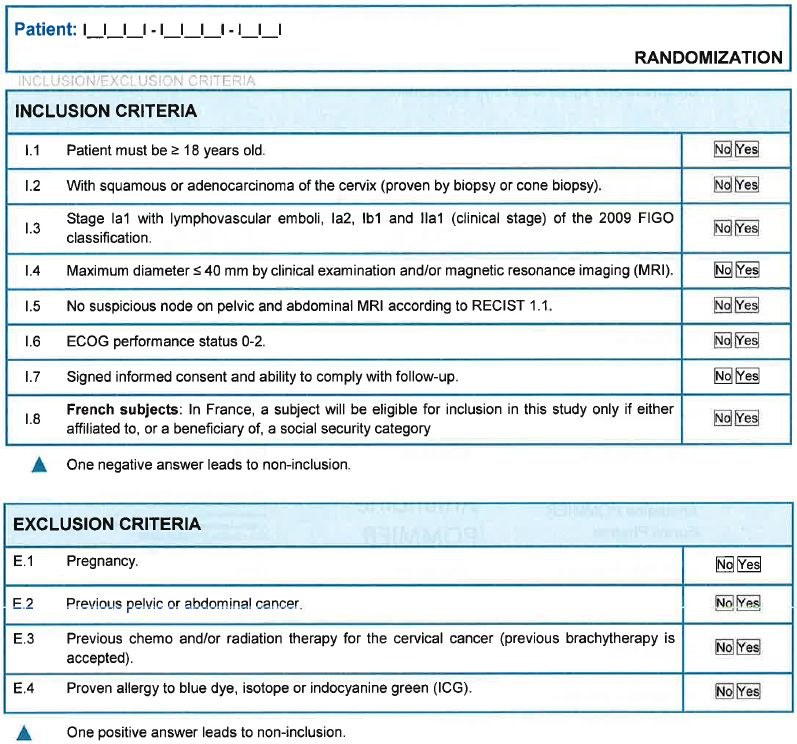
STUDY RATIONALE (2/2)
❖ Sentinel lymph node (SLN) mapping: technique introduced in the management of
gynaecologic malignancies for nearly 20 years. It aims to maintain survival and
improve quality of life in good prognosis patients by surgery de-escalation
❖ SLN biopsy also provides additional information compared with routine pelvic
dissection:
➢ Diagnosis of low volume metastasis,
➢ SLN can be found in « unexpected » areas, outside of the classical lymphadenectomy
territories.
❖ Despite these data, SLN biopsy is not a standard of care in most guidelines.
❖ Missing data: Survival! No study demonstrated that patients assessed with SLN
biopsy have the same prognosis than after a classical pelvic dissection.
Outcomes of patients after SLN biopsy vs SLN biopsy
+ pelvic dissection must be compared!
6
SENTICOL IIII STUDY DESIGN
An international, prospective, randomized, multicenter, single blind trial to
compare sentinel lymph node (SLN) biopsy versus SLN biopsy + pelvic
lymphadenectomy in term of DFS and HR-QoL.
7
STUDY DESIGN
•Squamous or adenocarcinoma of the cervix,
•Stage Ia1 with lympho vascular emboli , Ia2, Ib1, Ib2, IIa1 (FIGO
2018)
•Maximum diameter ≤ 40mm.
Randomization
Patients with bilateral detection without
macroscopic suspicious node and negative frozen Patients with nodal involvement
section on SLN (pN1)
(pN0)
Randomisation
1 : 1
Arm A (experimental) : Arm B (reference) :
SLN biopsy only SLN biopsy
+ hysterectomy or trachelectomy + Pelvic Lymphadenectomy
+ hysterectomy or
trachelectomy
DFS, RFS, QOL, OS Followed in a separate cohort to
record treatment and outcomes
8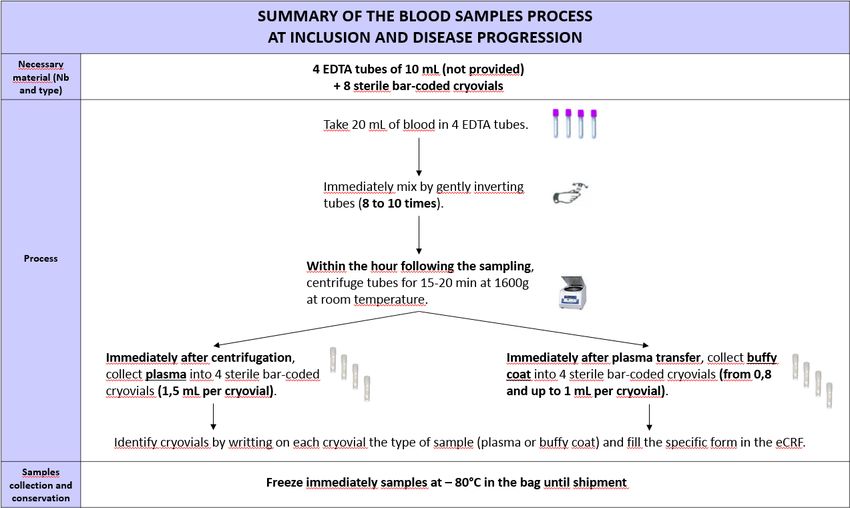
SENTINEL LYMPH NODE (SLN) and
NON SENTINEL LYMPH NODE (nSLN)
9 ARCAGY - GINECO
1) Pre-randomization assessment (SLN mapping and biopsy):
➢ SLN Mapping
Planar lympho-scintigraphy
or SPECT/CT -> number General anesthesia,
Pelvic examination -> clinical
and location of SLN laparotomy or laparoscopic
stage verification
according to the Marnitz or robotic access
classification
SLN biopsy -> pathological
examination Collection of a paraffin
Intracervical injection of blue embedded sample
dye or ICG nSLN sample (only for
patients in arm B)->
translationnal research
101) Pre-randomization assessment (SLN mapping and biopsy):
➢ Techniques of SLN detection:
❖ In case of isotope alone
➢ The surgical access will be obtained by laparoscopy, laparotomy or robotically assisted laparoscopy
➢ Correlation performed with the result of the lympho-scintigraphy
Number, location according to Marnitz classification, and intensity are noted on a schema
➢ The “hot” nodes are biopsied.
Pelvic nodes: no more than 5 SLN/side should be harvested. If numerous per-operative SLN, the lymphoscintigram
could help to limit the harvest to first echelon SLN only.
➢ SLN given to the pathologist for frozen section
❖ In case of blue dye (associated with isotope) or in case of ICG (alone or in association with
isotope)
➢ Dye injected into the cervix under anaesthesia at the beginning of the operation or after set-up of the endoscopic
access
➢ The progression of the dye under the peritoneum is followed to localize the first labelled nodes
Number, location according to Marnitz classification, and intensity are noted on a schema
➢ The “hot” and/or “colored nodes” are biopsied by a specific incision. Only the first echelon nodes should be harvested
(and no more than 5 SLN/pelvic side)
➢ SLN given to the pathologist for frozen section
111) Pre-randomization assessment (SLN mapping and biopsy):
➢ Techniques of surgical SLN biopsy:
❖ MSKCC algorithm
➢ All the mapped nodes must be harvested,
➢ All suspicious node must be removed,
➢ In case of unilateral pelvic detection, perform a lymphadenectomy. These patients will not be
randomized.
➢ Inspection of the nodal areas during the radical hysterectomy (especially parametria).
12TUTORIAL
132) Pathology of SLN and nSLN (non-sentinel lymphnode):
One part examined in FS in
. one level after staining with
HES
SLNs cut in half along
their long axis Histological examination
performed after staining
One part immediately fixed with HES
for definitive examination on
sections of 200 microns Negative SLNs with HES
-> IHC with anti-
cytokeratine AE1-AE3
❖ nSLN sectioned once and examined after staining with HES. Histological analyses carried out
systematically in the same center by the same pathologist referent for SLN biopsy.
❖ The isolated tumour cells are defined as 2 mm
14AMENDEMENT AU PROTOCOLE
Definitive examination and ultrastaging
Each SLN (if nonmetastatic with frozen section) tissue blocks should be further examined by an ultrastaging
protocol consisting of five step sections spaced at 200-250 µm intervals with four sections stained with HES
and one section used for immunohistochemistry with pancytokeratin antibodies (e.g. AE1/AE3).
AE1/
HES HES AE3 HES HES
200-250 200-250 200-250 200-250
microns microns microns microns
Non-sentinel lymph nodes will be sectioned once and examined after staining with HES.
15AMENDEMENT AU PROTOCOLE
Protocol for collection of SLN and nSLN for translational research:
Before cutting specimens of each new patient, the blade must be
cleaned with an alcoholic solution and moved in order to avoid any
potential contamination
Then, proceed as follows:
- Cut 5 sections of 10 µm thick on each sentinel lymph node and store
it in a tube at room temperature
- Cut 10 sections of 10 µm thick of the cervix tumour biopsy and store it
in a tube at room temperature with one HES stained slide
16PROTOCOL OVERVIEW
17STUDY OBJECTIVES (1/2)
1) Co-Primary Objectives and associated endpoints:
Objective Outcome measure
To assess that Disease Free Survival Disease free survival (DFS) is defined as the time
(DFS) is similar between pN0 patients interval between randomization and physical or
after SLN biopsy versus SLN biopsy + radiographic evidence of recurrence (local/
PLN distant) or second cancer or death (all causes)
whichever occur first
To assess a superiority of SLN biopsy HR-QoL of patients assessed with EORTC QLQC 30
for quality of life (HR-QoL) and QLQ-CX24 with 3 targeted dimensions: pain,
global health score and physical functioning
scores at 3 years.
18STUDY OBJECTIVES (2/2)
2) Secondary Objectives:
❖ Outcome of pN1 patients according to the size of metastasis and treatment
(isolated tumor cells and micrometastasis)
❖ Evaluation of mapping with indocyanine green (ICG)
❖ Surgical morbidity and mortality
❖ Other dimensions of HR-QoL (QLQ-C30 and QLQ-CX24) at three years and
longitudinal analysis of all HR-QoL dimensions
❖ Positive and negative predictive values of SLN biopsies
❖ Overall survival (OS)
❖ Recurrence free survival (RFS)
❖ A cost analysis will be performed in France
❖ Lymphatic and lower limb complications, LEL screening questionnaire
19STUDY POPULATION (1/2)
1) Inclusion criteria:
Patient must meet ALL of the following criteria to be eligible for inclusion in
this study
❖ I 1. Patient must be ≥ 18 years old,
❖ I 2. With squamous or adenocarcinoma of the cervix (proven by biopsy or cone biopsy),
❖ I 3. Stage Ia1 with lymphovascular emboli, Ia2, Ib1, IIa1 and Ib2 (clinical stage) of
the 2018 FIGO classification
❖ I 4. Maximum diameter ≤ 40 mm by clinical examination and/or magnetic resonance
imaging (MRI),
❖ I 5. No suspicious node on pelvic MRI with an exploration up to the left renal vein
(according to RECIST 1.1),
❖ I 6. ECOG performance status 0-2
❖ I 7. Signed informed consent and ability to comply with follow-up,
❖ I 8. French subjects: In France, a subject will be eligible for inclusion in this study
only if either affiliated to, or a beneficiary of, a social security category.
20STUDY POPULATION (2/2)
2) Exclusion criteria:
Patient must meet NONE of the following criteria to be eligible for inclusion in this
study
❖ E 1. Pregnancy,
❖ E 2. Previous pelvic or abdominal cancer,
❖ E 3. Previous chemo and/or radiation therapy for the cervical cancer (previous brachytherapy
is accepted),
❖ E 4. Proven allergy to blue dye, isotope or indocyanine green (ICG).
! E.5. Other malignancy within the last 5 years except for treated cancer free of disease and
treatment,
! E.6. Patients with synchronous cancer
21STUDY CONDUCT
Pre-randomization assessment:
➢ Must be realized within the 30 days prior to randomization:
❖ Informed consent (before performing any specific study procedures)
❖ Eligibility criteria verification, which includes:
▪ Medical history (and particularly lymphatic risk factors),
▪ Childbirth history,
▪ Demographic data,
▪ Results of a punch biopsy or a cone biopsy (preferred option) available
▪ Tumor assessment with a pelvic MRI with an exploration up to the left renal vein.
A CT-scan can be performed in case of contra-indication or refusal of the MRI.
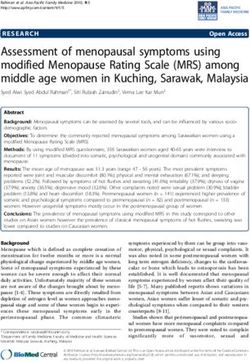
▪ Collection of an archival paraffin embedded tumor tissue sample (mandatory).
❖ Baseline conditions (ongoing pathologies, symptoms and concomitant medications)
❖ Physical examination (BMI, nodal areas, abdominal-lumbar-gynecological examination, specific
assessment for lymphatic and lower limb complications, PS, laboratory analysis, serum or urine
pregnancy test for women of childbearing potential, Quality of Life Questionnaires).
❖ LEL screening questionnaire for French sites only
❖ Blood sample and archived tumor sample (block) for translational research
22STUDY CONDUCT
Randomization:
The randomization will be processed the day of the surgery, after SLN biopsy results
available.
❖ Only patients with bilateral detection and fulfilling the “safety algorithm” without macroscopic
suspicious node and with negative frozen section on SLN will be randomized.
❖ Patient will be randomized using an Interactive Web Response System (IWRS) in a 1:1 ratio to one of the
2 study arms:
➢ Arm A (experimental arm): SLN dissection only. A full lymphadenectomy will not be performed. The radical
hysterectomy or trachelectomy will be done.
➢ Arm B (reference arm): SLN + PLN dissection. A full lymphadenectomy will be performed. The radical
hysterectomy or trachelectomy will be done.
REMINDER:
For translational research, collect nSLN for patient randomized in arm B !
23•Squamous or adenocarcinoma of the cervix,
•Stage Ia1 with lympho vascular emboli , Ia, Ib1, Ib2, IIa1 (FIGO
2018)
•Maximum diameter ≤ 40mm.
At the time of surgery
Patients with bilateral detection without
macroscopic suspicious node and negative frozen Patients with nodal involvement including
section on SLN unilateral and bilateral detection
(pN0) (pN1 cohorte)
Randomisation
1 : 1
Arm A (experimental) : Arm B (reference) :
SLN biopsy only SLN biopsy
+ hysterectomy or trachelectomy + Pelvic Lymphadenectomy
+ hysterectomy or
trachelectomy
24STUDY CONDUCT
Randomization:
❖ Be careful:
❖ Single blind study.
To ensure the blinding, we recommande to indicate in the surgical report that, in
the context of SENTICOL III study, the SLN procedure was performed and that a
complementary lymphadenectomy may be performed according to the allocated
arm.
The screening section of the CRF must be completed JUST before the
surgery!
Stratification:
Patients randomized will be stratified according to:
❖ Center,
❖ Stage of the disease (FIGO stage).
❖ Laparotomy vs laparoscopy or robotics ?
25 ARCAGY - GINECO 2014QUESTIONS
- Avez-vous des difficultés à conserver le simple insu?
- Que pensez-vous de la stratification sur le type de chirurgie?
26STUDY CONDUCT
pN1 cohorte
❖ Patients pN1: Are not randomized in the study.
➢ If the nodal involvement (bilateral or unilateral) is diagnosed
during surgery, the radical hysterectomy (or trachelectomy) should
be aborted and only lymphadenectomy should be performed.
➢ These patients will be followed up as a separate cohort to
record treatment and survival outcomes on the eCRF.
27 ARCAGY - GINECOSTUDY CONDUCT
Screening/ baseline failure:
A subject is considered to be a screen/baseline failure if she signs the
informed consent but could not be randomized.
All subjects screened for enrolment, including screening/baseline
failures, will be entered in the eCRF and listed on the Subject Screening
Log/Identification List.
Reasons for exclusion will be recorded in the CRF for subjects who do not
enter the study.
28AMENDEMENT AU PROTOCOLE
Autres modifications du protocole : Ajout des traitements autorisés:
- La curiethérapie avant l’hystérectomie selon les habitudes des centres : SLN
puis curieT - HT OU curieT puis SLN-HT
- La chimiothérapie néoadjuvante avant la trachélectomie
Amendement à déposer dans les prochaines semaines
29STUDY CONDUCT
Post-operative visit :
❖ Post-operative follow-up performed 30 days (+/- 7 days) after surgery
❖ Pathological results and proposal of management given and explained to the patient.
❖ Assessments to be done:
➢ Physical examination,
➢ Body weight,
➢ ECOG PS,
➢ Laboratory analysis (according to symptoms or examination findings evocating recurrence),
➢ Adverse events and particularly: surgical morbidity, complications (infection,
necrotizing fasciitis, mycoses…), specific assessment of lymphatic and lower limb
complications (anesthesia, paresthesia, dysesthesia)
➢ Patient education regarding sexual health will be performed,
➢ Health Related Quality of Life questionnaires (EORTC QLQ-C30 and QLQ-CX24)
➢ LEL questionnaire
30STUDY CONDUCT
Post-operative treatment recommendations:
❖ Post-operative treatment is not imposed in this protocol
❖ Recommendations are described in paragraph 5.7 according to the NCCN
guidelines.
Follow-up visits:
❖ To be done:
➢ Every 3 months +/- 1 week during the first year,
➢ Every 4 months +/- 1 week during the second year,
➢ Every 6 months +/- 2 weeks during the third-fifth year.
❖ Assessments: same as post operative visit assessments
31SAFETY (1/4)
1) Definitions (1/2):
❖ A serious adverse event (SAE) is an AE occurring during the study that fulfils one or more of the
following criteria:
➢ Results in death,
➢ Is immediately life-threatening,
➢ Requires in-patient hospitalization or prolongation of existing hospitalization,
➢ Results in persistent or significant disability/incapacity or substantial disruption of the ability to conduct
normal life functions,
➢ Is a congenital abnormality or birth defect,
➢ Is an important medical event that may jeopardize the patient or may require medical intervention to
prevent one of the outcomes listed above.
❖ should not be considered as SAEs in the context of this trial:
➢ Disease progression or death as a result of disease progression,
➢ Elective hospitalization and surgery for treatment of cervix cancer or its complications,
➢ Elective hospitalization to simplify treatment or procedures,
➢ Elective hospitalization in palliative care or respite care unit,
➢ Elective hospitalization for pre-existing conditions that have not been exacerbated by acts performed or
methods used in the study and also hospitalizationSAFETY (2/4)
1) Definitions (2/2):
❖ An expected serious adverse event is an event that is mentioned in the information described in the
SENTICOL study or information relative to the acts and methods used during the research.
❖ An unexpected adverse event (SUSAR) is an event that is not mentioned in the information relative to the
acts and methods used during the research, or for which the nature, the intensity or the outcome is not
consistent with the information relating to the practised acts and to the methods used during the research.
❖ An adverse event of special interest (AESI) is one of scientific and medical interest specific to
understanding of the acts and methods used and may require close monitoring and rapid communication by
the investigator to the sponsor. An AESI may be serious or non-serious.
The following adverse events have been identified as AESI and require that they should be followed
longer than regular AEs and should be declared as SAE even if occurred after the 30 day post -
operative period:
➢ Lymphatic and lower limb complications and particularly lymphedema, neurological symptoms
(anaesthesia, paraesthesia, dysesthesia) and venous insufficiency.
❖ A new fact is any new data which may lead to:
➢ A reassessment of the risk-benefits balance of the research or acts and methods used on the research,
➢ Changes in the acts or methods used, the conduct or documents related to the research,
➢ Suspend or interrupt or modify the protocol of the search or similar searches.
33SAFETY (3/4)
2) Recording of adverse events:
❖ AEs will be collected from time of informed consent throughout the 30-days following the surgery where
acts or methods are used.
❖ All ongoing and any new AEs/SAEs identified during the 30 calendar days post-operative period after surgery
or methods used in the study must be followed to resolution.
❖ The severity should be graded according to CTC-AE V4.03 and to:
• Clavien-Dindo classification for surgical complications
• Stage in case of lymphodema
❖ Deterioration as compared to baseline in protocol-mandated laboratory values, vital signs should be reported
as AEs only if they fulfil any of the SAE criteria.
❖ Deterioration of a laboratory value, which is unequivocally due to disease progression, should not be reported
as an AE/SAE.
34SAFETY (4/4)
3) Reporting of Serious Adverse Events:
❖ From the day when the informed consent form is signed to the surgery where acts will be performed, only
SAEs related to study procedures must be reported.
❖ from the surgery and until 30 days after surgery where acts and methods are used, or until the initiation of
alternative cancer therapy, all SAEs, whether or not considered causally related to the acts and methods
used or to the study procedures must be reported.
❖ All SAEs will be recorded in the CRF.
❖ If any reportable SAE occurs in the course of the study, then investigators or other site personnel inform
ARCAGY-GINECO for safety immediately after he or she becomes aware of it.
❖ The notification shall be made using an SAE form, documented as accurately as possible, by fax or e-mail
to the ARCAGY-GINECO pharmacovigilance department:
Pharmacovigilance ARCAGY-GINECO
Fax: +33 (0)1 84 25 40 68
pharmacovigilance@arcagy.org
35TRANSLATIONAL RESEARCH
36 ARCAGY - GINECO 2014 DateTRANSLATIONAL RESEARCH (1/5)
❖ Each site participating to the SENTICOL III study will participate to a tumor bank. The
translational research program will be performed in a second step.
❖ Collection of tumor and blood samples will be used for exploratory work to search for
biological predictors of relapse in “low risk” early cervical cancer.
Samples for translational research
Time of the study Type of sample Optional/mandatory
• Archival tumor sample from cervix biopsy or part
Inclusion of the conisation, Mandatory
• Blood sample (20 mL)
• 1 SLN sample from the surgery
Surgery • nSLN sample from the surgery (for patient in arm Mandatory
B only)
• Tumor samples
Disease progression • Optional and if available
Blood sample (20mL)
37TRANSLATIONAL RESEARCH (2/5)
Provided material:
❖ The CHU of Besançon, as sponsor, provides the material to constitute and ship bood samples
with the exception of EDTA tubes.
Use a kit dedicated to SENTICOL III and 1 bag/patient.
❖ Each site will receive one kit at its activation
❖ Additional kit will be sent at each randomization
38TRANSLATIONAL RESEARCH (3/5)
Blood samples process at inclusion and progression:
39TRANSLATIONAL RESEARCH (4/5)
Biological samples traceability:
❖ Samples collected for translational research must be identified with patient ID in real time
by filling a specific form in the eCRF.
40TRANSLATIONAL RESEARCH (5/5)
Biological Samples shipment:
❖ Samples collected will be centralized to the biological resources center (CRB) of the Institut
Curie (Paris, France) until analysis.
❖ Tumor samples collection will be organized by the sponsor. Sites will be informed as soon as a
collection is planned.
41COMMUNICATION AND TIMELINES
42STUDY CALENDAR
❖ Sites number: 300, including 50 in France
❖ Patients number : 950, including 200 in France
❖ Study start: 1st patient enrolled on the 3rd May 2018 in France
❖ Accrual period: 36 months
❖ End of accrual period: Q2 2021
❖ Follow-up period: 5 years
❖ Total study duration: 8 years
❖ Last follow-up: Q2 2026
43STATUT EN FRANCE
39 centres déclarés
31 centres ouverts (en noir)
19 centres recruteurs (en bleu)
Etablissement Ville PI
CHU Amiens - Picardie AMIENS Fabrice SERGENT
Hôpital Jean Minjoz BESANCON Rajeev RAMANAH
Clinique Tivoli BORDEAUX Sophie RICHARD
Institut Bergonié BORDEAUX Frédéric GUYON
Centre Hospitalier Universitaire Caen CAEN Raffaèle FAUVET
Centre François Baclesse CAEN Sandrine MARTIN-FRANCOISE
Hôpital Antoine Béclère CLAMART Xavier DEFFIEUX
CHU Estaing CLERMONTFERRAND Nicolas BOURDEL
Centre Hospitalier Intercommunal de Créteil CRETEIL Cyril TOUBOUL
CHU de Dijon DIJON Serge DOUVIER
Centre Hospitalier de Marne-la-Vallée JOSSIGNY Estelle WAFO
Centre Hospitalier Universitaire Kremlin- Le Kremlin-Bicêtre Hervé FERNANDEZ
Centre Hospitalier Régional Universitaire de
Lille - Hôpital Jeanne de Flandre LILLE Pierre COLLINET
44STATUT EN FRANCE
Etablissement Ville PI
Institut Paoli Calmettes MARSEILLE Eric LAMBAUDIE
Hôpital Saint-Joseph MARSEILLE Elisabeth CHEREAU-EWALD
ICM Val d'Aurelle MONTPELLIER Pierre-Emmanuel COLOMBO
Centre Hospitalier de Mulhouse - Hôpital du
Hasenrain MULHOUSE Ramzi KACEM
Centre Antoine Lacassagne NICE YvesFOUCHE
Centre Hospitalier Bichat - Claude Bernard PARIS Martin KOSKAS
Hôpital Européen Georges Pompidou PARIS Fabrice LECURU
Groupe Hospitalier Pitié Salpétrière PARIS Catherine UZAN
Hôpital Tenon PARIS Sofiane BENDIFALLAH
Centre Hospitalier Lyon Sud PIERRE-BENITE François GOLFIER
Hôpital de Poissy-Saint-Germain-en-Laye POISSY Cyrille HUCHON
Hôpital de la Milétrie - Centre Hospitalier
Universitaire de Poitiers POITIERS Cédric NADEAU
Centre Hospitalier Universitaire_Institut
Mère et Enfant Alix de Champagne REIMS Olivier GRAESSLIN
CHU de Rennes - Hôpital Sud RENNES Vincent LAVOUE
Hôpital Félix Guyon Saint Denis Peter VON THEOBALD
Institut Claudius Regaud IUCT-O TOULOUSE Gwénaël FERRON
ICL Institut de Cancérologie de Lorraine VANDOEUVRE-LES-NANCY
Frédéric MARCHAL
Gustave Roussy VILLEJUIF Sébastien GOUY
45STATUT EN FRANCE
11 centres ont inclus > 1patiente
Patientes
Ptes Pts screen
enregistr randomi failure (sauf Patientes
Etablissement PI ées sées pN1) PN1
Institut Paoli Calmettes Eric LAMBAUDIE 7 5 2
Centre Hospitalier Bichat - Claude
Bernard Martin KOSKAS 6 4
Institut Claudius Regaud IUCT-O Gwénaël FERRON 4 2 1 1
Clinique Tivoli Sophie RICHARD 3 2
Hôpital Européen Georges Pompidou Fabrice LECURU 3 2 1
Groupe Hospitalier Pitié Salpétrière Catherine UZAN 3 2 1
CHU Amiens - Picardie Fabrice SERGENT 2 1 1
Centre Hospitalier Universitaire Caen Raffaèle FAUVET 2 1 2
Centre Hospitalier Lyon Sud François GOLFIER 2 1 1
Sandrine MARTIN-
Centre François Baclesse FRANCOISE 2 1
ICL Institut de Cancérologie de Lorraine Frédéric MARCHAL 2 2
46STATUT EN FRANCE
➢ 8 centres en attente d’ouverture
Etablissement Ville PI
Hôpital Henri Duffaut AVIGNON Laurene LUGANS
Groupement Hospitalier Est -
Hôpital Femme Mère Enfant BRON Gautier CHENE
Hôpital de la Conception MARSEILLE Aubert AGOSTINI
ICO Centre René Gauducheau SAINT-HERBLAIN Cécile LOAC
Centre Jean Perrin CLERMONT-FERRAND Christophe POMEL
Hôpital des Diaconesses PARIS Marcos BALLESTER
Institut Curie - Hopital Claudius
Régaud PARIS Virginie FOURCHOTTE
Centre Hospitalier Universitaire
Dupuytren LIMOGES Tristan GAUTHIER
47COURBE D’INCLUSION
44 screening
29 randomisées
2 pN1
10 échec de screening
Nous avons besoin de vous!
48STATUT PAYS ETRANGERS
▪ Soumission aux comités d’éthique faite pour Le japon et la Chine
Pays Statut
Canada
Soumission règlementaire en cours de
New york
préparation
Démarrage international Q3/Q4 2019
49➢ Sélection et préparation des soumissions en cours
Allemagne Pays-Bas
UK Pays
Cuba Nordiques
Thaïlande Suisse
Vietnam Brésil
Perou
Colombie Inde
Italie
Texas
50STUDY TOOLS AND MONITORING
51eCRF (1/3)
❖ Data Management: EURAXI
❖ eCRF: CLINSIGHT
❖ E CRF Link: https://ecrf.euraxipharma.fr/CSOnline/
❖ Each investigator and CRA will have his access code for randomization and to complete the CRF, they will
received it by Email:
52eCRF (2/3)
eCRF home page
53eCRF (3/3)
eCRF Section overview
54IWRS (1/2)
❖ Randomization by IWRS, linked to the eCRF
❖ Be careful: randomization during the surgery
→ dedicated study staff for this procedure
should be available
→ Mandatory items to be filled for
randomization: inclusion and exclusion
criteria, Figo stage
→ All the screening forms should be
completed before the surgery
55IWRS (2/2)
❖ Confirmation of randomization sent to site (CRA + investigator) and sponsor
56Focus on pN1 cohorte
❖ If nodal involvement at frozen section:
-> record the patient as a screening failure and complete the pN1
forms
❖ If nodal involvement at definitive examination (ie after
randomization):
-> the patient is no longer followed in the principal study.
Don’t complete the eCRF sections after the “SLN and nSLN definitive
examination” one.
Complete the pN1 forms.
57MONITORING
❖ Monitoring realized by CHU Besançon:
▪ CRA: Caroline CARETTE and Aude Le Breton
▪ Project Manager for France sites: Kristina MOUYABI : kmouyabi@chu-besancon.fr
❖ Realized according to the Risk-based monitoring
❖ Site Initiation Visit will be conducted by phone
❖ First on-site monitoring visit: One month after the first patient’s surgery
❖ Generally, subsequent monitoring visits will be done. The frequency could be modified according to the
monitoring plan
❖ High level considerations :
▪ Informed Consent Form
▪ Inclusion criteria
▪ Primary Objectives
▪ Secondary Objectives
▪ Serious Adverse Event
▪ Investigator Site File
❖ Don’t forget data for patient in pN1 cohort!
58THANK YOU FOR YOUR ATTENTION!
Any question?
59REGULATORY CONSIDERATIONS (1/2)
❖ Principal Investigator responsibilities:
➢ Respect the study confidentiality,
➢ Give his curriculum vitae and those of the co-investigators,
➢ Give a GCP certificate dated less than 2 years ago (see following slide)
➢ Identify the members of the team who participate to the study and define their role and
responsibilities,
➢ Start the patient recruitment after sponsor authorization,
➢ Make himself available for the monitoring visit (if any) and for investigator meetings.
❖ Each Investigator responsibilities:
➢ Respect the study confidentiality,
➢ Collect informed consent that should be signed and personally dated by patients before any study
procedure,
➢ Regularly complete the eCRF of each patient included,
➢ Notify as soon as possible any SAE arising in the course of the research,
➢ Accept calls or monitoring visits of the CRA and possibly by auditors mandated by the sponsor or by
the competent authorities,
➢ Give direct access to source documents about patients (medical or hospital record, nursing follow-
up, results of additional tests …) to CRA or auditors.
60REGULATORY CONSIDERATIONS (2/2)
GCP certificates:
❖ Good Clinical Practice (GCP) is an international ethical and scientific quality standard
for designing, conducting, recording and reporting trials that involve the participation of
human subjects.
❖ Each Principal Investigator must provide a GCP certificate dated less than 2 years ago before its site
initiation.
❖ If the PI doesn’t have GCP certificate, he can ask the CHU of Besançon for registering him to an
online training
Consent withdrawal:
❖ Reminder: If the patient withdraws her consent, sponsor is not allowed to collect any data about
the patient after the date of withdrawal.
❖ Make the difference between a consent withdrawal and a refusal to participate in one aspect of
the study (completion of HR-Qol questionnaires at follow-up, for instance).
61You can also read