SEPSIS Leighton Smith MD CMO Florida Hospital Fish Memorial
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

SEPSIS
Leighton Smith MD
CMO Florida Hospital Fish Memorial
FLORIDA HOSPITAL FISH MEMORIAL 175 Bed Acute Care Hospital No Obstetrics or Pediatric in patient beds No Neurosurgery or Cardiac surgery 5000 ED visits per month 1000 bed Quaternary Hospital 35 miles away Tertiary Hospital 35 miles in the other direction Undergoing a 100 million dollar expansion


Adventist Health System Cerner Electronic Medical Record Standardized evidence based order sets called power plans Many sets of data available through the electronic system Examples: Mortality, bundle compliance, antibiograms etc.
44 campuses in 10 states More than 7,700 inpatient beds From sole community providers to large tertiary facilities
17 long-term care facilities in 6 states 1,997 beds

FIVE YEAR SEPSIS JOURNEY Situation 5 years ago The need to change The milestones of progress The surviving sepsis campaign The 3 hour and six hour bundle Sirs criteria sofa criteria Results so far Future challenges

Institute for Healthcare Improvement
2x2 Mortality Matrix
2017 ICU No ICU
n = 160 Admission Admission
Box 1 Box 2
Comfort Care
0% (0) 0% (0)
Non Comfort Box 3 Box 4
Care 57.5% (92) 42.5% (68)
2x2 Matrix for Mortalities in Box 3 & 4. To consider:
• Failure to Recognize (change in heart rate, respirations, etc.)
• Failure to Plan (diagnosis, treatment, calling rescue team, etc.
• Failure to Communicate (patient to staff, clinician to clinician,
etc.)
CONFIDENTIAL Patient Safety Work Product. Protected under the Patient Safety And Quality Improvement Act.
Do Not Disclose unless authorized by the FHFM PSES Advisory Committee.2x2 Morality Matrix
Move Your Dot Annual Trends
2x2 Mortality Matrix
Goal is Box 3 = >50% of mortalities with an initial level of care admission into the ICU
80.0%
70.0% 67.0%
60.0% 57.5%
55.0%
50.0%
45.0%
45.1% 42.9% 42.5%
40.0% 38.2% 37.9%
32.0%
30.0%
20.0%
14.1%
10.4%
10.0% 6.4% 5.1%
0.0%0.8% 0.0%0.0% 0.0%0.0%
0.0%
2013 2014 2015 2016 2017
Box 1 Box 2 Box 3 Box 4 Goal
CONFIDENTIAL Patient Safety Work Product. Protected under the Patient Safety And Quality Improvement Act. Do Not Disclose
unless authorized by the FHFM PSES Advisory Committee.Key Definitions of SEPSIS
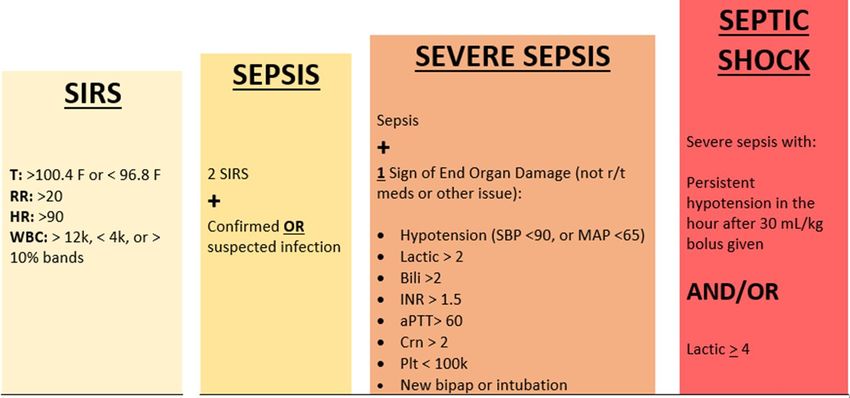
SEPSIS Signs & Symptoms
SEPSIS: Systemic inflammation due to an infection.
The patient exhibits at least two of the
following symptoms:
• Body temperature above 100.9 F (38.3 C) or
below 96.8F (36 C)
• WBC greater than 12,000 or less than 4,000
• Heart rate higher than 90 bpm
• Respiratory rate higher than 20 breaths per
minute
• AND
• Probable or confirmed infectionSevere SEPSIS Signs & Symptoms
SEVERE SEPSIS: The patient’s condition will be
upgraded if they also exhibit at least one of the
following signs and symptoms, which indicate an
ORGAN may be failing
• Significantly decreased urine output
• Abrupt change in mental status
• Decrease in platelet count
• Difficulty breathing as evidenced by need for
intubation or bipap
• Hypotension
• Increased Creatine
• Elevated INR, or aPTT and not on blood thinners
• Lactic acid > 2.0SEPTIC SHOCK Signs & Symptoms
• SEPTIC SHOCK: Infection + SIRS+ organ dysfunction + hypotension
despite fluid resuscitation
OR SEVERE SEPSIS and LA >=4.0
• The Onset Of SEPTIC SHOCK is determined when a patient with suspected infection has:
• Two (2) SIRS Criteria:
• Temperature > 38.3 C/100.9 F or 90 bpm
• RR > 20 breaths/per/min.
• WBC > 12,000 or < 4,000
• AND One (1) of the following:
• And 1 of the following
• Hypoperfusion: SBP < 90mm HG; MAP < 60 mmHg;
• After a 30mL/kg bolus has been administered
OR
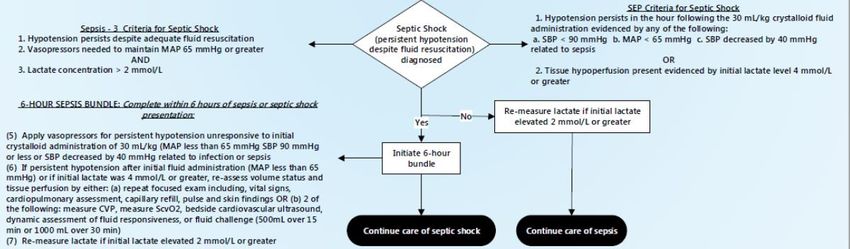
• Serum lactate 4 mmol/L regardless of the BPHow is SEPTIC SHOCK Defined?
SEPTIC SHOCK is defined when:
Documentation by the MD/NP/PA of septic shock, or that septic
shock is suspected
OR
Must be documentation of or criteria met for SEVERE SEPSIS
AND
Tissue hypoperfusion as evidenced by:
Persistent hypotension (2 or more consecutive values within an hour
after fluids are completed)
SBPCerner SEPSIS Alert
The computer/Cerner is constantly checking for SIRS or SEPSIS criteria
When a patient qualifies the alert will fire
You do not have to be in the patients chart for the alert to fire
Call the SEPSIS ALERT Code in your facility if the Alert indicates it’s
appropriateWhat makes the SIRS & SEPSIS Alerts Fire within Cerner?
The Sepsis 3 Hour Bundle…Don’t WAIT!!
Obtain physician order for:
- Broad spectrum IV antibiotics AND
- Fluid bolus for initial hypotension (SBPSEPSIS Cerner Alert
Patient Information
*Clicking on the link will take
you into the patient’s chart
that the alert pertains to.
*You could be on one patients Link to the patient chart
chart when this alert fires for
another patient. Pay close
attention to the patient
information displayed within
the alert.
Criteria that caused the alert to fireURGENT SECOND MARKER: 6 Hour
MUST BE completed within SIX HOURS of time of presentation:
Apply VASOPRESSORS (for hypotension that does not respond to initial fluid
resuscitation) to maintain a mean arterial pressure (MAP) ≥65mmHg
If persistent hypotension after initial fluid administration (MAP < 65 mm Hg)
or if initial lactate was ≥4 mmol/L, RE-ASSESS VOLUME STATUS AND TISSUE
PERFUSION and document findings accordingly
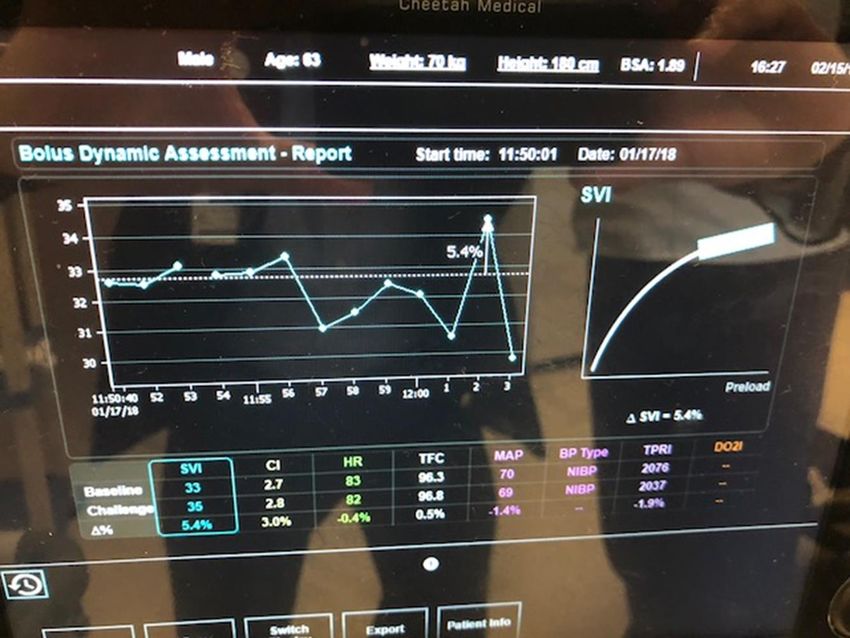
Re-measure LACTIC ACID LEVEL if initial lactate elevatedDynamic variables for assessing fluid responsiveness
Leg raising Leg raising
Passive leg raise or fluid challenge
Patient is seated at 45 degrees head
up semi-recumbent position
Patient’s upper body is lowered to
horizontal and legs passively raised
to 45 degrees up
Maximal effect occurs at 30–90
secondsPassive Leg Raise 10% increase in stroke volume on a cardiac output monitor reflects a positive test (9% increase in stroke volume has 86% sensitivity and 90% specificity) OR 10% increase in pulse pressure via an arterial line (79% sensitivity and 85% specificity)
CMS Approved Monotherapy Antibiotics
CMS Approved Combination Antibiotics
Vasopressor Use if indicated
Procalcitonin in Sepsis
Procalcitonin in Sepsis
Blinded, prospective multicenter observational clinical trial
Study group were consecutive patients meeting criteria for severe sepsis or
septic shock who were admitted to the ICU
Procalcitonin was collected within the first 12 hr. & measured daily over the
first 5 days
A procalcitonin decrease of more than 80% from baseline to day 4 was
associated with a two-fold lower mortality at 28 days as compared to those
without the decrease (20% vs 10%; p = 0.001)Procalcitonin in Sepsis
Serum lactate is a biomarker commonly used to help guide response to
resuscitation measures
Procalcitonin (PCT) has been demonstrated to be helpful in antibiotic
stewardship decisions
Kinetics of PCT have also been shown to predict mortality and treatment
failure in sepsisProcalcitonin Conclusions
Inability to decrease procalcitonin by more than 80% is a significant
independent predictor of mortality in sepsis
To simplify, in secondary analysis, if PCT increased from baseline to day 1
there was a three-fold higher mortality than if PCT decreased
May translate into better informed clinical decisions regarding intensification
of care or ICU dischargeHydrocortisone, Vit C and Thiamine Rx for Sepsis
Hydrocortisone, Vit C and Thiamine for
Sepsis
Treatment Arm – 47 consecutive patients with severe sepsis (53%) and septic
shock (47%) January 2016 and July 2016 treated with of 1.5 g vitamin C IV
every 6 hours, hydrocortisone 50 mg IV every 6 hours, and thiamine 200
mg IV every 12 hours within 24 hours of admission to ICU
Thiamine inhibits oxalate production and has potential
benefits in septic shockHydrocortisone, Vit C and Thiamine for
Sepsis
Exclusions - < 18 years of age, pregnancy, limitations of care, and septic
patients with PCT < 2ng/ml
Threshold PCT of 2ng/ml to increase the certainty that the patients had
severe sepsis and were at risk of developing sepsis-related organ dysfunctionHydrocortisone, Vit C and Thiamine for
Sepsis
The control group consisted of the same number of consecutive patients
admitted to the ICU between June 2015 and December 2015 using the same
inclusion and exclusion criteria as the treatment group, and were matched in
baseline characteristicsHydrocortisone, Vit C and Thiamine for
Sepsis
Hospital mortality was 4 of 47 (8.5%) in those in the treatment arm
compared to 19 of 47 (40%) in the comparator group (pCURRENT ACTION PLAN
Code sepsis in ED
Point of service lactate
Review of all fall outs
Feed back to providers with fall outs
Multidisciplinary group that meets every two weeks and reports to the
executivesQuestions??
You can also read

















































