Step I: White Paper Application
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Step I: White Paper Application
Application Guidelines
1. The application should be submitted electronically per requirements via the web site
of any of the NIAID Genomic Sequencing Centers for Infectious Diseases. Include all
attachments, if any, to the application.
2. There are no submission deadlines; white papers can be submitted at anytime.
3. GSC personnel at any of the three Centers can assist / guide you in preparing the
white paper.
4. Investigators can expect to receive a response within 4-6 weeks after submission.
5. Upon approval of the white paper, the NIAID Project Officer will assign the project
to a NIAID GSC to develop a management plan in conjunction with the participating
scientists.
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 1White Paper Application
Project Title: Escherichia coli as human pathogen: Uncomplicated urinary tract
infection (UTI) and UTI induced bacteremia
Authors:
Primary Investigator Contact:
Name Niels Frimodt-Moller
Position Head, Antibiotic Research
Institution Statens Serum Institut
Address Artillerivej 5, Copenhagen S
State/Country Denmark
ZIP Code DK-2300
Telephone +45 32 68 36 46
Fax +45 32 68 32 31
E-Mail nfm@ssi.dk
1. Executive Summary (Please limit to 500 words.)
Provide an executive summary of the proposal.
Escherichia coli is a major human pathogen, causing up to 80% of uncomplicated UTI and
30% of bacteremia cases. Escherichia coli is the most prominent cause of both
community-acquired (CA) and nosocomial (NA) bloodstream infections worldwide, and
the associated rate of mortality due to sepsis is high (Laupland et al., 2008). In the U.S., E.
coli related urinary tract infections kill ~7200 persons annually, and the annual mortality
associated with E. coli bacteremia in the U.S. is around 36,000-40,000 (Russo & Johnson,
2003).
Urinary tract infections (UTIs) are among the most common bacterial infections
encountered in clinical practice and account for significant morbidity and high medical
costs (Foxman, 2002). During any single year, 11% of women aged 18 and older develop
UTI, and the lifetime risk of UTI among women is 60% (Foxman et al., 2000). Escherichia
coli is the most predominant pathogen causing 80–90% of community-acquired UTIs and
more than 30% of nosocomially acquired UTIs (Ferry et al., 2004; Kahlmeter, 2000;
Bouza et al., 2001). Recurrent UTIs (RUTIs) are reported in 16–25% of women within 6
months of an UTI episode and in 40% of women within one year of an UTI episode, and
thus pose a major problem (Foxman, 1990; Foxman et al., 1995; Ikaheimo et al., 1996;
Karkkainen et al., 2000). Although most common among women, UTI is also a significant
problem among men, who can experience cystitis, pyelonephritis, acute and chronic
prostatitis and febrile UTI (Lipsky et al., 1989; Ulleryd, 2003).
We propose sequencing several collections of E. coli urinary and blood isolates in order to
provide insight into:
1) the genetic determinants associated with infection of the urinary tract both among
women and men.
2) the genetic determinants associated with the relapse and persistence of E. coli in
spite of treatment for UTI.
3) the genetic determinants associated with the dissemination to the blood.
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 2Such knowledge could be used to predict the likelihood that patients with uncomplicated
UTI will be at risk for persistence/relapse or spread to bloodstream as well as identify risk
factors in the fecal E. coli of healthy people. The data produced will increase our
understanding of the mechanisms of E. coli pathogenesis. Further, this data may be used to
develop intervention strategies to prevent and treat infections with this pathogen.
2. Justification
Provide a succinct justification for the sequencing or genotyping study by describing the
significance of the problem and providing other relevant background information.
This section is a key evaluation criterion.
1. State the relevance to infectious disease for the organism(s) to be studied; for
example the public health significance, model system etc.
2. Are there genome data for organisms in the same phylum / class / family / genus?
What is the status of other sequencing / genotyping projects on the same organism
including current and past projects of the NIAID GSC? Provide information on
other characteristics (genome size, GC content, repetitive DNA, pre-existing arrays
etc.) relevant to the proposed study. Have analyses been performed on the raw data
already generated/published? If additional strains are proposed for a species,
please provide a justification for additional strains?
3. If analyses have been conducted, briefly describe utility of the new sequencing or
genotyping information with an explanation of how the proposed study to generate
additional data will advance diagnostics, therapeutics, epidemiology, vaccines, or
basic knowledge such as species diversity, evolution, virulence, etc. of the proposed
organism to be studied.
Recurrent UTI:
Treatment, host and pathogen characteristics are considered to have an impact on
development and frequency of RUTI; however, many aspects are unclear or poorly
described. Up to 77% of RUTIs are caused by E. coli identical to the primary infecting E.
coli; however, characteristics of E. coli associated with relapse of UTI remain poorly
defined (Ejrnaes et al., 2006; Russo et al., 1995; Skjøt-Rasmussen et al., 2011).
Phylogenetic group B2 has been found to be associated with strains causing persistence or
relapse of UTI (Johnson et al., 2007). A wide variety of virulence factors (VFs) have been
associated epidemiologically or experimentally (in vivo) with uropathogenic E. coli
(UPEC) including adhesins, iron uptake systems, toxins and protectins; however, only a
few minor, older studies have addressed the relation between VFs and relapse of UTI in
women (Johnson & Russo, 2005; Foxman et al., 1995; Johnson et al., 2001).
Although the fecal and vaginal flora were thought to constitute the reservoir for RUTI-
causing E. coli strains, this view has become increasingly challenged by the finding that E.
coli can invade and replicate within the murine bladder forming biofilm-like intracellular
bacterial communities (IBCs) (Anderson et al., 2003; Garofalo et al., 2007). These IBCs
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 3dissociate and E. coli flux out and ultimately establish quiescent intracellular reservoirs that may represent stable reservoirs for RUTI (Mysorekar et al., 2006; Schilling et al., 2002). The IBC pathogenic cycle has not been studied in humans; however, recently exfoliated IBCs were detected in urine from women with acute uncomplicated cystitis which supports the presence of the IBC pathway and occurrence of an intracellular bacterial niche in some women with UTI (Rosen et al., 2007). IBC formations contain biofilm-like structures and it has been shown that E. coli causing persistence or relapse exhibited significantly increased biofilm formation on plastic surface in vivo, but the prevalence of virulence factors associated with biofilm formation (e.g. agn43) has not been examined in relation to E. coli causing relapse (Ejrnaes, K., A. Reisner, B. Lundgren, S. Ferry, T. Monsen, S. Holm, E. Zechner, and N. Frimodt-Moller, submitted for publication; Soto et al., 2006). Recently, heme- and siderophore-associated iron have been shown to play a key role in IBC development in mice; however, it is not known whether this observation is reflected in an association between prevalence of genes coding for different iron uptake systems and E. coli strains causing relapse of UTI (Reigstad et al., 2007). Male UTI: Many aspects on male UTI are unclear or poorly described. Knowledge of male UTI is less than that of female UTI even though it is estimated that one-third of all 80-year-old men will have had an episode of bacturia (Lipsky, 1989). It is generally believed, that all UTIs in men must be considered complicated since the infections results from an anatomic or functional anomaly, however there is little evidence to support this hypothesis. A better understanding of the pathogenesis of UTI in men is needed in order to identify possible targets for preventive and protective measures. Bacteremia: Around 17-37% of invasive bacteremic E. coli infections are due to Extraintestinal Pathogenic E. coli (ExPEC), which often originate from an infection in the patients´ urinary tract (Olesen et al., 1995; Russo & Johnson, 2003). ExPEC possess a wide variety of specialized virulence factors (VFs), however the requirements for bacterial invasion of the bloodstream are yet undetermined (Ron, 2006). Non-presence of virulence factors such as adhesins has been shown to relate to infections in patients with immune depression (Maslow et al., 1993). However, few studies have investigated the decisive virulence factors involved in UTI pathogenic E. coli strains invading the blood stream (Johnson & Stell, 2000; Moreno et al., 2005; Rijavec et al., 2008). In order to identify and develop new targets for antimicrobial agents or develop a vaccine, it is necessary to understand the pathogenesis and virulence of bacteremic E. coli. Previous work: The Broad Institute has recently completed sequencing of over eighty five commensal E. coli. A major goal of that work was to provide a commensal, non-pathogenic context in order to better understand the genomics of E. coli pathogenesis. Specifically, this project sequenced nine commensal strains from the ST95 clone, which is one of the most predominant UTI clones. Analysis of the proposed UTI and bacteremia isolates, in conjunction with those commensal isolates, will enable us to identify pathogenesis-specific loci. Other GSCIDs have focused on other pathogenic groups of E. coli, such as the Genomic Sequencing Centers for Infectious Diseases: White Paper Form 4
O157:H7 serotype. A comparison with those data will further refine our understanding of
how genetic variation contributes to specific E. coli-related disease syndromes.
The study has major relevance for the understanding of the virulence potential of E. coli
isolated from healthy persons or from patients with uncomplicated UTI. These data
ultimately could aid the prediction of the course of infection or complications, or lead to
intervention strategies in E. coli-related disease. To our knowledge, similar studies using a
well-designed E. coli collection from UTI and bacteremia have not been performed before,
especially at this scale. The public health benefit from such a project concerning this
particular pathogen has enormous potential.
3. Rationale for Strain Selection
4. Provide the rationale behind the selection of strains and the number of strains proposed
in the study. The focus of the program is on potential agents of bioterrorism or
organisms responsible for emerging or re-emerging infectious diseases. Non-select
agents or non-pathogenic organisms will be considered when they can provide insight
into these scientific areas.
E. coli strains were isolated from three populations:
1) Umeå collection: Female UTI patients with uncomplicated UTI experiencing either cure (n =
30), relapse (n = 46) or persistence of infection (n = 32)
2) Køge collection: Male UTI patients with uncomplicated (n = 7) or recurrent UTI (n = 3) and
female patients experiencing recurrent UTI (n = 10)
3) Hvidovre collection: Bacteremia patients (n = 197)
This will yield a total of 315 E. coli strains for sequencing.
Female recurrent UTI (Umeå collection):
The Umeå collection of female recurrent UTI E. coli strains were obtained through a study
performed by Ferry et al., 2007, where about 1200 women with uncomplicated UTI were
randomized to one of four groups: Three groups received mecillinam orally for 3 or 7 days,
while the fourth group received placebo. Control visits occurred 1 week after treatment and 4
weeks after treatment.
The patients consisted of a cohort of women with uncomplicated urinary tract infection, who
delivered three urine samples:
1) at the first visit at the family doctor (general practitioner), where the diagnosis of UTI
was confirmed,
2) first control sample one week after the end of antibiotic treatment, and
3) second control sample one month after the end of treatment.
Based on PFGE typing of E. coli isolates, patients could be divided in three groups: i) cure (no
growth in control samples); ii) relapse (no growth in the first control sample, but growth of the
same PFGE type in the second of control samples); iii) persistence (growth in the first control
sample of the same PFGE type). In all, 57 E. coli strains from cured patients and 88 E. coli
strains from patients with persistence/relapse were isolated.
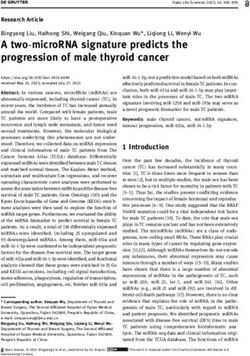
Table 1 shows the distribution of E. coli strains in the mecillinam treated groups, where cure,
persistence or relapse was discerned by PFGE-typing (100% band similarity was used as a
criterion for identity). Overall, around 80% similarity was found for strains causing relapse or
persistence (Ejrnaes et al., 2006). This illustrates, that most strains remaining in the urine were
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 5the same as the originally infecting strain. It is therefore highly likely that these strains were
surviving in a urinary tract reservoir, unreached by antibiotic treatment; experimental mouse
UTI studies have shown that E. coli infecting the bladder are not removed by antibiotic
treatment (Hvidberg et al., 2000). The reason for this can be biological biofilm formation or
some other factor protecting the bacteria from antibiotic present both in urine and in blood.
Table 1.
E. coli distributed according to PFGE typing: “Same” means 100% similar in PFGE-profile.
Pivmecillinam
a
Culture Result Course of Infection Groups
n = 155
400 200 200
mg mg mg
st b nd c d d d
Initial Visit 1 follow-up 2 follow-up n BID BID TID
for 3 for 7 for 7
days days days
E. coli Negative Negative Cure 37 11 13 13
E. coli Negative Missing Cure 0 0 0 0
e
E. coli Same E. coli Same E. coli Persistence 15 7 4 4
E. coli Same E. coli Negative Persistence 5 3 1 1
E. coli Same E. coli Missing Persistence 12 10 0 2
E. coli Negative Same E. coli Relapse 46 17 16 13
f
E. coli Negative New E. coli Reinfection 14 4 5 5
E. coli New E. coli New E. coli Reinfection 2 1 0 1
E. coli New E. coli Negative Reinfection 2 1 0 1
E. coli New E. coli Missing Reinfection 2 2 0 0
Total 62 46 47
a
Course of infection according to PFGE results by Ejrnaes et al. (5)
b
8-10 days post inclusion
c
35-49 days post inclusion
d
BID, twice a day; TID, three times a day
e
Same E. coli as the primary infecting E. coli at inclusion according to
PFGE (5)
f
E. Coli different from the primary infecting E. coli at inclusion according to
PFGE (5)
Male and female (recurrent)UTI (Køge collection):
Between December 2005 and April 2006, consecutive urine culturing on patients with symptoms
of UTI was performed at a primary care clinic (not associated to any hospital). E. coli isolates
were collected from 102 patients with community-acquired UTI, and 13 of these patients (10
women and 3 men) experienced recurrent UTI (Skjøt-Rasmussen et al., 2011). Besides the 3
men experiencing RUTI, 7 male patients experienced uncomplicated UTI. The following
isolates from this strain collection will be included in the study: Isolates from male
uncomplicated (n = 7) and recurrent UTI (n = 3) and female recurrent UTI (n = 10).
Bacteremia (Hvidovre collection):
This strain collection consists of 197 E. coli isolates from the blood of 196 adult patients with
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 6both bacteremia and bacturia. From one patient, two E. coli blood isolates were cultured. Isolates
were collected from January 2003 through May 2005 from all patients older than 18 years
admitted to four hospitals in Copenhagen. Isolates represent all consecutive episodes of E. coli
bacteremia with bacturia, where a positive E. coli urine culture was performed +/- three days
within the blood culture date.
References:
- Anderson, G. G., J. J. Palermo, J. D. Schilling, R. Roth, J. Heuser, and S. J. Hultgren. 2003. Intracellular
bacterial biofilm-like pods in urinary tract infections. Science 301:105-107.
- Bouza, E., R. San Juan, P. Munoz, A. Voss, and J. Kluytmans. 2001. A European perspective on nosocomial
urinary tract infections I. Report on the microbiology workload, etiology and antimicrobial susceptibility
(ESGNI-003 study). European Study Group on Nosocomial Infections. Clin Microbiol Infect 7: 523-531.
- Ejrnaes, K., D. Sandvang, B. Lundgren, S. Ferry, S. Holm, T. Monsen, R. Lundholm, and N. Frimodt-Moller.
2006. Pulsed-field gel electrophoresis typing of Escherichia coli strains from samples collected before and
after pivmecillinam or placebo treatment of uncomplicated community-acquired urinary tract infection in
women. J Clin Microbiol 44: 1776-1781. (Part of this study).
- Ferry, S. A., S. E. Holm, H. Stenlund, R. Lundholm, and T. J. Monsen. 2004. The natural course of
uncomplicated lower urinary tract infection in women illustrated by a randomized placebo controlled
study. Scand J Infect Dis 36: 296-301.
- Ferry, S. A., S. E. Holm, H. Stenlund, R. Lundholm, and T. J. Monsen. 2007. Clinical and bacteriological
outcome of different doses and duration of pivmecillinam compared with placebo therapy of
uncomplicated lower urinary tract infection in women: the LUTIW project. Scand J Prim Health Care 25:
49-57.
- Foxman, B. 1990. Recurring urinary tract infection: incidence and risk factors. Am J Public Health 80: 331-
333.
- Foxman, B. 2002. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J
Med 113 Suppl 1A: 5S-13S.
- Foxman, B., R. Barlow, H. D'Arcy, B. Gillespie, and J. D. Sobel. 2000. Urinary tract infection: self-reported
incidence and associated costs. Ann Epidemiol 10: 509-515.
- Foxman, B., L. Zhang, P. Tallman, K. Palin, C. Rode, C. Bloch, B. Gillespie, and C. F. Marrs. 1995.
Virulence characteristics of Escherichia coli causing first urinary tract infection predict risk of second
infection. J Infect Dis 172: 1536-1541.
- Garofalo, C. K., T. M. Hooton, S. M. Martin, W. E. Stamm, J. J. Palermo, J. I. Gordon, and S. J. Hultgren.
2007. Escherichia coli from urine of female patients with urinary tract infections is competent for
intracellular bacterial community formation. Infect Immun 75: 52-60.
- Hvidberg, H., C. Struve, K. Krogfelt, N. Christensen, S. N. Rasmussen, and N. Frimodt-Møller. 2000.
Development of a long term ascending urinary tract infection mouse model for antibiotic treatment studies.
Antimicrob Agents Chemother 44: 156-163.
- Ikaheimo, R., A. Siitonen, T. Heiskanen, U. Karkkainen, P. Kuosmanen, P. Lipponen, and P. H. Makela.
1996. Recurrence of urinary tract infection in a primary care setting: analysis of a 1-year follow-up of 179
women. Clin Infect Dis 22: 91-99.
- Johnson, J. R., B. Johnston, A. Murray, M. A. Kuskowski, J. N. Maslow, and C. Johnson. 2007. Bacterial
characteristics as predictors of posttherapy recurrent bacteriuria among children with acute uncomplicated
cystitis caused by Escherichia coli. Pediatr Infect Dis J 26: 1151-3.
- Johnson, J. R., T. T. O'Bryan, P. Delavari, M. Kuskowski, A. Stapleton, U. Carlino, and T. A. Russo. 2001.
Clonal relationships and extended virulence genotypes among Escherichia coli isolates from women with a
first or recurrent episode of cystitis. J Infect Dis 183: 1508-1517.
- Johnson, J. R. and T. A. Russo. 2005. Molecular epidemiology of Extraintestinal pathogenic (uropathogenic)
Escherichia coli. Int J Med Microbiol 295: 383-404.
- Johnson, J. R. and A. L. Stell. 2000. Extended virulence genotypes of Escherichia coli strains from patients
with urosepsis in relation to phylogeny and host compromise. J Infect Dis 181: 261-272.
- Kahlmeter, G. 2000. The ECO.SENS Project: a prospective, multinational, multicentre epidemiological
survey of the prevalence and antimicrobial susceptibility of urinary tract pathogens--interim report. J
Antimicrob Chemother 46 Suppl. 1: 15-22.
- Kahlmeter, G. 2003. An international survey of the antimicrobial susceptibility of pathogens from
uncomplicated urinary tract infections: the ECO.SENS Project. J Antimicrob Chemother 51: 69-76.
- Karkkainen, U. M., R. Ikaheimo, M. L. Katila, and A. Siitonen. 2000. Recurrence of urinary tract infections
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 7in adult patients with community-acquired pyelonephritis caused by E. coli: a 1-year follow-up. Scand J
Infect Dis 32: 495-499.
- Laupland, K. B., D. B. Gregson, D. L. Church, T. Ross, and J. D. D. Pitout. 2008. Incidence, risk factors and
outcomes of Escherichia coli bloodstream infections in a large Canadian region. Clin Microbiol Infect 14:
1041-1047.
- Lipsky, B. A. 1989. Urinary tract infections in men: epidemiology, pathophysiology, diagnosis, and
treatment. Ann. Intern. Med. 110: 138–150.
- Maslow, J. N., M. E. Mulligan, K. S. Adams, J. C. Justis, and R. D. Arbeit. 1993. Bacterial adhesins and host
factors: role in the development and outcome of Escherichia coli bacteremia. Clin Infect Dis 17: 89-97.
- Moreno, E., I. Planells, G. Prats, A. M. Planes, G. Moreno, and A. Andreu. 2005. Comparative study of
Escherichia coli virulence determinants in strains causing urinary tract bacteremia versus strains causing
pyelonephritis and other sources of bacteremia. Diagn Microbiol Infect Dis 53: 93-99.
- Mysorekar, I. U. and S. J. Hultgren. 2006. Mechanisms of uropathogenic Escherichia coli persistence and
eradication from the urinary tract. Proc Natl Acad Sci U S A 103:14170-14175.
- Olesen, B., H. J. Kolmos, F. Orskov, I. Orskov, and A. Gottschau. 1995. Bacteraemia due to Escherichia coli
in a Danish university hospital, 1986-1990. Scand J Infect Dis 27: 253-7.
- Reigstad, C. S., S. J. Hultgren, and J. I. Gordon. 2007. Functional genomic studies of uropathogenic
Escherichia coli and host urothelial cells when intracellular bacterial communities are assembled. J Biol
Chem 282: 21259-21267.
- Rijavec, M., M. Müller-Premru, B. Zakotnik, and D. Zgur-Bertok. 2008. Virulence factors and biofilm
production among Escherichia coli strains causing bacteraemia of urinary tract origin. J Med Microbiol 57:
1329-1334.
- Ron, E. Z. 2006. Host specificity of septicemic Escherichia coli: human and avian pathogens. Curr Opin
Microbiol 9: 28-32.
- Rosen, D. A., T. M. Hooton, W. E. Stamm, P. A. Humphrey, and S. J. Hultgren. 2007. Detection of
intracellular bacterial communities in human urinary tract infection. PloS Med 4: e329.
- Russo, T. A. and J. R. Johnson. 2003. Medical and economic impact of extraintestinal infections due to
Escherichia coli: focus on an increasingly important endemic problem. Microbes Infect 5: 449-456.
- Russo, T. A., A. Stapleton, S. Wenderoth, T. M. Hooton, and W. E. Stamm. 1995. Chromosomal restriction
fragment length polymorphism analysis of Escherichia coli strains causing recurrent urinary tract
infections in young women. J Infect Dis 172: 440-445.
- Schilling, J. D., R. G. Lorenz, and S. J. Hultgren. 2002. Effect of trimethoprim-sulfamethoxazole on
recurrent bacteriuria and bacterial persistence in mice infected with uropathogenic Escherichia coli. Infect
Immun 70: 7042-7049.
- Skjøt-Rasmussen, L., A. M. Hammerum, L. Jakobsen, C. H. Lester, P. Larsen, and N. Frimodt-Møller. 2011.
Persisting clones of Escherichia coli isolates from recurrent urinary tract infection in men and women. J
Med Microbiol 60: 550-554.
- Soto, S. M., A. Smithson, J. P. Horcajada, J. A. Martinez, J. P. Mensa, and J. Vila. 2006. Implication of
biofilm formation in the persistence of urinary tract infection caused by uropathogenic Escherichia coli.
Clin Microbiol Infect 12: 1034-1036.
- Ulleryd, P. 2003. Febrile urinary tract infection in men. Int J Antimicrob agents 22: S89-S93.
4a. Approach to Data Production: Data Generation
5. State the data and resources planned to be generated. (e.g draft genome sequences,
finished sequence data, SNPs, DNA/protein arrays generation, clone generation
etc.)
As we wish to identify novel genetic elements that are potentially unique to certain disease
states, persistence, and spread, we will generate draft de novo genome sequences for all
proposed strains using the Illumina platform. Our experience in sequencing numerous E.
coli strains suggests that a major issue is that many genes of interest, such as those
associated with virulence and antibiotic resistance, are associated with transposable
elements and other repetitive motifs. To overcome this problem, we will use large jumping
library insert sizes (~5 kb) that should enable us to scaffold over the repeated elements.
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 84b. Approach to Data Production: Data Analysis
6. Briefly describe the analysis (value-add) envisioned to be performed subsequently
by the community and the potential to develop hypotheses driven proposals given
the datasets and resources produced by this work.
UTI (Umeå and Køge collections):
Umeå strains: Sequencing and comparison of strains related to cure (n = 37) vs. strains
related to persistence (n = 32) or relapse (n = 46) may reveal genetic factors – so far
unknown – which would be related to cure or relapse. Total sequencing of the bacterial
genomes may reveal genes, clusters of genes such as pathogenicity islands or others that
would differentiate relapsing strains from those found in patients, who were cured by
mecillinam treatment. All strains were susceptible to mecillinam, so resistance towards the
study drug was not an issue.
Køge strains: Sequencing and comparison of strains isolated from male UTI (n = 7+3) and
comparison with female strains (n = 10; and from Umeå, see above) may reveal genetic
factors related to male UTI and recurrent UTI both among men and women.
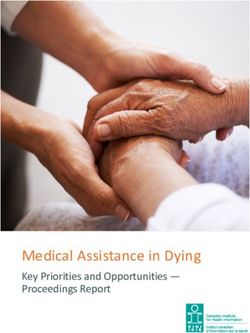
Table 2. Summary of E. coli UTI strains to be sequenced.
E. coli strains Number
Female patients cured 37
Female patients with persisting E. coli 32
Female patients with relapse 46
Female patients with RUTI 10
Male patients with RUTI 3
Male patients with uncomplicated UTI 7
Outcome:
The detection of genes/clusters that are predictable of relapse/persistence would enable
physicians to stratify patients prior to treatment of UTI, so that appropriate treatment could
be directed to patients deemed at higher risk for complications. Such treatments could
include longer duration of antibiotic treatment or choice of antibiotics, which are
particularly effective in curing E. coli infection residing in the bladder. This stratification
could be based on rapid SNP detection or gene presence in the primary culture, which
again would be suggested mandatory in patients with symptoms of UTI at the primary care
level. Currently, many general practitioners do not perform urinary culture in primary care,
but treat the patients empirically with a broad spectrum antibiotic and await whether the
patient is cured or returns with symptoms, where a urine culture is then first performed. A
genomically-informed algorithm such as that suggested could prevent the widespread use
of broad-spectrum antibiotics, currently felt to be fueling the increasing antibiotic
resistance problem, and tailor therapy to each patient.
Further, sequencing of the present strain collection would lead to detailed insight into the
genome of E. coli causing UTI. As described in the Justification section, these data, when
compared to the large commensal collection of E. coli currently sequenced by the Broad
Institute, as well as other E. coli-related disease syndromes, will help us pinpoint the
genetic underpinnings of both male and female UTI infection.
Bacteremia (Hvidovre collection):
Genomic Sequencing Centers for Infectious Diseases: White Paper Form 9The objectives of this study are to characterize E. coli causing bacteremia as a
complication of UTI with respect to the presence of VFs and antimicrobial resistance.
Sequencing of these strains would be a unique opportunity to study and explore possible
differences in the prevalence and distribution of all present bacterial genomic content such
as virulence factor genes, antimicrobial resistance genes etc. among E. coli causing UTI
and bacteremia. Furthermore, the E. coli strains in this collection can be compared with
other E. coli strains – strains from healthy humans and strains causing both uncomplicated
and complicated UTI.
Outcome:
Description of genes or gene-clusters, which are peculiar for E. coli causing bacteremia,
will have several important consequences for handling patients with UTI or bacteremia: i)
Detection of such genes in E. coli isolated in urine from UTI will enable particular
attention to this kind of infection, effective antibiotics to cope with the infection and
prevention of bacteremia. ii) Knowledge of important virulence factors for invasive strains
may lead to preventive measures such as vaccines; iii) The existence of particular E. coli
strains causing bacteremia and originating from UTI may provide the clinicians with one
or more tags, which can enable the detection of the focus of infection causing bacteremia, a
prerequisite for effective treatment of bacteremia.
5. Community Support and Collaborator Roles:
7. Provide evidence of the relevant scientific community’s size and depth of interest in
the proposed sequencing or genotyping data for this organism or group of
organisms. Please provide specific examples.
In light of the novel collections described here, this proposal should be of broad interest to
ID specialists, UTI experts, and those interested in developing diagnostics for primary
care.
8. List all project collaborators and their roles in the project.
Line Skjøt-Rasmussen (Dept. for Microbiological Surveillance and Research, Statens
Serum Institut, Copenhagen, Denmark). Line Skjøt-Rasmussen is performing the PhD-
project regarding virulence in Extraintestinal Pathogenic Escherichia coli based on the
Hvidovre and Køge E. coli strain collections. She will perform analysis and interpretation
of the E. coli genomes, along with the other analyses of this project.
Niels Frimodt-Møller (Dept. for Microbiological Surveillance and Research, Statens
Serum Institut, Copenhagen, Denmark). Niels Frimodt-Møller is supervisor for Line
Skjøt-Rasmussen on her PhD-project and is the major developer of this project. He will
supervise Line during the analysis and assist with interpretation of results.
Karen Ejrnæs (Dept. for Microbiological Surveillance and Research, Statens Serum
Institut, Copenhagen, Denmark; Dept. of Clinical Microbiology, Hvidovre Hospital,
Copenhagen, Denmark; Dept. of Pathology, Herlev Hospital, Copenhagen,
Denmark). Karen Ejrnæs has performed the PhD-project “Bacterial characteristics of
importance for recurrent urinary tract infections caused by Escherichia coli” based on the
Genomic Sequencing Centers for Infectious Diseases: White Paper Form
10Umeå E. coli strain collection. Also, she collected the Hvidovre E. coli strain collection.
She will assist with interpretation of results.
Lotte Jakobsen (Dept. for Microbiological Surveillance and Research, Statens Serum
Institut, Copenhagen, Denmark). Lotte Jakobsen has completed the PhD-project
“Evaluation of the possible association between Escherichia coli from animals and meat
with E. coli causing urinary tract infections in humans” based on the Køge E. coli strain
collection. She will assist with interpretation of results.
Paal Skytt Andersen (Dept. for Microbiological Surveillance and Research, Statens
Serum Institut, Copenhagen, Denmark). Paal Skytt Andersen has experience in whole
genome sequencing, annotation, alignment and will assist and supervise in the analysis of
the genomes.
Bettina Lundgren (Dept. of Clinical Microbiology, Hvidovre Hospital, Copenhagen,
Denmark; The Centre of Diagnostic Investigations, Rigshospitalet, Copenhagen,
Denmark). Bettina Lundgren is supervisor for Line Skjøt-Rasmussen on her PhD-project.
She will supervise Line during the analysis and assist with interpretation of results.
Tor Monsen and Sven Ferry (Department of Clinical Microbiology, Umeå, Sweden).
Tor Monsen and Sven Ferry collected the Umeå strain collection of female recurrent UTI
E. coli strains. They will assist with interpretation of results.
Michael Feldgarden (The Broad Institute). Dr. Feldgarden has organized several large-
scale, GSC-funded population genomics projects, including one focused on ~100 E. coli
commensal genomes. He is also involved with the analysis of the data from these projects.
9. List availability of other funding sources for the project.
Funding of the project has been provided from the Danish Medical Research Council
(grant number 22-02-0373 ct/mp), the Danish Integrated Antimicrobial Resistance
Monitoring and Research Programme (DANMAP), and the University Hospital in
Hvidovre, Copenhagen, Denmark.
6. Availability & Information of Strains:
Genomic Sequencing Centers for Infectious Diseases: White Paper Form
1110. Indicate availability of relevant laboratory strains and clinical isolates. Are the
strains/isolates of interest retrospectively collected, prepared and ready to ship?
Note: If samples are prospectively prepared the GSC can provide protocols and
recommendation based on the Centers past experiences. The samples must however meet
minimum quality standards as established by the Center for the optimal technology
platform (sequencing/ genotyping) to be used in the study.
All strains are readily available and DNAs can be prepared.
11. Attach relevant information, if available in an excel spreadsheet for multiple
samples: e.g.
• Name
• Identifier
• Material type (DNA/RNA/Strain)
• Genus
• Species
• Specimen / Strain
• Isolation source
• Isolated from
• Select agent status
• International permit requirement
• BEIR/ATCC repository accession number
• Other public repository location
• Other public repository identifier
• Sample provider’s name
• Sample provider’s contact
12. What supporting metadata and clinical data have been collected or are planned on
being collected that could be made available for community use?
Available metadata are data concerning the patients’ gender and age, source of the E. coli
isolate (urine or blood) and year of collection.
Genomic Sequencing Centers for Infectious Diseases: White Paper Form
127. Compliance Requirements:
7a. Review NIAID’s Reagent, Data & Software Release Policy:
NIAID supports rapid data and reagent release to the scientific community for all
sequencing and genotyping projects funded by NIAID GSC. It is expected that projects
will adhere to the data and reagent release policy described in the following web sites.
http://www3.niaid.nih.gov/research/resources/mscs/data.htm
http://grants.nih.gov/grants/guide/notice-files/NOT-OD-08-013.html
Once a white paper project is approved, NIAID GSC will develop with the collaborators
a detailed data and reagent release plan to be reviewed and approved by NIAID.
Accept Decline
7b. Public Access to Reagents, Data, Software and Other Materials:
13. State plans for deposit of starting materials as well as resulting reagents,
resources, and datasets in NIAID approved repositories. Sequencing projects will
not begin until the strain is deposited into NIAID funded BEI repository
(http://www.beiresources.org/). This includes web based forms are completed by
the collaborator and received by the NIAID BEI (http://www.beiresources.org/).
All strains current unavailable through public repositories will be deposited at BEI. All
data produced will be published and available to the public.
7c. Research Compliance Requirements
Upon project approval, NIAID review of relevant IRB/IACUC documentation is
required prior to commencement of work. Please contact the GSC Principal
Investigator(s) to ensure necessary documentation are filed for / made available for
timely start of the project.
Investigator Signature:
Investigator Name: Date:
Genomic Sequencing Centers for Infectious Diseases: White Paper Form
13Blank Last Page
14You can also read