TECHNOLOGY IN GAIT REHABILITATION - 2021 MDS-AOS BYUNG-MO OH, MD, PHD - MOVEMENT DISORDER SOCIETY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2021 MDS-AOS
Technology in Gait Rehabilitation
Byung-MO Oh, MD, PhD
Associate Professor
Department of Rehabilitation Medicine
Seoul National University College of Medicine
Seoul National University Hospital
Disclaimer
• I have no financial interest/arrangement or affiliation with any
organization that could be perceived as real or apparent conflicts
of interest related to this presentation.
• Research Grants on Robotic-Assisted Gait Training
– Korea Evaluation Institute of Industrial Technology (No. 10076752),
Ministry of Trade, Industry and Energy, Korea
– Seoul National University Hospital (04-2013-0810)
– Translational Research Center for Rehabilitation Robots (#NRCTR-
EX18009), National Rehabilitation Center, Ministry of Health and Welfare,
Korea.
Learning Objectives After listening to this talk, audience will be able to… 1. Can list more than 3 newly emerging technologies for gait rehabilitation 2. Can tell the difference between the end-effector type and exoskeletal devices 3. Can understand the possible mechanism of robotic-assisted gait training (RAGT) 4. Can summarize the current level of evidence for RAGT on the gait abnormalities in Parkinson’s disease

Contents • Introduction • Robotic devices in Gait Rehabilitation • Other Technologies – Wearable sensors – Virtual reality • Summary

Introduction

Core Components of NeuroRehabilitation
Task-Specific Training
Aerobic Exercise
Medical Care
Prevention and Management of Complication
• Enabled earlier and more
Has any genuine advancement been intensive rehab in more severe
made in neurorehabilitation? patients
• High-Intensity training General
• Standardized training
• Quantitative assessment Medical Care
• Combined with new technologies
(e.g. VR)
Medical
Robotics Technology and
Pharmacological
Armamentarium • Ultrasound-Guided
Intervention
Assistive • Botulinum toxin
• New light-weight material • Use of medication with
• Advanced engineering Devices and proven efficacy
• 3D scanner and printer • Amantadine for TBI
Orthosis • SSRI after stroke
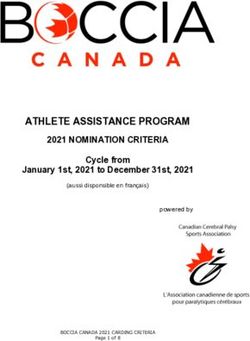
Locomotor activity in spinal man
Dietz V et al, Lancet, 1994
BWSTT in stroke

RAGT
• End-effector based device
– Advantage
• Simple structure, less complicated algorithms
– Disadvantage
• Difficult to isolate specific movements of a particular joint
• Exoskeleton-based device
– Advantage
• Independent, concurrent control of particular movement in many joints
– Disadvantage
• Significant amount of time for setting-up
• Complex control algorithmSNUH Health System
§ SNUH Healthcare System
§ Main Hospital § Children’s Hospital
Gangnam Center
§ Cancer Hospital § Biomedical Research Institute
§ Dental Hospital (~1,800 beds)
Seoul, Korea
§ NTRH Rehab Hospital
(~220 beds)
§ SNU Boramae Hospital
(~800 beds) § SNU Bundang Hospital
(~1,300 beds)Robotic devices in our hospital network
Walkbot (x2) Lokomat (x2) Exoatlet
SUBAR AngelegsRobotic devices
Robotic Devices as Compared to the Human Nervous System
Modulating
Center Higher Level
Control
Slow, Complex or
Decision-Based
Response
Efferent Afferent
system system Central Nervous system
Control system
Quick, Simple or
Patterned Response
Lower Level
Control
Action Information
Muscle, Actuators Sensory organ, SensorsRobotic Devices in Rehabilitation Medicine
Types of Robotic Devices for Gait Rehabilitation
(Exoskeleton type)
Walkbot Lokomat
Reo Ambulator
(End-effector type)
GEO system
(Hybrid type)
ExoWalkWearable Robots in the Market
WalkON Suit ANGELEGS
Hybrid Assistive Indego (SG Mechatronics) (SG Mechatronics)
ReWalk
Limb (Cyberdyne) (Parker Hannifin)
HEXAR-WA20 HEXAR-CR50
Ekso Bionics SuitX (US Bionics) AlterG Bionic Leg (HEXAR systems) (HEXAR systems)Purposes of the Use of Robotic Devices:
Assistive vs. Rehab
Assistive Device Rehabilitation Robot
• Function in daily life • Applied to patients especially in
• Not necessarily related to changes their recovery
in body function • Aim to improve body functionRobotic-assisted gait training in Stroke
RAGT in Stroke • Meta-analysis of 36 studies • RAGT + conventional PT was superior to conventional PT alone in terms of independent gait (OR=1.94, 95% CI=1.39-2.71; p < 0.001). • More effective in patients with severe disability. Mehrholz J et al. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2017;5:CD006185.
Gait speed: favors end-effector type devices
Gait distance:
Favors end-effector type devicesRobotic-assisted gait training in PD
RAGT in PD patients
• A meta-analysis showed short-
term beneficial effect of RAGT in
UPDRS part III, stride length, gait
speed, and balance compared
with conventional PT.
• The improvement were not at
the level of MCID.
Alwardat M et al., Int J Rehabil Res, 2018RAGT vs. treadmill training
• 60 patients with PD (H&Y stage 3)
• 3 groups
– Robotic gait training group (1.0 km/h -> 2.0 km/h)
– Treadmill training group (1.0 km/h -> 2.0 km/h)
– Physical therapy group
• Results
– Robotic training = Treadmill training > Physical therapy (except BBS)
• Robotic gait training is not superior to equal intensity treadmill training for
improving walking ability in mild to moderate PD
Picelli A et al., Parkinsonism Relat Disord, 2013Proposed therapeutic mechanism
• Several repetitions of gait-like movements could act as an external
proprioceptive cue by setting the walking pattern and reinforcing the
neuronal circuits that contribute to gait pacing.
• Robotic training could have also enhanced the automating of motor
control by stimulating the central pattern generators through a greater
activation of hip extensors.
• The augmented physical activity induced by active robotic training
compared with less walking during physical therapy.
Picelli A et al., Neurorehabil Neural Repair, 2012Evaluation of gait automaticity
• Dual-task interference (%)
= (dual task – single task) / single task *100
Rochester L et al., Neuroscience, 201410MWT: single & dual task
Single Dual(cognitive) Dual(physical)Effect of RAGT: A pilot study
Clinical Trials ID: NCT02993042
(12 sessions)
Yun SJ et al., in submissionEffect of RAGT: A pilot study
Table. Changes in the outcome variables between T0, T1, and T2
Within-group
T0 T1 T2 comparisons
(n=11) (n=11) (n=10)
T1 - T0 T2 – T0
1.13 1.24 1.17
Single task .041* .445
(0.23) (0.28) (0.34)
10MWT† Dual task 0.94 0.98 0.92
1.000 .721
(m/s) (cognitive) (0.25) (0.24) (0.26)
Dual task 0.89 0.98 0.90
.075 .721
(physical) (0.22) (0.23) (0.29)
52.00 54.00 54.00
BBS†† .004* .024*
(8.00) (4.00) (5.25)
28.00 30.00 32.50
KFES†† .235 .086
(9.00) (13.00) (15.75)
T0; Before treatment, T1; After treatment, T2; 1 month post-treatment, 10MWT; 10 Meter Walking Test, BBS; B
erg Balance Scale, KFES; Korean version of the Falls Efficacy Scale-International, †Mean (SD), ††Median (IQR
), *pEffect of RAGT: A pilot study
Table. Changes in percentage of dual-task interference (%)
Within-group
T0 T1 T2 comparisons
(n=11) (n=11) (n=10)
T1 - T0 T2 - T0
Dual task -15.78 -.21.50 -20.75
.026* .203
(cognitive) (7.78) (7.62) (6.40)
Step
velocity†
Dual task -21.23 -21.10 -23.51
.929 .646
(physical) (7.42) (5.79) (12.55)
T0; Before treatment, T1; After treatment, T2; 1 month post-treatment, †Mean (SD),
*pAdditional components for gait training
• Virtual reality (Mirelman A et al., Lancet, 2016)
– Intervention combining TT with VR
– TT+VR reduced fall rates compared with TT alone
• Dual-task gait training (Strouwen C et al., Mov Disord, 2017)
– Gait and cognitive task, consecutive vs. integrated
– Both improved dual-task gait velocity without increasing fall risk
• Music-contingent stepping training (Chomiak T et al., Medicine, 2017)
– Auditory playback in real-time upon maintenance of repeated large amplitude stepping
– Increased motor automaticityIn preparation of manuscript
Effect of RAGT: An RCT
• Study design
– Prospective, single-center, single-blind, RCT (Clinicaltrials.gov:
NCT03490578)
Auditory cue Visual feedback
10mWT; 10 meter Walk Test
MDS-UPDRS; Movement Disorder Society-
Unified Parkinson's disease rating scale
BBS; Berg Balance Scale
KFES; Korean version of Fall Efficacy Scale-
International
NFOGQ; New Freezing Of Gait QuestionnaireEffect of RAGT: An RCT
• Intervention
– 45 minutes, 3 times a week for 4 weeks (total 12
sessions)
– RAGT group
• Gait training using an exoskeletal type robot (Walkbot-S)
• Applying individual training velocity protocol depending on
participant’s height
• Auditory cue & visual feedback
– TT group
• Gait training on a treadmill under instruction by a physical
therapist
• Speed was set as identical to RAGT protocolEffect of RAGT: An RCT • Participants CONSORT flow diagram
Effect of RAGT: An RCT
• Estimated marginal means and standard errors of cognitive
dual-task interference at each time points (adjusted)
-30 Dual-task interference, unadjusted (%)
Estimated Marginal Means (%)
Cognitive Physical
RAGT TT RAGT TT
-20
T0 -16.07 ± 13.66 -11.51 ± 11.65 -12.44 ± 13.43 -12.00 ± 17.50
T1 -13.30 ± 9.26 -16.58 ± 9.86 -9.98 ± 8.32 -6.59 ± 9.72
-10
RAGT
TT T2 -15.49 ± 19.77 -16.58 ± 9.84 -10.01 ± 11.04 -8.84 ± 14.13
T1-T0 2.78 ± 13.54 -5.06 ± 14.11 2.46 ± 10.83 5.40 ± 16.33
0 T2-T0 0.59 ± 16.58 -5.06 ± 15.96 2.42 ± 17.87 3.16 ± 21.08
T0 T1 T2
TimeEffect of RAGT: An RCT
• Changes of the brain
corrected (t ≥ 3)
A FA, T1>T0 pEffect of RAGT: An RCT
• Group difference between
functional connectivity
changes
• uncorrected P < 0.001 with cluster-based family
wise error (FWE) rate correction P < 0.05
• 4 nuisance variables: age, gender, UPDRS scores,
existence of FOGFuture direction
Combined with other technologies Overground gait robots
HAL, Cyberdyne GEMS, Samsung SMA, HondaWearable sensors
Trigno, IMU+EMG sensor
PICO, EMG sensor
Actigraph, IMU sensor
Shimmer,
IMU or EMG sensor
Wave Track, IMU sensor
RUNVI, pressure sensor Galaxy gear Apple watch
IMU sensor: fall detection
Physilog, IMU sensorVirtual reality
VR for the Disabled
New experience Rehabilitation
Project Sansar by Linden Lab Rapael Smart Glove by Neofect
Google Earth VR CAREN by Motekforce LinkFully-immersive
RehabWare• Hardware: HTC vive • Rehabilitation program – Hammering – Ball catch – Cup pour – Bubble touch – Playing a xylophone
Fully-immersive
Enriched virtual environment for cognitive rehabilitationFully-immersive
Enriched virtual environment for cognitive rehabilitationSummary
• Robot
– Sensors, Actuators, and Control system
• Types of Robot
– Exoskeleton-based robot
– End-effector based robot
• RAGT in PD
– Can improve walking capacity and balance
• No clear benefit over intensity-matched treadmill training
– May improve gait automaticity with adequate cue and feedback
– May induce the different changes of functional brain networks related to sensorimotor areas
• Future direction of RAGT in PD
– With additional component: dual-task, cue and feedback, VR
– Exoskeleton vs. end-effector vs. hybrid (e.g. overground)
– More severe patient population (e.g. H&Y 4, 5)SNUH Laboratory of Neurorehabilitation
Oh’s (Oz?) Lab
Special thanks to…
TBI
Seoul National University Hospital
Pf. Han-Gil Seo (lecture slides) Virtual
Stroke
Pf. Woo-Hyung Lee (lecture slides) Reality
Seo Jung Yun (lecture slides)
SNU Bundang Hospital
Pf. Jae Won Beom (lecture slides)
Parkinson’s
Robotics
disease
National Traffic Injury Rehabilitation Hospital
Pf. Tae Woo Kim (lecture slides)
Swallowing
Ulsan University
Pf. Seung-Hak LeeYou can also read