Testosterone Therapy in Men with Hypogonadism - (Endocrine Society 2018 Guideline) - UCSF Fresno
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Testosterone Therapy in Men with Hypogonadism
(Endocrine Society 2018 Guideline)
Ngwe Yin, MD
Assistant Clinical Professor of Medicine, UCSF
Fresno Medical Education Program
Feb 2, 2019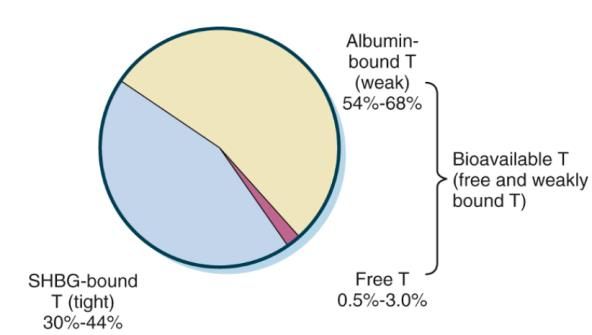
Disclosures • None Feb 2, 2019
Objective
• At the end of the talk, you will be able to
Diagnose androgen deficiency syndromes in men
Choose therapeutic options for patient with diagnosed
androgen deficiency
Monitor during testosterone therapy
Feb 2, 20193 Key Questions • Does the patient have hypogonadism? • If yes, primary or secondary hypogonadism? • Any contraindication to start T therapy? Feb 2, 2019
Case 1 • 44 M was referred for management of hypogonadism • Fatigue, mood changes x 6mo • Morning total T 155.7 ng/dL [Immunoassay] (267-870 ng/dL) at a local lab confirmed with 2nd morning sample • 4 biologic children (wife got pregnant without assistance) • Exam: BMI 28, no gynecomastia, normal testicular exam Feb 2, 2019
Case 1 • What is the appropriate next step? 1. Patient has hypogonadism and start testosterone 2. Confirmed that testosterone assay is accurate and reliable • Total T measured by LC/MS/MS 479 (250-1100 ng/dL), Free T 85 (35-155 pg/ml) • Take home point – assay does matter! Feb 2, 2019
2018 Testosterone guidelines: T assays
• Emphasize on use of
Accurate and reliable assay - equilibrium dialysis or
LC/MS/MS
Lab certified by CDC or another accuracy based certifying
program
https://www.cdc.gov/labstandards/pdf/hs/CDC_Certified
_Testosterone_Procedures-508.pdf
Feb 2, 2019T assays • 1. Immunoassay: a great deal of variability at lower ranges, measures above 250 ng/dL, automated, simple to perform, faster turnaround time, sensitivity and interference issues. • 2. LC/MS/MS: good sensitivity, accuracy and precision especially in the low range, can measure as low as low 20 ng/dL, high level of complexity. • 3. Equilibrium Dialysis: gold standard method for measuring free T, high level of complexity, takes 2 days to perform. Feb 2, 2019
T assays (large interassay & interlaboratory variability)
Immunoassays LC/MS/MS Equilibrium Dialysis
Total T Total T
Quest 250-827 ng/dL 250-1100 ng/dL
Free T (calculated) Free T
18-69 yrs 46.0 – 224.0 pg/mL 69 yrs 6.0 – 73.0 pg/mL >70 yrs 30.0 – 135.0 pg/mL
Total T Total T
LabCorp 264 −916 ng/dL 264 −916 ng/dL
Free T (calculated) Free T (equilibrium ultrafiltration) Free T (equilibrium dialysis)
50-59 yrs 7.2 – 24.0 pg/mL 5.00−21.00 ng/dL 52.0 – 280.0 pg/mL
>59 yrs 6.6 – 18.1 pg/mL
Total T
St Agnes 275 – 781 ng/dL
Free T – send out to Quest
Feb 2, 2019Epic order Feb 2, 2019
Case 2 • 39 M is referred for management of hypogonadism • No energy, fatigue x 3 years and getting worse recently • Lab: Hb 16.9, Hct 48.2%, total T 232 LC/MS/MS (250-1100 ng/dL), Prolactin 5.3, SHBG 7 (10-50), free T 48.9 (35-155 pg/ml) • Normal libido, no decreased erection • Underwent normal puberty, has 3 biologic children (13, 8, 2 years old – wife got pregnant without assistance) • ROS: snoring, daytime sleepiness • Exam: BMI 39, no gynecomastia, well-virilized, normal testicular exam Feb 2, 2019
Case 2 Which of the following is false? 1. Patient likely has OSA and get sleep study 2. Patient has hypogonadism and start T replacement 3. Patient has low total T and SHBG likely due to obesity 4. Relative low total T likely improve if patient loses weight Feb 2, 2019
Diagnosis • 1.1 We recommend diagnosing hypogonadism only in men with symptoms and signs consistent with testosterone deficiency and unequivocally and consistently low serum total T and/or free T concentration (when indicated). • 1.2 We recommend against routine screening of men in the general population for hypogonadism. Feb 2, 2019
Diagnosis
Symptoms and signs consistent with androgen deficiency
2 fasting 8am total T
Free T (if suspect altered SHBG)
LH & FSH
Semen fluid analysis (if fertility issue)
Low T, low or normal LH & FSH Low T, high LH & FSH
Secondary hypogonadism Primary hypogonadism
Pituitary hormones, Transferrin Saturation, MRI Karyotype (Klinefelter syndrome)
Obesity, Opioid, Anabolic steroid use
Feb 2, 2019Diagnosis Specific symptoms and signs Nonspecific symptoms and signs Incomplete or delayed sexual development Decreased energy, motivation, self-confidence Loss of axillary and pubic hair Depressed mood Testes
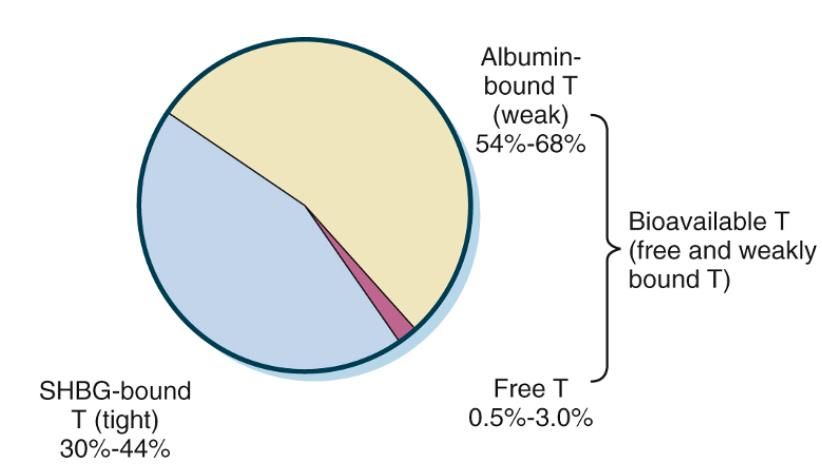
Testosterone Transport • Total T = Free T + albumin-bound T + SHBG-bound T • Bioavailable T = Free T + albumin-bound T • Free Androgen Index = T (ECLIA) : SHBG ratio Feb 2, 2019
Measure Free T • 1. Conditions associated with ↓ SHBG (obesity, DM, glucocorticoid, anabolic steroid use, hypothyroidism, acromegaly, nephrotic syndrome, polymorphisms in SHBG genes) • 2. Conditions associated with ↑ SHBG (aging, HIV, hepatitis, cirrhosis, hyperthyroidism, estrogen, polymorphisms in SHBG genes) • 3. Total testosterone in borderline zone of reference range (eg., 200-400 ng/dL) Feb 2, 2019
Case 3 • 36 M p/w headache, low libido, decreased erection x 4mo, referred for management of hypogonadism • 1 biologic child • Exam: BMI 24, normal secondary sexual characteristics and testicular exam • Morning total T 150 LC/MS/MS (250-1100 ng/dL) x 2 • LH 2.0 (1.0-9.0 mIU/ml) • FSH 3.0 (1.0-13.0 mIU/ml) Feb 2, 2019
Case 3 • Which of the following is next best step? 1. Start testosterone therapy 2. Measure prolactin and pituitary panel 3. Order MRI pituitary w/wo contrast 4. Karyotyping Feb 2, 2019
• Prolactin 4000 (2.0 – 18.0 ng/dL) Feb 2, 2019
Diagnosis • 1.3 In men who have hypogonadism, we recommend distinguishing between primary (testicular) and secondary (pituitary–hypothalamic) hypogonadism by measuring serum LH and FSH. • 1.4 In men with hypogonadism, we suggest further evaluation to identify the etiology of hypothalamic, pituitary, and/or testicular dysfunction. Feb 2, 2019
Diagnosis
Primary Hypogonadism Secondary Hypogonadism
Organic
Klinefelter syndrome Hypothalamic/Pituitary tumor
Cryptorchidism, Anorchia Iron overload syndromes
Chemotherapy Infiltrative disease of hypothalamus/Pituitary
Testicular irradiation, trauma, torsion, Orchiectomy Idiopathic hypogonadotropic hypogonadism
Advanced age
Functional
Medications (androgen synthesis inhibitors) Hyperprolactinemia
ESRD Opioids, anabolic steroid, glucocorticoid
Alcohol, marijuana abuse
Systemic illness
Severe obesity
Feb 2, 2019Case 4 • 44 M with chronic alcohol use p/w gynecomastia, decreased muscle mass x 1 yr • Drank heavily until 2 mo ago, currently drink ½ bottle of vodka a week • 2 children (age 10 and 7) • Exam: +gynecomastia, normal testicular exam • Lab: total T 240 (250-1100), free T 32.4 (35-155), LH & FSH normal, hCG
Case 4 • Next step? 1. Start T therapy 2. Abstinence from EtOH and repeat total T in 3 months • Alcohol is known to cause functional secondary hypogonadism • Therefore, to repeat testing after abstinence from alcohol • Total T improved to 627 ng/dL 6 months of no EtOH • Gynecomastia also improves Feb 2, 2019
Treatment • 2.1 We recommend testosterone therapy in hypogonadal men to induce and maintain secondary sex characteristics and correct symptoms of testosterone deficiency. • 2.2. We recommend against T therapy in men planning fertility or in men with breast or prostate Ca, a palpable prostate nodule/induration, PSA >4 ng/mL, PSA >3 ng/mL combined with a high risk of prostate Ca, elevated hematocrit, untreated severe OSA, severe LUTS, uncontrolled HF, MI or stroke within the last 6 months, or thrombophilia. Feb 2, 2019
Older men with age-related decline in T concentration • 2.4 We suggest against routinely prescribing testosterone therapy to all men 65 years or older with low T. • In men 65 years who have symptoms consistent with T deficiency and consistently and unequivocally low morning T, we suggest that clinicians offer testosterone therapy on an individualized basis after explicit discussion of the potential risks and benefits. Feb 2, 2019
Treatment
Formulation Starting doses Monitoring (measure T)
T enanthate or 150-200 mg IM every 2 weeks Midway between injection (IM)
T cypionate or 75-100 mg IM weekly
T transdermal gel 50-100 mg of 1% 2-8 h following application
1%, 1.62%, 2% 20.25-81 mg of 1.62%
T transdermal 1 or 2 patches (2-4 mg) daily 3-12 h after application
patch
T undecanoate LA 750 mg IM, at 750 mg at 4 wk, at the end of dosing interval
then 750 mg every 10 wk
T pellets 600-1200 mg implanted SC at the end of dosing interval
Feb 2, 20192018 Testosterone guidelines: Monitoring
Assess symptoms respond to treatment At 3 months, each visit
Assess any adverse effects
Serum T (target mid-normal range) At 3 months, dose change, annually
Hematocrit (stop if Hct >54%, evaluate OSA) Baseline, at 3 months, annually
Bone density if osteoporosis Every 2 years
Prostate monitoring (shared decision making) DRE + PSA before initiation
Age 55-69 and age 40-69 who at increased At 3-12 months after initiation, then
risk for prostate Ca who choose monitoring in accordance with prostate Ca
screening guidelines
Feb 2, 2019Monitoring Urology consultation if Increase in serum PSA >1.4 ng/dL within 12 months of initiating T treatment PSA >4 ng/dL at any time Abnormal DRE Substantial worsening of LUTS (lower urinary tract symptoms) Feb 2, 2019
Take home points • Recommends making a diagnosis of hypogonadism only in men with symptoms and signs consistent with testosterone deficiency and unequivocally and consistently low serum T concentrations. • Recommends the use of accurate assays for the measurement of total and free testosterone and rigorously derived reference ranges for the interpretation of testosterone levels. • Recommend confirming the diagnosis by repeating the measurement of morning fasting total T concentrations. • In men determined to have androgen deficiency, we recommend additional diagnostic evaluation to ascertain the cause of androgen deficiency. • We recommend against starting T therapy in patients who are planning fertility in the near term or have any of a number of specified conditions. Feb 2, 2019
References • https://www.endocrine.org/guidelines-and-clinical- practice/clinical-practice-guidelines/testosterone-therapy Feb 2, 2019
You can also read