Vision for Australia's Health - Australian Medical Association's - Australian Medical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Australian Medical Association’s Vision for Australia’s Health

General Public Private A health A health
Practice hospitals health system system for
for all the future
Fostering
Patient
Independence Sustainability Quality medical
empowerment
leadership
June 2021
42 Macquarie Street Barton ACT 2600
Telephone: 02 6270 5400
www.ama.com.au
Please be aware that this document may contain images or names of deceased persons.
Contents
President’s introduction..........................................................................2
Health context...........................................................................................4
Economic context.....................................................................................6
Medical profession context and impact on patients............................8
Core principles........................................................................................10
Policy pillars.............................................................................................12
Pillar 1. General Practice........................................................................14
Pillar 2. Public hospitals.........................................................................18
Pillar 3. Private health............................................................................24
Pillar 4. A health system for all.............................................................28
Pillar 5. A health system for the future................................................36
Endnotes..................................................................................................40
AMA’s Vision for Australia’s Health 1
President’s Introduction
Health reform in this country is sorely needed, Investment requires vision and ethical commitment. We
and long overdue. must invest now to correct critical deficiencies within
the Australian healthcare system. Failure to do so will
If the Australian health system is to evolve, then it
translate into suboptimal outcomes and declining
needs to be reorganised to tackle the challenges
quality of life and access for Australians in the future.
of the future. We cannot expect an underfunded
system to absorb the late-stage complications of an Drawing upon the expertise of our broad member base,
ageing, chronically ill and obese society. Already our the Australian Medical Association (AMA) is uniquely
hospitals, especially our emergency departments, positioned to identify and understand systemic issues
are over-stretched. We cannot keep doing things the in the healthcare system that cut across preventative
same way. health, General Practice, public and private healthcare.
Members provide advice and make policy through
It is realistic for Australia to become the healthiest
committees, state AMAs, and Federal Council; our vision
country in the world, and that should be our
is a product of that significant effort and expertise.
collective aim.
The AMA’s Vision for Australia’s Health represents
We cannot expect to manage the increasing chronic
a clear blueprint for all Governments, and players
disease burden if we do not engage earlier in
in the system, built around five pillars of detailed
prevention and appropriately fund integrated general
policy reform.
practitioner medical homes, as the foundation
for improved care co-ordination across the entire For too long, health reform has been stagnant or
health system. Seminal in this will be the effective piecemeal. The AMA believes now is the time for a
adoption of innovative technologies and an emphasis comprehensive plan to be put forward, funded and
on quality models of care where safety and clinical implemented. The AMA stands ready to lead reforms
appropriateness protect patients. in these areas and is eager to partner with other
organisations, providers, and individuals. Our health
The beginning point of all reform should be safe,
system has responded to the immediate threat of
high-quality, patient-centred care.
COVID-19, while continuing to deliver care. Now is the
We must engage our patients in their own healthcare time for Government to respond and future proof it for
and improve health literacy. We must invest in our the challenges ahead.
medical practitioners to ensure appropriately funded,
efficient, evidence-based practice is at the heart of any
new approach to healthcare.
Dr Omar Khorshid
Federal AMA President
2 AMA’s Vision for Australia’s Health
If the Australian
health system
is to evolve,
then it needs to
be reorganised
to tackle the
challenges of
the future.
AMA’s Vision for Australia’s Health 3
Health Context
stay10. The number of available hospital beds per
Australia’s response to COVID-19 has
1,000 residents aged 65 years or older – an important
been rapid, and largely successful. Our measure of public hospital capacity – has also been in
success owes a lot to our dedicated persistent decline for decades11.
doctors and nurses, but equally, the
Australia’s private health system is also facing challenges.
Australian community. Pre-COVID, from June 2015 to June 2020, private health
insurance membership fell for 20 successive quarters.
There were already warning signs before COVID-19 that Like the broader population, the age of the insured
without reform, our health system was under strain
population is increasing; while Australians aged 75 and
and in danger of producing an inferior outcome for
older have increased their insurance membership by
patients. A rapidly aging population1 has put our health
3 per cent, 25-34 year olds have dropped a full 6 per
system under unprecedented demand. People aged 65
cent, between 2015 and 2018. This creates a cycle of
and over represent 16 per cent of the population but
increasing insurance premiums as insurers seek to
account for 50 per cent of total admitted bed days2.
deal with the increased cost of care per policy holder. It
Chronic disease and injury dominate the Australian
creates a health system out of balance for everyone, with
health landscape, contributing nearly two-thirds of the
a dwindling funding pool12.
overall burden of disease3. Obesity data suggest that 67
per cent of Australian adults and 25 per cent of children Australia has a maldistributed medical workforce. We
are obese or overweight. For Aboriginal and Torres Strait have a chronic shortfall of doctors in rural and remote
Islander peoples, these figures are even higher, at 74 Australia, while more broadly some medical specialties
per cent of adults and 38 per cent of children4. Chronic have an oversupply, and some have an undersupply.
respiratory disease affects seven million Australians, We are training doctors at one of the highest rates
impacting 33 per cent of Aboriginal and Torres Strait in the world, but we have not identified the correct
Islander peoples and 30 per cent of non-Indigenous mechanisms or levers to direct the workforce where it
people5. This complexity burden is increasing6, which is needed, particularly in rural and regional areas where
has implications for the workforce and necessitates the pressure on the public system is exacerbated by low
protection of appropriate training opportunities for rates of private health insurance and private practice.
medical practitioners.
General Practice is one specialty where training has been
Mental health represents an increasingly large undersubscribed for three consecutive years. Australia’s
proportion of the health system; 8.7 million (45 per cent) GPs are a central component of our health system but
of Australian adults will experience a mental disorder in the extent of successive funding reductions in General
their lifetime7. Data suggest the rate of having a common Practice and loss of focus on this critical, unique function
mental disorder is 4.2 times higher for Aboriginal and they fulfill, has diminished the coordination of care and
Torres Strait Islander peoples than for the general endangered outcomes for patients. Primary healthcare
population8. Many health professionals, including GPs, professionals control or influence approximately 80 per
psychiatrists, and emergency physicians, are witnessing cent of healthcare costs, with 83 per cent of patients
significant growth in the number of patients seeking seeing a General Practitioner (GP) each year. Yet
treatment and support for their mental health. Due spending on General Practice accounts for only 8 per
to decades of under-resourcing and under-staffing, cent of total government health spending.13
public mental healthcare services were struggling to
In 2017-18, 7 per cent of all hospitalisations were due
deliver accessible and high-quality care before the
to 22 preventable conditions that could be managed by
pandemic crisis.
General Practice. This accounted for almost 3 million
Australians are waiting longer for public hospital elective bed days14. The increased prevalence of chronic health
surgery, with the median wait time before COVID-19 conditions has greatly increased the demand for
(2018-19) of 41 days, eight days longer than in 2008-09. It and cost of treatments15. But with sufficiently funded
is our worst performance on this measure since 2001- longer consult item numbers GPs could have the time
029. Likewise, our public hospital emergency system and resources to spend with patients with complex
access block continues to worsen, increasing emergency conditions, which would deliver major improvements for
department overcrowding which is associated with the health system.
increased mortality, morbidity and length of hospital
4 AMA’s Vision for Australia’s Health
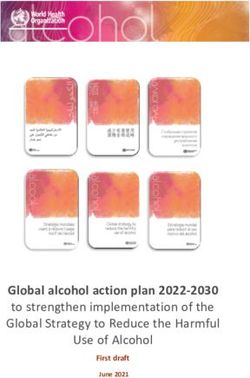
38 8.7
Due to decades of
%
under-resourcing
and
under-staffing,
of the
chronic disease burden public
MILLION mental
in Australia
could be AUSTRALIAN ADULTS healthcare
prevented will experience a services
through a reduction in were struggling to deliver
modifiable risk factors such as mental disorder accessible and high-quality care
overweight and obesity and before the pandemic crisis.
insufficient physical activity.
in their lifetime.
In 2018-19 more than
8.3 million patients
presented to a public hospital
emergency department – an increase
of 4.2 per cent on the previous year.
7%
In 2017-18,
Primary healthcare professionals
control or influence approximately 7% of all
We are training doctors at 80 per cent hospitalisations
one of the of healthcare costs, with were due to 22 preventable
highest rates 83 per cent conditions that could be managed
by General Practice.
of patients seeing a GP each year.
in the world, This accounted for almost
but we have not identified the
correct mechanisms or levers
to direct the workforce where it 3 million bed days
is needed.
AMA’s Vision for Australia’s Health 5
Economic Context
restrictions and demands required for a COVID-19
The COVID-19 pandemic remains a
existence. This will require an expansion of our health
critical reminder of the importance of
system to respond to increased demand, recognising
health investment as the best spend a however that many Australians have been financially
government can make for its people, impacted by the pandemic.
and its economy.
Prior to the pandemic, Australia’s health spending was
9.3 per cent of GDP — less than many similar countries,
With a significant increase in national deficits, it is
and close to half of the USA with its managed care
reasonable to expect that the ability of the Government
model. It’s clear our health funding provides a strong
to fund significant new health expenditure will be
return on investment. The opportunity now exists to
constrained, and the dubious temptation may be to
invest further into the reforms shown to be efficient
cease new spending, and instead search for savings
and effective, such as integrated General Practice,
by cutting services or delaying necessary innovation.
telehealth and e-prescribing. It is important to recognise
But now is not the time to reduce spending on
that the health sector is also a major employer, and
healthcare. A healthy society is a critical component of
therefore investment in health has an additional benefit
a healthier economy.
in increasing economic activity and employment.
As Australia continues to suppress COVID-19, the
We also need to fix the historical underinvestment in
health system will need to be ready to deal with dual
health. Average Weekly Earnings increased by 4 per
challenges: low-level infections and outbreaks, as well
cent per year from 1995 to 2020, and practice costs for
as ‘pent-up’ demand for non-pandemic healthcare
General Practice for example, rise by the same amount,
compounding routine activity. There are significant
with health inflation also 4 per cent16.
unrealised consequences of delayed care and
worsening health conditions. Medicare rebates only increased by 1.2 to 2.5 per cent
between 1995 and 2012, before the recent Medicare
There are fundamental changes needed to
freeze prevented indexation completely, furthering the
accommodate ongoing disease identification, testing,
erosion of rebate values into the future17. This impacts
infection control and suppression in our health system.
practice viability and affordability for patients and will
The patient flow through health systems needs to be
only be more severe in harsh economic climates.
reconsidered, with appropriate resources, funding
and infrastructure provided to accommodate the
6 AMA’s Vision for Australia’s Health
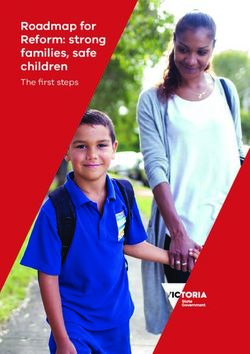
Pre-COVID, from June 2015 to June 2020,
+3
Australians
%
private health
aged insurance membership
75 and fell for 20 successive quarters.
Australians
older aged
25-34
-6%
The age
of the insured
population
is increasing,
with Australians aged 75 and
older increasing their insurance
membership by 3 per cent, while
25-34 year olds have dropped
a full 6 per cent, between 2015
and 2018.
Organisation for Economic Co-operation
and Development (OECD) data indicates that
countries who were more successful
at containing the COVID-19 virus
are economically better off.
Source: Smithson, M. (26 November 2020). “Data from 45 countries show containing COVID vs saving the economy is a false
dichotomy.” The Conversation. Retrieved 21/01/2021 from: https://theconversation.com/data-from-45-countries-show-containing-
covid-vs-saving-the-economy-is-a-false-dichotomy-150533
Median waiting time for elective surgery (days) - all States and Territories
Australians are waiting longer for public hospital elective surgery,
with the median wait time of 41 days - eight days longer than in 2008-09.
Source: Australian Institute of Health and Wefare (AIHW). Elective surgery data cubes (2001-02 to 2006-07): Australian hospital statistics. Australian Institute of Health and Welfare (AIHW). Elective
surgery waiting tims (2007-08 to 2018-19): Australian hospital statistics.
AMA’s Vision for Australia’s Health 7
Medical Profession
Context and Impact
on Patients
want to work in the right areas to meet community
The reforms in this document are
healthcare needs.
designed to improve the operation
of the health system for patient and GPs increasingly feel disconnected from the rest of
the health system and curtailed in their ability to
practitioner alike.
efficiently manage a patient’s care through the life
They respond to the experiences of our members, cycle. Despite being at the centre of the medical
the insights offered by our patients, and the lessons system, expansions in the scope of practice in allied
health, an increasingly fractured model of health
learned from our rapid reform to respond to
service delivery, and extreme financial pressures mean
COVID-19. They embody the principles of building
the next generation of GPs face significant challenges.
a sustainable, inter-connected, high-quality health
Meanwhile the current generation feel beleaguered
system that provides access for all, with leadership
and under-appreciated, lamenting the lack of focus on
and independence of the medical profession, while
prevention and innovation.
empowering our patients. It is not only possible, but
absolutely necessary, to ensure that any reforms to the Our hospital doctors deal with the most complex
health system support our doctors – for otherwise we life-saving treatments, 24 hours a day, seven days
will fail to improve the health of Australia’s patients. a week. Yet the AMA’s research has shown many
doctors are working dangerously unsafe hours, putting
Australia’s medical practitioners have shown
them at a higher risk of fatigue to the extent that it
themselves to be adaptable, knowledgeable and
could impact on performance, and affect the health
resilient in times of need within the healthcare system.
of the doctor and the safety of the patient. Patients
But Australia’s doctors face some significant challenges
continue to wait longer for treatment. Aboriginal and
resulting from COVID-19, which are compounded by Torres Strait Islander doctors continually experience
our current policy and funding settings. Public hospitals instances of racism and discrimination from patients
are already operating at dangerously high capacity, and peers, which impacts the cultural safety of
and this could be made worse by people presenting hospitals and clinics18. Funding agreements continue
with late-stage disease following a reluctance to attend to drive quantity and haste, not quality and training.
hospital (e.g. to partake in cancer screening) at the
The prolonged COVID-19 shutdown, financial
height of the pandemic.
pressures stemming from insurer changes, and
COVID-19 has also had significant impacts on trainee reduced private health coverage threaten access
progression and therefore the workforce pipeline to the critical private health pillar of the system.
into the future. Beyond COVID-19, we have medical Complicated, variable insurance policies often leave
training shortfalls in key areas, and significant areas patients confused and unknowingly underinsured, or
of workforce maldistribution. At the same time, we significantly out of pocket. Practitioners often bear the
have a projected oversupply of medical students in brunt of a system in need of urgent further reform.
some specialty disciplines, creating significant training In addition, the private system has not been funded
pressures and negatively impacting our ability to train to adapt to the ongoing changes needed to deal
the right number of doctors in the right specialties who with COVID-19.
8 AMA’s Vision for Australia’s HealthAMA’s Vision for Australia’s Health 9
Core Principles
Core Principles for a Stronger Health System:
The AMA’s vision is underpinned by core
principles that the AMA considers necessary for
any success in health reform.
Access to appropriate Independence of the Sustainability of the
healthcare for all medical profession by: medical workforce and
Australians by: healthcare system by:
• Ensuring accessible, integrated,
• Accessible, integrated, navigable navigable and convenient • Acknowledging the diversity of the
and convenient medical-led care, medical-led care, coordinated medical workforce and assuring
coordinated through nominated through nominated General doctor satisfaction with work
General Practice. Practice. conditions. Providing conditions
• Protecting the health system that are safe and free of bullying
• Informed by the COVID-19
from any form of funder-led, and discrimination, ensuring an
experience, a new approach
managed care. environment that is free from
to health coordination across
racism, and promoting greater
jurisdictions, with doctors • Ensuring the future of private representation of women.
leading well-coordinated practice — promote a system
patient-centered care within and supported with fair Medicare • Promoting efficient use of resources
across health systems, (enhanced and private health insurance and cultivating systems/targets that
by technology). patient rebates. use healthcare resources efficiently
with reduction in waste.
• Patient-centered focus on • Building a system that is efficient,
prevention and wellness with transparent and accountable with • Acting on health determinants
engagement in care. a focus on evidence-based care. beyond the control of the healthcare
system, particularly climate impacts
• Specific consideration of
and social determinants of health.
Indigenous Australians, and those
impacted by economic downturn. • Providing a vision of Australia’s
future medical workforce, with clear
• Investment in models of care that
training pathways and solutions
improve geographic variation in
to rural medical workforce needs
healthcare opportunity.
and distribution.
10 AMA’s Vision for Australia’s HealthQuality of the medical Patient empowerment to Fostering medical
system by: ensure that people can take leadership by:
charge of their health by:
• Embracing data and international • Recognising enhanced safety
evidence to improve quality, rather • Ensuring choice within the private and efficiency in healthcare
than taking a punative approach system by making it affordable for systems resulting from
based on existing policy or funding more Australians. investment in empowering diverse
constraints of new technology. medical leadership.
• Striving to introduce technology
• An ongoing profession-wide that promotes engagement, • Enhancing training opportunities
commitment to excellence and interaction and access as well as for medical practitioners to develop
patient-centred care. literacy. management and leadership skills
to complement clinical expertise.
• Introducing new technologies • A concerted push for public health
that deliver doctors’ and patients’ and prevention activities aimed at • Building a positive work culture
health information seamlessly preventing illness from occurring. through system design, leading
across different parts of the by example to promote equity,
• Recognising environmental and
health system. diversity, reward for effort, expertise
social determinants of health in
in training/research/administration,
• Committing to appropriately policy development.
and actively managing bullying and
resourced and accessible teaching
harrassment.
and research.
• Supporting the appointment of
professionally trained and qualified
specialist medical administrators in
medical leadership roles.
• Ensuring doctors are trained in and
appointed to positions in clinical
governance, workforce planning
and wellness.
AMA’s Vision for Australia’s Health 11Policy Pillars
The AMA’s Vision for Australia’s Health
represents a clear blueprint for all Governments,
and players in the system, built around five
pillars of detailed policy reform.
Pillar 1: General Practice Pillar 2: Public hospitals Pillar 3: Private health
Integrated, multi-disciplinary GP An evolved and adequately funded A reinvigorated and resilient private
led patient-centred medical homes public hospital sector, providing health system, which complements
represent the foundation of an for timelier elective and emergency the public hospital system by
evidence-based healthcare system. treatment, greater linkages to providing high-quality, timely and
This is underpinned by increased primary care and more transparent affordable care in a sustainable
funding rewarding quality, as well and simplified Commonwealth-State way. Demographics, chronic
as industry and expertise to achieve funding arrangements. Key to disease, technology, and healthcare
the most cost-effective optimisation this will be striking the right are all changing rapidly, and our
of health outcomes for patients and balance, so our focus is patient policies must change accordingly.
families, regardless of geography. care and improving outcomes, and Having cleared the first hurdles
This focuses on management of reforming burdensome audit and for telehealth and home-based
chronic and/or complex diseases, accreditation requirements which hospital care, we need to develop
reduction in preventable hospital can, if poorly designed, detract them further as part of a deliberate
admissions and improved from limited resources. A new design of a better system. A system
stewardship of resources, including funding approach to supplement that provides the right programs
in the aged care sector. Equally, it is the current focus on activity-based which are cost effective, clinically
important to recognise that General funding – one that includes funding advantageous, medical practitioner
Practice is critical to aged care for positive improvement, increased led and insurer funded. One that
services and mental health services capacity, and reduced demand, and focuses on continual improvement
– two significant and growing puts an end to the blame game. – including, but not limited to
health areas. prostheses reform, addressing the
issue of private patients in public
hospitals, new and improved clinician
led models of care and the adoption
of new technology.
12 AMA’s Vision for Australia’s HealthPillar 4: A health system Pillar 5: A health system for
for all the future
A sustainable health system achieved Embracing new technology and
via policy and sustainable funding innovation, consolidating the
reform to ensure: gains from COVID-19 reforms, and
building upon them to facilitate
• prevention becomes a foundation
better access for all patients
of healthcare planning and design;
and greater understanding and
• access for all Australians remains a engagement between patients and
key feature of our system, including practitioners. It will also require
identifying and filling service gaps better use of data and technology
for: Aboriginal and Torres Strait to aid diagnosis, clinical audit
Islander peoples, people living and patient engagement, and to
in aged care settings, and other provide solutions to deliver care in
vulnerable groups, in conjunction circumstances currently not possible.
with the National Disability Key to consideration of a future
Insurance Scheme; health system is the opportunities
• emphasis is placed on key offered by new innovative models of
environmental, social and moral care, integrated care at a lower cost
determinants of health; and and value-based healthcare – that is,
sustainable system redesign.
• efficiencies in care are identified,
with reduction in waste and
savings reinvested.
AMA’s Vision for Australia’s Health 13Pillar 1.
General Practice
Integrated, multi-disciplinary GP led
patient-centred medical homes represent the
foundation of an evidence-based healthcare
system. This is underpinned by increased
funding rewarding quality, as well as industry
and expertise to achieve the most cost-effective
optimisation of health outcomes for patients
and families, regardless of geography. This
focuses on management of chronic and/or
complex diseases, reduction in preventable
hospital admissions and improved stewardship
of resources, including in the aged care sector.
Equally, it is important to recognise that
General Practice is critical to aged care services
and mental health services – two significant and
growing health areas.
14 AMA’s Vision for Australia’s HealthAMA’s Vision for Australia’s Health 15
Pillar 1: General Practice
GOALS ENABLERS OUTCOME MEASURES
1.1 Implement • Embed the concept of the patient- • 80 per cent of all patients have a
voluntary GP centred medical home in Australia. nominated General Practice by end
nomination, allowing of 2022.
• Improve the coordination of long-term
all patients to
care for patients, leading to improved
nominate their
healthcare outcomes for patients.
preferred or regular
GP/General Practice.
1.2 Medicare • More flexible access to care for patients. • Number of new telehealth MBS items
Benefits Schedule and their uptake by General Practice.
• Cost and mobility barriers for patients
(MBS) rebates for
are improved, including the need to
GP telehealth via a
take time off work, travel and pay
patient’s nominated
for travel – thus helping the most
General Practice
vulnerable in our society.
are available for all
clinically appropriate • Improved productivity in both
circumstances where a General Practice as well as
face-to-face visit is not the broader workforce, where
required/possible. telehealth is appropriate and
infrastructure provided.
1.3 Improve access • Link Medicare Chronic Disease • Improved management of chronic
to GP coordinated Management and health assessment disease in General Practice.
community care items to voluntary patient nomination
• Reduction in avoidable
for patients. from 2021.
hospital admissions.
• Introduce an extended ‘Level B’
• Reduction in some
consultation to allow greater routine
preventable presentations at
care of more complex patients without
emergency departments.
disrupting current routine care.
• Measurable increase in average GP
• Restructure MBS consultation items
consultation times via an established
to remove the current remuneration
and agreed methodology and
bias so that longer, more complex
mechanism, noting the loss of the
consultations are better valued.
Bettering the Evaluation and Care of
• Support patients with hard to heal Health (BEACH) reporting.
wounds by funding the costs of
• Increased access to after-hours care
dressings for targeted patient groups.
by patients.
• Improve Medicare funding
arrangements for after-hours GP
services provided by a patient’s usual/
nominated General Practice.
1.4 Lift caps on • Enhanced access to GP-led team-based • Increased employment of nurses,
subsidies available care for patients. pharmacists and allied health
through the professionals in General Practices.
Commonwealth
Department of
Health’s Workforce
Incentive Program.
16 AMA’s Vision for Australia’s HealthGOALS ENABLERS OUTCOME MEASURES
1.5 Improved access • Greater access to GPs in nursing • Significant investment in funding
to GP care for elderly homes, improved management models that better support the delivery
patients through their of health conditions, falls of GP services in nursing homes.
usual GP, ensuring reporting, polypharmacy.
continuity of care.
1.6 Introduction of • General Practice perceived as a more • GP trainees have equivalent
the Single Employer attractive career option for graduating working conditions to their
Model for GP trainees, medical students and doctors hospital-based colleagues.
offering competitive in training.
• GP training meeting its annual
remuneration and
• Reverse the decline in recruitment to recruitment targets.
working conditions for
the GP training program and ensure
GP trainees. • Sustainable growth in GP numbers,
that Australia has a strong GP-led
matched to community need.
primary care system.
• Increased desire of medical students to
choose a General Practice career upon
leaving medical school.
• Introduction of the Single Employer
Model for GPs in Training by start of
2022 or 2023.
• All Australian General Practice Training
(AGPT) spots filled nationally, with
surety to prioritise and incentivise rural
placements and areas of workforce
shortage to meet community needs.
1.7 General Practice • Targeted annual rounds of • Number and take-up of
funded and resourced infrastructure grant funding to support grant opportunities.
to transform and training and multi-disciplinary care in
• Adoption of new technology in
innovate. General Practice.
General Practice including point of
• Funding support through the Practice care testing, video consultations and
Incentive Program and the MBS that remote monitoring.
enables the adoption of innovative
• Conversion to 50 per cent
models of care including telehealth,
e-prescriptions by end of 2022.
point of care testing and remote
monitoring of patients. • Enhanced My Health Record
upload rate.
• Funding for ACCHOs infrastructure and
practice beyond COVID-19 prevention. • Increased facilities and infrastructure
at ACCHOs.
• Improved access for rural and regional
areas and disadvantaged communities.
AMA’s Vision for Australia’s Health 17Pillar 2.
Public Hospitals
An evolved and adequately funded public
hospital sector, providing for more timely
elective and emergency treatment, greater
linkages to primary care and more transparent
and simplified Commonwealth-State funding
arrangements. Key to this will be striking the
right balance, so our focus is patient care
and improving outcomes, and reforming
burdensome audit and accreditation
requirements which can, if poorly designed,
detract from limited resources. A new funding
approach to supplement the current focus
on activity-based funding – one that includes
funding for positive improvement, increased
capacity, and reduced demand, and puts an end
to the blame game.
18 AMA’s Vision for Australia’s HealthAMA’s Vision for Australia’s Health 19
Pillar 2: Public Hospitals
GOALS ENABLERS OUTCOME MEASURES
2.1 Simplified funding • Greater responsibility for all • Patients do not remain in emergency
arrangements, Governments with equal funding departments after decision to admit.
which see the commitment to activity. • Reduced waiting times for elective
Commonwealth surgery and emergency admissions.
• State and Territory Governments
increasing their
benefit from a 5 per cent increase in • No overcrowding of emergency
contribution to 50
funding, but are required to invest these departments and improved hospital
per cent for activity
additional funds into improved capacity flow, with elimination of access block
(as per current
and quality of care. in emergency departments.
COVID-19 partnership
agreement), as well • Elimination of ambulance ramping.
as providing funding • Hospitals are funded to resolve the
for improvement and cause of complications and adapt
capacity. The States future workflow, resulting in fewer
and Territories could patient complications, re-admissions
use the 5 per cent and shorter length of stay – rather
of ‘freed-up’ funds than a penalty approach.
on improvement,
• Improved efficiencies and
as determined by
patient throughput.
the needs of the
region/ network. • Compliance with industrial conditions
that facilitate doctors’ health and
2.2 Commonwealth • Commonwealth funding is fully indexed, safety, education and training and
and State and and additional funding is made available, quality of patient care delivery.
Territory funding so that hospitals are resourced to
increase capacity as needed and invest • Residual and surge capacity in our
at a sufficient scale
in improving their performance. A shift in health system. This is essential
to allow increased
focus from penalising struggling hospitals both to maximise efficiency in the
capacity and growth, setting of entirely predictable normal
operating at breaking point, to resourcing
beds where needed, surges, but also to accommodate for
hospitals for scalable, efficient and
and improved improved care. predictable future pandemics and
performance. This disasters. Residual capacity that is
• Hospitals are funded so that staff are not
means funding that is working unsafe hours and overtime is not used every day can be invested
appropriately indexed recognised and rewarded. back into improving quality, culture,
and incentivises • Funding to support investment and teaching, training and research.
positive outcomes. wellness of hospital staff, including
fostering medical leadership in hospital
administration and management.
• Funding to adapt to post-COVID-19
healthcare, allowing implementation of:
• Methods of managing patient flow
in light of social distancing and
infection control;
• Additional infrastructure and
modifications to ensure safety for
healthcare staff, patients and visitors;
and
• Surge facilities and Personal Protective
Equipment (PPE) in case of winter spike,
and to deal with increased testing
requirements during winter months.
20 AMA’s Vision for Australia’s HealthGOALS ENABLERS OUTCOME MEASURES
2.3 Transition of • Scalable, simplified and transparent • Measurable reduction in
Medicare public funding that significantly reduces the administration costs, with savings
hospital outpatient administration workload within public reinvested into clinical care.
clinic funding to an hospitals to capture Medicare income.
appropriately indexed
funding system.
2.4 Deeper • Hospitals provide best practice, full • Lower emergency presentations and
connections between discharge summaries and seamless re-admissions, post-discharge.
General Practice and integration of clinical systems between
• Greater management of chronic
public hospitals, with hospital and community to facilitate
patients in the community.
appropriate funding information sharing.
provided. • GP download rate of hospital
• Governments fund improved delivery
discharge summaries
of integrated care post-discharge
to prevent avoidable admissions,
co-designed with the profession.
• Improved integration of medical care to
nursing homes, hospital in the home,
and GP integration pre-discharge.
2.5 Alternative • Adopt digital health technologies to • Reduced re-admission rates
delivery options for maintain clinical connections with post-discharge for vulnerable
outpatient care. vulnerable patients post-discharge. patients.
• Expand hospital in the home services for • Reduced cost and improved quality of
simple treatments that otherwise require patient care.
hospital admission.
• Increased GP satisfaction with
• Invest in communications channels hospital communication.
to facilitate quality and efficiency
across health spheres – GPs, hospital,
aged care.
2.6 Expanded uptake • Telehealth is an integral part of care • Reduced patient acuity for chronic
of telehealth across delivery across hospital networks. disease patients and reduced
hospital networks. complications if admission
• Deeper connections between public
is required.
hospital clinicians and primary care
services across hospital networks.
AMA’s Vision for Australia’s Health 21GOALS ENABLERS OUTCOME MEASURES
2.7 Regulation change • Enhanced fully informed financial • Increased transfer of patients
to ensure patient is consent provided to patients before from public hospital emergency
offered choice when proceeding with care. departments to private hospitals for
presenting for care, ongoing inpatient care.
• Increase in genuine attempts to allow
and availability of
patients holding private hospital • Greater coordination and streamlining
private sector options
insurance to transfer care to a private of the system, including timely patient
are investigated
facility where spare capacity exists in transfers to private emergency
and discussed with
order to unburden the public hospital department facilities.
patients holding
system for patients without insurance.
credible private
hospital insurance • Regulation change to prevent public
cover. This to hospitals from advertising to patients
be documented in order to pressure them to use their
before public private health insurance in public
hospital admission. hospitals to enhance system capability
or resourcing.
2.8.1 Ensure adequate • Ensure appropriate training via the • More appropriate policy, and
representation RACMA or equivalent as a basis for all importantly implementation, that
and diversity of medical leadership roles. does not impact negatively on patients
practicing medical or practitioners, while reflecting the
• Medical responsibility for health and
practitioners from the specific requirements of differing
workplace culture within organisations
full range of public medical environments.
recognised at executive level.
and private services,
• Hospital accreditation process
on government • Recognition that diversity is essential
amended or introduced.
working groups for quality of leadership and
and committees. organisational performance. • Increase in appointments of Executive
Director of Medical Services in line
2.8.2 Hospital • Hospital accreditation to require further
with these criteria.
accreditation training for current medical leaders in
requirements for management and healthcare policy, and
a fully empowered identification of new medical leaders.
executive director of
medical services (or
equivalent) who is a
registered medical
practitioner with a
Fellowship of the
Royal Australasian
College of Medical
Administrators
(RACMA), to have
responsibility for
clinical service
delivery, safety/quality
and credentialing
within each hospital.
22 AMA’s Vision for Australia’s HealthGOALS ENABLERS OUTCOME MEASURES
2.9 Accreditation of • Postgraduate Medical Council (PMC) • Accreditation by PMC of all
all pre vocational accreditation of pre vocational training postgraduate year 2+ training places
training years for prior to vocational training would by end of 2023.
junior doctors. provide a structured, safe, high-quality
training experience for all doctors.
AMA’s Vision for Australia’s Health 23Pillar 3.
Private Health
A reinvigorated and resilient private health
system, which complements the public hospital
system by providing high-quality, timely
and affordable care in a sustainable way.
Demographics, chronic disease, technology,
and healthcare are all changing rapidly, and our
policies must change accordingly. Having cleared
the first hurdles for telehealth and home-based
hospital care, we need to develop them further
as part of a deliberate design of a better system.
A system that provides the right programs
which are cost effective, clinically advantageous,
medical practitioner led and insurer funded.
One that focuses on continual improvement –
including, but not limited to prostheses reform,
addressing the issue of private patients in public
hospitals, new and improved clinician led models
of care and the adoption of new technology.
24 AMA’s Vision for Australia’s HealthAMA’s Vision for Australia’s Health 25
Pillar 3: Private Health
GOALS ENABLERS OUTCOME MEASURES
3.1 Recalibrate • A private health insurance system that • Increasing numbers of younger people
the private health offers affordable and appropriate cover taking up private health insurance
insurance policy within reach of all Australians. hospital cover.
levers around rebates,
• Enhanced levels of membership for • Greater retention of existing
Lifetime Health Cover
younger Australians. policy holders.
(LHC) loading, and
Youth Discounts • Greater incentives to hold private health • Reduced premium inflation due
to account for the insurance among older Australians and to a rebalanced and sustainable
ageing demographic existing policy holders. insurance pool.
and changing • Measures to assist people, especially
insurance pool. through the COVID-19 period by
extending the age allowed under family
policies, and pausing LHC loadings
for those impacted by COVID-19
related losses.
3.2 Engage in further • A minimum threshold level of premiums • Reduced number of complaints
policy reform to returned to the health consumer to Ombudsman about benefits,
put greater value as health benefits, i.e. payout ratio membership and service.
and protections minimum of 90 per cent.
• A greater proportion of premiums being
into private health
• A higher standard of transparency paid towards benefits, not management
insurance in the eyes
for private health insurance policies expenses or profit taking, instilling
of consumers.
to clarify what benefit rates are, greater consumer confidence in
so patients can determine their for-profit insurers.
out-of-pocket costs.
• Protection against managed care,
• Lower levels of variation between which has been shown to lead to
private health insurance rebates. increased costs.
• An independent regulator to regulate • A higher standard of transparency for
the legal conduct of the private health private health insurance policies to
insurance industry. clarify benefits and reduced number of
patients experiencing “bill shock”.
• Consider and adapt for the additional
costs of responding to COVID-19 in the
long term.
• Add private health insurance rebates on
to the Commonwealth Government’s
doctors’ fees (Medical Costs
Finder) website.
26 AMA’s Vision for Australia’s HealthGOALS ENABLERS OUTCOME MEASURES
3.3 Ensure patient • Invest in developing new medical-led, • Increased number of medical
choice and medical-led innovative models that will ultimately services being carried out in the most
care remains central, create new best-practice care. This clinically appropriate and efficient
while also developing should include adoption of new settings, including home-based care,
new models of technology to support care provision, community-based care and other
more efficient including community-level care where non-admitted day programs.
care and reducing clinically appropriate.
• Ongoing efficiency and cost savings
low-value care.
• An independent regulator to oversee related to acute treatment.
the legal conduct of the private health
insurance industry and guard against
insurer-directed care.
• Consider potential cost savings and
efficiencies in other areas of outlays
such as devices/prostheses.
3.4 Hospital • Ensure appropriate training via RACMA • Hospital accreditation process amended
accreditation or equivalent as a basis for all medical or introduced.
requirements for leadership roles.
• Increase in appointments of Executive
a fully empowered
• Medical responsibility for wellness and Director of Medical Services in line with
executive director of
workplace culture within organisations these criteria.
medical services (or
recognised at executive level.
equivalent) who is a
registered medical • Hospital accreditation to require further
practitioner with a training for current medical leaders in
Fellowship of RACMA, management and healthcare policy, and
to have responsibility identification of new medical leaders.
for clinical service
delivery, safety/quality
and credentialing
within each hospital.
AMA’s Vision for Australia’s Health 27Pillar 4.
Health for All
A sustainable health system achieved via policy
and sustainable funding reform to ensure:
• prevention becomes a foundation of
healthcare planning and design;
• access for all Australians remains a key feature
of our system, including identifying and
filling service gaps for: Aboriginal and Torres
Strait Islander peoples, people living in aged
care settings, and other vulnerable groups,
in conjunction with the National Disability
Insurance Scheme;
• emphasis is placed on key environmental,
social and moral determinants of health; and
• efficiencies in care are identified, with
reduction in waste and savings reinvested.
28 AMA’s Vision for Australia’s HealthAMA’s Vision for Australia’s Health 29
Pillar 4: Health for All
GOALS ENABLERS OUTCOME MEASURES
4.1 Prevention of • Increased funding directed towards • Five per cent of total health
illness becomes preventative health. expenditure dedicated to
a foundation of illness prevention.
• A tax on sugar sweetened beverages.
Australia’s health
• Number of GP MBS items dedicated to
system policy and • GPs at the centre of preventative
preventative health.
funding response health system design.
in the immediate • Funding to establish a CDC.
• Increased Medicare rebates and
future. improved indexation to lessen patient • Application of best-practice principles
out-of-pocket costs and encourage of infection prevention, control
greater access to medical services. and treatment of COVID-19, which
reflect continuously evaluated
• An Australian Centre for Disease
emerging evidence.
Control (CDC) is established with
a focus on current and emerging • Increased prevention and identification
communicable disease threats, and of disease at earlier stages.
to engage in global health surveillance,
• Reduced acute demand on
health security, epidemiology,
hospital facilities.
and research.
• Evidence of improved patient
• Maintain the funding and support
experience and flow through the
needed for each sector of the health
health system.
system to remain vigilant in response
to COVID-19, while allowing treatment
and prevention services to run.
30 AMA’s Vision for Australia’s HealthGOALS ENABLERS OUTCOME MEASURES
4.2.1 Ensure that • Specific needs-based Aboriginal • Health outcomes of Aboriginal and
health policy and Torres Strait Islander health Torres Strait Islander communities
addresses the needs funding allocated to address health improved against the new National
of Aboriginal and needs of Aboriginal and Torres Strait Agreement on Closing the Gap
Torres Strait Islander Islander communities, including targets and health policy benchmarks
Australians. unimplemented parts of the National – including at least 90 per cent
Aboriginal and Torres Strait Islander population access to fluoridated water.
Health Plan 2013-2023, as well as
• Significant performance uplift
greater investment in primary care.
against the age-standardised
• Build on the fine examples of rate of potentially preventable
Aboriginal and Torres Strait Islander hospitalisations, as outlined in the
healthcare service delivery already National Health Reform Agreement
operating in Australia – such as the and State and Territory Aboriginal and
Institute for Urban Indigenous Health – Torres Strait Islander health plans.
and replicate this or equivalent models
• The level of funding for healthcare
as appropriate throughout Australia.
for Aboriginal and Torres Strait
• Mandate regular cultural safety Islander people is based on the level
training for all medical practitioners. of need indicated by the Burden of
Disease studies.
• Increase in Aboriginal and Torres
Strait Islander people having a health
assessment with a GP, as measured
by an increase in MBS item 715 -
Indigenous Health Assessment.
4.2.2 Ensure that • Adequate nursing staff in nursing • Disadvantaged communities accessing
health policy homes and enhanced integration healthcare more regularly and
addresses the needs between the aged care and achieving improved health outcomes.
of those who are health systems.
marginalised and
• Universal healthcare and affordability
those who suffer
achieved for all, particularly people in
socioeconomic
socioeconomic disadvantage.
disadvantage, as
well as those in • Options for telehealth between the GP
aged care who have and a carer or nursing home nurse on
limited access to behalf of a patient, where patients are
health services. non-communicative.
• Adequate healthcare for those in other
institutional care settings, and those
within the disability sector.
AMA’s Vision for Australia’s Health 31GOALS ENABLERS OUTCOME MEASURES
4.3.1 Establishing a • Stronger recruitment into General • All CRP places filled each year.
Community Resident Practice, by providing doctors in
Program (CRP). training with more opportunities to
undertake pre vocational training in
General Practice.
• Ensuring more doctors have a
fundamental understanding of the
functioning of General Practice and
primary care.
4.3.2 Expand the • An increased focus on generalism • All STP places filled each year.
Commonwealth within the specialist workforce.
• Evidence of improved recruitment into
Government’s
• Improved access to specialist services under-supplied medical specialties.
Specialist Training
in rural Australia.
Program (STP) to
1700 places by 2022,
giving priority to rural
areas, generalist
training and
specialties that are
under-supplied.
4.3.3 Increase the • Improve workforce distribution by • Increased numbers of
focus of medical encouraging the development of a Australian-trained specialists
schools on rural rural training pipeline which takes working in rural Australia.
training opportunities students all the way through to the
• Evaluation of end-to-end rural
by supporting completion of specialist fellowship
medical training to ensure it is
end-to-end rural training.
providing positive rural exposure,
medical school
• Dedicating at least one-third of all leading to retention of rural
programs.
domestic first-year medical school medical practitioners.
places to students with a rural
background and requiring one-third
of all medical students to undertake
at least one year of clinical training in
rural areas.
4.3.4 Rollout of • Improved access to GPs in rural areas. • NRGP places fully subscribed by end
the National Rural of 2021.
Generalist Pathway
(NRGP) nationally
by 2021.
32 AMA’s Vision for Australia’s HealthGOALS ENABLERS OUTCOME MEASURES
4.3.5 Regulate all • Avoiding the boom-bust cycle • Medical school intakes reflect the
medical school that has characterised medical advice of the Medical Workforce
places, including workforce planning. Reform Advisory Committee (MWRAC).
domestic and
• Ensuring that medical school intakes • Annual reporting of medical school
overseas full fee-
are matched to the available number places through the Medical Education
paying places to
of training places in the pre vocational and Training data reporting.
match medical
and vocational training pipeline.
school intakes with • Greater proportion of OTDs serving full
community need. • Ensuring medical school intakes are 10-year moratorium and current loop-
linked to workforce planning and holes closed, while working towards
community need. dismantling the 10-year moratorium
over time. More robust incentives
• Regulation to limit the number of full-
and support mechanisms should be
fee paying overseas medical student
introduced to encourage increasing
in Australian universities to no more
numbers of locally-trained doctors
than 15 per cent of the total number
and appropriately skilled international
of students.
medical graduates alike to consider a
• Ensuring the 10-year moratorium career in rural and remote practice.
rules for overseas trained doctors
(OTDs) are enacted simply, fairly
and uniformly.
4.3.6 Promotion of • Quarantined National Health and • Greater coverage and access to
regional training and Medical Research Council research non-GP specialist capacity in regional
research teaching grant funding for regional teaching training centres, aiming for a 20 per
hospital hubs to grow hospitals. cent increase by end of 2023.
non-GP specialist
• Commonwealth Medical Workforce
capacity outside
Strategy to recognise importance
metropolitan areas.
of development and investment
in regional teaching hospitals with
sufficient capacity to host STP-funded
non-GP specialist registrars.
4.4.1 Mental health- • Accredited mental health • Greater continuity of care, shorter
specific investment in nurses/ social workers embedded in follow-up times, increased compliance
developing capacity General Practice, with appropriate with mental health plans.
in mental health training and support.
support services
in GP practices
in a coordinated
manner, rather than
siloed funding to
non-government
organisations.
AMA’s Vision for Australia’s Health 33You can also read