World Journal of Surgery and Surgical Research - World Journal of Surgery and Surgical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

World Journal of Surgery and Surgical Research Research Article
Published: 17 Sep, 2018
Comparative Study of Standard Fundoplication (Nissen
and Toupet) vs. Modified Toupet Fundoplication for GERD
Repair
Mihael Sok1,2*, Boris Greif1, Tomaž Štupnik1,2 and Matevž Srpčič1
1
Department of Thoracic Surgery, University Medical Centre Ljubljana, Slovenia
2
Department of Medicine, University of Ljubljana, Slovenia
Abstract
Introduction: Failure following anti reflux surgery for GERD is reported from 3% to 30%,
predominantly from reflux recurrence. Modified Fundoplication follows the principles of standard
Nissen or Toupet Fundoplication. The difference is in the fixation of esophagogastric junction
intraabdominally, technically with two retro esophageal Fundo-crural muscle stitches and a
retroesophageal fundo- right crus stich. No stitches in the esophagus are used.
Aim: A comparative study of modified fundoplication vs. standard (Toupet or Nissen) fundoplication
was carried out.
Material and Methods: Patients with documented gastroesophageal reflux entered a prospective
nonrandomized, feasibility study. Patients who underwent a different type of operation were
comparable for age, gender, BMI, functional esophageal test before operation, number of hiatal
stitches, and hiatal hernia presence at operation and hospitalization time.
Aim: To compare modified Toupet with standard Fundoplication with respect to functional
postoperative results.
Results: A total of 70 patients, 42 female and 28 male patients, were operated on laparoscopically for
OPEN ACCESS GERD. Standard Fundoplication was carried out in 61 patients and modified Toupet in 9 patients.
After 2-5 years of follow up 4(6%) patients from the standard Fundoplication group underwent re
*Correspondence: operation, among them one for reflux recurrence. No patients from the modified Toupet group
Mihael Sok, Department of Thoracic needed repeat surgery. In the same postoperative period 37(69%) patients were without PPI from
Surgery, University Medical Center the standard group in comparison to 6(75%) patients from the modified Toupet group.
Ljubljana, Zaloškacesta 7, 1000
Conclusion: The modified Toupet Fundoplication is technically simpler to perform, is not inferior
Ljubljana, Slovenia, Tel: +386- 41-
to standard Fundoplication and is feasible with promising results. The importance of GEJ fixation
776823; Fax: +386- 5222485;
to crural muscles and plastics of Gastroesophageal flap valve is discussed.
E-mail: miha.sok@kclj.si
Received Date: 24 Aug 2018 Keywords: Gastroesophageal reflux; Antireflux surgery; Reflux recurrence; Modified
Accepted Date: 14 Sep 2018 Fundoplication
Published Date: 17 Sep 2018
Citation:
Introduction
Sok M, Greif B, Štupnik T, Srpčič In surgical therapy, despite clear operative principles, short and long-term failures following
M. Comparative Study of Standard Fundoplication for GERD still remain a serious problem. Failure following Antireflux surgery for
Fundoplication (Nissen and Toupet) GERD is reported from 3% to 30%, predominantly from persistent or recurrent symptoms [1,2].
vs. Modified Toupet Fundoplication for This variability may be explained by differences in the definition of failure from center to center.
GERD Repair. World J Surg Surgical Over the past 15 years, arrays of innovative surgical and endoscopic techniques have been
Res. 2018; 1: 1056. developed for the treatment of Gastroesophageal Reflux Disease (GERD) [3]. The basic operative
Copyright © 2018 Mihael Sok. This is principles in GERD or Hiatus Hernia (HH) repair is Retro-esophageal cruroplasty and fixation of
the stomach within the abdomen, namely posterior attachment of the Esophagogastric Junction
an open access article distributed under
(EGJ) [4-7]. The predominant operative approach for fixation at present appears to be laparoscopic
the Creative Commons Attribution
circumferential Fundoplication, such as the Nissen or Toupet procedures [8].
License, which permits unrestricted
use, distribution, and reproduction in Some years ago at the demanding operation of a patient with recurrent HH an improvisation of
any medium, provided the original work the Fundoplication was carried out as an exit from force. Only firm stitches of the Retroesophageal
is properly cited. gastric fundus to the crural muscles were made without fundus –esophagus stitches. After a good
Remedy Publications LLC., | http://surgeryresearchjournal.com 1 2018 | Volume 1 | Article 1056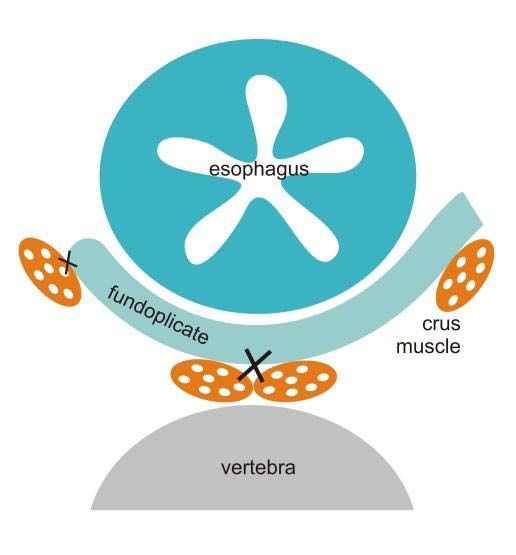
Mihael Sok, et al., World Journal of Surgery and Surgical Research - Thoracic Surgery
Table 1: Patient's characteristics of two fundoplications.
Standard fundoplication group (Nissen or Toupet) (n=61) Modified Toupet group (n=9) p
Female n 39 3
Male n 22 6
Age (years, mean, range) 48.5 (16-75) 46.7 (26-65) 0.37
BMI (kg/m2), mean, range) 27.6 /17-37) 27.0 (19-33) 0.36
*Number of stiches for hiatus closure (mean, range) 2.7 (1-4) 2.2 (2-3)
De Mesteer (mean, range) 25.1 (2-160) 17.3 (5-29) 0.15
Hospitalization time (days, mean, range) 2.1 (1-4) 2.6 (1-3) 0.39
Hiatal hernia at operation n (%) 30 (50%) 3 (33%) 0.37
BMI: Body Mass Index
Table 2: HH recurrences and PPI consumption after 2-4 years follow up.
Standard fundoplication (Nissen or Toupet) (n=61) Modified Toupet n=9
Radiologic hiatus hernia n (%) 8 (13%) 1 (11%)
Repeat operation 4 (2x dysphagia, 1x reflux, 1x hiatus hernia) 0
PPI consumption
no 37 (69%) 6 (75%)
regularly 9 (17%) 1 (12.5%)
on demand 7 1
unknown 7 1
outcome, this simplified Fundoplication was taken into consideration. closure as the indirect measure of the hernia size. After the procedure,
This is 180° fundoplication and follows Toupet principles with some all patients were monitored in the recovery room of the operating
modifications. Two big bite stitches are done posteriorly between the unit for two hours and then transferred to the intensive care unit.
gastric fundus in the retroesophageal position and crural muscles On the first postoperative day contrast examination of the esophagus
medially as caudally as possible followed by one stitch between was performed and patients began to consume liquids. The patients
the retroesophageal gastric fundus and right crus. No Esophago- were discharged as soon as they were able to consume mixed food,
fundoplicate stitches are made. The aim is solid fixation of the EGJ when the postoperative pain was well controlled by oral analgesics,
and gastric fundus intra abdominally and reinforcement of potential and if there were no other conditions or complications requiring a
weak crural muscles with alive, vascularized tissue, namely the gastric prolonged hospital stay.
fundus. Simple modification was later recognized as a potential
Patients who underwent a different type of operation were
and good approach for better laparoscopic fixation of EGJ intra
comparable for age, gender, BMI, functional esophageal test before
abdominally with anti-reflux power in patients with GERD and HH.
operation, number of hiatal stitches, and hiatal hernia presence at
Aim: The aim of the study was to compare the feasibility and operation and hospitalization time. Patients were followed from 2 to
late results of standard fundoplication namely Nissen or Toupet 5 years. PPI consumption, reflux recurrence, dysphagia and hiatus
fundoplication with the modified Toupet procedure. Postoperative hernia advent were registered.
course and postoperative results 2-5 years after operation were
registered. Postoperative reflux recurrence rate and dysphagia were
Surgery
the primary endpoints of the study. Antireflux operation was performed following the standard
technique: laparoscopy, resection of the hernia sack from the
Material and Methods
mediastinum but not from the abdomen, if present, elevation of the
From January 2012 to January 2014, a prospective nonrandomized EGJ with retroesophageal window creation and cruroplasty with
study of consecutive patients undergoing operations for GERD Teflon pledges. Then fundoplication followed: either the Nissen or
was made at a single tertiary institution. The indication for surgical Toupet fundoplication as the standard fundoplication or modified
treatment of GERD was documented Gastroesophageal reflux that Toupet fundoplication. Modified Toupet was carried out using
persisted despite maximal medical therapy, patient's preference, extra two firm big bite retroesophageal fundo-crural stitches, the first
esophageal manifestations and GERD related esophageal injury. approximately 1 cm from the angle of Hiss on the anterior aspect
Patients were without previous or present dysphagia and without of the gastric fundus to the crural muscle medially as caudally as
esophageal stenosis. 24-hr pH monitoring was performed selectively possible where hiatus stitches were already in place. The second
in patients with extraesophageal symptoms and in those without retroesophageal fundo-crural stitch was made about 2 cm cranially.
erosive esophagitis. Manometer was also selectively carried out. BMI The distance between the first and second stitches was the size of an
of the patients was calculated. Optimal data for specific analysis was open standard grasper jaw. The third big bite stitch was a regular
eligible for 70 patients and these patients entered the study. The hiatus Toupet retroesophageal fundus- right diaphragmatic crus stitch
hernia was registered at laparoscopy but the size of the hernia was not (Figure 1). The logic behind this method was that these stitches
measured in cm, but rather with the number of stitches for crural would create a fundoplication-like effect to control reflux and
Remedy Publications LLC., | http://surgeryresearchjournal.com 2 2018 | Volume 1 | Article 1056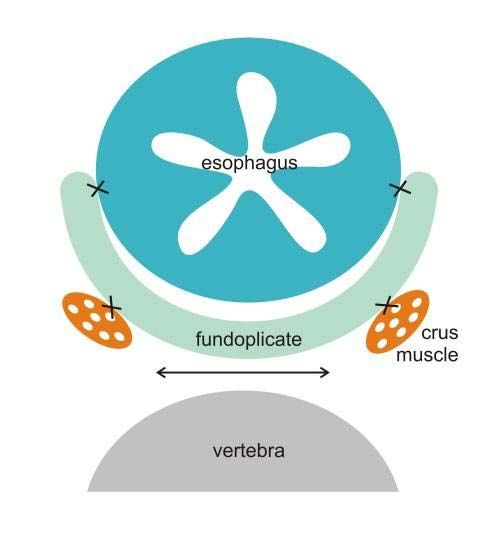
Mihael Sok, et al., World Journal of Surgery and Surgical Research - Thoracic Surgery
Figure 1: Schematical representation of stitches (1,2,3) for modified Toupet.
Figure 3: Schematical representation of modified Toupet. Fundo-crural
space is obliterated.
in 9 patients. All patients were operated upon laparoscopically. In
the standard fundoplication and modified Toupet the mean age of
patients was 48.5 and 46.7 years, mean BMI was 27.6 and 27.0 kg/m2,
mean number of stitches was 2.7 and 2.2, mean hospitalization time
was 2.1 and 2.6 days and mean DeMeester score was 25.1 and 17.3
respectively. At operation hiatal hernia or at list dilatated hiatus was
registered in 30 and 3 patients in the standard and modified Toupet
groups respectively (Table 1). The differences were not significant.
After 2-5 years of follow up problems were registered and are
shown in Table 2. Four patients from the standard group needed
reoperation: dysphagia - two patients, reflux - one patient and
symptomatic hiatus hernia - one patient. In the modified group no
Figure 2: Schematical representation of Toupet fundoplication with potential
forces (↔) from intraabdominal tissue that can spread crural muscles and patients needed reoperation. In the same period in the standard group
place where intra abdomilal tissue can enter. 9 patients took a PPI regularly and 7 on demand (31%) in comparison
with 1 patient who took a PPI regularly and 1 who took a PPI on
intra abdominal EGJ fixation, obliteration of the retroesophageal demand (25%) in modified the Toupet group. These differences were
or retrofundal space, stable tamponation of the hiatus region and not significant.
possible adhesion formation of the crural region and reinforcement
of the hiatal muscle with vital tissue, namely the gastric fundus.
Discussion
Figures 2 and 3 show a schematic representation of the Toupet and After the first description of the 360° esophagogastric
modified Toupet procedures. All operations were performed without fundoplication in 1956, the Nissen fundoplication surgery
bougie, without dissection of the gastric short vessels, without the armamentarium has changed little until now. All is about
Collis procedure and without mesh. All patients were operated on fundoplication to augment the Lower Esophageal Sphincter (LES).
under the same conditions and by the same surgical team, using the Some modifications are described with the intention to improve
same brand of laparoscopic instruments, with an abdominal CO2 in upon postoperative complications, late results, cost of the operation
sufflation pressure of 15 mmHg. Modified fundoplication was made and postoperative quality of life. The operation should be safe for the
by one surgeon and was not selected randomly. patient, cost-effective and complications free [9-13].
Statistics According to the literature the failure rate of open or laparoscopic
approaches ranges from 3% to 30% [1,2]. In our study failure that
Data were analyzed using the Statistical Package for Social
needed reoperation was registered in 4(6%) patients, two for dysphagia,
Sciences version 16.0 for Windows (SPSS, Chicago, IL) software.
one for severe reflux and gas bloat and one for hiatus hernia. All re-
Categorical variables were tested for associations using a χ2 test.
operated patients were from the standard fundoplication group (7%).
The descriptive data were expressed as a mean and range. For the
No patients in the modified Toupet group needed reoperation.
normally distributed variables, at-test was used. The Sperm and Rho
association test was used to measure the relationship between two From the patients that presented for follow-up 2-5 years after
variables. A p-value ofMihael Sok, et al., World Journal of Surgery and Surgical Research - Thoracic Surgery
have criticized the Toupet procedure as having a higher long-term technically simpler to perform. The basic idea is to fix ERJ intra
failure rate than the Nissen approach, especially for patients with abdominally, to obliterate retroesophageal and retrofundal space,
severe GERD forms [15]. On the other hand Toupet fundoplication to tamponate crural region with fundus, to advance adhesion
should be considered in redo interventions for patients who initially formation in the hiatus region, to reinforce hiatal muscle by vital
underwent Nissen fundoplication [16]. tissue and to support the antireflux barrier affecting GEFV. It appears
to be a promising alternative and affair compromise to other well-
Some positive effect on reflux control of the modified Toupet
established antireflux operations. This study shows that the modified
can be speculated on the basis of the Gastroesophageal Flap Valve
Toupet fundoplication is not inferior to standard fundoplication. The
(GEFV) function. The exact means by which fundoplication controls
modification is safe for the patient. Further studies are needed for
gastroesophageal reflux is still a matter of debate. It is often assumed
objectivation of these speculations.
that reflux is controlled by increased resting Lower Esophageal
Sphinter (LES) pressure and intra-abdominal length of the esophagus. The limitations of the study include the small sample size
However, there are several studies that show that the resting pressure of comparable patients, non-randomized study, single surgeon
does not always increase after fundoplication and that in the majority experience and short postoperative follow up.
of such cases reflux is perfectly controlled. Resting LES pressure may
even decrease as the intra-abdominal length of the esophagus [17].
References
GEFV was established as an important component in the anti-reflux 1. Soper NJ, Dunnegan D. Anatomic fundoplication failure after laparoscopic
barrier [18]. Three distinct anatomic structures, the clasp and sling antireflux surgery. Ann Surg. 1999;229(5):669-76.
muscle fibers, crural diaphragm and LES were identified to form 2. Watson DI, de Beaux AC. Complications of laparoscopic antireflux
the antireflux barrier [19,20]. Miller et al. [21] report that the basic surgery. Surg Endosc. 2001;15(4):344-52.
principle of the most usual antireflux surgeries e.g. Nissen and Toupet 3. Ganz RA. A Review of new surgical and endoscopic therapies
is retroesophageal fundus extra position. The angle of his is changed for gastroesophageal reflux disease. Gastroenterol Hepatol (NY).
and the gastric oblique muscle of the fundus is strained. It was shown 2016;12(7):424-31.
that Nissen fundoplication prevents reflux by artificially bolstering
4. Naunheim KS, Edwards M. Paraesophageal hiatal herna. In: General
the area of the defective gastric sling fiber/clasp fiber complex and thoracic surgery. Shilds TW, Locicero J III, Reed CE, editors. Lippincott
is an important factor in generating the antireflux barrier [22]. Later Williams & Wilkins, Philadelphia, PA,USA. 2009;951-9.
on it was discovered that the gastric sling fiber/clasp fiber complex
5. Mori T, Nagao G, Sugiyama M. Paraesophageal hernia repair. Ann Thorac
is not present in patients with GERD, suggesting that GERD may
Cardiovasc Surg. 2012;18:297-305.
be a pathophysiologic defect within the gastric clasp/sling smooth
muscle fiber complex [23]. The modified Toupet technique, like the 6. Morse C, Pennathur A, Luketich JD. Laparoscopic techniques in
standard technique, involves fundus retroesophageal extra position reoperation for failed antireflux repairs. In: Pearson's Thoracic and
Esophageal Surgery. 3rd ed. Patterson GA, Pearson FG, Cooper JD,
and has the potential to influence GEFV. Hill repair is the only known
editors. Churchill Livingstone, Philadelphia, PA, USA. 2008;367–75.
repair done on firm anchoring of EGJ within the abdominal cavity
and accentuating the flap valve [24]. We believe that fundo-crual 7. Huang J, Low D. Hill repair. In: Esophageal Surgery. Pearson FG, Cooper
JD, Deslauriers J, editors. Churchill Livingstone, Philadelphia, PA, USA.
stitches in the modified Toupet have the same power. Further studies
2008;288–97.
are needed to confirm this statement. The angel of He was pointed to
as important objective in the WTP procedure [13]. 8. Allen MS, Trastek VF, Deschamps C, Pairolero PC. Intrathoracic
stomach. Presentation and results of operation. J Thorac Cardiovasc Surg.
Two patients from the standard fundoplication group required 1993;105(2):253-8.
reoperation for persistent dysphagia. The reason is likely that bougie
9. Castelijns PSS, van de Poll MCG, Smulders JF. A modified technique to
was not used. Sages recommend the use of an esophageal dilator but Create a standardized floppy Nissen fundoplication without a bougie. J
use should be weighed against the risk of esophageal injury [25]. In Laparoendosc Adv Surg Tech A. 2018;28(7):853-8.
the past we perfomed bougie but after two consecutive intraoperative
10. Lukish J, Pryor H, Rhee D, Salazar J, Goldstein S, Gause C, et al. A novel
perforations we decided to stop using the bouginage. We believe that
continuous stitch fundoplication utilizing knotless barbed suture in
the reasons behind the problem involved the organization of the children with gastroesophageal reflux disease: a pilot study. J Pediatr Surg.
team, as there was a high turnover of members in the team responsible 2015;50(2):272-4.
for bougie replacement in our tertiary center. We routinely used
11. Shapey IM, Agrawal S, Peacock A, Super P. A prospective cross-
an esophageal dilator twice, first for hiatus closure and second for
sectional study of laparoscopic subtotal Lind fundoplication for gastro-
fundoplication formation with twice the risk for perforation. Today oesophagealreflux disease--a durable and effective anti-reflux procedure.
we prefer to use the Toupet operation, short floppy Nissen and dissent Int J Surg. 2015;13:257-60.
hiatus opening around the esophagus.
12. Smith CD, DeVault KR, Buchanan M. Introduction of mechanical
One patient underwent reoperation for hernia recurrence from sphincter augmentation for gastroesophageal reflux disease into practice:
the standard fundoplication group. This patient had a hiatus hernia early clinical outcomes and keys to successful adoption. J Am Coll Surg.
2014;218(4):776-81.
intraoperatively and a sliding hernia on a barium study preoperatively.
13. Wróblewski T, Kobryn K, Nowosad M. Surgical treatment of GERD.
Conclusion Comparative study of WTP vs. Toupet fundoplication - results of 151
To summarize, some advantages of the modified Toupet consecutive cases. Video surgery Miniinv. 2016;11(2):60-6.
180° fundoplication are no esophago-fundoplicate sutures, no 14. Hatch KF, Daily MF, Christensen BJ, Glasgow RE. Failed fundoplications.
intraoperative bouginage, no short gastric artery resection, no Am J Surg. 2004;188:786-91.
possibility of sleep Nissen or malposition of the wrap. It is also 15. Erenoğlu C, Miller A, Schirmer B. Laparoscopic Toupet versus Nissen
Remedy Publications LLC., | http://surgeryresearchjournal.com 4 2018 | Volume 1 | Article 1056Mihael Sok, et al., World Journal of Surgery and Surgical Research - Thoracic Surgery
fundoplication for the treatment of gastroesophageal reflux disease. 21. Miller L, Clavé P, Farré R, Lecea B, Ruggieri MR, Ouyang A, et al. Physiology
IntSurg. 2003;88(4):219-25. of the upper segment, body, and lower segment of the esophagus. Ann N Y
Acad Sci. 2013;1300:261-77.
16. Al Hashmi AW, Pineton de Chambrun G, Souche R, Bertrand M,
De Blasi V, Jacques E, et al. A retrospective multicenter analysis on 22. Dai Q, Chung CY, Nowrouzzadeh F. Simultaneous ultrasound and
redo-laparoscopic anti-reflux surgery: conservative or conversion manometry in the evaluation of Nissen fundoplication. Gastroenterology.
fundoplication? Surg Endosc. 2018. 2003;124:A418-M2113.
17. Bancewicz J, Mughal M, Marples M. The lower oesophageal sphincter after 23. Miller L, Dai Q, Vegesna A, Korimilli A, Ulerich R, Schiffner B, et al. A
floppy Nissen fundoplication.Br J Surg. 1987;74(3):162-4. missing sphincteric component of the gastro-oesophageal junction in
patients with GORD. Neurogastroenterol Motil. 2009;21(18):813-e52.
18. Hill LD, Kozarek RA, Kraemer SJ, Aye RW, Mercer CD, Low DE, et al. The
gastroesophageal flap valve: in vitro and in vivo observations. Gastrointest 24. Huang J, Low D. Hill repair. In: Pearson FG, Cooper JD, Deslauriers J,
Endosc. 1996;44(5):541-7. editors. Esophageal Surgery. New York: Churchill Livingstone; 2007:288–
97.
19. Mittal RK, Balaban DH. The esophagogastric junction. N Engl J Med.
1997;336:924-32.
20. Miller LS, James B, Ulerich R. A new theory to explain the pathophysiology
of GERD. Gastroenterology. 2004;126:A503-T1741.
Remedy Publications LLC., | http://surgeryresearchjournal.com 5 2018 | Volume 1 | Article 1056You can also read

















































