Microscopic Pathology of the Gray Collie Syndrome
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Path. vet. 7: 225-245 (1970)
From ' I h c National Animal Discasc Laboratory, Vetcrinary Scicnces Research
Division, ARS, USDA, Amcs, 1ou.n
Microscopic Pathology of the Gray Collie Syndrome
Cyclic Neutropenia, Amyloidosis, Enteritis, and Bone Necrosis
N.F. CHEVILLE, I P H.W. MOON
R.C. C U T I ~and
The gray collie syndrome (GCS) is a lethal hereditary diseasc
associated with abnormal hair pigmentationl3, cyclic depression of
circulating neutrophils18, enteric disease25, and bilateral ocular scleral
ectasiag, 2B. Neutrophils disappear from the peripheral blood at inter-
vals of 10.5 to 11.5 daysg. 18 although intervals bctween neutropenic
phases vary with the severity of disease. Episodes of fever, diarrhea,
gingivitis, rcspiratory infection, lymphadenitis, and lameness (bone
necrosis) follow neutropcnic phases. Most untreated affcctcd dogs die
within a few days of birth, yet some survive only t o succumb in early
adulthood. The life-span of thosc surviving puppyhood is markedly
lengthened if they receive supportive clinical treatment9 ; even so, they
eventually develop lymphoid exhaustion, rcticuloendothclial (RE)
hyperplasia with monocytosis, anemia, and amyloidosiss.
The wide spcctrum of clinical signs and lesions in thc GCS may
be due t o one basic defect; i.e., cyclic ncutropcnia. However, the
pathogenesis of severe diarrhea, of the bone lesions, and of amyloidosis
may involve other basic deficiencies in affected dogs. It is therefore
the objective of this rcport to document the spectrum of lesions which
occurred in a serics of cases of the GCS.
Materials and Methods
Eight collic dogs with GCS (1 to 8) and 5 related, non-gray dogs (9-13)
were examined ('Iable I). Data on env~ronment,hereditary background, and clin-
Downloaded from vet.sagepub.com by guest on February 4, 2015Yable I . Clinical and pathologic observations on 8 dogs with gray collie syndrome
and 5 related (nun-gray) collics
GCS dogs Rclatcd dogs
Neonatal Pups Adults (non-Era y)
Case number 1 2 3 4 5 6 7 8 9 10111213
Sex ? d 0 < ) < t 1 d d $" d Y ? d ?
Age at death (Wks) 1/7 1 1/2 10 20 26 38 106 170 50 64 87 87
Chief clinical signs
Cyclic neutropenia 0 0 0 + + + + +
+++++++++
- - - - -
Diarrhea + 0
i- i- ++ ++ ++
It - - - - -
Lameness - - - - - - - -
Epilepsy _ _ _ - _ _ - -
+ -k-+-
Paiholo& lesioiis
Lymphoid atrophy + + + ++
+ + ++
- - -
Amyloidosis _ - -
+ ++++o
-
Enteritis _ _ _
Gingivitis, Rhinitis - - - + ++ ++ ++
Bone necrosis _ _ _ + + + + + ++
Bronchopneumonia + ++- +
+
- - -
Nephritis _ _ _ - -
+
-
Liver abscesses - _ _
+ + +
-
- -
Gonadal hypoplasia - - -
-
Malacia (cerebrum) - - - - - -
0
* Pulmonary edema and hypercmia
0 = not cxamined.
ical laboratory procedures have been reported on 6 of thcseg. Dogs 3, 6, 7, and 8
received antibiotic and immune globulin therapy; othcrs receivcd no treatment.
Dogs 3, 7, and 10 were found dead. Dogs 11 and 13 wcrc normal in appearance
whcn killed with succinyl chloride; all other dogs were killed when they were mor-
ibund and survival appeared unlikely. The following dogs were littermates: 1 and
2, 4 and 6, 5 and 7, and 10 to 13. Dog 9 was the sire of dogs 10 t o 13. D o g 13 after
mating with dog 12 produced 8 normal-appearing non-gray puppies. Tissues from
all dogs were fixed in 10% formalin, cmbcdded in paraffin, sectioned, and stained
with hcmatoxylin-eosin. Alcian blue-periodic acid-Schiff, Congo red, and thio-
flavin T stains were used"". Frozen sections of spleens (dogs 4 to 8) were stained
with commercial fluorescein-conjugated rabbit anti-dog-globulin antiserum (hli-
crobiological Associates) and with fluorescein-conjiigatcd chicken anti-dog-globu-
lin antiserum which we prepared using ammonium sulfate-precipitated dog glo-
bulin as antigen]". Portions of spleen from dogs 6 to 8 were fixed in 2.5'%, glutaral-
dehydc (1 hour), rinsed in buffer (1 hour), post-fixed in osmium tetroxide (1 hour),
washed in buffer (overnight), dehydrated in graded ethanols, and embedded in
Epon. Sections were cut on an Ultrotome and examined with a Philips electron
microscope model 200 at 60 K v . Bone sections from dogs 6 and 7 mere mounted
Downloaded from vet.sagepub.com by guest on February 4, 2015Microscopic Pathology of the Gray Collie Syndrome 227
on large slides (2 x 3 inches) and includcd: nasal cavity, tooth, ribs, femur (head),
stifle joint, tarsal-metatarsal joints, humerus (head), elbow joint, carpal-metacarpal
joint, and the vertebral column (cervical, thoracic, and lumbar). Ribs were exam-
ined from dogs 5, 8, and 10 t o 12. Splenic biopsy on dog 7 was done a t 30 and
36 weeks of age by laparotorny under general anesthesia. Blood cells and serum
werc examined on dogs 1 , 2 , 7 , and 9 to 13 as previously described". Thrombocyte
counts were begun at the termination of the disease of d o g 7; all values were low.
Peripheral blood was examined periodically with the electron microscope. To
avoid producing anemia, a modification of buffy-coat fixation's 2 was used. Blood
collected in microhematocrit capillary tubes was centrifuged, the buffy coat over-
laid in situ with 2.50/, glutaraldehyde, and the resulting buffy-coat pellet processed
as described above. Serum obtained at weckly intervals from dogs 6 and 10 to 12
was examined using cellulose-acetate electrophoresis and immunoelectrophoresis
(models RlOO and R103, Beckman Co.).
Results
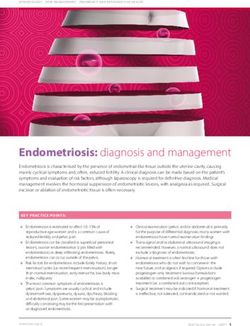
The differential and total leukocyte counts of case 7 (Fig. 1) were
similar to the periodic depressions in neutrophils described previously
in dogs 4 to 8. Dogs 1 and 2 did not live long enough to develop a
neutropenic cycle ; their leukocyte counts at death were elevated and
neutrophils predominated. No marlied abnormality was noticed in the
ultrastructure of the granules of neutrophils in most affected dogs.
They seemed slightly smaller than those of normal dogs. Neutrophils
examined during the terminal days of dogs 3 and 5, however, had large
pleomorphic granules, excessive cytoplasmic fibrillar material, and
areas of small dense granules. Circulating large monocytes were dom-
inant in some dogs following terminal neutropenic stages and their
cytoplasm contained many primary lysosomes and active Golgi sys-
tems. Circulating plasma cells (Fig. 2) and macrophages were not un-
common during chronic disease. The tracings from electrophoresis
of serum proteins were normal in dog 7 during the first months of
life. As episodes of disease began to accompany neutropenic phases,
slight elevation of y - and P-globulins (Fig. 3) were noted. As the dis-
ease progressed, there were marked increase in ccz-globulin and marked
decrease in albumin. Previous studies on serum proteins of dogs 5
and 7 9 revealed increase in y-globulin early in the disease with in-
crease in cc- and j3-globulins and decreased y-globulin and albumin
later in the disease.
The electrophoretic patterns for serum proteins for dogs 10 to
12 revealed no abnormality.
Downloaded from vet.sagepub.com by guest on February 4, 2015228 (1H E V I L L E / ( 1 U T L I P / h l O O N
20,000 1 0Eosinophiles
Neutrophiles
1500C
L 0 Monocytes
LvmDhocvtes
t
.
L
ff 10,ooc
2.
y
Y
3
5300
25,000 1
I r 150,000 EE
August September October
Fig. 1. Graphic presentation of differential and total white blood counts of Dog 7.
Neutropenic episodes are accompanied by thrombocytopenia. Mono-
cytosis follows neutropenic phases.
Splcen
Extramedullary hcmatopoiesis was prominent in the 3 puppies
dying nconatally (dogs 1 to 3). The white pulp (periarterial lymphoid
sheath) was well developed in dogs 2 and 3 but minimal in dog 1.
There were large numbers of plasmacytcs throughout the red pulp
of dog 3 which had hepaiic abscesscs.
The 2 dogs which died during puppyhood (dogs 4 and 5) had
minimal evidence of cxtramedullary hematopoiesis. Dog 4, which died
with severe diarrhea, had large lymphoblastic “cuffs” surrounding the
lymphoid sheath but germinal centers were not seen.
Downloaded from vet.sagepub.com by guest on February 4, 2015Microscopic Pathology of the Gray Collic Syndrome 229
2. Electron micrograph of circulating plasmacyte fixed from peripheral blood
1;i~.
during the terminal stagcs of disease (Dog 4). Dilatations of the cisternae
of thc rough cndoplasmic rcticulum arc filled with dciisc material.
Thc 3 GCS dogs which survived into adulthood (dogs 6 to 8) had
severe lymphocytic exhaustion of the lymphoid sheath. There were
massive deposits of amyloid around the periphery of the sheath (peri-
follicular amyloid), extending peripherally from the marginal zone
into the red pulp (Fig. 4). Amyloid also occurred in globules among
the small lymphoid cells of the lymphoid sheath and immediately
surrounding the central artery. The spleen of dog 7 at 30 weeks had
lymphoid exhaustion but no amyloid; at 36 weclts it had well-deve-
loped dcposits of amyloid. Amyloid was slightly eosinophilic and
stained inconsistently and only in small foci with Congo red and thio-
flavin T. Masses of amyloid wcrc bound by reticular cells and pyro-
ninophilic blast cells and were minimally birefringcnt when stained with
Congo red. Fluorescein-conjugated chclien anti-dog globulin attached
to the periarteriolar amyloid dcposits (Fig. 5). Fluorescence was
demonstrable also in the central artcry and splenic sinuses. The strong-
est fluorescencc was in areas which had thc strongest affinity for Congo
red.
Downloaded from vet.sagepub.com by guest on February 4, 2015230 CHEVILLE/CUTLIP/MOON
2
4
n
JULY 17
Fig. 3. Electrophoretograms of serum proteins from 4 pre-neutropenic phases of
Dog 7. The serum o n July 17 was normal. 'The a-, ,5-, and y-globulins
increased as the disease progressed.
Fig. 4. D o g 7. Dense amyloid extending peripherally from the splenic white pulp
into the red pulp. There are homogenous globules of amyloid (arrow)
within the lymphoid sheath (see Fig. 6 for ultrastructure) and depletion of
lymphoid cells around the central artery. H&E.
Fig. 5. D o g 7. Frozen section of spleen containing perifollicular amyloid stained
with fluorescein-conjugated chicken anti-dog globulin. The fluorescence
occurs in areas of dense amyloid and around the central artery (arrow).
Fig. 6. Masses of extracellular amyloid similar to those occurring in globules
within the lymphoid tissue surrounding the central artery (see Fig. 4).'The
capillary contains platelets and fibrin thrombi (uppcr right). Dark spindle-
shaped reticular cells (arrow), stellate amyloid-producing cells (A), and
degranulated neutrophils (lower right) are dispersed through the amyloid.
x 6,300.
Downloaded from vet.sagepub.com by guest on February 4, 2015hllcroscopic Pathology of the Gray Collic Syndrome 231
Downloaded from vet.sagepub.com by guest on February 4, 2015232 c I 1 r; V I L L E /
Rlicrosccipic I’athology (if thc
234 c H E V I L L E / c LIT L I P / hf 0 0 N
FYR. 9. Central artery of thc white pulp. There arc microfibrils in the endothelial
cells surrounding the lumcn (upper right). Amyloid fibers infiltrate the
glycoprotein at the base of endothelial cells (upper left) and the smooth
muscle cells of the media. Necrotic amyloid producing cells (left) surround
the artery. Large, dense, membrane-bound granules in the myocyte a t
center appear to be lysosomcs. Similar but smaller granules are in the endo-
thelial cells at upper right. x 6,580.
poorly developed diffuse lymphoid fields. Dogs 2 to 5 had active
centers, a reflection of their infectious diseases. Dog 4, which died of
severe enteritis, had focal or diffuse necrosis in mesenteric lymph nodes.
Lymph nodes of dogs surviving into adulthood had marlied al-
terations. Lymphocytes were depleted in the paracortical areas and
Downloaded from vet.sagepub.com by guest on February 4, 2015h l i c r c x o p i c Pathology o f the Gray Collie Syndrome 235
._._ *---wrU__Lr*__r. s .”. .
.nl -. __
I-zg. 10. An enlargement of Fig. 9 showing collagen fibers (C) and unknown small
fibers (arrow), possibly abnormal myofibrils, interspersed among thc shor-
ter amylold fibers. ~ 3 1 , 2 0 0 .
germinal centers were not seen. Masses of histiocytes contained hemo-
siderin which stained intensely for iron. Many histiocytes contained
intact red blood cells. Dog 6 had foci of necrosis in mesenteric lymph
nodes. In dog 8, the nodal architecture was obliterated by focal areas
of amyloid surrounded by cuffs of large pale histiocytes. Dogs 6 and
7, in which definite amyloid was seen only in the spleen, had preamy-
loid changes : large PAS-positive histiocytes and pale granular pre-
cipitates in the cortical sinuses. Lymph nodes of the non-gray control
dogs did not have remarkable alterations.
Tonsil
The tonsils of dogs 1 to 3 consisted of reticular cells; they were
not populated with lymphocytes. The tonsils of dogs 4 and 5 had
lymphoid hyperplasia with large secondary germinal centers; those
of adult dogs had marked reticuloendothelial hyperplasia and histiocy-
tosis with lymphoid depletion. The tonsils of non-gray dogs 9 to 13
were within normal limits,
Downloaded from vet.sagepub.com by guest on February 4, 2015236 C H I:V I L L I ; / CU T L I P / hr 0 0 N
1.q. 11. Rcd pulp of spleen. Necrotic plasma cell (center) and degenerating degra-
nulated neutrophil (bottom) in thc sinus. Amyloid fibers (center right)
are adjacent to the plasma cell periphery. An atypical plasmablast is at left.
x 11.500.
Thymus
Thymuses of neonatal dogs 1 to 3 appeared similar: their cor-
tical areas were slightly to moderately populated with lymphocytes
and their medullary areas appeared inactive, i.e., Hassall’s bodies were
small and non-cystic and the reticular network was relatively acellular.
Both the immature and adult gray collies had thymic atrophy. The
cortical areas were moderately to markedly depleted of lymphocytes
Downloaded from vet.sagepub.com by guest on February 4, 2015hlicroscopic Pathology of the Gray Collie Syndrome 237
and the medullary areas had histiocytosis and hyperplastic Hassall’s
bodics. Thymuscs of dogs 9 to 13 were atrophic with cystic changes
in the ductal remnants of the branchial pouch.
Alimentary Tract
There was acute diffuse inflammation and edema of the gastric
submucosa in dog 1. Other arcas of the alimentary tract of dogs 1 to 3
and 9 to 13 were normal.
There were focal areas of congestion and hemorrhage in the cecal
mucosa of dog 7. Other changes observed in the alimentary tract of
dogs 4 through 7 were confined to the jejunum and ileum. These were
similar in puppies and adults but more scvere in the lattcr. Jcjunal
villi were short, and crypts were elongated. The lamina propria was
thick and contained numerous lymphocytes and plasma cells, along
with occasional neutrophils. Villous epithelial cells were cuboidal and
had basophilic cytoplasm. There were numerous adhesions between
the epithelial surfaces of adjacent villi (Fig. 12). Similar but more ex-
tcnsivc changcs occurred in the ileum whcrc arcas with short blunt
villi had an appearance similar to colon (Fig. 13). Thc lamina propria
was congested and contained numerous macrophagcs, lymphocytes,
plasma cells, and ncutrophils. Some crypts were distended with debris
and neutrophils resulting in “crypt abscesses”. The ileal epithelium
was disorganized and contained many neutrophils ; epithelial cells
were cuboidal with a basophilic cytoplasm.
Oral Cavity
No lesion was seen in dogs 1 to 3 and 9 to 13. Dogs 4 to 8 had
severe purulent inflammatory lesions of the tongue, nasal cavity, and
gingival mucosa (similar lesions were around the genital orifices). In
dogs 6 to 8, somc deciduous teeth had failed to dislodge from the
alveoli. Although there were microabscesses, purulent inflammation
of the pulp cavity and periodontal membrane was generally absent.
Dogs 4 to 8 had rhinitis, associated with scvere atrophy of the tur-
binate bones in dogs 6 to 8.
Downloaded from vet.sagepub.com by guest on February 4, 2015238 C H T.V I L L E / C U T L IP/ hl o o N
Bone
No abnormality was seen in the bones of neonatal (GCS) or re-
lated non-gray dogs. Dogs 4 to 8 were severely lame and had bone
lesions characterized by vascular degeneration, hemorrhage, and ne-
crosis of the epiphysis (see Fig. 6, ref. 9). The puppies (4 and 5) had
lesions of less severity, generally limited to the epiphysis of the long
bones and ribs ; the cartilaginous plates were not markedly altered.
By contrast, the adult GCS dogs which had survived multiple neu-
tropenic phases had severe skeletal lesions. Hemorrhage and necrosis
occurred chiefly at the epiphyseal plate. Dog 7 had severe lesions
throughout all long bones, the vertebral column, and the ribs.
Lung
Two dogs (2 and 5) died with severe acute purulent broncho-
pneumonia. All major bronchiolar pathways and most alveoli con-
tained neutrophils. Scattered throughout all lobes were focal areas
of eosinophilic coagulative necrosis surrounded by dense rims of neu-
trophilic debris and containing several bacterial colonies. Lesions in
the lungs of dogs 3, 4, 6, and 7 consisted of scattered foci of atelectasis
and emphysema. In dogs 6 and 7, the alveolar walls were thickened
and the media of the interlobular arteries were hyalinized. Dog 8 had
similar lesions as well as thickened alveoli which contained dense
spherical mineralized bodies (Fig. 14) that stained with PAS and von
Kossa techniques.
Dogs 9, 10, and 13, which died during epileptiform seizures, had
moderate to severe pulmonary edema and hyperemia.
Kidney
Dog 8 had slight chronic diffuse pyelitis and diffuse chronic
lymphocytic interstitial nephritis with foci of fibrous scars and intra-
tubular albuminous precipitates extending through the cortex and me-
dulla. The proximal convoluted tubules were filled with dense hyaline
droplets. They also contained, as did cells in the ascending and descend-
ing loops, dense golden brown granules. There was amyloid, which
stained faintly with Congo red, in glomeruli, peritubular areas, and
Downloaded from vet.sagepub.com by guest on February 4, 2015Microscopic Pathology o f thc G r a y Collie Syndromc 239
the media of the interlobular arteries. Scattered glomerular capsules
and arteriolar basement membranes were thickened.
The kidneys of dogs 4 to 7, 9, and 10 had various degrees of
congestion and cloudy swelling of tubular epithelium. In dog 9, this
was severe and accompanied by glomerular swelling with albuminous
precipitates in Bowman’s space. No lesion was seen in kidneys of the
other dogs.
Liver
Diffuse passive hyperemia, hyperplasia of Kupffer’s cells, slight
to moderate fatty degeneration, and depletion of glycogen character-
ized the livers of dogs 1 to 10 and 13. Dogs 5 and 9 also had severe
congestion, hemorrhage, and early necrosis surrounding the central
veins. Small multiple abscesses were scattered throughout the liver
of dog 3. Amyloid was deposited diffusely between hepatocytes and
Kupffer’s cells of dog 8.
Blood Vessels
Vasculitis and perivascular inflammatory lesions were common
findings and are described under the appropriate organs. Dog 7 had
severe vascular lesions. Multiple thrombi were in the veins of the
mesenteric lymph nodes, liver, and heart. There were mineralized,
sub-intimal plaques in the ascending aortas of dogs 5, 7, 8, and 9.
Dog 5 had several foci of myocardial necrosis in the right atrium and
dog 8 had extensive mineralized foci in the abdominal aorta, renal
interlobar arteries, and larger arteries of the lung. Fragmentation and
globular accumulations occurred within scattered foci of ventricular
myocardial degeneration in dogs 5, 9, and 10. Dogs 5 and 9 had ex-
tensive and diffuse hyalinization of the media of small muscular ar-
teries in the spleen, heart, liver, and lung.
Endocrine Glands
The gonads of dogs 9 to 13 appeared normal. Those of 1 to 5
were immature, as were the dogs. Dogs 6 to 8, all males, had abnor-
mal testes which contained giant cells, primary spcrmatocytes, and
Downloaded from vet.sagepub.com by guest on February 4, 2015240 c I I E V I L L E / c I1 T L I P / i\/I 0 0 N
Fig. 12. Jejunal mucosa with short villi, cuboidal epithelium, and adhesions be-
tween thc epithclium of adjacent villi. Dog 6 ; H&E.
Downloaded from vet.sagepub.com by guest on February 4, 2015Microscopic Pathology of the Gray Collie Syndrome 241
spermatogonia; spermatids and mature sperm were absent. The ad-
renals, although judged slightly hyperplastic in some dogs, were not
markedly affected except for dog 8 which contained heavy deposits of
amyloid in the cortical sinuses. The parathyroids and thyroids appeared
within normal limits. No abnormality of the pituitary was seen.
Brain
No CNS lesion was seen in dogs 1 to 8 and 11. Dogs 9, 10, and
13 which died during severe sustained epileptic seizures had laminar
malacic lesions in the motor areas of the cerebral cortex (Fig. 15).
Affected areas consisted of free lipid with destruction of the neuropil
and adjacent neurons and scattered gitter cells ; other inflammatory
cells did not occur in these lesions. No microembolus was seen.
Discussion
In the GCS, cyclic neutropenia appears to be directly responsible
for a wide spectrum of acute and chronic inflammatory lesions, e.g.,
gingivitis, rhinitis, vulvitis, and bronchopneumonia. In spite of clin-
ical repression of these lesions with antibioticsg, severe diarrhea and
aseptic bone necrosis develop and (coincident with lymphoid atrophy
and amyloidosis) progress to cause incapacitation and death of the
affected dog.
Amyloidosis developed in all GCS dogs which survived to adult-
hood. It was preceded by increased levels and heterogeneity of serum
globulins, particularly crz-globulin. Although antibody prepared a-
gainst purified amyloid fibrils reacts in agar gel diffusion with cre-glo-
bulin7, its precise relation to deposition of amyloid is unclear. Chronic
overstimulation of the R E system characterized GCS dogs and we
ascribe lymphoid depletion, elevated globulins, and histiocytosis to
this protracted antigenic stimulation. The role of endotoxin, recently
F g . 13. Ileal mucosa with short blunt villi, cuboidal epithelium, and inflamzd
lamina propria. Dog 7 ; H&E.
F ~ R14.
. Spherical deposits of mineral in the thickened pulmonary alveolar walls of
Dog 8; H & E .
Fig. 15. Foci of malacia in the ganglion cell layer of the motor area of the cerebral
cortex. Dog 9; H & E .
Downloaded from vet.sagepub.com by guest on February 4, 2015242 c H E V I L L E / c U T L I P / hI 0 O N
incriminated in amyloidosis5, is unknown. It appeared that amyloid
was secreted by and polymerizes at the surface of abnormal R E cells
which contain large numbers of polyribosomes but no extensive endo-
plasmic reticulum. Although it was found in other cell types, it is
most probable that this represents either an attempt at phagocytosis
and resorption of existing amyloid by histiocytes and giant cells11 or,
less likely, amyloid formation by abnormal protein-secreting cells
of types other than R E cellsls. Intracellular amyloid has been seen in
abnormal plasma cells with extensive endoplasmic reticulum26. If
aberrant circulating glycoproteins be important in induction of
generalized amyloidosis, it follows that sites with greatest access and
affinity for uptake would therefore be most likely to produce amyloid.
The sites in the spleen at which we saw amyloid are all areas considered
highly responsive to antigenic stimulation. Most amyloid was pro-
duced in the marginal zone and the type of cell producing amyloid is
similar to cells shown by BARIet al.3 to produce amyloid in long-term
cell cultures of spleens from amyloidotic mice.
We were unable to demonstrate any histological lesion in the in-
testinal tract to explain the diarrhea which occurred in neonatal dogs
1 and 2. It may be that either segmental lesions occurred and were not
detected or that diarrhea occurred in the absence of histological al-
teration. Changes in the intestinal tracts of dogs 4 to 7 were inter-
preted as chronic progressive enteritis. The basophilic, cuboidal
epithelial cells were either immature or degenerate. The short, blunt
villi probably resulted in reduced epithelial surface area. These enteric
lesions were assumed to be the cause of the episodes of diarrhea. They
may also explain the malabsorption of fat in the G C W . It is not known
whether enteritis occur secondarily as the result of neutropenia or as
the result of some concomitant primary alteration in the kinetics of
the replacement of intestinal epithelium.
We believe the bone lesion to be an infarct which may result from
thrombosis. The neutrophil functions normally by sequestering and
hydrolyzing fibrin and its dysfunction or absence contributes to dis-
eases involving inflammation and thrombosis4. There was no specific
abnormality suggesting failure of bone formation or resorption. The
bone lesions do not resemble those of the gray lethal mouse12 (per-
sistent spongiosa, failure of bone resorption leading to osteosclerosis
and retarded development), bone lesions that allegedly were due to
immunologic injury24, or aseptic bone necrosis associated with human
autoimmune diseasel4.
Downloaded from vet.sagepub.com by guest on February 4, 2015Microscopic Pathology of the Gray Collie Syndrome 243
The basis for CNS lesions in dogs 9, 10, and 13 we believe to be
of vascular origin. Prolonged epileptiform seizures accompanied by
vasospasm or ischemia are associated with similar laminar malacic le-
sions in manl7. Although epilepsy was seen only in non-gray related dogs
which were older than the GCS dogs, we have no evidence indicating
it to be related to other manifestations of the GCS.
The basis for periodic infectious disease that is due to cycling of
blood cells is unknown. Cyclic neutropenia occurs in children21; it has
also been judged a physiologic parameter in man and its presence used
to indicate normal hemostatic control20. Any causal relationship of
the GCS with other diseases of man involving periodic or cyclic change
in blood cells 6,167 19 is unknown.
Microscopic changes in tissues of 8 dogs with the gray collie syndrome
(GCS) and in 5 related non-gray dogs were described. Three of the GCS dogs died
as neonates, 2 as puppies, and 3 (treated clinically) as adults.
Clinical signs of disease were abnormal hair pigmentation, cyclic neutrope-
nia, diarrhea, lameness, and chronic ulceration of oral and genital mucosa. Lesions
included lymphoid atrophy, amyloidosis, enteritis, aseptic bone necrosis, and acute
and chronic purulent inflammation of several organs. Abnormalities in serum
included decreased albumin and increased y- and az-globulin. Electron microscopy
of the spleen revealed amyloid fibers deposited chiefly at the periphery of the sple-
nic follicles and within the central artery.
'Tissues from non-gray related dogs were normal except for laminar malacia
of the motor areas of the cerebral cortex in 3 of these dogs which probably resulted
from ischemia due to epileptiform seizures.
Acknowledgement
The authors thank Dr. W.S. MONLUX,
National Animal Disease Laboratory,
for reviewing the manuscript.
References
1. ACHONG, B.G. and EPSTEIN, M.A.: A method for preparing microsamples of
suspended cells for light and electron microscopy. J . rcy. nzicr. SOC.84: 107-110
(1964).
2. ANDERSON, D.R.: A method of preparing peripheral leukocytes for electron
microscopy. J . Ultrastrzict. Res. 17: 263-268 (1965).
Downloaded from vet.sagepub.com by guest on February 4, 2015244 CIIEVILLE/CUTLIP/MOON
3. BARI,W.A.; PETTENGILL, O.S. and SORBNSON, G.D.: Electron microscopy and
electron microscopic autoradiography of splenic cell cultures from mice with
amyloidosis. Lab. Invest. 20: 234-242 (1969).
4. BARNHART, M.I. : Importance of neutrophilic leukocytes in the resolution of
fibrin. Fed. Proc. 24: 846-853 (1965).
5. BARTH,W.F.; WILLERSON, J.T.; ASOFSKY, R.; SHEAGREN, J.N. and WOLPF,
S.M. : Experimental murine amyloid. 111. Amyloidosis induced with endo-
toxins. Arthritis Rheum. 12: 615-626 (1969).
6. BREY,0.; GARNER, E. and WELLS,D.: Cyclic thrombocytopatnia associated
with multiple autoantibodies. Brit. med. /. i: 396 (1969).
7. CATHCART, E.S.; COMERFORD, F.R. and COHEN,A.S.: Immunologic studies on
a protein extracted from secondary amyloid. New Engl. J. Med. 273: 143-146
(1965).
8. CHEVILLE, N.F. : Amyloidosis associated with cyclic neutropenia of the dog.
Blood3I: 111-114 (1968).
9. CHBVILLE, N.F.: The gray collie syndrome.]. a m r . vet. med. Ass. 152: 620-630
(1968).
10. COONS,A.H. : Fluoresccnt antibody methods. Zn: General Cytocheinical hle-
thods, Vol. I, pp. 399-422. J.F. DANIELLI, ed. (Academic Press, New Yorlc
1958).
11. De LELLIS,R.A.; SRI RAM,J. and GLENNER,G.G.: Amyloid. IX. Further
kinetic studies on experimental murine amyloidosis. Int. Arch. Allerg)) 37:
175-183 (1970).
12. DOYKOS, J . D . ; COHEN,M.M. and S H K L A RG.: , Physical, histological and ro-
entgenographic characteristics of t h e gray lethal mouse. Anzer. J. A n a t . 121:
29-40 (1967).
13. FORD,L. : Possible pleiotrophic effects of the “gray” gene in collie dogs. Proc.
10th Internatl. Corg. Genet. 83: 1-2 (1958).
14. GOLDIE,I. ; TIBBLIN,G. and SCHELLER, S. : Systemic lupus erythematosis and
aseptic bone necrosis. A c t a med. scand. 182: 55-64 (1967).
15. JOHNSON, K.H. ; OSBORNE, C.A. and BARNES, D.M. : Intracellular substance
with some amyloid staining affinities in pancreatic acinar cells of a cat with
amyloidosis. Path. vet. 7: 153-162 (1970).
16. KRETSCHMER, R.; AUGUST,C.S.; ROSEN,F.S.and JANEWAY, C.A.: Recurrent
infections episodic lymphopenia and impaired cell ular immunity. Ne~vEngl.
/. Med. 281: 285-290 (1969).
17. LINDENBERG, R. : Patterns of CNS vulnerability in acute hypoxaemia including
anaesthesia accidents. Zn: Selective Vulnerability of the Brain in Hypoxaemia,
pp. 189-209. J.P. SCHADE andW.13. MCMENEMEY, ed. (Blackwell, Oxford1963).
18. LUND,J.E.; PADGETT, G.A. and OTT, R.L.: Cyclic neutropenia in gray collies.
Blood 29: 453-461 (1967).
19. MORLEY,A.A. and STOHLMAN, F. : Periodic hemoconcentration. Science 165:
1025-1027 (1969).
20. MORLEY,A.A.; BAIKIE,A.G. and GALTON,D.A.G.: Cyclic leucocytosis as
evidence for retention of normal homeostatic control in chronic granulocytic
leukzmia. Lancet ii: 1320-1323 (1967).
21. PAGE,A.R. and GOOD,R.A.: Studies o n cyclic neutropenia. J. Dis. Child. 94:
623-662 (1957).
Downloaded from vet.sagepub.com by guest on February 4, 2015hlicroscopic Pathology of the Gray Collie Syndrome 245
22. PEARST:, A.G.E. : Histochemistry ; ‘Theoretical and Applied (Little, Boston
1960).
23. ROBERTS,S.R.; DELLAPORTA, A. and WINTER,F.C.: The collie ectasia syn-
drome. Pathology of eyes from young and adult dogs. Amer.]. Ophth. 62: 1-23
(1967).
24. SIMMONS, D.J. and SIMbioNs, R.L.: Skeletal changes in murine runt disease.
Ameu.]. A n a f . 121: 15-28 (1967).
25. WINDHORST, D.B.; LUND,J.E.; DECKER, J. and SWATEZ,I.: Intestinal mal-
absorption in the gray collie syndrome. Fed. Pvoc. 26: 260 (1967).
26. ZUCKER-FRANKLIN, D. and FRANKLIN, E.C. : Intracellular localization of hu-
man amyloid by fluorescence and electron microscopy. A m w . ./. Path. 59:
23-41 (1970).
,\uthor’s ilddicss: Dr. N. I:. CIII:VILLL,
l h c National Animal Iliscaso L i b r m t o r y , Vctcrinarg Scienccs Ilcscsrch I l i v i -
S K ~ ,ARS, USDA, 1’. 0. Ikix 70, AI)IP.J,Iowa 50010[ USA).
Downloaded from vet.sagepub.com by guest on February 4, 2015You can also read