A Boxer Dog with Chronic Hypertrophic Gastritis Resembling Menetrier's Disease in Man
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Vet. Pathol. 13: 172-185 (1976)
A Boxer Dog with Chronic Hypertrophic Gastritis Resembling
Menetrier’s Disease in Man
INGRID VAN DER GAAG,R. P. H A P Pand
~ W. TH.C. WOLVEKAMP
Institute of Veterinary Pathology, Small Animal Clinic and Institute of Radiology, State
University, Utrecht
Abstract. Chronic hypertrophic gastritis in a 7-year-old Boxer dog is described. This
gastritis resembles Menetrier’s disease in man. The dog was emaciated, lethargic, vomiting
and had a poor appetite over a 4-month period. There was anaemia, and the blood smear
was characterized by hypochromasia, strong anisoplania and striking poikilocytosis. There
was a protein loss and at a later stage of the disease, a hypoalbuminaemia. On gastroscopic
examination the plicae gastricae were numerous and strongly marked; moreover, they
were granulated with numerous small haemorrhages. Radiographically, the stomach had
a marked folding, primarily at the greater curvature. The passage of contrast medium from
the stomach into the duodenum was strongly retarded. The pathological findings included
macroscopical folding caused by local gland cell hyperplasia in the body as well as the
pylorus, foveolar hyperplasia and, in the fundus and in the corpus near the greater curva-
ture, folding of the muscularis mucosae and the submucosa. A superficial gastritis was
found particularly in the fundus and corpus, whereas the pyloric antrum showed a more
diffuse inflammation.
Chronic hypertrophic gastritis, a well-known disease in man [9, 11, 16,
19, 20, 251, has not been described in the dog. The present case was in a
male Boxer dog with chronic hypertrophic gastritis that clinically, radio-
logically and pathologically resembled Menetrier’s disease in man.
Materials and Methods
The absorption function of the small intestine was examined by the xylose tolerance
test [12]. Faecal excretion of fat and fatty acids was estimated quantitatively over a 4-day
period by the method of VAN DE KAMER et al. [16]. Proteolytic enzymes were assayed semi-
quantitatively by the gelatine digestion test [I31 in faecal samples diluted 1 : 10, 1 : 100,
1 : lo00 and 1 :10 OOO with aqua dest. Loss of plasma protein via the gastrointestinal tract
was traced by the Gordon test, in which 50 pCi of 1Y51-polyvinyl-pyrrolidone (1*51-PVP)
were administered intravenously. Faecal excretion of radioactivity was measured during
the next 8 days by well-type liquid scintillation counter (Nuclear, Chicago, Ill.) as described
P81.
Downloaded from vet.sagepub.com by guest on August 24, 2015VAN DER GAAG/HAPPE/WOLVEKAMP 173
The dog was sedated with AcepromazineB and methadone HCI, and gastroscopy was
performed with a fiberscope (Olympus, C F model, type LB) after food and water had been
withheld for 18 and 12 h, respectively. Haematological and clinical chemical examinations
were done (table I).
Radiographs were obtained with a conventional X-ray unit (Siemens Gigantos,
Siemens A.G. W.W. Med., Erlangen, FRG), with exposure factors of 52 kV and 50 mA
(lo00 mA) for the lateral and 56 kV and 100 mA (lo00 mA) for the ventrodorsal radio-
graphs, at a film to focus distance of 115 cm. Regular-speed intensifying screens (‘Saphir’
universal intensifying screens, Siemens) and 30 x 40 cm black and white films (Agfa-
Gevaert films, type Curix-R.P.2) were used with an 8: 1 ratio grid mounted in a Buckey
device. Radiographs printed on this paper were electronically compensated with Log-
Etronic type IogE M. 3516 (Logetronics Ltd., Zurich, Switzerland). Radiographic contrast
examination of the stomach was obtained with barium suspension consisting of micronized
BaSO, powder (Micropaque, Damancy & Co. Ltd., England), water, and stabilizers
mixed to a creamy consistency [21]. The mixture was administered through a stomach
tube at a rate of 5 ml/kg body weight [25].
Beforecontrast examination, food and water were withheld for 24and 12 h, respectively.
The dog was not sedated during the examination. For histological examination, tissues
were removed 8 h after death and were fixed in 10% formalin. Paraffin sections, 6 pm thick,
were stained with haematoxylin and eosin (HE), van Gieson, periodic acid-Schiff (PAS),
alcian blue, toluidine blue and von Kossa stains.
Case History
An emaciated 7-year-old male Boxer dog with a 4-month history of vomiting, diarrhoea
and poor appetite was presented at the Small Animal Clinic, Utrecht. Vomiting occurred
regularly regardless of the type of meal. The dog was lethargic and weighed 17.5 kg. The
skin had moderate turgor, and the haircoat over the dorsum of the trunk was thin. The
mucous membranes were pale, and there was a purulent discharge from both nostrils.
The right tonsil was enlarged. The abdomen was tucked up but on abdominal palpation
the dog showed no signs of pain, and no abnormal masses were found. The faeces were
greenish and watery and contained neither blood nor mucus. The dog was given small
quantities of a homogeneous semimoist cereal diet every 4 h during its stay in the hospital.
The dog’s general condition improved considerably during the first 2 weeks, and it had
a healthy appetite. There was no vomiting. The faeces varied from soft and unformed to
normal. During this period body weight increased by 1.5 kg. Thereafter the condition
deteriorated. Vomiting occurred regularly, and appetite declined. In spite of treatment
with anabolic corticosteroids, antibiotics and B complex vitamins, there was continuing
deterioration, and the dog died 26 days after admission. Its weight had fallen to 14.6 kg.
Results
Blood values for urea nitrogen, alkaline phosphatase, serum glutamic
oxaloacetic transaminase, serum glutamic pyruvic transaminase, cholin-
esterase, bilirubin, total lipids, sodium, potassium and inorganic phosphate
Downloaded from vet.sagepub.com by guest on August 24, 2015174 V A N DER GAAG/HAPP~/WOLVEKAMP
Table I. Hematologic and chemical analyses
Day I Day7 Day I3 Day 19 Normal Method
values
Hemoglobin, mmol Fe(Hb)/liter 6.52 5.34 4.30 4.60 8.7-1 I .2 cyanohemoglobin method
(Merck No. 3317)
Packed cell volume, YO 30 24 22 21 42-54 micromethod
Erythrocytes, IO’*/liter 4.56 6.00-7.50 Coulter counter model D
MCHCI, mmol Fe(Hb)/liter 19.5 20.5-22.5
MCV, fl 48 70-80
MCH, fmol 1 .o 1.45-1.75
Reticulocytes, YO I .4Chronic Hypertrophic Gastritis I75
Intestinal absorption of fat was studied after the dog had been maintained
on the test diet for 5 days. The amount of fat excreted in the faeces during
4 days was 14.6 g. Considering the calculated quantity of fat consumed in
the diet, the absorption of fat appeared to be greater than 90%. Proteolytic
enzymes were detectable even in faecal dilutions of 1 : 1000. The loss of
1251-PVPin the faeces was 16.3% of the administered dose of 1251-PVPin
5 days. In eight clinically normal dogs the loss was less than 5 % in 5 days.
Routine urinalysis showed no abnormalities.
On gastroscopic examination the stomach appeared to contain a great
amount of fluid. The stomach of the normal dog is empty after fasting. The
gastric mucosa was abnormal in that the folds were numerous, pronounced,
and granulated with many small haemorrhages. Several biopsy specimens
of the mucosa showed hypertrophic gastritis, with infiltration by mono-
nuclear cells, polymorphonuclear leucocytes and mast cells. There was a
slight increase in the amount of connective tissue. The biopsies contained
only the superficial part of the mucosa, suggesting that the mucosa was
abnormally thick.
Thoracic radiographs showed no abnormalities. Owing to the absence of
a normal quantity of intraabdominal fat, the abdominal radiographs were
difficult to interpret, but the shadow caused by the stomach was striking.
The stomach was greatly dilated, the shadow of the greater curvature ending
outside the arch of the last rib. The contents appeared to be fluid, and there
was a considerable amount of gas. Because of the gas in the widened antrum,
the contracted state of the pylorus was evident. A thorough radiographic
examination of the stomach followed. Before the actual contrast examina-
tion a new set of plain radiographs was taken, and in these the stomach still
appeared to be distended. In spite of this dilation, however, the stomach
wall appeared to be markedly thickened, and there was a coarse folding of
the wall of the fundus and corpus. Image-intensified fluoroscopy was used
to monitor the filling of the stomach. There was considerable distention of
the stomach. Strong peristaltic contractions were still being transmitted from
the corpus via the antrum to the pylorus. In spite of this, the pylorus did not
open. Also, there was extensive folding of the wall of the fundus and corpus,
particularly over the greater curvature. The stomach wall appeared to be
diffusely thickened (fig. 3,4).
The broad and tall mucosal folds resembled filling defects lengthwise
across the fundus and corpus. The surfaces of these folds were slightly
irregular. As the radiographic aspects of the antrum and pylorus strongly
resembled those of pyloric stenosis, the contrast medium was followed as
Downloaded from vet.sagepub.com by guest on August 24, 2015176 VAN DER GAAG/HAPP~/WOLVEKAMP
-
a
., .
-*
"5
d
F'Chronic Hypertrophic Gastritis 177
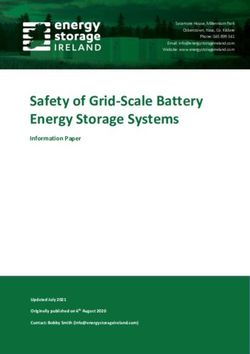
Fig. 3. Stomach, filled with contrast medium, DS. Lateral position. Big and broad
folds of the wall of the fundus and corpus. The height of one fold is outlined by the black
arrows.
Fig. 4. Stomach filled with contrast medium VD. Recumbent position. Same impres-
sion as on figure 5. Enlarged mucosal folds (arrow).
The dog’s body was extremely emaciated. The major abnormality was a
striking change in the stomach. Both in the fundus and the corpus, the mu-
cosa was considerably thickened and folded, particularly along the greater
curvature (fig. 6). The folding varied from rather straight and long to
strongly tortuous, the latter resembling the pattern of gyri and sulci of the
brain (fig. 7). The thickness of these tortuous rolls varied from 1.5 to 2 cm.
The thickness of the mucous membrane of the pyloric antrum was also
slightly increased.
The superficial lymph nodes were enlarged. There was rhinitis, and the
right side of the mouth had an ulcerative inflammation as well as an epulis,
1-1.5 cm in diameter. There was fibrosis of the left atrioventricular valve of
the heart. Anthracosis and a number of calcified nodules were in the lungs.
The spleen showed haemosiderosis and fibrosis along its margin. There was
a 2 x 2 cm tumour in the right testicle.
Microscopic examination of the stomach showed three changes. In the
fundus and corpus, near the lesser curvature, the changes were restricted to
Downloaded from vet.sagepub.com by guest on August 24, 2015178 V A N DER GAAG/HAPPE/WOLVEKAMP
5
6
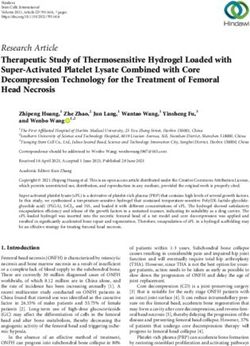
Fig. 5. Contrast radiograph, 8 h after administration of contrast medium. Stomach is
still distended. Concentration of contrast medium in the caecum and colon. Notice con-
tours of the pylorus (arrows). Antrum is distended.
Fig. 6. Chronic hypertrophic gastritis, particularly in the fundus and corpus. Folding
is strongest along the greater curvature.
Fig. 7 . Chronic hypertrophic gastritis (corpus near the greater curvature). Pattern of
the gyri and sulci of the brain.
Fig. 8. Chronic hypertrophic gastritis (corpus near the lesser curvature). Folding
caused by local glandular hyperplasia and foveolar hyperplasia. Muscularis and sub-
mucosa unaltered. HE.
Downloaded from vet.sagepub.com by guest on August 24, 2015Chronic Hypertrophic Gastritis 179
Fig. 9. Chronic hypertrophic gastritis (corpus near the greater curvature). Folding
caused by local glandular hyperplasia, foveolar hyperplasia and folding of the muscularis
and submucosa. Focal secondary folding of the muscularis mucosae and subrnucosa.
Focal cyst formation (arrow). HE.
Fig. 10. Chronic hypertrophic gastritis (pyloric antrum). Thickening of the mucosa
owing to glandular and foveolar hyperplasia. HE.
Downloaded from vet.sagepub.com by guest on August 24, 2015180 V A N DER GAAG/HAPPI?/WOLVEKAMP
the mucosa. As the result of hyperplasia of the deep gastric glands, which
were up to 1.0 mm long, and hyperplasia of the foveolae, which were up
to 0.6 mm deep, the mucosal folds were up to 1.6 mm thick. The muscularis
mucosae and the submucosa appeared to be normal (fig. 8). In the fundus
and corpus, near the greater curvature identical changes were seen. The
glands were up to 2 mm long and the foveolae up to 0.6 mm deep. Here the
muscularis mucosae and the submucosa also had folds up to 12 mm thick
(fig. 9). In some areas a secondary folding of the muscularis and the sub-
mucosa had occurred. Between the areas with these two types of changes,
both types occurred. Thickening of the mucosa had also taken place in the
pyloric antrum but without tortuosity. The mucosa here was up to 3.0 mm
thick, with glands up to 1.0 mm long and foveolae up to 2.0 mm deep
(fig. 10).
In areas with the most significant abnormalities, the gastric pits seemed
to be reduced in number. The columnar superficial epithelial cells were
often cuboidal. The mucous neck cells were normal. Cysts were found not
only in the fundus and corpus, but also in the pyloric antrum. Occasionally
these cysts were covered by slightly papilliform proliferation and elsewhere
by flattened epithelial cells.
The inflammatory response, consisting mainly of lymphocytes, plasma
cells and some fibrous connective tissue, was localized in the surface of the
fundus and the corpus, whereas in the pyloric antrum it was more diffuse
throughout the lamina propria.
In the glands, many interepithelial lymphocytes were seen. The number
of mitoses of the epithelial cells seemed to be increased, not only in the
neck region, but also in more basal areas (fig. 11). Many parietal cells
contained a poorly stained, swollen nucleus with a distinct chromatin mar-
gin. The nucleus often contained an amorphous PAS-positive round body
or a number of PAS-positive granules (fig. 1 I). These nuclear inclusions did
not stain with PAS after treatment with diastase, which suggests that they
were composed of glycogen.
The surface epithelial cells and the mucous neck cells stained only vaguely
PAS-positive, except for a thin edge just beneath the cell surface, which was
clearly positive. This was in contrast to mucous cells and the cells of the
cysts, which were clearly positive.
Except for many cystic crypts of Lieberkuhn in the duodenum, there were
no other changes in the intestine. The hypoactive testicle contained an inter-
stitial cell tumour. Many calcium deposits were found in the lumina of the
kidney tubules and in Bowman’s spaces.
Downloaded from vet.sagepub.com by guest on August 24, 2015Chronic Hypertrophic Gastritis 181
Fig. I I . Chronic hypertrophic gastritis (corpus near the greater curvature). Chronic
superficial gastritis, interepithelial lymphocytes, mitoses of the epithelial cells in the neck
region (white arrows) and amorphous PAS-positive round bodies in some parietal cells
(black arrow and inset). The surface epithelial cells and mucous neck cells of the isthmus
stain only vaguely PAS-positive in contrast with the more basal mucous neck cells. PAS.
Discussion
Chronic hypertrophic gastritis has not been reported previously in dogs.
This condition slightly resembles the parasitic changes seen in the gastric
fundus of the pig and the horse and in the abomasum of ruminants [14].
However, there are a great many eosinophils in the parasitic lesions that
were lacking in our Boxer.
The type of gastritis in this dog bears a strong resemblance to Menetrier’s
disease in man [18]. The disease is also known as ‘giant rugae gastritis’,
‘gastritis hypertrophica gigantica’ or ‘Riesenfalten-gastritis’[8]. This dis-
order may be suspected in man when there are fatigue, vomiting, emaciation,
or upper abdominal complaints of vague to typical ulcer or colic. In most
cases there are no significant abnormalities except the patient has an un-
pleasant sensation when the upper abdomen is palpated. Occasionally there
is anaemia and oedema of the legs. There may also be ascites. Other factors
in man are hypoalbuminaemia, intestinal loss of protein, wide tortuous folds
of the stomach on radiographic examination, and polyadenomes en nappe
on pathologic-anatomic examination. The lethargy, emaciation and vomit-
ing in our dog were similar to that in Menetrier’s disease in man. On stomach
palpation there was no pain and the dog was anaemic. The anaemia probably
Downloaded from vet.sagepub.com by guest on August 24, 2015182 VAN DER GAAG/HAPPE/WOLVEKAMP
was due to blood loss and defective erythropoiesis from iron deficiency. The
microcytosis, hypochromasia, leptocytosis and poikilocytosis (fig. l), as
well as the reticulocytopenia, the increased osmotic resistance of the red
cells and the high platelet count, are compatible with this [2,26]. Blood loss
was also demonstrated by endoscopy. Oedema and ascites were absent.
Hypoalbuminaemia occurred at a later stage. The results of the blood
and urine tests showed hypoalbuminaemia was not caused by poor liver
function, nor by loss of protein via the kidneys. It appeared from the 1251-
PVP test that there was a considerable loss of protein in the faeces. This loss
probably took place via the abnormal mucosa of the stomach. Parasitic
infestations of the stomach in pigs and ruminants also cause loss of plasma
proteins [7, 111.
Although the various serum proteins are lost through the affected gastric
mucosa at the same rate, irrespective of molecular size, one might expect
the lowering of circulating albumin and y-globulin concentrations to be
more persistent since these two have the slowest rates of normal turnover
[30] and hence are replenished at the slowest rates. In the absence of other
factors, this would result in a relative elevation of the other serum proteins.
In our dog, both total serum protein concentration and the relative and
absolute levels of albumin were consistently low (table I). However, there
were absolute elevations of a,-globulin and fi,-globulin as well as normal
or elevated levels of y-globulin. The only apparent explanation for this finding
was the chronic inflammation of the stomach.
Other serum components may be lost in patients with gastrointestinal
protein loss. This may explain the decreased calcium concentration. Cell
damage may have induced the increase of lactate dehydrogenase. The results
of the fat balance tests, the normal quantity of proteolytic enzymes in the
faeces and the negative pathologic findings suggest that the small intestinal
functions of fat and protein digestion and absorption were normal. The
xylose tolerance test curve was flat and rose only slightly. In our dog, how-
ever, the results of this test are invalid as a measure of intestinal absorption
[ 121, because the radiographic studies indicated food passage through the
stomach was retarded.
Radiographically, there is a remarkable similarity between patients with
Menetrier’s disease [4, 5, 9, 231 and our dog. In addition to the marked
folding, the location of the gross lesions, primarily in the greater curvature
of the stomach, is also strikingly similar. I n man, carcinoma of the stomach
is always mentioned as a differential diagnosis for these radiographic ab-
normalities, but this is not the case in the dog. Carcinoma of the stomach
Downloaded from vet.sagepub.com by guest on August 24, 2015Chronic Hypertrophic Gastritis 183
wall in the dog is radiographically different, for it results in either a noticeable
decrease in the number of rugae or a distinct local increase in thickness of
the stomach wall, usually of the pyloric antrum [I, 201. The radiographic
findings in this dog were similar to those in one of our previous dogs with
gastric leucosis. The dog’s stomach wall was diffusely infiltrated with
leucotic cells.
The pathologic findings in our dog are also strikingly similar to those of
Menetrier’s polyadenomes en nappe [ 181. He reported two types of changes
in the stomach - polyadenomes polypeux, multiple discrete polyps, and
polyadenomes en nappe, well-defined areas with a dense, complex folding
caused by hypertrophy and hyperplasia of the mucosa. The latter type is
known as Menetrier’s disease. In man this abnormality is in the central
part of the stomach, particularly along the greater curvature. The folds,
occasionally about 1 cm thick, more or less follow the course of the greater
curvature. They sometimes strongly resemble the pattern of gyri and sulci
in the brain [8]. Our dog had this pattern. This disorder in humans has been
divided into four types as follows : (a) glandular hyperplasia without exten-
sions of the submucosa ; (b) glandular hyperplasia with septal extensions
from the submucosa, which throw the mucosa into folds; (c) little or no
hyperplasia but with folds formed by septal extensions from the submucosa,
and (d) partial or complete glandular atrophy, foveolar hyperplasia and
septal extensions [22].
In our dog we found type a particularly in the fundus and corpus close
to the lesser curvature, whereas type b was mostly near the greater curvature.
There was some resemblance to type d in that there was occasionally foveolar
hyperplasia. No manifestations of type c were seen. The inflammatory in-
filtrate may vary markedly in man. At times there are many lymphocytes,
plasma cells and eosinophils throughout the mucosa [lo], whereas at other
times there may only be a distinct superficial gastritis [15]. In some cases
there is no inflammation at all. Superficial gastritis was seen in our dog,
but it appeared to be more chronic than that in man [15]. According to one
classification the gastritis would be described as local hypertrophic glandular
and local hypertrophic proliferative gastritis [27]. One report used the term
gastric mucosal hypertrophy and suggested that gastritis is a secondary rather
than primary phenomenon [31]. With this view, the lesion should not be
regarded as hypertrophic gastritis. Another author recently described this
lesion as glandular hyperplasia with foveolar hyperplasia accompanied by
chronic gastritis [32]. He also believes that true hypertrophic gastritis does
not exist.
Downloaded from vet.sagepub.com by guest on August 24, 2015184 V A N DER GAAG/HAPPE/WOLVEKAMP
In man, Menetrier’s disease has been regarded as a potential site of car-
cinoma, but there was no evidence of this in the dog. Also in man, the disease
occurs four times as often in males as in females [8, 19, 231. One report
suggests that man usually is affected between the ages of 30 and 50 [29],
and another states the disease is more likely to occur between the ages of
45 and 65 [19].
Our male dog was 7 years old. Its age relative to the usual lifespan of the
Boxer was thus comparable to that of patients with Menetrier’s disease. The
cause of Menetrier’s disease is not known. A congenital abnormality [8],
a relationship with multiple adenomas of endocrine origin [17], or even lues
[8] have been considered.
Although the Boxer also had an interstitial cell tumor of the testicle,
it is impossible to establish a causal relationship between these two ab-
normalities.
Although the chronic hypertrophic gastritis described here was not iden-
tical to that of Menetrier’s disease, there was a remarkable resemblance in
its clinical as well as its pathologic-anatomic aspects.
References
1 BERG, P.; RHODES,W.H., and O’BRIEN,J.B.: Radiographic diagnosis of gastric
adenocarcinoma in a dog. J. Am. vet. rad. SOC.5: 47-53 (1964).
2 BRITTON, C.J.C.: in WHITBYand BRlnoN Disorders of the blood; 10th ed., p. 63
(Churchill, London 1969).
3 BRUCKNER, J.: Estimation of the direct and total bilirubin in serum investigations and
observation by a modified method. Clinica chim. Acta 6: 370-376 (1961).
4 BURKLE,G. und FROMMHOLD, W.: Tumorsimulierende Magenerkrankungen und ihre
Differentialdiagnose. I. Fortschr. Rontgenstr. 114: 231-246 (1971).
5 CUMMACK, D.H.: Gastro-intestinal X-ray diagnosis. A descriptive atlas, p. 76 (Living-
stone, Edinburgh 1969).
6 DACIE,J. V. and LEWIS,S.M. : Practical haematology ; 4th ed., pp. 30-34, 72, 166- 173
(Churchill, London 1970).
7 DEY-HAZRA, A.; KOLM,H.P.; ENIGK,K. und GRIESE,W.: Zum gastrointestinalen
Plasmaproteinverlust beim Hyostrongylus-Befall des Schweines. 2. Parasitkde 38:
14-20 (1 972).
8 DOERR,W.; SEIFERT, G. und UEHLINGER, E.: Spezielle pathologische Anatomie,
vol. 2/1, pp. 215-216, 246-252, 273-279, 543 (Springer, Berlin 1971).
9 FELDMAN, M. :Clinical roentgenology of the digestive tract, p. 174 (Williams & Wilkins,
Baltimore 1957).
10 G ~ R S C HH., : Uber die Gastritis hypertrophica gigantea. Menetriersche Erkrankung.
Ergebn. allg. Path. path. Anat. 46: 156-205 (1965).
Downloaded from vet.sagepub.com by guest on August 24, 2015Chronic Hypertrophic Gastritis 185
1 1 HALLIDAY,
G. J. and MULLIGAN,
W.: Parasitic hypoalbuminaemia studies on type 11
ostertagiosis of cattle. Res. vet. Sci. 9: 224-227 (1968).
12 HILL,F.W.G.; KIDDER,D.E., and FREW,J.: A xylose absorption test for the dog.
Vet. Rec. 87: 250-255 (1970).
13 JASPER,D.E.: A simple diagnostic test for pancreatic enzyme deficiency in dogs.
N. Am. Vet. 35: 523-525 (1954).
14 JOEST,E.: Handbuch der speziellen psthologischen Anatomie der Haustiere, vol. V,
pp. 467-468 (Parey, Berlin 1970).
15 JONES,E.A.; YOUNG,W.B.; MORSON, B.C., and DAWSON, A.M.: A study of six
patients with hypertrophy of the gastric mucosa with particular reference to albumin
metabolism. Gut 13: 270-277 (1972).
16 KAMERVAN DE,J.H.; TEN BOKKEL HUININK, H., and WEYERS, H.A.: Rapid method
for the determination of fat in feces. J. biol. Chem. 77: 347-355 (1949).
17 KENNEY,F.D.; DOCHERTY, M.B., and WAUGH,J.M.: Giant hypertrophy of gastric
mucosa. A clinical and pathologic study. Cancer 7: 671-681 (1954).
18 MENETRIER,P.: Des polyadenomes gastriques et de leurs rapports avec le cancer de
I'estomac. Archs Phys., 4e serie, pp. 32-55 (1888).
19 MORSON, B.C. and DAWSON, I. M. P.: Gastrointestinal pathology, pp. 74-76 (Oxford,
London 1972).
20 MURRAY,M.; ROBINSON, P. B.; KEATING, F. J.; BAKER,G. J., and LAUDER, I. M.:
Primary gastric neoplasia in the dog. A clinical-pathological study. Vet. Rec. 91:
474-479 (1972).
21 OP DEN ORTH,J.O.: De dubbele contrastmethode; een essentieel onderdeel van het
rontgenonderzoek van maag en bulbus. Ned. Tijdschr. Geneesk. If5: 535-538 (1971).
22 PALMER, E. D.: Gastritis, a reevaluation. Medicine, Baltimore 33: 199-290 (1954).
23 REINDERS, J.E. and LENS,J.: Het syndroom van Menetrier. Ned. Tijdschr. Geneesk.
116: 2094-2099 (1972).
24 Fotometrische bepaling van ureum in bloed volgens het Nederlands Normalisatie
Instituut. K"266. R. I.V. Standaard Voorschrift (1966).
25 ROOT,C. R. and MORGAN, J. P. : Contrast radiography of the upper gastrointestinal
tract in the dog. J. small Anim. Pract. 10: 279-285 (1969).
26 SCHALM, O.W.: Veterinary hematology; 2nd ed., p. 599 (Lea & Febiger, Philadelphia
1965).
27 SCHINDLER, R.: ubersichten. Chronische Gastritis. Klin. Wschr. 44: 601-612 (1966).
28 SCHWARTZ-PORSCHE, D. M. und BOTSCH,H. : Nachweis des gastroenteralen Protein-
verlustes beim Hund mit 's' I-PVP (Gordon-Test). Berl. Munch. tierarztl. Wschr. 83:
313-318 (1970).
29 TAENZER, V. and RUIZ-TORRES, A. : Gastromegalie bei Polyadenomatosis (Menetrier-
sches Syndrom). Fortschr. Rontgenstr. 107: 288-290 (1967).
30 WALDMANN, T. A. : Protein-losing enteropathy. Gastroenterology 50: 422-443 (1966).
31 WHITEHEAD, R.: Mucosal biopsy of the gastrointestinal tract, pp. 48-51 (Saunders,
London 1973).
32 WOLFF,G.: Chronische Gastritis, pp. 17C171 (Barth, Leipzig 1974).
INGRIDVAN DER GAAG,Veterinary Medicine, State University Utrecht, Biltstraat 166,
Utrecht (the Netherlands)
Downloaded from vet.sagepub.com by guest on August 24, 2015You can also read