A contrast-enhanced-CT-based classification tree model for classifying malignancy of solid lung tumors in a Chinese clinical population
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
A contrast-enhanced-CT-based classification tree model for
classifying malignancy of solid lung tumors in a Chinese clinical
population
Xiaonan Cui1,2^, Marjolein A. Heuvelmans3,4, Grigory Sidorenkov3, Yingru Zhao1, Shuxuan Fan1,
Harry J. M. Groen5, Monique D. Dorrius2, Matthijs Oudkerk6, Geertruida H. de Bock3,
Rozemarijn Vliegenthart2, Zhaoxiang Ye1
1
Department of Radiology, Key Laboratory of Cancer Prevention and Therapy, Tianjin Medical University Cancer Institute and Hospital, National
Clinical Research Centre of Cancer, Tianjin, China; 2Department of Radiology, University Medical Center Groningen, University of Groningen,
Groningen, The Netherlands; 3Department of Epidemiology, University Medical Center Groningen, University of Groningen, Groningen,
The Netherlands; 4Department of Pulmonology, Medisch Spectrum Twente, Enschede, The Netherlands; 5Department of Pulmonary Diseases,
University Medical Center Groningen, University of Groningen, Groningen, The Netherlands; 6Faculty of Medical Sciences, University of
Groningen, Groningen, The Netherlands
Contributions: (I) Conception and design: X Cui, Z Ye, R Vliegenthart; (II) Administrative support: Z Ye, R Vliegenthart, MA Heuvelmans; (III)
Provision of study materials or patients: Z Ye; (IV) Collection and assembly of data: X Cui, Y Zhao, S Fan; (V) Data analysis and interpretation: X
Cui, G Sidorenkov; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Correspondence to: Zhaoxiang Ye, MD. Tianjin Medical University Cancer Institute and Hospital, Huan-Hu-Xi Road, Ti-Yuan-Bei, He Xi District,
Tianjin 300060, China. Email: yezhaoxiang@163.com.
Background: To develop and validate a contrast-enhanced CT based classification tree model for
classifying solid lung tumors in clinical patients into malignant or benign.
Methods: Between January 2015 and October 2017, 827 pathologically confirmed solid lung tumors
(487 malignant, 340 benign; median size, 27.0 mm, IQR 18.0–39.0 mm) from 827 patients from a dedicated
Chinese cancer hospital were identified. Nodules were divided randomly into two groups, a training group
(575 cases) and a testing group (252 cases). CT characteristics were collected by two radiologists, and
analyzed using a classification and regression tree (CART) model. For validation, we used the decision
analysis threshold to evaluate the classification performance of the CART model and radiologist’s diagnosis
(benign; malignant) in the testing group.
Results: Three out of 19 characteristics [margin (smooth; slightly lobulated/lobulated/spiculated),
and shape (round/oval; irregular), subjective enhancement (no/uniform enhancement; heterogeneous
enhancement)] were automatically generated by the CART model for classifying solid lung tumors. The
sensitivity, specificity, PPV, NPV, and diagnostic accuracy of the CART model is 98.5%, 58.1%, 80.6%,
98.6%, 79.8%, and 90.4%, 54.7%, 82.4% 98.5%, 74.2% for the radiologist’s diagnosis by using three-
threshold decision analysis.
Conclusions: Tumor margin and shape, and subjective tumor enhancement were the most important CT
characteristics in the CART model for classifying solid lung tumors as malignant. The CART model had
higher discriminatory power than radiologist’s diagnosis. The CART model could help radiologists making
recommendations regarding follow-up or surgery in clinical patients with a solid lung tumor.
Keywords: Pulmonary nodules; classification tree model; prognosis; lung cancer
^ ORCID: 0000-0002-4019-6680.
© Journal of Thoracic Disease. All rights reserved. J Thorac Dis 2021;13(7):4407-4417 | https://dx.doi.org/10.21037/jtd-21-588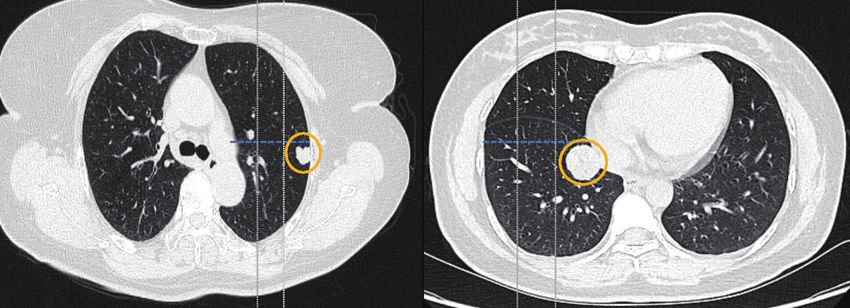
4408 Cui et al. A contrast-enhanced CT based classification tree model for classifying solid lung tumors
Submitted Apr 03, 2021. Accepted for publication Jun 25, 2021.
doi: 10.21037/jtd-21-588
View this article at: https://dx.doi.org/10.21037/jtd-21-588
Introduction of CT enhancement can differentiate the nature of the lung
tumor (12,13). Absence of significant tumor enhancement
The diagnosis of lung nodules is a common and expensive
(≤15 HU) at contrast-enhanced CT is strongly predictive of
challenge in medicine. Chest computed tomography (CT)
a benign nature (11). Therefore, the use of difference in CT
is widely used for lung disease diagnosis (1,2). Lung nodules
density between non-contrast and contrast CT may help to
are divided into solid and sub-solid based on their density
establish a classification model to effectively improve the
on CT, and the consensus of multiple guidelines is that
diagnosis of pulmonary nodules, especially for patients with
lesions of different densities should be managed differently
a large solid tumor considered for surgery.
(3-6). Sub-solid nodules are often considered to be early
Our purpose was to develop and to validate a classification
stage adenocarcinoma (6,7), however, the histologic types
tree model based on contrast-enhanced CT characteristics of
of solid nodules or tumors vary widely. The 2015 World
solid lung tumors to differentiate between the malignant or
Health Organization Classification of Lung Tumors reports
benign nature in clinical preoperative patients.
there are four major histological types of solid pulmonary We present the following article in accordance with the
malignancies, including adenocarcinoma, squamous cell TRIPOD reporting checklist (available at https://dx.doi.
carcinoma, large cell carcinoma, and small cell carcinoma; org/10.21037/jtd-21-588).
and four major types of benign lesions, including pulmonary
hamartoma, inflammatory myofibroblastic tumor, sclerosing
pneumocytoma and granuloma (8). This brings a challenge Methods
to the stratification of solid tumors into malignant or benign The institutional ethics committee board of Tianjin Medical
based on radiological imaging. University Cancer Institute and Hospital (No. bc2018039)
In recent years, research has focused on the work- approved this study. All participants signed an informed
up of smaller solid lung nodules. The Fleischner Society consent form before participating in this study, and this
2017 guidelines for the management of incidentally study conformed to the provisions of the Declaration of
detected pulmonary nodules (4), advises that a solid nodule Helsinki (as revised in 2013).
larger than 8 mm with suspicious morphology or upper
lobe location should be considered for CT at 3 months,
positron emission tomography/computed tomography Patients
(PET/CT), or tissue sampling. However, the challenge A total of 1,789 consecutive patients from Tianjin Medical
that radiologists often face is to give a definitive diagnosis University Cancer Institute and Hospital who underwent
of a certain nodule to be malignant or benign, especially surgical resection of a lung tumor with postoperative
in cancer centers where patients usually present with histopathological confirmation from January 2011 to
larger nodules or masses. Tissue biopsy is limited by October 2017 were considered. The inclusion criteria were:
difficulty to access locations and size of the tumor, and has (I) solitary solid lung tumor on CT (diameter ≥8 mm);
potential complications such as pulmonary hemorrhage, (II) preoperative thin-section non-contrast and contrast-
pneumothorax, and risks associated with general anesthesia enhanced CT images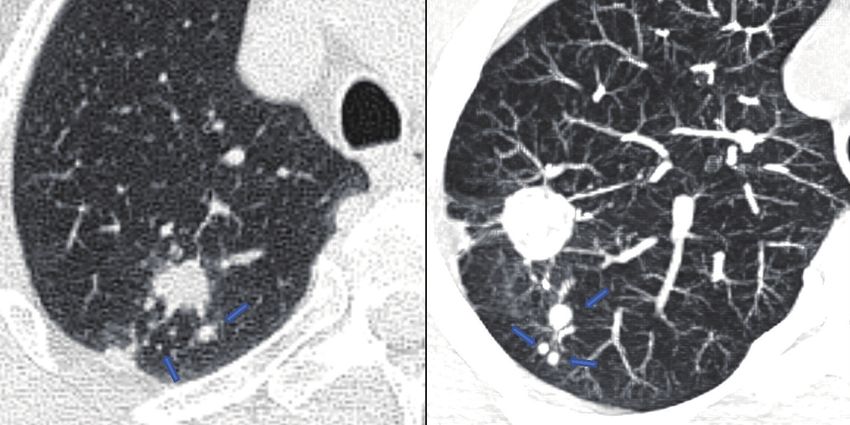
Journal of Thoracic Disease, Vol 13, No 7 July 2021 4409 Computed tomography examination Decision analysis for the radiologist’s diagnosis CT examinations, consisting of an acquisition without We used the clinical CT report to assess the diagnostic and with iodine contrast, were performed on Somatom performance of radiologist evaluation. All CT diagnostic Sensation 64 (Siemens Medical Solutions, Forchheim, reports were double read by two radiologists at the time Germany) CT scanner, Lightspeed 16 (GE Medical of CT acquisition and assigned to one of five categories: Systems, Milwaukee, WI), or Discovery CT 750 HD (GE (I) benign; (II) probably benign; (III) undetermined; (IV) Medical Systems). The scan tube voltage was 120 kVp with probably malignant; (V) high suspicion of malignancy. automatic tube current modulation. The iodine contrast These categories represent the radiologist classification agent Visipaque (Iodixanol, 270 mg/mL) was administered of malignancy probability of the evaluated nodule in intravenously through the upper extremity (1.5 mL/kg, real clinical setting. In total, 27 radiologists in the injection rate: 2.5 mL/s). The scan range included the radiology department were involved in CT reporting. In pulmonary apex level to below the diaphragm, and scanning this study, we classified into three management groups was performed 70 seconds after injection of the contrast defined the radiologist diagnosis risk thresholds based agent. For the Siemens CT system pitch was 0.95, acquired on the malignancy probability of the five categories and reconstructed slice thickness of 1.5 mm, B70f and (observe =1, indeterminate =2 or 3 or 4, surgery =5). The B30 reconstruction kernels were used. Pitch for the GE “Observe” group was recommended for CT follow-up, the CT systems was 0.984, acquired and reconstructed slice “indeterminate” group was recommended for further work- thickness of 1.25 mm, and Stnd and Lung reconstruction up (short interval CT follow-up, PET-CT or biopsy), and kernels were used. the “surgery” group was recommended for surgery. Evaluation of contrast-enhanced CT characteristics Statistical analysis All contrast-enhanced CT scans were reviewed by two We randomly divided the tumors (n=827) into a training experienced radiologists (6-year and 9 year reading group (n=575) and testing group (n=252). Student’s t-test, experience in chest CT) blindly and independently by using chi-square test, and Kolmogorov-Smirnov test were used the RadiAnt DICOM Viewer (version 2020.2). The two to assess each indicator in the training and testing group. radiologists determined the final radiological characteristics Finally, a classification and regression tree (CART) method after a mutual consultation. The radiologists evaluated was constructed to assess variables that might discriminate the pulmonary solid tumor on pulmonary window setting between benign and malignant tumors (P value
4410 Cui et al. A contrast-enhanced CT based classification tree model for classifying solid lung tumors
Table 1 Characteristics of patients in the study
Characteristics Total (n=827) Training (n=575) Testing (n=252) P
Age, mean (SD) years 57.5±9.4 57.7±9.3 57.0±9.5 0.271a
Sex, n (%)
Man 466 (56.3) 328 (57.0) 138 (54.8) 0.543b
Woman 361 (43.7) 247 (43.0) 114 (45.2)
Histologic type, n (%) 0.338b
Malignant 487 (58.9) 352 (61.2) 135 (53.6)
Adenocarcinoma 319 (65.5) 226 (64.2) 93 (68.9)
Squamous cell carcinoma 118 (24.2) 87 (24.7) 31 (23.0)
Large cell 50 (10.3) 39 (11.1) 11 (8.1)
Benign 340 (41.1) 223 (38.8) 117 (46.4)
Inflammatory pseudotumor 80 (23.5) 55 (24.7) 25 (21.4)
Hamartoma 156 (45.9) 101 (45.3) 55 (47.0)
Sclerosing pneumocytoma 54 (15.9) 37 (16.6) 17 (14.5)
Tuberculosis 50 (14.7) 30 (13.5) 20 (17.1)
a b
, Student’s t-test (Normally distributed) and Kolmogorov-Smirnov test (non-normally distributed); , Pearson’s chi-square test and Fisher’s
exact test. HU, Hounsfield units.
as ‘observe’ group, ST2 suggested for further work-up statistically significant differences between the training and
(see above), and ST3 advised for surgery, similar to the testing group in patient and nodule characteristics.
radiologist’s decision (Appendix 2). Finally, we used the
testing group to validate the discriminatory performance of
Development of the CART model for predicting malignant
the CART model. P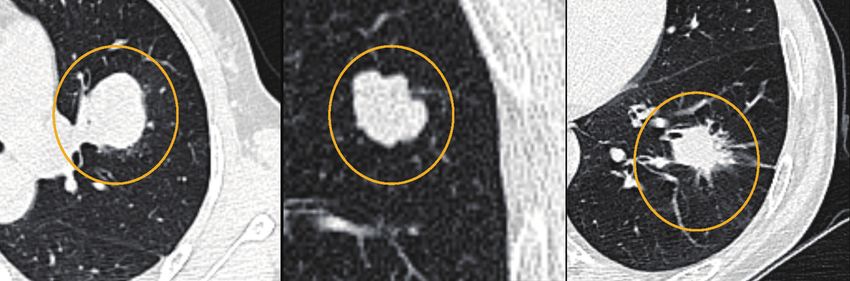
Journal of Thoracic Disease, Vol 13, No 7 July 2021 4411
Table 2 Characteristics of benign vs. malignant tumors in the training group
Characteristics Subgroup Malignant (n=352) Benign (n=223) P
Patient age, mean± SD, years 60.2±8.7 53.9±8.9 0.000a
Sex, n (%) Man 227 (64.5) 101 (45.3) 0.000b
Woman 125 (35.5) 122 (54.7)
Morphological
Location, n (%) Left upper lobe 103 (29.3) 59 (26.5) 0.627b
Left lower lobe 67 (19.0) 44 (19.7)
Right upper lobe 91 (25.9) 52 (23.3)
Right middle lobe 27 (7.7) 16 (7.2)
Right lower lobe 64 (18.2) 52 (23.3)
Nodule type, n (%) Peripheral 268 (76.1) 198 (88.8) 0.000b
Central 84 (23.9) 25 (11.2)
Shape, n (%) Round/oval 180 (51.1) 154 (69.1) 0.000b
Irregular 172 (48.9) 69 (30.9)
Margin, n (%) Smooth 21 (6.0) 95 (42.6) 0.000b
Lobulated 182 (51.7) 71 (3.18)
Spiculated 149 (42.3) 57 (25.6)
Calcification, n (%) No 311 (88.4) 176 (78.9) 0.002b
Yes 41 (11.6) 47 (21.1)
Fat, n (%) No 351 (99.7) 189 (84.8) 0.000b
Yes 1 (0.3) 34 (15.2)
Necrosis, n (%) No 288 (81.8) 195 (87.4) 0.073b
Yes 64 (18.2) 28 (12.6)
Cavitation, n (%) No 278 (79.0) 201 (90.1) 0.000b
Yes 74 (21.0) 22 (9.8)
Air Bronchograms, n (%) No 247 (70.2) 214 (96.0) 0.000b
Yes 105 (29.8) 9 (4.0)
Pleural indentation, n (%) No 80 (22.7) 123 (55.2) 0.000b
Yes 272 (77.3) 100 (44.8)
Vascular invasion, n (%) No 247 (70.2) 222 (99.6) 0.000b
Yes 105 (29.8) 1 (0.4)
Postobstructive pneumonia, n (%) No 215 (61.1) 165 (74.0) 0.001b
Yes 137 (38.9) 58 (26.0)
Satellite nodules, n (%) No 347 (98.6) 206 (92.4) 0.000b
Yes 5 (1.4) 17 (7.6)
Table 2 (continued)
© Journal of Thoracic Disease. All rights reserved. J Thorac Dis 2021;13(7):4407-4417 | https://dx.doi.org/10.21037/jtd-21-588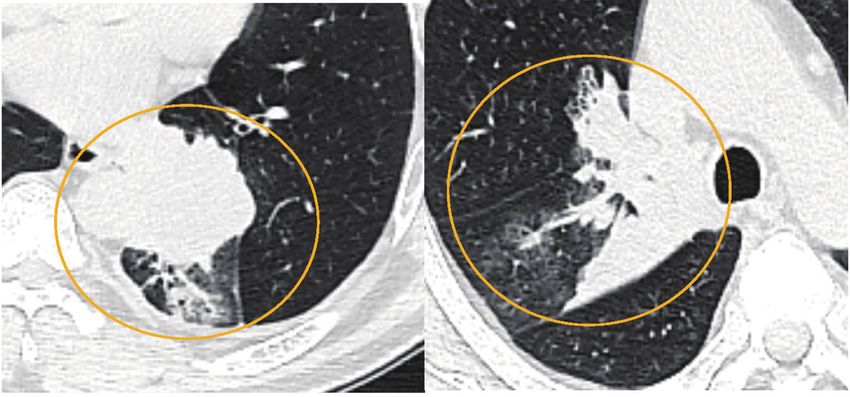
4412 Cui et al. A contrast-enhanced CT based classification tree model for classifying solid lung tumors
Table 2 (continued)
Characteristics Subgroup Malignant (n=352) Benign (n=223) P
Pleural effusion, n (%) No 340 (96.6) 220 (98.7) 0.130b
Yes 12 (3.4) 3 (1.3)
Lymph nodes, n (%) No 248 (70.5) 218 (97.8) 0.000b
Yes 104 (29.5) 5 (2.2)
Subjective enhancement, n (%) No 6 (1.7) 89 (39.9) 0.000b
Uniform 3 (0.9) 38 (17.0)
Heterogeneous 343 (97.4) 96 (43.0)
CT attenuation (HU), mean± SD Plain CT 28.6±11.4 23.0±27.0 0.001a
Enhanced CT 63.1±19.9 50.8±40.2 0.000a
Difference in HU 34.5±17.7 27.9±27.4 0.001a
Size, median (IQR), mm Diameter 32.0 (23.0–42.8) 17.6 (13.5–28.4) 0.000a
Radiologist’s diagnosis, n (%) Observe 12 (3.4) 117 (52.5)
Indeterminate 24 (6.8) 52 (23.3)
Surgery 316 (89.8) 54 (24.2)
a b
, Student’s t-test (Normally distributed) and Kolmogorov-Smirnov test (non-normally distributed); , Pearson’s chi-square test and Fisher’s
exact test. HU, Hounsfield units.
Validation of the CART models and radiologist’s diagnosis 27.0 mm, IQR 18.0–39.0 mm) in case only CT is available
in the testing group as a diagnostic tool.
Radiological characteristics (nodule type, size, shape,
Both the radiologists and the CART model used three
margin and location) and clinical information (age, gender,
thresholds to determine the solid tumor malignancy risk.
cancer history, smoking history) have been used to develop
The classification performance of the CART models and
classification models (such as the models developed by
radiologist’s diagnosis were evaluated using the testing
group. The sensitivity specificity, PPV, NPV, and diagnostic Mayo Clinic, Brock University and Veterans Affairs)
accuracy to differentiate malignant from benign tumors to predict the probability of malignancy of pulmonary
were 98.5%, 58.1%, 80.6%, 98.6, and 79.8% for CART tumors (17-19). However, several previous studies showed
model and 90.4%, 54.7%, 82.4% 98.5% and 74.2% for that the performance of these models, especially in large
radiologist’s diagnosis, respectively (Table 3). tumors, is moderate (20-23). Our previous study (24),
comparing classification models (Veterans Affairs, Mayo,
and Brock model) to the diagnosis of the radiologist for
Discussion differentiation of lung nodules (median size: 17.0 mm, IQR
Three radiological CT characteristics of solid lung lesions 13.0–21.0 mm) into benign and malignant in a Chinese
were shown to have discriminatory ability for malignant population, showed a lower discriminatory power for the
and benign lung tumors. These characteristics were: three models compared with the radiologist’s diagnosis. In
subjective enhancement, margin and shape. The CART that study, less than 15.5% out of 207 malignancies were
model for solid tumors in our clinical population resulted classified at and above the surgical threshold using the
in a higher diagnostic accuracy compared to radiologist’s three classification models, while the remaining malignant
diagnosis. Our results suggest that our contrast-enhanced nodules were considered indeterminate (VA model 44.9%,
CT based CART model can support radiologists in making Mayo model 85.5%; Brock model 93.7%). The radiologist’s
a diagnosis decision of solid lung tumors (median diameter diagnosis showed higher performance contrast to the three
© Journal of Thoracic Disease. All rights reserved. J Thorac Dis 2021;13(7):4407-4417 | https://dx.doi.org/10.21037/jtd-21-588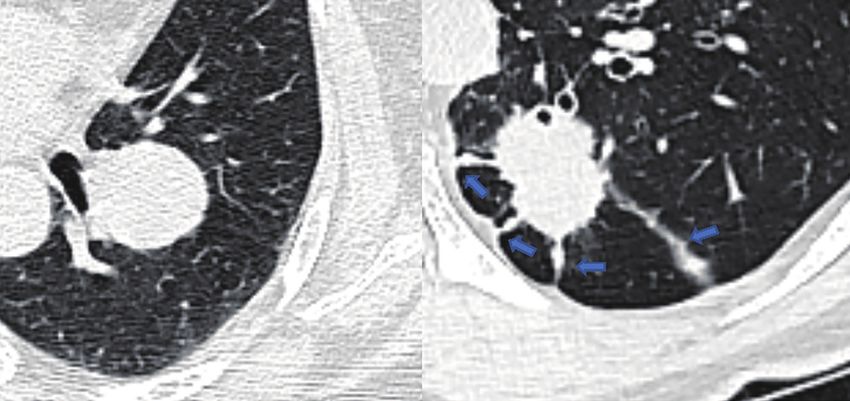
Journal of Thoracic Disease, Vol 13, No 7 July 2021 4413
1=M 0=B
Node 0
Category % n
0.000 38.8 223
1.000 61.2 352
Total 100.0 575
0.000
1.000
−
0=No enhancement 1=Uniform
enhancement 2=Heterogeneous
enhancement
lmprovement=0.185
2 1; 0
Node 1 Node 2
Category % n Category % n
0.000 21.9 96 0.000 93.4 127
1.000 78.1 343 1.000 6.6 9
Total 76.3 439 Total 23.7 136
−
0=smooth; 1=Lobulate; 2=Spiculatc
lmprovement=0.025
0 1; 2
Node 3 Node 4
Category % n Category % n
0.000 60.0 27 0.000 17.5 69
1.000 40.0 18 1.000 82.5 325
Total 7.8 45 Total 68.5 394
− +
o=roundioval 1 irregular
lmprovement=0.014
0 1
Node 5 Node 6
Category % n Category % n
0.000 75.0 27 0.000 0.0 0
1.000 25.0 9 1.000 100.0 9
Total 6.3 36 Total 1.6 9
Figure 1 CART model for the classifying the malignancy of pulmonary solid tumor in the training group. CART, classification and
regression tree.
© Journal of Thoracic Disease. All rights reserved. J Thorac Dis 2021;13(7):4407-4417 | https://dx.doi.org/10.21037/jtd-21-588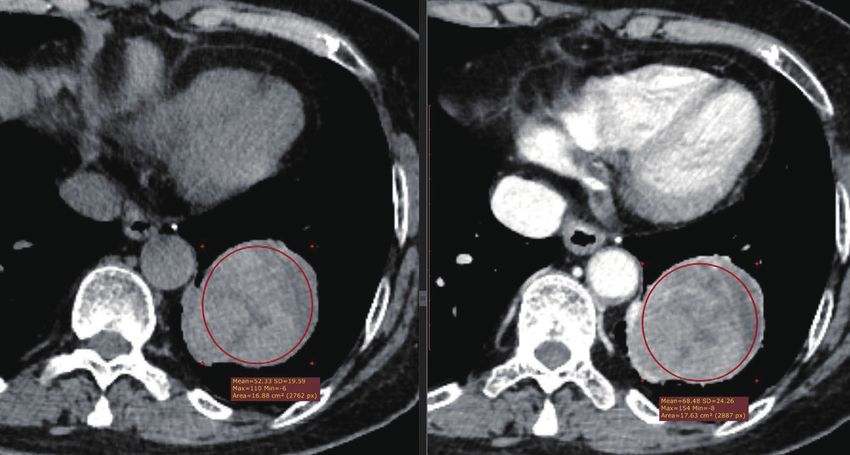
4414 Cui et al. A contrast-enhanced CT based classification tree model for classifying solid lung tumors
Heterogeneous enhancement
None/Uniform enhancement
Shape Smooth Lobulate/Spiculate
Round/oval ST1 ST1 ST2 ST3
Irregular ST1 ST1 ST3 ST3
Figure 2 The optimized classification diagram of CART model (ST1 = IF Malignant% ≤ 20%; ST2 = IF 20% < Malignant% < 80%; ST3 =
IF Malignant% ≥ 80). CART, classification and regression tree.
Table 3 Decision analysis using the three thresholds in the testing group
Risk threshold for Pathological results (No. %) Predictive value
Method Prediction
malignancy Benign (n=117) Malignant (n=135) (NPV/PPV)
Radiologist’s diagnosis Observe 1 64 (54.7) T.N 1 (0.7) F.N 98.5%
Indeterminate 2–4 27 (23.1) 12 (8.9) –
Surgery 5 26 (22.2) F.P 122 (90.4) T.P 82.4%
CART model ST1 ≤20% 68 (58.1) T.N 1 (0.7) F.N 98.6%
ST2 20–80% 17 (14.5) 1 (0.7) –
ST3 ≥80% 32 (27.4) F.P 133 (98.5) T.P 80.6%
P, true positive; T.N, true negative; F.P, false-positive; F.N, false-negative; NPV, negative predictive value; PPV, positive predictive value; 1,
benign; 2, probably benign; 3, undetermined; 4, probably malignant; 5, high suspicion of malignancy. ST1= IF Malignant% ≤20%; ST2= IF
20%< Malignant%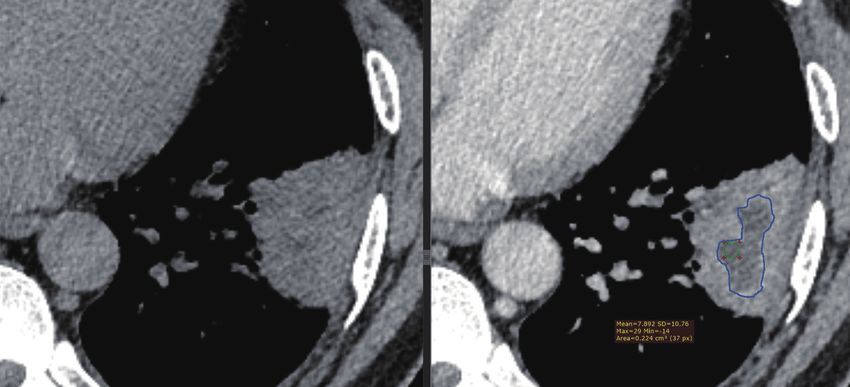
Journal of Thoracic Disease, Vol 13, No 7 July 2021 4415
50–60% by using 15HU as enhancement cut-off (13). 2018YFC1315600 and No. 2016YFE0103000), the Royal
In a study by Yi et al. (26) the sensitivity for malignant Netherlands Academy of Arts and Sciences (grant number.
nodules was 99% with specificity of 57% by using 30 HU PSA_SA_BD_01), and the University Medical Center
as the enhancement cut-off value. The authors concluded Groningen PhD Scholarship program.
that contrast-enhanced CT is highly sensitive to detect
malignant tumors but has low specificity. The latter might
Footnote
be explained by the fact that some benign nodules, such as
sclerosing hemangioma (27), can enhance as well. These Reporting Checklist: The authors have completed the
findings are similar to our study’s training group, 93.7% TRIPOD reporting checklist. Available at https://dx.doi.
(89/95) of the lesions with no enhancement (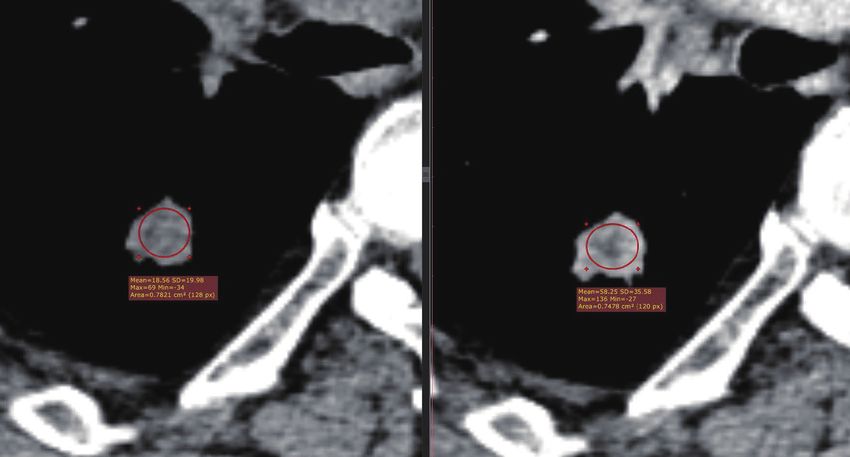
4416 Cui et al. A contrast-enhanced CT based classification tree model for classifying solid lung tumors
DR, Adams AM, et al. Reduced lung-cancer mortality with Acute Pancreatitis Using a Decision Tree Model Based on
low-dose computed tomographic screening. N Engl J Med the Revised Atlanta Classification of Acute Pancreatitis.
2011;365:395-409. PLoS One 2015;10:e0143486.
3. Zhou Q, Fan Y, Wang Y, et al. China National Guideline 15. Kim YH, Kim MJ, Shin HJ, et al. MRI-based decision
of Classification, Diagnosis and Treatment for Lung tree model for diagnosis of biliary atresia. Eur Radiol
Nodules (2016 Version). Zhongguo Fei Ai Za Zhi 2018;28:3422-31.
2016;19:793-8. 16. Cui X, Heuvelmans MA, Fan S, et al. A Subsolid Nodules
4. MacMahon H, Naidich DP, Goo JM, et al. Guidelines for Imaging Reporting System (SSN-IRS) for Classifying
Management of Incidental Pulmonary Nodules Detected 3 Subtypes of Pulmonary Adenocarcinoma. Clin Lung
on CT Images: From the Fleischner Society 2017. Cancer 2020;21:314-325.e4.
Radiology 2017;284:228-43. 17. Swensen SJ, Silverstein MD, Ilstrup DM, et al. The
5. Lung CT Screening Reporting & Data System (Lung- probability of malignancy in solitary pulmonary nodules.
RADS). Available online: https://www.acr.org/Clinical- Application to small radiologically indeterminate nodules.
Resources/Reporting-and-Data-Systems/Lung-Rads Arch Intern Med 1997;157:849-55.
6. Callister ME, Baldwin DR, Akram AR, et al. British 18. McWilliams A, Tammemagi MC, Mayo JR, et al.
Thoracic Society guidelines for the investigation and Probability of cancer in pulmonary nodules detected on
management of pulmonary nodules. Thorax 2015;70 Suppl first screening CT. N Engl J Med 2013;369:910-9.
2:ii1-ii54. 19. Gould MK, Ananth L, Barnett PG, et al. A clinical
7. Travis WD, Brambilla E, Noguchi M, et al. International model to estimate the pretest probability of lung cancer
association for the study of lung cancer/american thoracic in patients with solitary pulmonary nodules. Chest
society/european respiratory society international 2007;131:383-8.
multidisciplinary classification of lung adenocarcinoma. J 20. Isbell JM, Deppen S, Putnam JB Jr, et al. Existing general
Thorac Oncol 2011;6:244-85. population models inaccurately predict lung cancer risk in
8. Travis WD, Brambilla E, Nicholson AG, et al. The patients referred for surgical evaluation. Ann Thorac Surg
2015 World Health Organization Classification of Lung 2011;91:227-33; discussion 233.
Tumors: Impact of Genetic, Clinical and Radiologic 21. Perandini S, Soardi GA, Motton M, et al. Limited
Advances Since the 2004 Classification. J Thorac Oncol value of logistic regression analysis in solid solitary
2015;10:1243-60. pulmonary nodules characterization: a single-center
9. Ozeki N, Iwano S, Taniguchi T, et al. Therapeutic surgery experience on 288 consecutive cases. J Surg Oncol
without a definitive diagnosis can be an option in selected 2014;110:883-7.
patients with suspected lung cancer. Interact Cardiovasc 22. Iaccarino JM, Simmons J, Gould MK, et al. Clinical
Thorac Surg 2014;19:830-7. Equipoise and Shared Decision-making in Pulmonary
10. Merritt RE, Shrager JB. Indications for surgery in patients Nodule Management. A Survey of American Thoracic
with localized pulmonary infection. Thorac Surg Clin Society Clinicians. Ann Am Thorac Soc 2017;14:968-75.
2012;22:325-32. 23. Tanner NT, Porter A, Gould MK, et al. Physician
11. Cui X, Han D, Heuvelmans MA, et al. Clinical Assessment of Pretest Probability of Malignancy and
characteristics and work-up of small to intermediate-sized Adherence With Guidelines for Pulmonary Nodule
pulmonary nodules in a Chinese dedicated cancer hospital. Evaluation. Chest 2017;152:263-70.
Cancer Biol Med 2020;17:199-207. 24. Cui X, Heuvelmans MA, Han D, et al. Comparison of
12. Schillaci O, Travascio L, Bolacchi F, et al. Accuracy Veterans Affairs, Mayo, Brock classification models and
of early and delayed FDG PET-CT and of contrast- radiologist diagnosis for classifying the malignancy of
enhanced CT in the evaluation of lung nodules: pulmonary nodules in Chinese clinical population. Transl
a preliminary study on 30 patients. Radiol Med Lung Cancer Res 2019;8:605-13.
2009;114:890-906. 25. Choi Y, Gil BM, Chung MH, et al. Comparing
13. Swensen SJ, Viggiano RW, Midthun DE, et al. Lung attenuations of malignant and benign solitary
nodule enhancement at CT: multicenter study. Radiology pulmonary nodule using semi-automated region of
2000;214:73-80. interest selection on contrast-enhanced CT. J Thorac
14. Yang Z, Dong L, Zhang Y, et al. Prediction of Severe Dis 2019;11:2392-401.
© Journal of Thoracic Disease. All rights reserved. J Thorac Dis 2021;13(7):4407-4417 | https://dx.doi.org/10.21037/jtd-21-588Journal of Thoracic Disease, Vol 13, No 7 July 2021 4417
26. Yi CA, Lee KS, Kim EA, et al. Solitary pulmonary 2004;233:191-9.
nodules: dynamic enhanced multi-detector row CT 27. Doyle DJ, Khalili K, Guindi M, et al. Imaging features
study and comparison with vascular endothelial of sclerosed hemangioma. AJR Am J Roentgenol
growth factor and microvessel density. Radiology 2007;189:67-72.
Cite this article as: Cui X, Heuvelmans MA, Sidorenkov
G, Zhao Y, Fan S, Groen HJM, Dorrius MD, Oudkerk M,
de Bock GH, Vliegenthart R, Ye Z. A contrast-enhanced-CT-
based classification tree model for classifying malignancy of
solid lung tumors in a Chinese clinical population. J Thorac Dis
2021;13(7):4407-4417. doi: 10.21037/jtd-21-588
© Journal of Thoracic Disease. All rights reserved. J Thorac Dis 2021;13(7):4407-4417 | https://dx.doi.org/10.21037/jtd-21-588Supplementary
Appendix 1 Evaluation of the CT characteristics
A B
Figure S1 Distance to costal pleura (peripheral/non-peripheral). (A) Peripheral nodules: The distance to costal pleural was
1/3 from total distance
hilum-costal pleura.
A B
Figure S2 Shapes (round/oval, irregular). (A) Round/Oval; (B) irregular.
A B C
Figure S3 Margins (smooth, lobulated, spiculated). (A) Smooth; (B) lobulated; (C) spiculated.
A B
Figure S4 Pleural indentation. (A) There is no pleural indentation; (B) nodules adhering to pleura or pleural indentation with
>1 stripe (blue arrows).
© Journal of Thoracic Disease. All rights reserved. https://dx.doi.org/10.21037/jtd-21-588A B
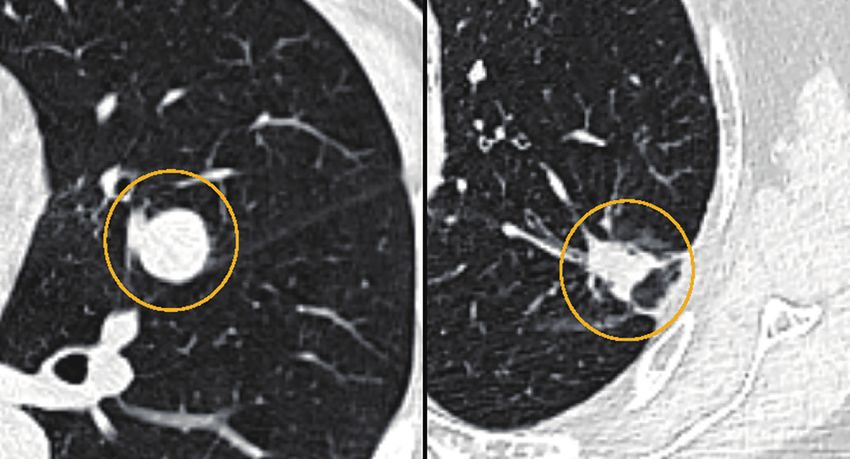
Figure S5 Vascular invasion. (A) There is no vascular invasion; (B) coexistence of irregular vascular dilation or vascular
convergence from multiple supplying vessels (blue arrow).
A B
Figure S6 Necrosis. Non-enhanced liquid area after enhancement (blue area).
A B
Figure S7 Satellite nodules. Satellite nodules appear around the tumor (blue arrow).
A B
Figure S8 Postobstructive pneumonia. Ground glass infiltration and atelectasis around tumor.
© Journal of Thoracic Disease. All rights reserved. https://dx.doi.org/10.21037/jtd-21-588A
B
C
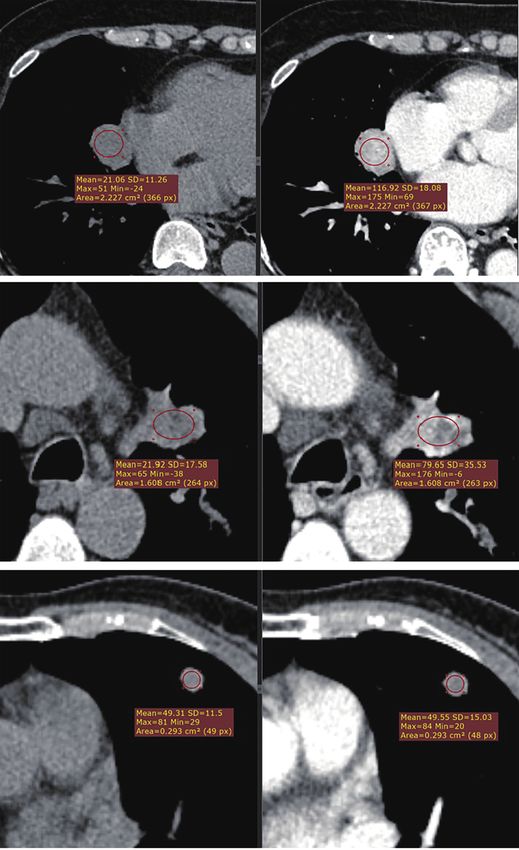
Figure S9 Subjective enhancement (uniform/heterogeneous/no). (A) The tumor enhanced difference is large than 15 HU with
uniform enhancement; (B) the tumor enhanced difference is large than 15 HU with heterogeneous enhancement; (C) the
tumor enhanced difference is less than 15 HU.
© Journal of Thoracic Disease. All rights reserved. https://dx.doi.org/10.21037/jtd-21-588Appendix 2 Case examples Figure S10 A 42 years old male patient with a solid oval, slightly lobulated tumor (15×14 mm2) located in the left upper lobe. The mean density of the nodule was 38.8 Hounsfield Units on 5 CT without iodine contrast, and 39.1 Hounsfield Units after contrast (no enhancement). Radiologist’s diagnosis: Benign; CART model classification: ST1; Histology: hamartoma. Figure S11 A 53 years old female patient with a solid round, smooth tumor (22×21 mm2) located in the left lower lobe. The mean density of the nodule was 33.9 Hounsfield Units on CT without iodine contrast, and 94.1 Hounsfield Units after contrast (uniform-enhancement). Radiologist’s diagnosis: Benign; CART model classification: ST1; Histology: sclerosing pneumocytoma. Figure S12 A 60 years old male patient with a solid irregular, lobulated tumor (23×19 mm2) located in the right lower lobe. The mean density of the nodule 12 was 18.6 Hounsfield Units on CT without iodine contrast, and a density of 58.3 Hounsfield Units after contrast (uneven-enhancement). Radiologist’s diagnosis: malignant; CART model classification: ST3; Histology: squamous cell carcinoma. © Journal of Thoracic Disease. All rights reserved. https://dx.doi.org/10.21037/jtd-21-588
Figure S13 A 78 years old female patient with a solid round, smooth tumor (60×51 mm2) located in the left lower lobe. The mean density of the nodule 16 was 52.3 Hounsfield Units on CT without iodine contrast, with uneven-enhancement 68.5 Hounsfield Units after contrast. Radiologist’s diagnosis: probably benign; CART model classification: ST2; Histology: sclerosing. Figure S14 A 56 years old female patient with a solid round, smooth tumor (18×16 mm2) located in the right lower lobe. The mean density of the nodule 20 was 15.1 Hounsfield Units on CT without iodine contrast, and uneven-enhancement 61.7 Hounsfield Units after contrast. Radiologist’s diagnosis: Probably malignancy; CART model classification: ST2; Histology: adenocarcinoma. © Journal of Thoracic Disease. All rights reserved. https://dx.doi.org/10.21037/jtd-21-588
You can also read

















































