AGENTS TO REDUCE LDL (AND FUTURE DEVELOPMENTS) - RAUL D. SANTOS MD, PHD HEART INSTITUTE-INCOR UNIVERSITY OF SAO PAULO BRAZIL
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Agents to reduce LDL
(and future developments)
Raul D. Santos MD, PhD
Heart Institute-InCor
University of Sao Paulo
Brazil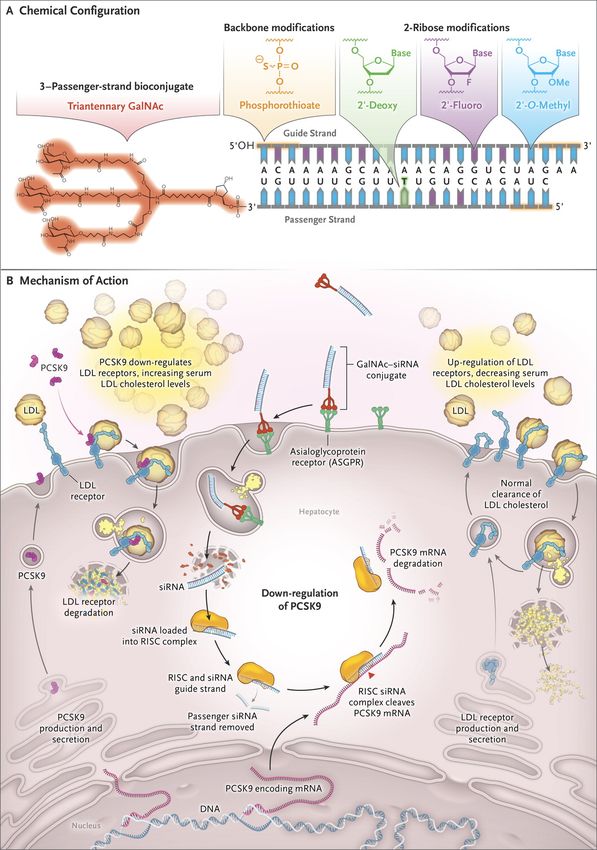
Disclosure
• Honoraria for consulting and speaker activities on the
last year from
– Amgen, Astra Zeneca, Akcea
– Biolab, Merck, Novo-Nordisk
– Pfizer,Kowa
– Sanofi/Regeneron
3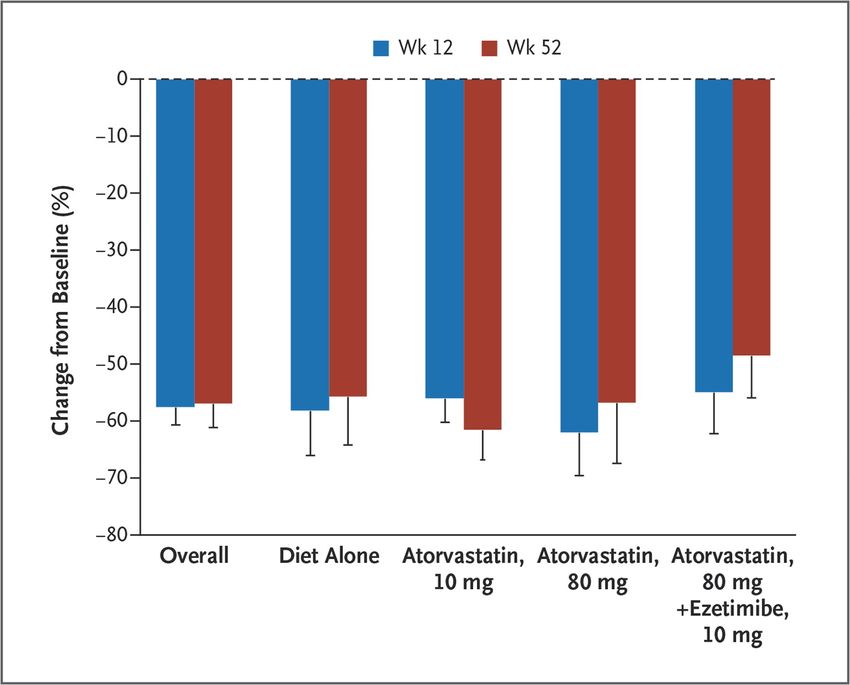
Agents do reduce LDL-C
• Current options
– Statins
– Ezetimibe
– PCSK9 inhibitors
– Niacin/Resins
– Lomitapide
– Mipomersen
• Future options?
– ATP CL Inhibition
4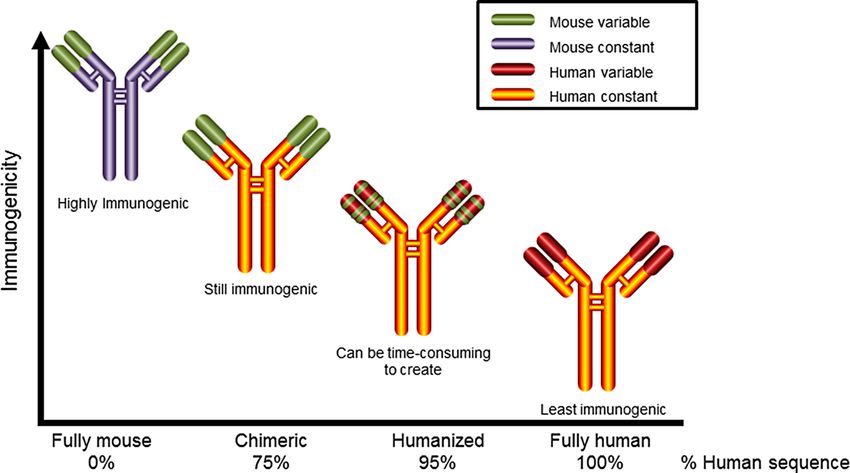
Statins
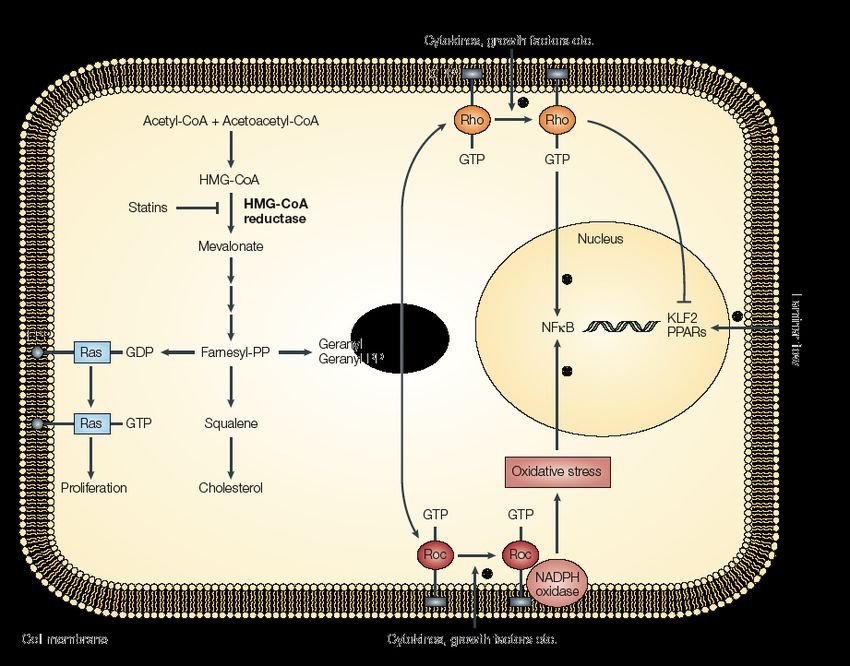
Statins: Mechanism of Action
HMG-CoA reductase
Statins inhibit HMG-CoA reductase
Intrahepatic cholesteorl pool reduction
Increment on LDL receptor expression Reduction of VLDL production
Incrementof LDL catabolsim Less VLDL particles available to become LDL
Reduction of : LDL-C, TC, non-HDL-C and TG
STELLAR LDL-C
(% Changes vs. Baseline)
RSV ATV SIN PRA
10 20 40 10 20 40 80 10 20 40 80 10 20 40
0
-10
-20
-20
-24
-30 -28
-30
% -35
-40 -37
-39
-43
-50 -46 -46
* -48
-52 -51
-60 ** -55
***
*P
Pravastatin Increases the Removal
From Plasma of Chylomicron Remnants
in CHD patients
P = 0.01
D%
Santos RD et al. Am J Cardiol 2000; 85:1163-6Impact of 1mmol/L reduction on LDL-C upon major
cardiovascular events and mortality
CTT 2010
Relative Risk (95% CI)
All cause mortality 0.90 (0.87-0.93), pNon-Lipid Lowering Effects of Statins
Jain MK, Ridker PM. Nature Rev Drug Discov, 2005in the rate of major vascular events (coronary deaths,
Proportional reductio
myocardial infarctions, strokes, and coronary
Statins: Benefits and Risks
revascularisations) during each year (after the first) that it 10
continues to be taken. Consequently, lowering LDL
ecause the cholesterol by 2 mmol/L reduces risk by about 45%.
surveillance Panel 4: Known adverse effects of statin therapy
• Lowering LDL cholesterol by 2 mmol/L with an effective
with other • The statin regimen
only adverse forevents
about 5that
yearshave
in 10 been
000 patients
reliablywould
shown to 0
simvastatin typically prevent major vascular events in about
be caused by statin therapy are myopathy (defined as 0
gher rate (at 1000 (10%) patients at high risk of heart attacks and M
muscle pain or weakness combined with large increases in
strokes (eg, secondary prevention) and 500 (5%) patients
ated yearly) creatine kinase blood concentrations) and new-onset
at lower risk (eg, primary prevention). Figure 3: Proportional ma
2
about one diabetes mellitus, along with a probable increase in cholesterol reductions in
imen is no • Despite reports based largely on non-randomised
strokes due to bleeding (ie, haemorrhagic strokes).
observational studies, there is not good evidence that statin
no routine statin use and
f reports of Adapted from CTT Collabor
• Typically, treatment of 10 000 patients for 5 years
therapy produces beneficial effects on other health outcomes with a against the average LDL cho
higher with standard statin
(eg, cancer, regimen
infections, (suchdisease,
respiratory as atorvastatin 40. mg
arrhythmias) routine statin therapy versu
pontaneous daily) would be expected to cause about 5 cases of cholesterol reduction great
versus less intensive statin t
sks are still myopathy, 50–100 new cases of diabetes, and cholesterol. The vertical axis
The rate of were adverse eff ects on non-vascular causes of death and because they represent redu
5–10 haemorrhagic strokes.
n statins are site-specific cancers. Consequently, data were sought for –log[0·9], –log[0·8], and –lo
79
• Despite
each reportstrials
of the eligible basedabout
largely
theon non-randomised
baseline characteristics average effects on risk obse
affect their Collins observational
of Reach
et al. Lancetand
patient studies,
2016; there is good
388:2532-2561
about myocardial evidence that
infarctions, statin treatment (when the risk re
strokes,
11Ezetimibe
NPC1L1 Transports Intestinal Cholesterol and
Phytosterols: Inhibition of NPC1L1 by Ezetimibe for
Hypercholesterolemia and Sitosterolemia
Cholesterol and
Plant Sterols
NPC1L1
SitosterolemiaEffects of ezetimibe, simvastatin and simvastatin/ezetimibe on
pro-atherogenic lipids and apoB
Farnier M et al. Atherosclerosis 2013; 229:415 - 422 14Ezetimibe + Statin Trials: SHARP
and IMPROVE-IT
IMPROVE-IT
SHARP
30%
Statins vs. control
Intensive (21 studies)
25%
of ischemic events (95% HF)
hypolipidemia
Relative risk reduction
treatment
20% SHARP
vs.
Conventional
(5 studies) 17%
15% risk
reduction
10% SHARP
32mg/dL
5%
0%
0 10 20 30 40
Baigent et al. Lancet 2011; 377;2181–2192.
Cannon CP et al. N Engl J Med 2015;372:2387-2397.
15Ezetimibe: Side Effects
• Gastro intestinal
16Antibodies against PCSK9
PCSK9 Promotes Degradation of LDLRs
LDLR
PCSK9 LDL-C
protein
PCSK9 X LDLR
protein
LDL-C
LDL-C=low-density lipoprotein cholesterol; LDLR=low-density lipoprotein receptor.
18Effects of Alirocumab on Lipoptoein Kinetics in Healthy Subjects Gissette Reyes-Soffer et al. Circulation. 2017;135:352-362
Monoclonal Antibodies: Immunogenicity
Potential
18 The Journal of Clinical Pharmacology / Vol 57 No 1 2017
Evolocumab
Alirocumab
Bococizumab
Figure 4. Evolution of therapeutic monoclonal antibodies. Fully mouse antibodies developed with early hybridoma technology were highly
immunogenic. Development of recombinant DNA technologies resulted in more humanized and less immunogenic antibodies: chimeric, humanized,
and fully human.45,46,48
20
Adaptedconvenience
from Ito MK &whoSantos
to patients, do not needRD J Clin
to receive the Pharmacol. 2017;57:7-32
hypercholesterolemia or HeFH was evaluated 58,65 67,68Percent Reduction from Baseline in Low-Density Lipoprotein (LDL) Cholesterol
Levels in the Evolocumab Group, as Compared with the Placebo Group, at
Weeks 12 and 52, According to Background Lipid-Lowering Therapy.
N=901
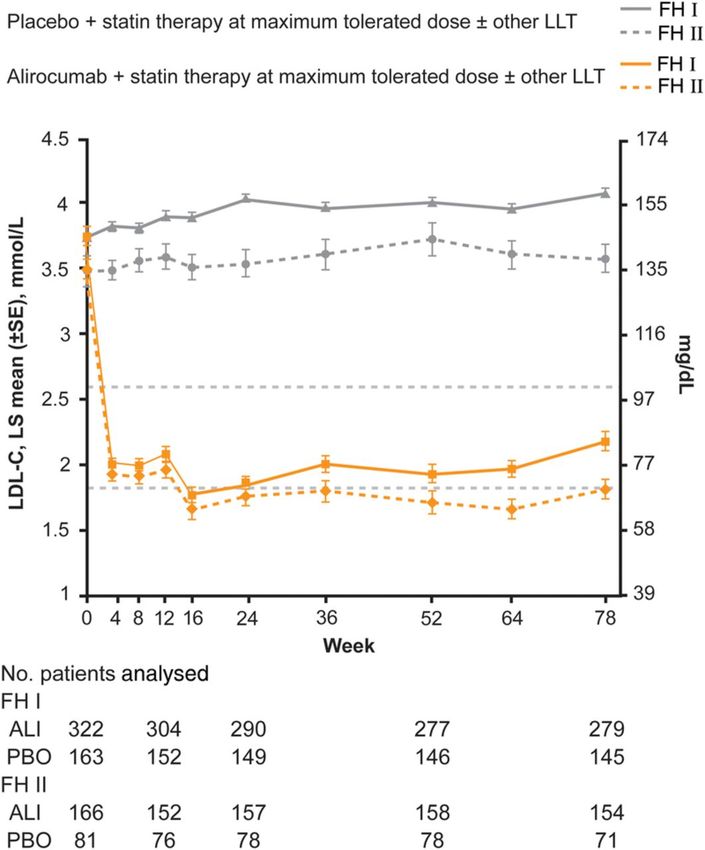
Blom DJ et al. N Engl J Med 2014;370:1809-1819.Alirocumab Reduces LDL-C in Familial
Hypercholesterolemia
John J.P. Kastelein et al. Eur Heart J. 2015;36:2996-3003After ≥12 weeks of 420 mg After 12 weeks of 420 mg mutations in the apheresis g
evolocumab every month evolocumab every 2 weeks apheresis group) and fewer
Long-term treatment
Value at baseline, mmol/L
with evolocumab
9·35 (3·35)
added
9·35 (3·35)
to LDLR mutations (12 [35%] v
conventional
Change from baseline, drug mmol/L therapy, with or without
–1·77 (2·05) apheresis,
–2·57 (2·14) reductions in LDL cholestero
Percentage change from baseline –20·1% (21·7) –28·3%(21·1) both at week 12 and 48, we
in patients with homozygous familial hypercholesterolaemia: significantly differ from th
Data are mean (SD). Data are for 47 patients who were not on apheresis who increased their dosing to every 2 weeks.
anp=0·0001
interim subset
for difference analysis
between groups ofbaseline.
in change from the open-label TAUSSIG study patients who were not on ap
testing; appendix). Four pati
Frederick
TableJ Raal, G Keesof
3: Effect Hovingh, Dirk Blom,
evolocumab Raul D Santos,
uptitration onMariko the frequency of the procedu
Harada-Shiba, Eric Bruckert, Patrick Couture, Handrean Soran, Gerald F Watts,
LDL cholesterol
Christopher Kurtz, Narimon Honarpour, Lihua Tang, Sree Kasichayanula, Scott M Wasserman, Evan A Stein
monthly or less often, and
Summary 60
discontinued apheresis. One
LDLR–/– (5%)
Background Homozygous familial hypercholesterolaemia is a genetic disorder characterised apheresis
by substantially raised forEndocrinol
Lancet Diabetes more2017 than 2 yea
LDL cholesterol, † reduced LDL receptor function, xanthomas, and cardiovascular disease *‡ before age 20 years. Published Online
40 *
Conventional therapy is with statins, ezetimibe, and apheresis. We aimed to assess the long-term safety and efficacy February 15, 2017
began apheresis: one who is
Change from baseline in LDL cholesterol (%)
PCSK9 withhttp://dx.doi.org/10.1016/
a heterozygous genoty
of the proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor evolocumab in a subset of patients with
20 ** GoF/LDLR S2213-8587(17)30044-X
homozygous familial hypercholesterolaemia enrolled in an open-label, non-randomised phase 3 trial.
negative remained above goal despite
See Online/Comment
LDLR unclassified (–25%) LDLR defective (–20%) *
Methods In *
(–65%) with evolocumab treatment.
http://dx.doi.org/10.1016/
0 this interim subset analysis of the TAUSSIG study, which was undertaken at 35 sites in 17 countries, we S2213-8587(17)30060-8
included patients aged ** 12 years or older with homozygous familial hypercholesterolaemia who
**
* were on stable LDL included in the no apheres
Carbohydrate and Lipid
* * * *
cholesterol-lowering
–20 therapy
** * for at least 4 weeks; all patients received
*
** *evolocumab
*
420 mg subcutaneously monthly, purposes. Research Unit,
Metabolism
or if on apheresis every 2 weeks. Dosing could be increased to every 2*weeks after 12 weeks in patients not on Faculty of Health Sciences,
* Reductions in apolipoprotei
University of Witwatersrand,
apheresis. The primary outcome *of *the TAUSSIG study was treatment-emergent * adverse events; secondary Johannesburg, South Africa
–40 * on LDL cholesterol and other lipids. We analysed patients onARH cholesterol, with greater redu
outcomes were the effects of evolocumab an intention- (Prof F J Raal MD); Department
* *
to-treat basis, and all statistical comparisons were done post hoc in this interim analysis. The TAUSSIG studyweek * (–15%) is of 12. We noted a small re
Vascular Medicine,
registered –60with ClinicalTrials.gov, number NCT01624142, * and is ongoing. * Academisch Medisch Centrum,
* * week 12,
Amsterdam, with some additiona
Netherlands
*
Findings–80 106 patients were included in this analysis, 34 receiving apheresis at study Apolipoprotein
entry andB 14 younger than (tableLipidology,
2; appendix).
(G K Hovingh PhD); Division of
Department of
These re
(–47%)
18 years. The first patient was enrolled on June 28, 2012, and the cutoff date for the analysis was Aug* 13, 2015; mean were not significant in patie
Medicine, University of Cape
Town, Cape Town, South Africa
follow-up–100was 1·7 years (SD 0·63). After 12 weeks, mean LDL cholesterol decreased from baseline by 20·6% either week 12 Heart
or 48 (po
(D Blom MD); Lipid Clinic
(SD 24·4; mean absolute decrease 1·50 mmol/L [SD 1·92]); these reductions were maintained at week 48. Institute (InCor), University of
47Figure
of 722: LDL
patients not onchange
cholesterol apheresis at studytoentry
from baseline week increased evolocumab
12, by underlying geneticdosing to every 2 weeks, with appendix).
abnormality an Sao Paulo Medical VerySchool
small red
additional mean reduction in LDL cholesterol of 8·3% (SD 13·0; mean absolute decrease
Mean change in LDL cholesterol is shown in parentheses after each genetic abnormality category. GoF=gain of 0·77 mmol/L [SD occurred
1·38]; Hospital andin patients
Preventive with L
Medicine Center and
p=0·0001). In a post-hoc analysis, mean reductions in LDL cholesterol in patients on
function. *Apheresis patient. †Patient missed apheresis before week 12 blood draw due to snowstorm. ‡Week 12apheresis were signifi cant at
bothCardiology
alleles, butHospital
median redu
Program,
week 12 (p=0·0012)
immediately and week
after vacation; 48indiscretion
dietary (p=0·0032), and didARH=autosomal
suspected. not differ from reductions
recessive achieved in patients not on Israelita Albert Einstein,
hypercholesterolaemia.
apheresis (p=0·38 at week 12 and p=0·09 at week 48). We noted a small reduction (median –7·7% [IQR –21·6 to 6·8]) –41) Sao
atPaulo,
week Brazil
12 and 67% (–6
in lipoprotein(a) at week 12 (p=0·0015), with some additional reduction at week 48 (–11·9% [–28·0 to 0·0]; seen(Prof
inRpatients
D Santos MD); with 23 PCSK9
Lancet Diabetes Endocrinol 2017 Published
pEvolocumab Reduces Lp(a) in Heterozygous
FH
% Change From Baseline
Raal F et al. Circulation 2012;126:2408-2417
24Clinical Impact
LDL Cholesterol
100 Placebo
90
80
LDL Cholesterol (mg/dl)
70 59% mean reduction (95%CI 58-60), P30
(0.3%), and development of neutralizing antibodies 0
Cu
20 0 6 12 18 24 30 36
did not occur in any patient.
10
FOURIER: Study Endpoints
0
Discussion 0 6 12 18 24 30 36
Months
When added to statin therapy, the PCSK9 inhibi-
with Cardiovascular Disease
tor evolocumab lowered LDL cholesterol levels No. at Risk
Placebo 13,780 13,278 12,825 11,871 7610 3690 686
by 59% from baseline levels as compared with Evolocumab 13,784 13,351 12,939 12,070 7771 3746 689
placebo, from a median of 92 mg per deciliter
d,
(2.4 mmol per liter) to 30 mg per deciliter (0.78 B Key Secondary Efficacy End Point
A Primary Efficacy End Point
up 100 mmol
16 per liter). This effect was sustained 14.6 with- 100 11 9.9
an Hazard ratio, 0.85 (95% CI, 0.79–0.92) Hazard ratio, 0.80 (95% CI, 0.73–0.88)
90 out
14 evidence of attenuation. In this dedicated 90 10
ed PCTTC Regression for the Risk of Major CV Events by Reduction of
LDL-C Considering Duration of Therapy in Statin and PCSK9i Trials
50%
≥4 years of treatment
Proportional reduction in major
40%
3 years of treatment
4S
vascular event (95% CI) HPS
30% 2 years of treatment
WOSCOPS
1 year of treatment
CARE
20% LIPID
SPIRE-2 (HR: 0.79, 95% CI: 0.65–0.97)
FOURIER (HR: 0.79, 95% CI: 0.74–0.84)
10%
IMPROVE-IT
0%
0.5 1.0 1.5 2.0
-10%
Reduction in LDL cholesterol (mmol/L)
Ference BA, et al; [published online ahead of print 2017]. European Heart Journal. doi:10.1093/eurheartj/ehx450.ODYSSEY OUTCOMES:
Study Design
Population Lipid criteria at entry Primary endpoint
••Patients 4-52 weeks post- ••LDL-C ≥70 mg/dL ••Composite of
ACS ••OR – CHD death
••Age ≥ 40 ••ApoB ≥80 mg/dL – Nonfatal MI
••Optimal statin treatment* ••OR – Ischemic stroke
••Non-HDL-C ≥100 mg/dL – UA requiring hospitalization
Run-in Period Double-Blind Treatment Period Post-treatment
(up to 16w) (~2-5 years) follow-up
Optimize statin; practice self- 2 weeks after end
injection with placebo; complete Alirocumab 75 mg Q2W until Month 2. of treatment
planned revascularization n=9,000 After Month 2, 75 mg or 150 mg Q2W,
adjusted based upon Month 1 LDL-C, in a
blinded fashion to achieve 15PCSK9 Inhibitors Adverse Events
• Cold like symptoms (not different from placebo)
• Neurocognitive changes not detected in Ebbinghaus
• Diabetes ? (genetic studies suggest)
30Other less used medications
Resins /Niacin
• Resins • Niacin
– Colesevelam and colestiramine – Reduce FFA input to liver
– Reduce cholesterol absorption – Increase Apo A-I synthesis
(bile acid binding) – Reduce Apo B synthesis
– Increase LDLR expression – Reduce LDL-25-30%
– Reduce LDL-C 20-25% – Reduce TG 20-30%
– Colestiramine (reduced MI) – Increase HDL-C 20-30%
– Colesevelam (reduces glucose) – Isolated use reduce MI
– Side effects: – Side effects
• GI • Flushing
• Reduce drug absorption • Gout
• Increase glucose
32Drugs for Homozygous FH
33LDL Receptor and Effect of Lipid Lowering Therapies
Sridevi 01/25/18 4 Color Fig: F1 17:42 Art: ATV310675
2 Arterioscler Thromb Vasc Biol March 2018
Figure. Mechanisms involved with low-density lipoprotein cholesterol (LDL-C) lowering by medications approved for homozygous familial
hypercholesterolemia and their possible associations with LDLR (LDL receptor) expression/function. apoB indicates apolipoprotein B; AQ10
HMGCR, 3-hydroxy-3-methylglutaryl-coenzyme reductase; IDOL, inducible degrader of LDL receptor; MTP, microsomal triglyceride trans-
Santos RD. ATVB 2018 in press
fer protein; PCSK9, proprotein convertase subtilisin kexin type 9; SREBP2, steroid regulatory element binding protein-2; and VLDL, very- 34
AQ11 low-density lipoprotein.Drugs Approved for Homozygous FH
• Lomitapide • Mipomersen
– Inhibits MTP – ASO inhibits Apo B synthesis
– Reduces VLDL and LDL – Reduces VLDL, LDL and Lp(a)
production production
– Reduces LDL-C by 40-50% on – Reduces LDL-C 25-30% on top
top of statins of statins
– Side effects – Reduces Lp(a) 25-30%
• Steatosis – Side effects
• Steatorrhea • Injection site reactions
• CYP3A4 interaction • Flu-like symptoms
• Steatosis
Cuchel M et al. Lancet 2013; 381:40-46
Raal FJ, Santos RD et al. Lancet. 2010;375:998-1006
Santos RD et al. ATVB. 2015;35:689-99 35Future Treatments?
36ATP Citrate Lyase Inhibition
Bempedoic Acid
37Use of Bempedoic acid to treat
hypercholesterolemia in patients with
statin intolerance
Thompson P et al. Journal of Clinical Lipidology, 9(3):295-304Inclisiran Chemical Configuration and Mechanism of
Action.
RNA inhibition
Reduce cholesterol
With 2-3 injections a year?
Khvorova A. N Engl J Med 2017;376:4-7.Conclusions
• LDL-C is an independent risk factor for atherosclerosis
• There are many proven therapies that reduce LDL-C and
prevent CVD
• Statins are the cornerstone of LDL-C lowering
• Other drugs should be added to control LDL-C
adequately (ezetimibe, PCSK9 inhibitors)
– Cost effectiveness
• Newer medications?
40You can also read