Anaphylaxis after ingestion of dust mite (Dermato-phagoides farinae)-contaminated food: A case report - Malaysian Society of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Tropical Biomedicine 37(2): 318–323 (2020)
Anaphylaxis after ingestion of dust mite (Dermato-
phagoides farinae)-contaminated food: A case report
Rangkakulnuwat, P.1, Sanit, S.2 and Lao-Araya, M.1*
1Department of Pediatrics, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
2Department of Parasitology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
*Corresponding author e-mail: laoaraya@gmail.com
Received 7 August 2019; received in revised form 25 February 2020; accepted 25 February 2020
Abstract. Domestic mites have been recognized as the most common allergen responsible
for respiratory allergy. Herein, we report a case of anaphylaxis due to ingestion of dust mite-
contaminated food. A 14-year-old boy presented to the Emergency Department with chest
discomfort, wheezing, eyelid angioedema, and urticarial rash twice in a month after eating
meals, including tempura fried squids and onion fritters (containing wheat flour, eggs, squid,
and onion). Anaphylaxis had been diagnosed and successfully treated. The investigations
showed that the patient was sensitive to house dust mites. Positive skin prick-to-prick test
response to incriminated flour and negative tests to wheat allergen extract and uncontaminated
flour were demonstrated. The microscopic analysis of causative cooking flour identified the
presence of Dermatophagoides farinae. During the oral food challenge test, the patient was
able to eat tempura-fried squids and onion fritters, made with uncontaminated flour, without
any adverse reaction. Hence, oral ingestion of dust mite-contaminated food was the culprit of
this severe allergic reaction.
INTRODUCTION been described in different parts of the world
(Tay et al., 2008; Sanchez-Borges et al., 2013;
Anaphylaxis is an acute serious systemic Takahashi et al., 2014; Sanchez-Borges &
hypersensitivity reaction which can be Fernandez-Caldas, 2015). It has now been
fatal. It requires immediate diagnosis and widely recognized that mites should be
treatment. Food is the most common cause regarded as a potential hidden food allergen
of anaphylaxis around the world (Dhami & (Sanchez-Borges & Fernandez-Caldas, 2015).
Sheikh, 2017; Rangkakulnuwat et al., 2020; Here we report a rare case of anaphylaxis
Chaaban et al., 2019). Domestic dust mites in a teenager caused by ingestion of mite-
(Dermatophagoides farinae, and Derma- contaminated food which is likely to be
tophagoides pteronyssinus) have been overlooked by clinicians.
identified to be the most common allergen
sources responsible for the pathogenesis
of respiratory allergy, especially asthma CASE REPORT
and allergic rhinitis (Malainual et al., 1995,
Thomas, 2010). The major route of dust A 14-year-old boy presented to the Emergency
mite exposure causing hypersensitivity Department (ED) at Chiang Mai University
reactions had been thought to be by Hospital, Chiang Mai, Thailand with chest
inhalation. However, in 1993, anaphylaxis discomfort, eyelid and lip swelling, and an
caused by the ingestion of mite-contaminated urticarial rash which started about ten
foods was first described by Erben et al. minutes after having meals. On arrival at
(Erben et al., 1993). Since then, a number the ED, his blood pressure, pulse rate, and
of patients with ‘oral mite anaphylaxis’ have oxygen saturation were within normal limits,
318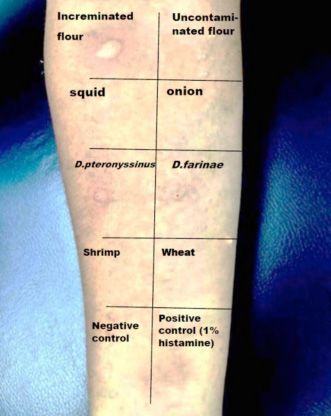
but his respiratory rate was rapid at 30 Investigations
breaths/min. The physical examination The patient’s mother prepared onion fritters
revealed generalized urticaria, eyelid and lip and tempura fried squids at home using
angioedema. Wheezing was auscultated over cooking flour (Gogi®, Bangkok, Thailand,
both lung fields. Anaphylaxis was diagnosed containing 90% wheat flour, 6% tapioca, 3%
and immediate treatment with intramuscular baking powder), eggs, cooking oil, squids, and
epinephrine, intravenous antihistamine and onion. The same cooking flour from the
corticosteroids was given. He fully recovered same container was used to cook both foods.
after the treatment. It was purchased two weeks ago within a
The patient had a similar episode of sealed package from the manufacturer, then
anaphylaxis one month before the incident. was unpacked and had been kept in a reused
The symptoms started about 15 minutes closed plastic container in the kitchen’s
after having a different meal at home. The cupboard.
triggering foods of the previous and present The mother provided a sample of the kept
episodes were onion fritters and tempura cooking flour. The gross appearance of the
fried squids. The foods were freshly prepared flour showed a color change which may
by the patient’s mother. He insisted that all imply some contamination (Figure 1). Under
food ingredients had been consumed before a stereomicroscope, living mites, mite feces,
several times without any problem. No other and mite’s molt were seen with the total count
family members who had eaten the same of ~18,310 mites/1 gram of flour. D. farinae
foods with the patient had any adverse was then identified by the entomologist at the
reaction. Department of Parasitology, Faculty of
Furthermore, the patient had a history of Medicine, Chiang Mai University using a
Naproxen (non-steroidal anti-inflammatory light microscope (Olympus CX41 with
drug; NSAID) hypersensitivity in the last two Olympus DP22 digital camera, Olympus
years. He complained of having rashes after Corporation, Tokyo, Japan) and the key of
eating shrimp several years ago. Neither Matthew J. Colloff (2009) for dust mites
personal history of allergic rhinitis and (Colloff & SpringerLink (Online service),
asthma nor allergic history in the family was 2009) (Figure 2).
identified.
Figure 1. Gross Appearance of the Cooking Flour.
319Figure 2. Dermatophagoides farinae (A: female, B: male; light microscopic with 10x objective
lens).
Figure 3. Skin Prick Test Results.
A skin prick test (SPT) was performed a prick-to-prick method (Bernstein et al.,
using commercial allergen extracts (Alk 2008) using the kept cooking flour from the
ABello®, Port Washington, NY, USA). The patient’s kitchen, newly opened cooking
patient had a positive skin prick test for both flour from the manufacturer’s package
dust mites, D. farinae, and D. pteronyssinus, (Gogi®), cooked squid and cooked onion. The
but negative results for wheat grain and results revealed positive only for the kept
shrimp. We also performed skin prick test with cooking flour (Figure 3).
320Table 1. Specific IgE Results * to food made with flour which had been
previously tolerated. Although oral food
Allergen Value (kUa/L) challenge with contaminated flour was not
D. pteronyssinus 6.54
done regarded patient’s history of severe
D. farinae 7.86 reactions, strongly positive results of
Shrimp 1.37 sensitivity to house dust mites and
Wheat 2.69 contaminated flour, and a negative result
Squid 1.80 for uncontaminated flour, squid and onion
supported our diagnosis.
* ImmunoCAP, Thermo Fisher, USA.
However, there were weakly positive
sensitivities in vitro to shrimp, squid and
Specific IgE in the blood was determined wheat. This could be the cross-reactivity
by ImmunoCAP®, (Thermo Fisher, USA) and which was already confirmed with the
results are shown in Table 1 with a cut-off tolerance of an oral food challenge with
value of 0.35 kUa/L. It revealed positive to shrimp, wheat, and the same foods prepared
D. farinae, D. pteronyssinus, shrimp, and with uncontaminated flour. In patients
wheat. In order to identify the culprits, we with oral mite anaphylaxis, NSAID hyper-
performed the oral food challenge tests with sensitivity has been observed in up to 40%
squid, onion, shrimp, and newly opened of the patients. It has been included as one
(uncontaminated) cooking flour. Shrimp was of the risk factors and the proposed criteria
included in our investigation to exclude for diagnosis (Sanchez-Borges et al., 2013;
allergen cross-reactivity and to confirm Sanchez-Borges & Fernandez-Caldas, 2015).
clinical relevant with laboratory results. Moreover, a case of dust mite ingestion-
Patients passed all the oral food challenge associated, exercise-induced anaphylaxis
test without any reactions. has been reported recently (Sompornrat-
tanphan et al., 2020).
Oral mite anaphylaxis is a rare con-
DISCUSSION dition. The prevalence is still unknown. It
is identified as the immediate occurrence of
We have demonstrated a case of anaphylaxis severe allergic hypersensitivity after eating
due to ingestion of mite contaminated food contaminated with mites. New cases
food or ‘oral mite anaphylaxis’ which was have been reported from various regions of
confirmed by means of the microscopic the world. It is frequently reported mainly
identification of D. farinae in the con- from the geographical areas with high
taminated flour. The patient fulfilled the temperature and humidity (Sanchez-Borges
described criteria for the diagnosis of oral et al., 2009; Sanchez-Borges et al., 2013).
mite anaphylaxis (Sanchez-Borges et al., Foods prepared with mite-contaminated
2013) which is based on clinical and wheat flour have been the most frequently
laboratory characteristics of 1) rapid onset implicated (Sanchez-Borges et al., 2013).
of symptoms occurring after wheat-flour Many families of mites that have been
food intake 2) in vivo or in vitro testing demonstrated as triggers of oral allergic
demonstrating IgE-mediated sensitization reactions such as families Pyroglyphidae (D.
to mite allergen 3) positive immediate-type farinae and D. pteronyssinus), Glycyphagidae
skin test with suspected flour 4) negative (L. destructor), Echimyopodidae (B.
skin test to wheat and to uncontaminated tropicalis and B. freemani), Acaridae (A.
flour 5) clinical tolerance to food made with ovatus, T. putrescentiae, T. entomophagus),
uncontaminated flour 6) mite identified in and Suidasiidae (S. medanensis) (Sanchez-
suspected flour on microscopic examination Borges & Fernandez-Caldas, 2015, Masaki
and 7) hypersensitivity to NSAIDs. et al., 2019).
In this case, we suspected oral mite D. farinae, the mite species identified in
anaphylaxis rather than other ingredients the contaminated flour, is a common mite
in suspected foods because of the reaction found in the region of Southeast Asia and one
321of the most abundant allergens in Thailand should be taken into consideration in a patient
(Malainual et al., 1995; Thomas, 2010). The presenting with anaphylaxis after ingestion
name farinae comes from ‘farina’ in Latin of food made with flour even if it has
and originates from the observation that this previously been tolerated.
mite was found in flour. It is known to cause
deterioration of the food products it is living The authors have no conflict of
in, for example, wheat flour, food grains, dried interest to disclose
tea leaf, cereal, cheese, ham, chorizo, and The study was approved by the Research
salami. It was the most common cause of oral Ethics Committee of the Faculty of
mite anaphylaxis in previous studies. Medicine, Chiang Mai University
Inoculation with one gram of D. farinae mites Hospital, Chiang Mai University.
into six different common cooking flours in This study was carried out without
Thailand showed that room temperature any external support.
(average 25–28°C) and a relative humidity
of approximately 75% are the most suitable
conditions for mite proliferation. The REFERENCES
refrigerator condition could inhibit mite
growth. Interestingly, it was demonstrated Bernstein, I.L., Li, J.T., Bernstein, D.I.,
that the mites preferably proliferate in flour Hamilton, R., Spector, S.L., Tan, R.,
containing high wheat mixed with a baking Sicherer, S., Golden, D.B., Khan, D.A.,
powder such as our culprit flour (Gogi®) Nicklas, R.A., Portnoy, J.M., Blessing-
than in 100% wheat, corn, or tapioca flour Moore, J., Cox, L., Lang, D.M.,
(Suesirisawad et al., 2015). Although most of Oppenheimer, J., Randolph, C.C.,
the mite allergens are heat labile, Sanchez- Schuller, D.E., Tilles, S.A., Wallace,
Borges et al. (2012) also demonstrated a skin D.V., Levetin, E., Weber, R., American
reaction to 100°C heated-contaminated wheat Academy of Allergy, Immunology &
flour in a dust mite sensitive patients. It was American College of Allergy and
suspected that heat-resistant ‘Group 2 mite Immunology. (2008). Allergy diagnostic
allergens’ were responsible for this allergic testing: an updated practice parameter.
reaction which appeared even in cooked Annual of Allergy, Asthma and Immu-
mite-contaminated foods (Sanchez-Borges nology 100: S1-148.
et al., 2012, Sanchez-Borges & Fernandez- Chaaban, M.R., Warren, Z., Baillargeon, J.G.,
Caldas, 2015). A previous study showed Baillargeon, G., Resto, V. & Kuo, Y.F.
that group 10 allergens (tropomyosins) is (2019). Epidemiology and trends of
the cause of co-sensitization between dust anaphylaxis in the United States, 2004-
mites, crustaceans, and some species of 2016. International Forum of Allergy
insects and mollusks. This may explain the and Rhinology 9: 607-614.
positivity of specific IgE to shrimp and Colloff, M.J. (2009). Identification and
squid in the patient (Shafique et al., 2012). taxonomy, classification and phylogeny.
Oral mite anaphylaxis can be easily In: Dust Mites, Colloff, M.J. (editor) 1st
prevented. The most important measure is edition. Dordrecht: Springer, pp.1-44.
to prevent food especially cooking flour from Dhami, S. & Sheikh, A. (2017). Anaphylaxis:
being contaminated with mites (Sanchez- epidemiology, aetiology and relevance
Borges & Fernandez-Caldas, 2015). The flour for the clinic. Expert Review of Clinical
must not be stored under a hot and humid Immunology 13: 889-895.
condition for long periods. It must be stored Erben, A.M., Rodriguez, J.L., McCullough, J.
in a sealed clean glass or plastic containers & Ownby, D.R. (1993). Anaphylaxis after
in the refrigerator, once opened. The ingestion of beignets contaminated with
contaminated flour can look white and dry Dermatophagoides farinae. Journal of
like normal, as the gross cannot be reliable Allergy and Clinical Immunology 92:
(Masaki et al., 2019). Oral mite anaphylaxis 846-849.
322Malainual, N., Vichyanond, P. & Phan-Urai, Sompornrattanaphan, M., Jitvanitchakul, Y.,
P. (1995). House dust mite fauna in Malainual, N., Wongsa, C., Jameekornrak,
Thailand. Clinical and Experimental A., Theankeaw, O. & Thongngarm, T.
Allergy 25: 554-560. (2020). Dust mite ingestion-associated,
Masaki, K., Fukunaga, K., Kawakami, Y. & exercise-induced anaphylaxis: a case
Haque, R. (2019). Rare presentation of report and literature review. Allergy
anaphylaxis: pancake syndrome. BMJ Asthma and Clinical Immunology
Case Report 12: e228854. 16: doi: 10.1186/s13223-019-0399-1.
Rangkakulnuwat, P., Sutham, K. & Lao- eCollection 2020.
Araya, M. (2020). Anaphylaxis: Ten-year Suesirisawad, S., Malainual, N., Tung-
retrospective study from a tertiary care trongchitr, A., Chatchatee, P., Suratannon,
hospital in Asia. Asian Pacific Journal N. & Ngamphaiboon, J. (2015). Dust mite
of Allergy and Immunology 38: 31-39. infestation in cooking flour: experi-
Sanchez-Borges, M. & Fernandez-Caldas, E. mental observations and practical
(2015). Hidden allergens and oral mite recommendations. Asian Pacific
anaphylaxis: the pancake syndrome Journal of Allergy and Immunology
revisited. Current Opinion in Allergy 33: 123-128.
and Clinical Immunology 15: 337-343. Takahashi, K., Taniguchi, M., Fukutomi, Y.,
Sanchez-Borges, M., Fernandez-Caldas, E., Sekiya, K., Watai, K., Mitsui, C., Tanimoto,
Capriles-Hulett, A. & Caballero-Fonseca, H., Oshikata, C., Tsuburai, T., Tsuriki-
F. (2012). Mite-induced inflammation: sawa, N., Minoguchi, K., Nakajima, H.
More than allergy. Allergy and & Akiyama, K. (2014). Oral mite
Rhinology (Providence) 3: e25-29. anaphylaxis caused by mite-
Sanchez-Borges, M., Suarez-Chacon, R., contaminated okonomiyaki/ pancake-
Capriles-Hulett, A., Caballero-Fonseca, mix in Japan: 8 case reports and a review
F., Iraola, V. & Fernandez-Caldas, E. of 28 reported cases. Allergology
(2009). Pancake syndrome (oral mite International 63: 51-56.
anaphylaxis). World Allergy Organiza- Tay, S.Y., Tham, E., Yeo, C.T., Yi, F.C., Chen,
tion Journal 2: 91-96. J.Y., Cheong, N., Chua, K.Y. & Lee, B.W.
Sanchez-Borges, M., Suarez Chacon, R., (2008). Anaphylaxis following the
Capriles-Hulett, A., Caballero-Fonseca, ingestion of flour contaminated by
F. & Fernandez-Caldas, E. (2013). house dust mites – a report of two cases
Anaphylaxis from ingestion of mites: from Singapore. Asian Pacific Journal
pancake anaphylaxis. Journal of Allergy of Allergy and Immunology 26: 165-170.
and Clinical Immunology 131: 31-35. Thomas, W.R. (2010). Geography of house
Shafique, R.H., Inam, M., Ismail, M. & dust mite allergens. Asian Pacific
Chaudhary, F.R. (2012). Group 10 Journal of Allergy and Immunology
allergens (tropomyosins) from house- 28: 211-224.
dust mites may cause covariation of
sensitization to allergens from other
invertebrates. Allergy and Rhinology
(Providence) 3: e74-90.
323You can also read

















































