Approccio diagnostico alle - (Obstetric Brachial Plexus Lesion) lesioni del plesso brachiale del neonato - SYMPOSIA ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Approccio diagnostico alle
lesioni del plesso brachiale del neonato
(Obstetric Brachial Plexus Lesion)
e altre neuropatie acquisite in età pediatrica
P. Lanteri
UOSD Neurofisiologia
Istituto Giannina Gaslini - Genova
29/10/19 P. Lanteri 1
Approccio diagnostico alle
lesioni del plesso brachiale del neonato
(Obstetric Brachial Plexus Lesion)
e altre neuropatie acquisite in età pediatrica
• Maturazione del SNP –
nervo e muscolo
• Dati normativi
• Obiettivo dell’esame
– Sito
– Tipo
– Pattern
– Time-course
– Esordio
– Assonale vs demielinizzante
– Sintomi associati/sistemi
coinvolti
• Forme genetiche vs
acquisite, malattie rare
29/10/19 P. Lanteri 2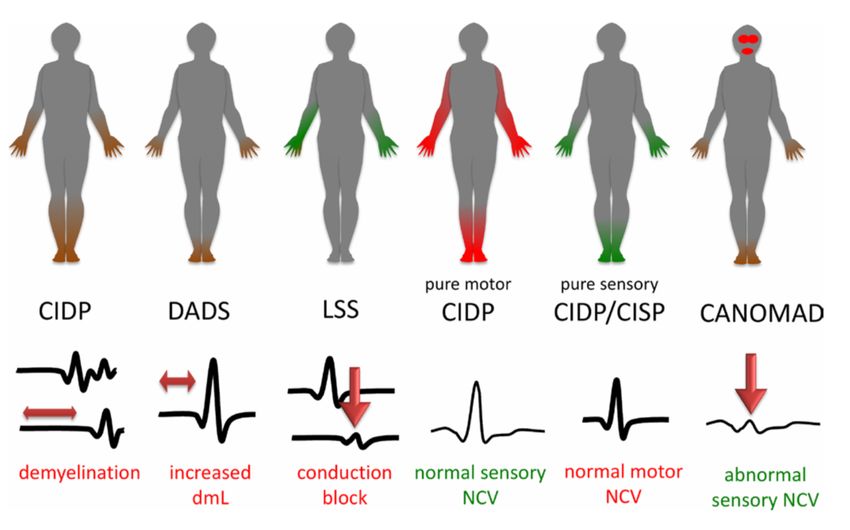
A considerable amount of work has been published about OBPP; the heterogeneity of the
injury has resulted in there being no clear paradigm of how to manage these children.
Furthermore, extrapolation of adult BPP management to OBPP has also caused confusion
as to the appropriate method and timing of repair.
important implications for the need and
timing of corrective surgery
29/10/19 P. Lanteri 3
29/10/19 P. Lanteri 4

Myogenic cells
Embryonic origins of
skeletal muscles
back muscles
head muscles
epaxial lip
of dermomyotom
paraxial
mesoderm
hypaxial lip of
dermomyotome
(and of cranial somites)
tongue diaphragm
posterior neck limb muscle
muscles
Nassari S, Duprez D and Fournier-Thibault C (2017) Non-myogenic
Contribution to Muscle Development and Homeostasis: The Role of
29/10/19 P. Lanteri Connective Tissues. Front. Cell Dev. Biol. 5:22. 5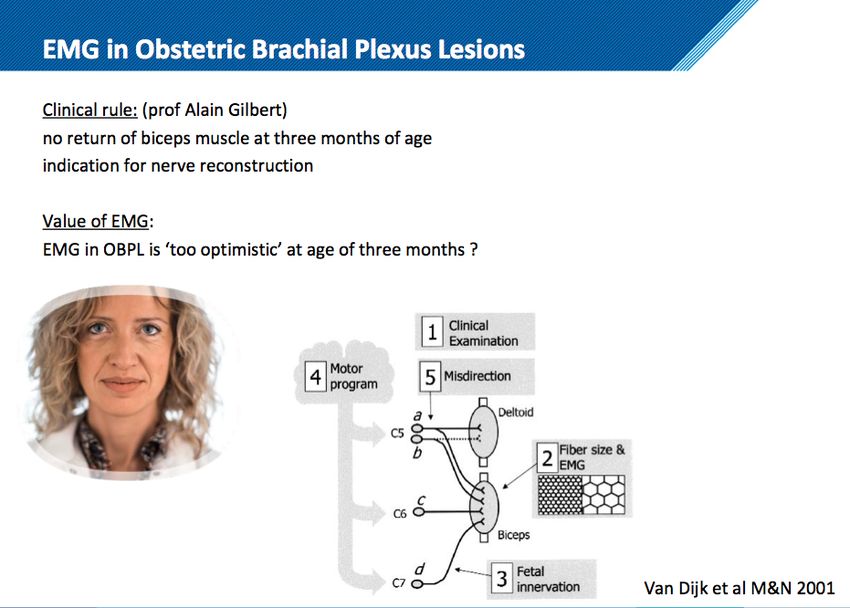
NERVE CONDUCTION AND ELECTROMYOGRAPHIC
CORRELATIONS WITH MOTOR UNIT MATURATION
• Some muscles such as
orbicularis oris and
genioglossus show a rapid
increase over the first 10 to 20
years followed by a little increase
over the rest of adulthood.
• Most other muscles do not show
the same rapid increase over the
first 2 decades of life.
• The increase in duration is
thought to be due to an increase
in the width of the endplate
zone with growth and to the
higher fiber density obtained by
a closer packing of the subunits.
29/10/19 P. Lanteri 6
29/10/19 P. Lanteri 7

Obstetric Brachial Plexus Lesion
• A closed nerve traction • Delivery by cesarean
injury to the brachial plexus section does not completely
in the perinatal period remove the risk of birth
palsy, although the
• Incidence: 0.4 and 5.1 likelihood drops to
approximately 0.02 %
children per 1000 births
• The extent of brachial plexus
damage and clinical
presentation varies
considerably, from transient
weakness to global paresis.
29/10/19 P. Lanteri 8
Obstetric Brachial Plexus Lesion
• Common fetal risk factors • Maternal risk factors
are: include:
– macrosomia, – gestational diabetes,
– high fetal birth weight, multiparity,
– SHOULDER DYSTOCIA, – cephalopelvic
– breech position. disproportion,
– prolonged second stage of
labor
29/10/19 P. Lanteri 9
Natural history • serial examinations are required to determine severity and recovery potential. • The majority of infants have spontaneous recovery within the first 3 months, with normal strength and range of motion • However, if by 3–6 months substantial recovery is not seen, a workup for surgical intervention is warranted. • Beyond physical impairment, OBPI impacts the family dynamic and the child’s global development. 29/10/19 P. Lanteri 10
Coroneos CJ, et al.
Obstetrical brachial plexus injury (OBPI):
Canada’s national clinical practice guideline.
BMJ Open 2017;7
• 1. Physically examine • Refer all newborns with
newborns for OBPI if upper OBPI to a
extremity movement is
asymmetric or delivery was
multidisciplinary
complicated by shoulder centre by 1 month of
dystocia, humeral fracture age.
or clavicular fracture. – A proportion of
newborns will
completely recover
within days of birth and
do not necessitate referral
to a multidisciplinary
centre.
‘good’ by 1 month of age, ‘satisfactory’ by 3 months of age and ‘poor’ thereafter.
29/10/19 P. Lanteri 11Physical exam • It is critical to recognize that the physical exam remains the most important tool for assessment and determination of the most impactful procedure for the individual patient. Clinical root level involvement (eg, presence of hand paralysis) and Horner’s syndrome are discerning characteristics in the Narakas classification for baseline injury classification. 29/10/19 P. Lanteri 12
Clinical presentation
• The shoulder is adducted and
internally rotated due to axillary and
suprascapular nerve injury (C5),
leading to deltoid, supraspinatus, and
infraspinatus muscle weakness.
• The elbow is extended due to
musculocutaneous nerve damage (C6)
and resulting biceps weakness.
• The forearm is pronated and wrist
and fingers flexed due to weakness in
the radial innervated supinator and
extensor carpi radialis longus and
brevis (C7)
29/10/19 P. Lanteri 13Narakas AO. The treatment of brachial plexus injuries.
Int Orthop 1985;9:29–36.
29/10/19 P. Lanteri 14• Timing of surgical intervention is unclear:
– Mild injuries with significant recovery by 1 month do not require
repair.
– Total plexus injuries require early repair to preserve function.
– However, 50–90% of referrals to specialty centres have injuries
between these extremes, with surgical indications and timing
varying between centres.
29/10/19 P. Lanteri 15The role of electromyography in the management of the brachial plexus palsy of the newborn
Matthew Pitt, Jan-Willem Vredeveld
Clinical Neurophysiology 116 (2005) 1756–1761
EMG
Can EMG assist in Can EMG help in
determining accurately assessing
AETIOLOGY? PROGNOSIS?
29/10/19 P. Lanteri 16The role of electromyography in the management of the brachial plexus palsy of the newborn
MaAhew PiA, Jan-Willem Vredeveld
Clinical Neurophysiology 116 (2005) 1756–1761
Can EMG
assist in
th viro rot e p
en t u
determining
e i n ec al
l
no ress
ata
nt me t f sie
AETIOLOGY?
p
n
ra n ro s
l o ??
p r
ut t d m
t a
n a r y?
er oe
re
P inju
in s
e
soon after birth:
changes of
chronic
denervation and
reinnervation.
more early
fibrillations and
appearance of the absence of the
no motor unit
fibrillations in CMAP
potentials,
the neonate
If EMG was clear of any
shortened by a in inverse correlation
fibrillations within 24 h
needle EMG changes of
factor of 7.5–10 to the volume of the chronic denervation,
of birth but showed them
denervated segment of which, if seen any time
times compared the nerve distal to
after 48 h: the birth itself
in the first week, è a
being the setting for the
to adults section. injury.
prenatal onset.
29/10/19 P. Lanteri 17The role of electromyography in the management of the brachial plexus palsy of the newborn
Matthew Pitt, Jan-Willem Vredeveld
Clinical Neurophysiology 116 (2005) 1756–1761
Can EMG help in It i
so
l f
accurately sig ife t ten
be ni ha on
t f l
assessing un wee ican t min y lat
aff n t t d or er
PROGNOSIS? ect he iff bu in
e a er t
ap d sid ffect ence
pa e ed s
ren be an
t com d
e
If neurapraxia is the
sole explanation for
the palsy no
intervention is
needed.
If there is any voluntary
movement: the
NCS will be normal, even
interference pattern
if the arm is paralysed or
recorded will be quite
even anaesthetic
easily distinguished
axonal discontinuity
29/10/19 P. Lanteri 18Neurotmesis
and
root avulsion
Muscle Nerve 55: 69–73, 2017
The accurate the loss of motor neurones is going to be very
identification
significant and become very rapidly apparent.
of
neurotmesis
and root the ‘overly optimistic EMG’ is a well recognised phenomenon
avulsion
should be the
primary a combination of the finding of fibrillation potentials, the preservation of
function of the SNAP, and a keen observation of how much the interference pattern has
EMG in the been reduced on needle EMG (Smith, 1996; Type C) can still be very accurately
correlated with the roots that are avulsed when seen at surgery (Kono and Birch, 1999).
assessment of
prognosis of the role of CMAP amplitude measurement as a method of
BPPN. quantification of the amount of nerve and root damage.
29/10/19 P. Lanteri 19CMAP and weakness è 10% rules
If the CMAP was less than 10% of that recorded from the opposite
CMAP and unaffected muscle it was highly correlated with significant
weakness at 6 months of age.
and Complete absence of a CMAP was associated with persistent weakness at
SNAP
6 months.
If this absence was in the C5/6 myotome then biceps would have persistent
weakness at 6 months.
reduced CMAP from stimulation of the musculocutaneous and axillary
nerves, correlated with severe involvement.
If an EMG was done before 7 days it is unlikely that reinnervation would
have started and the values of the CMAPs could be used as a baseline for
future comparison.
29/10/19 P. Lanteri 20Luxury
innervation
EMG
phenomenon of luxury
innervation seen only in neonates
and not in adults
it is present in both motor
(Vredeveld et al., 2000) and
sensory fibres (Colon et al., 2003).
at birth it is likely that C7 contributes to innervation of the biceps.
the explanation for a needle EMG If C5 and C6 are destroyed C7 may be the only nerve supply to
biceps and will reinnervate some of the denervated motor units.
showing a fullish interference
pattern but the muscle itself not Central remodelling may not be able to fully compensate and as a
result co-contraction may occur when elbow extension occurs
having the expected function. (Benaim et al., 1999) making the functional recovery worse than
would have been expected.
29/10/19 P. Lanteri 21Developmental apraxia
USE IT
OR
LOSE IT
Apraxia
Luxury innervation
Misrouting: outgrowing axons may end up in the wrong muscles.,
may still be driven by motor programmes. Explain co-contraction, a typical feature of
OBPLs at later age,
Neuroma in continuity
Central readaptation
29/10/19 P. Lanteri 22Timing
Electrodiagnosis in the period immediately following the birth within
48 h
performed at the nadir of the loss of the motor units,
presently unknown but likely to be at the end of the
first week, EMG, which specifically includes CMAP
amplitude measurements from proximal muscles,
one final EMG shortly before the operation for
preoperative planning.
29/10/19 P. Lanteri 23– However, recent studies have shown improved
reliability, where early EMG at 1 month
accurately predicted upper extremity paralysis
• Local extension
• Severity
• Child recovery potentials è evolution over time/speed
of recovery
29/10/19 P. Lanteri 24At 1 month of age, nEMG
had excellent sensitivity to
predict absent elbow
flexion at 3 months, which
was much better than
assessment at 1 week or 3
29/10/19
months.
P. Lanteri 25Needle electromyography at 1 month predicts paralysis of elbow flexion at 3 months in obstetric
brachial plexus lesions
If there are no active units in profound discrepancy
deltoid and biceps, this has a between nEMG and clinical
strong correlation with lack of findings (97% vs 45%) at the
recovery of biceps function by 3 age when clinical decisions
months of age. are usually made.
‘inactive MUPs’ in the biceps muscle >> >> >>
Absent movements > >>
rate of absent MUPsNeedle Electromyography
Positive sharp waves and fibrillation potentials
ADULTS
positive sharp waves and CHILDREN
fibrillation potentials
The time that fibrillations
appear is in inverse
correlation to the volume of
21 days the denervated segment of the
nerve distal to section.
The length of the nerves in
babies and their diameter
show that the appearance of
fibrillations may be shortened
by a factor of 7.5–10 times
positive sharp waves and compared to adults (Van Djjk
fibrillation potentials et al., 2001), in which case the
appearance of fibrillations
within a day or two of injury
Time 0 è DENERVATION can be expected.
29/10/19 P. Lanteri 27In infants, motor unit
potentials are simpler
in configuration,
shorter in duration
(≈ 70% adult values),
and lower in
amplitude (≈ 20% to
50% of adult values).
Personal data
29/10/19 P. Lanteri 28Shape properties of MUAPs
during maturation
29/10/19 P. Lanteri 29EMG D Bicipite brachiale
500µV 500ms
1.2
1.3
1.4
1.5
1.6
29/10/19 P. Lanteri 30EMG D Bicipite brachiale EMG D Bicipite brachiale
500µV 500ms 100µV 100ms
1.1 1.42
1.2 1.43
1.3 1.44
1.4 1.45
1.5 1.46
29/10/19 P. Lanteri 3129/10/19 P. Lanteri 32
L Mediano - APB D Ulnare - ADM
L Muscolocutaneo - Biceps
2mV 50ms 5mV 30ms 5mV2 20ms
1 3 Wrist 1
2
21,3mA
1 3 Wrist 2
2 40,5mA 2
1 3 B.Elbow 2
1 3 Erb's Pt 1 37,8mA
45,0mA 2
1 3 2
Elbow 3
1 3
40,5mA A.Elbow 3
37,8mA
D Muscolocutaneo - Biceps D Mediano - APB D Radiale - EIP
1mV 50ms 5mV 30ms 1mV 20ms
2
2 2 3
1 3 1 3 1 Forearm 1
Erb's Pt 1 Wrist 2
40,9mA
80,4mA 55,1mA
2 3
2 1 Elbow 2
2
1 3 1 3 Elbow 3 63,7mA
Erb's Pt 2
67,1mA 55,1mA
29/10/19 P. Lanteri 33CL, 05.02.2018, data esame 07.05.2018
Motor NCS
29/10/19 P. Lanteri 3429/10/19 P. Lanteri 35
CL, 05/02/2018, data esame 8/05/2018
parto distocico, estensione, intrarotazione ed adduzione AS dx,
motilità assente: lesione totale plesso br dx
• Plurimi pseudomeningoceli apparentemente post-gangliotici da C5
a T1 a dx
• Neuroma post-traumatico a sviluppo interscalenico e postscalenico
29/10/19 P. Lanteri 36• Lesione del tronco primario superiore allungato e con
neuroma in continuità
29/10/19 P. Lanteri 37A considerable amount of work has been published about OBPP; the heterogeneity of the
injury has resulted in there being no clear paradigm of how to manage these children.
Furthermore, extrapolation of adult BPP management to OBPP has also caused confusion
as to the appropriate method and timing of repair.
Entro 48h
1 mese
3 mesi
…..
CMAP
Cause muscolocutaneo
Prognosi ulnare
Programma pre operatorio radiale
Follow up SAP
EMG bicipite brachiale
…..
important implications for the need and
timing of corrective surgery
29/10/19 P. Lanteri 38Valori normativi
0-2 VCN Gruppo di studio
SINC Neurofisiologia Pediatrica
• The same parameters as in adults are
studied.
• No standard distances between
stimulation and recording.
• In children scheduled for EMG, the
NCS precede EMG.
29/10/19 P. Lanteri 3929/10/19 P. Lanteri 40
Median n 29/10/19 P. Lanteri 41
Peroneal n 29/10/19 P. Lanteri 42
type of nerve
injury
demyelinating axonal combined
NONUNIFORM UNIFORM
ACQUIRED
(but …CMTX, HNPP,
toxin exposure such as HEREDITARY
gasoline sniffing and
diphtheria)O.N. n. 20/02/2005: VCM
Motor NCS S ULNAR - ADM
2
1 3 5
Wrist 1
30ms 2mV
2 4
1 3
B.Elbow 2
4
30ms 2mV
A.Elbow 3
1 2
3 30ms 200µV
Motor NCS S COMM PERONEAL - EDB Motor NCS S TIBIAL (KNEE) - AH
2
2
1 3 1 3 4 5 Ankle 1
5 Ankle 1
50ms 1mV
4 50ms 2mV
2
1 3
5 Fib Head 2
4
50ms 2mV 2
2 3
1 1 4 5
3 Knee 2
3 50ms 100µV 50ms 1mVO.N. n. 20/02/2005: VCS
Sensory NCS S MEDIAN - Digit II
2
4
1
Wrist 1
3
10ms 20µV
2
CIDP
Sensory NCS S SURAL - Lat Malleolus 10ms 10µV
10 Sensory NCS S ULNAR - Digit V
Calf 1
10ms 10µV
9
3
2
1
2
1
3 Wrist 1
10ms 20µVLehmann HC, et al. J Neurol Neurosurg Psychiatry 2019;0:1–7.
Variants of CIDP
82% 18%
7% 4% 4% 3.5%
29/10/19 P. Lanteri 4629/10/19 P. Lanteri 47
Pz di 3 aa, Giorno 5= persistenza di difficoltà di deambulazione,
trasferimento presso il P.S. ecografia delle articolazioni coxo-femorali
(negativa), areflessia
•Studio elettrofisiologico (14/11):
Sensory NCS D SURAL - Lat Malleolus
Motor NCS D COMM PERONEAL - EDB
2
1 Ankle 1
2
20ms 1mV
2 1
4 Calf 1
3 15ms 10µV
1 Fib Head 2
20ms 1mV
30 10
HReflex D TIBIAL (KNEE) - Soleus F Wave S TIBIAL (KNEE) - AH
1.29
F Wave 2mV 500µV
1.27
Nervo Lat. F min Lat. F max LatF media 2mV 500µV 74V
ms ms ms 1.28
S TIBIAL (KNEE) - AH 35,05 36,35 35,52 200µV 500µV
1.6
1.5
1.30 1.1
1.4
1.8
1.3
200µV 100ms 500µV 58V 1.10
HReflex 5mV 100ms 500µV
Nervo Resp. No H Max H Lat. H Amp. 1.26
ms mV 500µV 500µV
D TIBIAL (KNEE) - Soleus 0,0
Neurofisiologia con incremento della latenza distale del CMAP e rallentamento della velocità di conduzione motoria,
riflesso H assente
Rachicentesi: proteine totali 145 mg/dl (v.n. 20-40), conteggio cellule 8/mm3 (prevalenza mononucleati) ==>
poliradicolonevrite infiammatura acuta demilinizzante
29/10/19
è Ciclo di immunoglobuline 2gr/Kg in 5 giorni. P. Lanteri 48A I J,
f nata il 08/12/2010
ricovero dal 13/11 al 18/12/2013
peggioramento clinico e risposta alla terapia
Motor NCS D TIBIAL (KNEE) - AH Motor NCS D COMM PERONEAL - EDB
2
2
3 Ankle 1
1 3 Ankle 1 1 2 5 50ms 500µV
5 30ms 100µV 4
4
3
1
Fib Head 2
50ms 500µV
4
29/10/19 P. Lanteri 49CRITICAL ILLNESS NEUROPATHY 29/10/19 P. Lanteri 50
sospetta encefalopatia epilettica severa con stato di male epilettico
refrattario del tipo FIRES:
FIRES = febrile infection related epileptic syndrome ESORDIO
• EEG: presenza di complessi punta/onda sincroni ed UTI IGG
asincroni in sede centro-temporo-occipitali dx>sn.
TERAPIE
eseguite
ACCERTA
MENTI
DECORSO
CONSIDE
RAZIONIalcune
29/10/19 crisi disautonomiche con ipertensione,
P. Lanteri rossore al volto ed AA 5229/10/19 P. Lanteri 53
D Tibiale - AH
5mV 60ms
2
1
3 Ankle 1
100mA
2
1 3
Pop fossa 2
99,6mA
29/10/19 P. Lanteri 5429/10/19 P. Lanteri 55
29/10/19 P. Lanteri 56
QUANTIFICAZIONE DELL’INNERVAZIONE EPIDERMICA
L’innervazione epidermica appare ridotta in maniera significativa in
sede distale e prossimale dell’arto inferiore esaminato
(sec. “Epidermal Nerve Fiber Density” Arch.Neurol/Vol.55,Dec1988).
Coscia prossimale: 8.09/mm Gamba distale: 4.34 /mm
(12.8 IENF/mm; SE= 0.035) (13.5 IENF/mm; SE= 0.026)
29/10/19 P. Lanteri 57S Mediano - Digit II (Antidromic)
20µV 15ms
2
1 Wrist 2
3
7,94mA
6
29/10/19 P. Lanteri 58TALIDOMIDE
Neurotossicità Periferica
(TIPN - Thalidomide-induced peripheral neuropathy)
modificazioni funzionali e metaboliche
dei gangli delle radici dorsali
proprietà anti-angiogeniche
danno microvascolare a livello dei vasa nervorum
conseguente riduzione del flusso ematico a nervo
inibizione del fattore nucleare (NF)-
Motor NCS D COMM PERONEAL - EDB
kB fattore di trasduzione di fattori di crescita
2
neuronali, con conseguente disregolazione
!"#$%&'()# *%)+,$%( -,".'/)$01 NOB
dell’attività neurotrofinica Motor NCS D COMM PERONEAL - EDB
2
1 3
4 2
!"#$ % S4,$%(&#+, /%+2"$%# '"4*&;+$)-7 :"+!"/ G2*" ;*";+*+$%&'! &( $)" "'/&'"4*%+, #&'$"'$ +($"* &!0%#+$%&'7 5&9 D+$%"'$ B8T $)" G*!$ $.&
*&.! !)&. G2*"! +$ /%(("*"'$ !$+1"! &( U+,,"*%+' /"1"'"*+$%&' +'/ &'" G2*" 5G2*" +9 !)&.%'1 $)*"" /"0-",%'+$"/ !"10"'$! 52"$.""'
+**&.!97 V!0%40 $"$*&>%/" !$+%'%'17 5'9 D+$%"'$ ET +,, $)" G2*"! &( $)%! 1*&4; +*" 4'/"*1&%'1 +>&'+, /"1"'"*+$%&'7 W+*T IJ !07
Neuropatia sensitiva assonale lunghezza dipendente
Ankle 1
20ms 1mV
1 3
4
5
Ankle 1
2 20ms 2mV
Downloaded from by guest on November 4, 2014
1 3 Fib Head 2
!"#$ ( W,&&/ 3"!!", ,"!%&'! +'/ *"/ #",, !"";+1" %' $)"
"'/&'"4*%40 &( ;+$%"'$ BJ7 X B !0 $)%#Y #*&!!L!"#$%&' !)&.%'1 +'
"'/&'"4*%+, #+;%,,+*- .%$) $)%#Y"'"/ .+,, +'/ *"/ #",, 5Z9 !"";+1"
%' $)" "'/&'"4*%407 [&$" $)" 0+*Y"/ *"/4#$%&' &( $)" /"'!%$- &(
!"#$ ) \+!#4,%$%! +'/ "'/&'"4*%+, )+"0&**)+1" %' ;+$%"'$ BO7
]&'1%$4/%'+, !"#$%&' &( + ;+*+(G'L"02"//"/ '"*3" !)&.%'1 +'
%0;&*$+'$ %'F+00+$&*- %'G,$*+$" .%$) 0&'&'4#,"+* #",,! +*&4'/
4 20ms 2mVTALIDOMIDE
Indicazioni
Patologie in cui è coinvolto il TNF-α come mediatore dell’infiammazione:
ü Mieloma multiplo
ü Cachessia ed ulcerazioni aftose esofagee correlate all’HIV
ü Malattia di Behçet
ü LES ed altre connettiviti
ü Malattie infiammatorie croniche intestinali
ü Pyoderma gangrenosum
ü Artrite reumatoide
ü Spondilite anchilosante
ü Sindrome di Sjogren
Motor NCS D COMM PERONEAL - EDB
2 ü Graft-versus-host disease
!"#$%&'()# *%)+,$%( -,".'/)$01 NOB
Motor NCS D COMM PERONEAL - EDB
ü alcune neoplasie solide 2
1 3 Ankle 1 1 3 5
Ankle 1
4 2
!"#$ % S4,$%(&#+, /%+2"$%# '"4*&;+$)-7 :"+!"/ G2*" ;*";+*+$%&'! &( $)" "'/&'"4*%+, #&'$"'$ +($"* &!0%#+$%&'7 5&9 D+$%"'$ B8T $)" G*!$ $.&
*&.! !)&. G2*"! +$ /%(("*"'$ !$+1"! &( U+,,"*%+' /"1"'"*+$%&' +'/ &'" G2*" 5G2*" +9 !)&.%'1 $)*"" /"0-",%'+$"/ !"10"'$! 52"$.""'
+**&.!97 V!0%40 $"$*&>%/" !$+%'%'17 5'9 D+$%"'$ ET +,, $)" G2*"! &( $)%! 1*&4; +*" 4'/"*1&%'1 +>&'+, /"1"'"*+$%&'7 W+*T IJ !07 20ms 1mV 4
2 20ms 2mV
Downloaded from by guest on November 4, 2014
1 3 Fib Head 2
!"#$ ( W,&&/ 3"!!", ,"!%&'! +'/ *"/ #",, !"";+1" %' $)"
"'/&'"4*%40 &( ;+$%"'$ BJ7 X B !0 $)%#Y #*&!!L!"#$%&' !)&.%'1 +'
"'/&'"4*%+, #+;%,,+*- .%$) $)%#Y"'"/ .+,, +'/ *"/ #",, 5Z9 !"";+1"
%' $)" "'/&'"4*%407 [&$" $)" 0+*Y"/ *"/4#$%&' &( $)" /"'!%$- &(
!"#$ ) \+!#4,%$%! +'/ "'/&'"4*%+, )+"0&**)+1" %' ;+$%"'$ BO7
]&'1%$4/%'+, !"#$%&' &( + ;+*+(G'L"02"//"/ '"*3" !)&.%'1 +'
%0;&*$+'$ %'F+00+$&*- %'G,$*+$" .%$) 0&'&'4#,"+* #",,! +*&4'/
4 20ms 2mV3,3% Incidenza TIPN
10%
30%
No TIPN
TIPN sensitiva
TIPN motoria 70%
56,7% TIPN sensitivo-
motoria
Evoluzione a
Primo episodio
SM
Nessun episodio di TIPN 18 (30%)
Motor NCS D COMM PERONEAL - EDB
2 TIPN Sensitive 34 (56,7%) 3/34 (8,8%)
!"#$%&'()# *%)+,$%( -,".'/)$01 NOB
Motor NCS D COMM PERONEAL - EDB
TIPN Motorie 6 (10%) 2/6 (33,3%)
2
1 3
4 2
!"#$ % S4,$%(&#+, /%+2"$%# '"4*&;+$)-7 :"+!"/ G2*" ;*";+*+$%&'! &( $)" "'/&'"4*%+, #&'$"'$ +($"* &!0%#+$%&'7 5&9 D+$%"'$ B8T $)" G*!$ $.&
*&.! !)&. G2*"! +$ /%(("*"'$ !$+1"! &( U+,,"*%+' /"1"'"*+$%&' +'/ &'" G2*" 5G2*" +9 !)&.%'1 $)*"" /"0-",%'+$"/ !"10"'$! 52"$.""'
+**&.!97 V!0%40 $"$*&>%/" !$+%'%'17 5'9 D+$%"'$ ET +,, $)" G2*"! &( $)%! 1*&4; +*" 4'/"*1&%'1 +>&'+, /"1"'"*+$%&'7 W+*T IJ !07
Ankle 1
20ms 1mV
TIPN Sensitivo-motorie 2 (3,3%) 1 3
4
5
Ankle 1
2 20ms 2mV
Downloaded from by guest on November 4, 2014
TIPN Totali 42 (70%) 1 3 Fib Head 2
!"#$ ( W,&&/ 3"!!", ,"!%&'! +'/ *"/ #",, !"";+1" %' $)"
"'/&'"4*%40 &( ;+$%"'$ BJ7 X B !0 $)%#Y #*&!!L!"#$%&' !)&.%'1 +'
"'/&'"4*%+, #+;%,,+*- .%$) $)%#Y"'"/ .+,, +'/ *"/ #",, 5Z9 !"";+1"
%' $)" "'/&'"4*%407 [&$" $)" 0+*Y"/ *"/4#$%&' &( $)" /"'!%$- &(
!"#$ ) \+!#4,%$%! +'/ "'/&'"4*%+, )+"0&**)+1" %' ;+$%"'$ BO7
]&'1%$4/%'+, !"#$%&' &( + ;+*+(G'L"02"//"/ '"*3" !)&.%'1 +'
%0;&*$+'$ %'F+00+$&*- %'G,$*+$" .%$) 0&'&'4#,"+* #",,! +*&4'/
4 20ms 2mVDose cumulativa
• TIPN sensitiva: compresa tra 7,9 g e 138 g con mediana di 25,5 g.
• TIPN motoria: compresa tra 1,1 g e 15,0 g con mediana di 9,4 g.
• TIPN mista: per un paziente 11,3 g e per l’altro 24,0 g.
Dose cumulativa soglia pari a 18,4 g per TIPN sensitiva
Cut-off: 18,375 g Evento di interesse: Comparsa della TIPN
1.00
Sensibilità: 66,7%
Specificità: 83,3%
0.75
0.50
0.25
0.00
Motor NCS D COMM PERONEAL - EDB
Area: 0,76 (IC95%: 0,62 – 0,87) 0 10 20 30 40 50
2
!"#$%&'()# *%)+,$%( -,".'/)$01 NOB
analysis time Motor NCS D COMM PERONEAL - EDB
TIPN Sensitiva TIPN Motoria
2
1 3 Ankle 1 1 3 5
Ankle 1
4 2
!"#$ % S4,$%(&#+, /%+2"$%# '"4*&;+$)-7 :"+!"/ G2*" ;*";+*+$%&'! &( $)" "'/&'"4*%+, #&'$"'$ +($"* &!0%#+$%&'7 5&9 D+$%"'$ B8T $)" G*!$ $.&
*&.! !)&. G2*"! +$ /%(("*"'$ !$+1"! &( U+,,"*%+' /"1"'"*+$%&' +'/ &'" G2*" 5G2*" +9 !)&.%'1 $)*"" /"0-",%'+$"/ !"10"'$! 52"$.""'
+**&.!97 V!0%40 $"$*&>%/" !$+%'%'17 5'9 D+$%"'$ ET +,, $)" G2*"! &( $)%! 1*&4; +*" 4'/"*1&%'1 +>&'+, /"1"'"*+$%&'7 W+*T IJ !07 20ms 1mV 4
2 20ms 2mV
Downloaded from by guest on November 4, 2014
1 3 Fib Head 2
!"#$ ( W,&&/ 3"!!", ,"!%&'! +'/ *"/ #",, !"";+1" %' $)"
"'/&'"4*%40 &( ;+$%"'$ BJ7 X B !0 $)%#Y #*&!!L!"#$%&' !)&.%'1 +'
"'/&'"4*%+, #+;%,,+*- .%$) $)%#Y"'"/ .+,, +'/ *"/ #",, 5Z9 !"";+1"
%' $)" "'/&'"4*%407 [&$" $)" 0+*Y"/ *"/4#$%&' &( $)" /"'!%$- &(
!"#$ ) \+!#4,%$%! +'/ "'/&'"4*%+, )+"0&**)+1" %' ;+$%"'$ BO7
]&'1%$4/%'+, !"#$%&' &( + ;+*+(G'L"02"//"/ '"*3" !)&.%'1 +'
%0;&*$+'$ %'F+00+$&*- %'G,$*+$" .%$) 0&'&'4#,"+* #",,! +*&4'/
4 20ms 2mVApproach to Evaluating Childhood
NeuropathiesL Estensore breve delle dita
1 2 1 2 1 2 1 2 1 2
1.1 1.2 1.3 1.4 1.5
1 2 1 2 1 2 1 2 1 2
1.6 1.7 2.1 2.2 2.3
Conclusioni
1 2 1 2 1 2 1 2 1 2
2.4 3.1 3.2 3.3 3.4
1 2 1 2 1 2 1 2 1 2
3.5 3.6 3.7 3.8 4.1
1 2 1 2 1 2 1 2 1 2
4.2 4.3 4.4 4.5 4.6
1 2 1 2 1 2
5.1 5.2 5.3
1mV
• Perché, Cosa e Quando?
50ms
• OBPL: importante controllo entro 1 mese
• L’esame elettroneuro/miografico può essere eseguito fin
dal primo giorno di vita
– Senza sedazione
– Al letto del paziente
– Attenzione alla corretta interpretazione
• Maturazione
• Valori normativi
– QEMG
– Importante:
• Inquadramento clinico per esame mirato
• eventualmente il controllo anche a breve distanza per conferma29/10/19 P. Lanteri 65
You can also read