ASCO 2022: Was gibt es Neues für die klinische Praxis? Varia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ASCO 2022:
Was gibt es Neues für die klinische Praxis?
Varia
Prof. Dr. med. Karin Jordan
Klinik für Hämatologie, Onkologie und Palliativmedizin, Klinikum Ernst von Bergmann, Potsdam
Nachlese zur Jahrestagung der Amerikanischen Gesellschaft für klinische Onkologie
Ernst-von-Bergmann Klinikum, 15.06.2022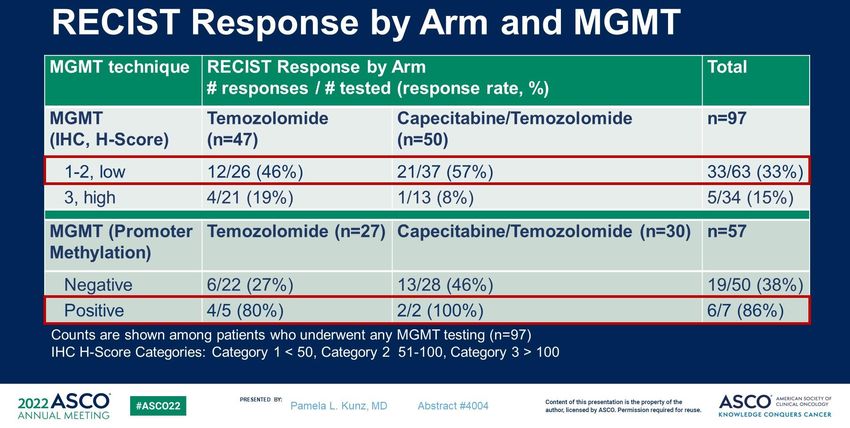
Studie und Hintergrund 6004: An open-label, noninferiority phase III RCT of weekly versus three weekly cisplatin and radical radiotherapy in locally advanced head and neck squamous cell carcinoma (ConCERT trial). Atul Sharma et al., Neu-Delhi, Indien Hintergrund: Patienten mit lokal fortgeschrittenen Plattenepithelkarzinome im Kopf- Hals-Bereich, Radiatio = Standard, Cisplatin = Standard, aber zeitliche Abfolge und Dosis von Cisplatin nicht abschließend geklärt Nicht-Unterlegenheitsstudie: wöchentliche Gabe von Cisplatin (40 mg/m2 x 7) versus 3-wöchentlichen Gabe Cisplatin (100 mg/m2 x 3)
Studiendesign
• Multizentrische Nichtunterlegenheitsstudie (6 Zentren in Indien)
N = 266 Patienten mit Tumoren im Kopf-Hals-Bereich
Strahlentherapeutische Intervention: 70 Gy, 35 Fraktionen über 7 Wochen
N = 133, Cisplatin 100 mg/m2 N = 133, Cisplatin 40 mg/m2
3-wöchentlich x 3 Gaben wöchentlich x 7 Gaben
• Primärer Endpunkt: 2 Jahre lokoregionale Kontrolle
• Sekundäre Endpunkte: Overall Survival (OS), Progression-free survivial (PFS),
Toxizität, Compliance
ASCO 2022: Atul Sharma et al., 6004: An open-label, noninferiority phase III RCT of weekly versus three weekly cisplatin and radical radiotherapy in locally
advanced head and neck squamous cell carcinoma (ConCERT trial).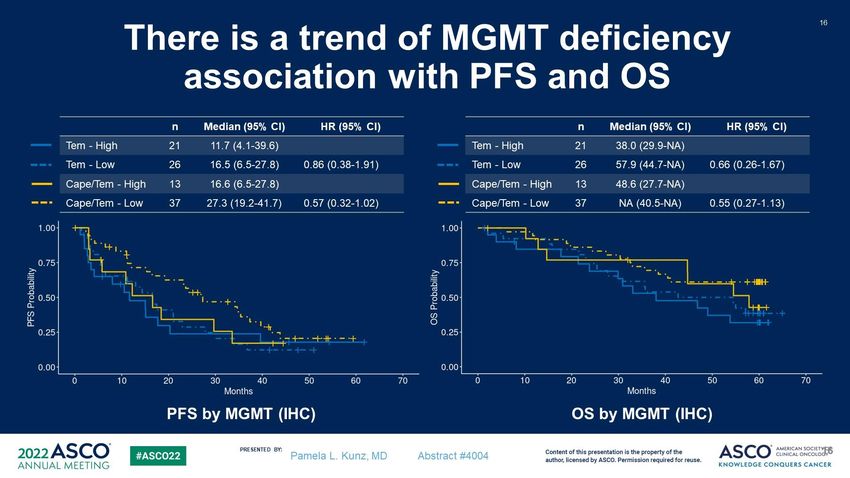
4
Treatment
Radiation treatment (similar in both arms):
• In 2D-conventional technique delivered on a Telecobalt machine patients
were treated to a dose of 70 Gray in 35 fractions over 7 weeks
• In SIB- IMRT or VMAT technique delivered on a medical linear accelerator, a
dose of 69.96 Gy in 33 fractions to high risk volume, 59.4 Gy in 33 fractions
to intermediate risk volume and 54Gy in 33 fractions at low risk volume
Chemotherapy:
• Standard (control): 3 weekly Cisplatin100 mg/m2 started on D1 of radiation
and given on days 1,22,43
• Test (experimental): Weekly Cisplatin40 mg/m2 started on D1 of radiation
and given on days 1,8,15,22,29,36,43
PRESENTED BY:
ATUL SHARMA, CONCERT TRIAL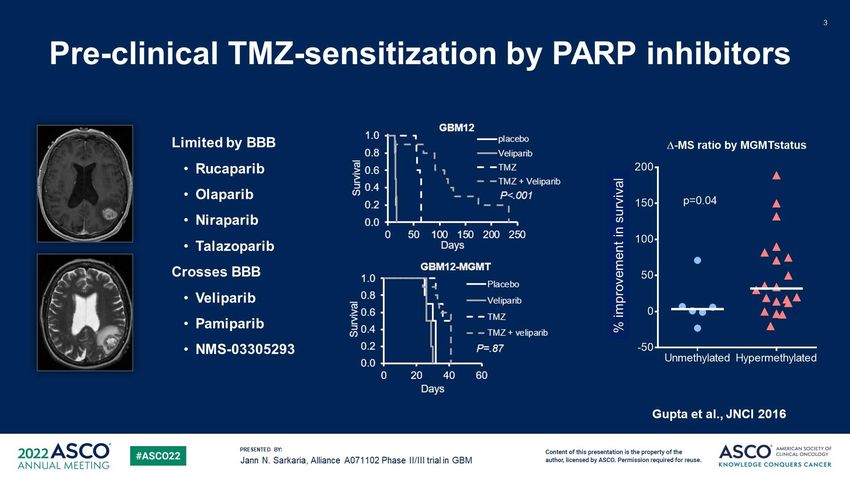
Ergebnisse - Endpunkte
Parameter Standard (Cis 100) arm Test (Cis 40) arm P value
No. (%) No.(%)
N = 133 (100) N = 133 (100)
Median Follow up (surviving patients) 25.7 months
Loco-regional failures 65 (48.9) 53 (39.9) 0.139
2 years loco-regional control % 56.39 % 60.90 %
Median Overall Survival (95% CI) 30 (20.4-39.7) 25.5 (13.3-37.5) 0.751
Median Progression-free survival 21.3 20.8 0.377
Median time to LRF 24.3 23 0.347
Restricted mean survival time 23.25 24.83 0.449
at 40 months
ASCO 2022: Atul Sharma et al., 6004: An open-label, noninferiority phase III RCT of weekly versus three weekly cisplatin and radical radiotherapy in locally
advanced head and neck squamous cell carcinoma (ConCERT trial).
Parameter Standard arm No. (%) Test arm No. (%) P value 6
133 (100), Cis 100mg/m² 133 (100)
Cumulative Chemo dose 0.312
Up to 199 mg/m2 25 (18.8) 21 (15.7)
200-279 mg/m2 54 (40.6) 69 (51.8)
280-300 mg/m2 49 (36.8) 77% 38 (28.5) 80%
No chemo received 3 3
Not treated 2 2
Median dose 225 (0-300) 240 (0-280)
Median % of chemo 76.6 85.7
Median number of Chemo 3 (0-3) 6 (0-7)
(range)
Median duration of Chemo 43 (0-94) 42 (0-81)
(range) days
Delays < 1 week 29 (21.8) 20 (15) 0.192
>1 week 27 (20.3) 25 (18.8)
No delays 74 (55.6) 83 (62.4)
PRESENTED BY:
ATUL SHARMA, CONCERT TRIAL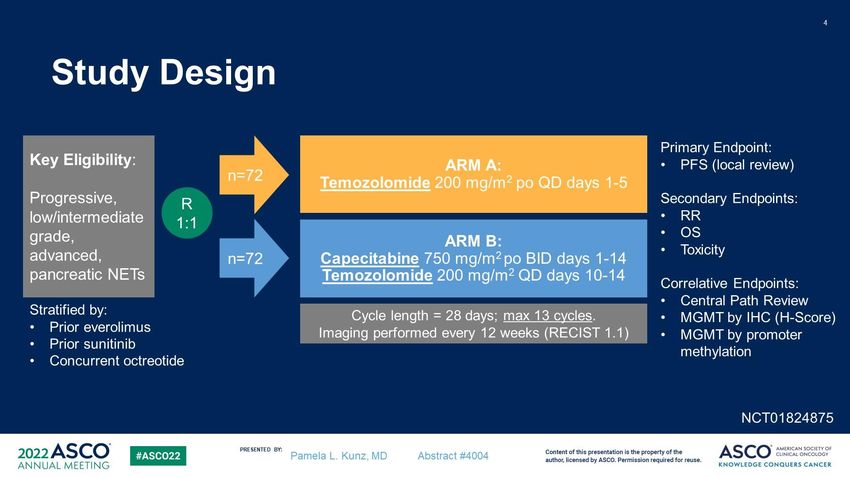
Toxicity 1- Grade III/IV
7
Parameter Standard arm Test arm 40 P value
100mg/m2 mg/m2
Number (%) Number (%)
133 (100) 133 (100)
Diarrhoea 5 (3.7) 0 .213
Mucositis 72 (54.1) 54(40.6) 0.039
Myelosuppression 20 (15) 10(7.5) 0.058
Ototoxicity 9(6.7) 5(3.7) 0.550
Renal 24(18) 5(3.7)
Toxicity-2 8
Parameter Standard arm Test arm 40 mg/m2 P value
100mg/m2 Number (%)
Number (%) 133 (100)
133 (100)
Hyponatremia 50 (37.5) 29 (21.8) 0.004
Hypokalemia 9 (6.7) 8 (6) 0.891
Weight reduction 54 (40.6) 46 (34.5) 0.811
>10%
IV fluids 83 (62.4) 46 (34.5) 0.0001
NG tube 53 (39.8) 40 (30) 0.072
Candida 34 (25.5) 28 (21) 0.400
Hospitalization 49 (36.8) 27 (20) 0.004
Interruptions 82 (61.6) 77 (57.8) 0.035
PRESENTED BY:
ATUL SHARMA, CONCERT TRIAL
Fazit
• Die kombinierte Radiochemotherapie mit wöchentlicher Cisplatin-Gabe ist 3-
wöchentlicher Cisplatin-Gabe nicht unterlegen
• Besser verträglich
• Weniger Unterbrechungen
• Weniger Hospitalisationen
• Geringere Toxizität
Concurrent weekly cisplatin in the dose of 40 mg/m2 along with RT should be
considered standard treatment in LA SCCHN in definitive setting
ASCO 2022: Atul Sharma et al., 6004: An open-label, noninferiority phase III RCT of weekly versus three weekly cisplatin and radical radiotherapy in locally
advanced head and neck squamous cell carcinoma (ConCERT trial).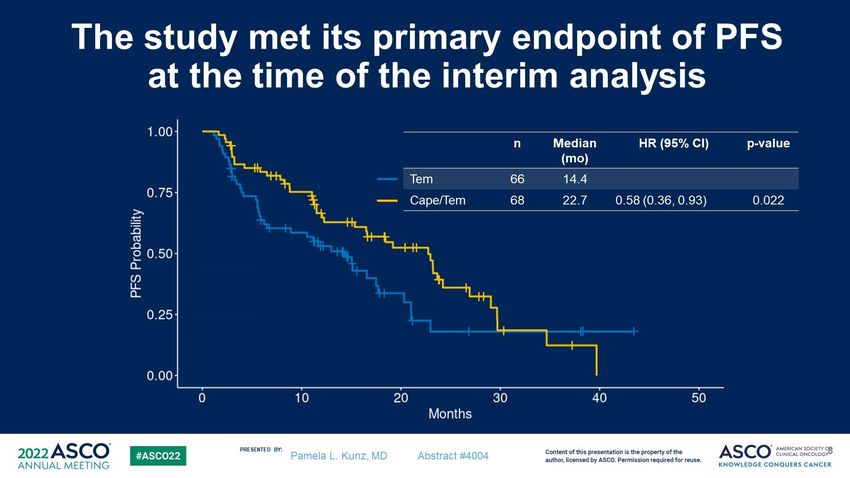
Prophylaxe der Mukositis 2022
• Standard ist und bleibt:
„Miracle Mouthwash“:
1001 Rezeptur
Leitlinienprogramm Onkologie: Supportive Therapie bei onkologischen PatientInnen – Langversion 1.0, 2016. AWMF Registernummer: 032/054OLStudie und Hintergrund 6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally advanced, nonmetastatic head and neck cancer (LAHNC). Carryn M. Anderson et al., Iowa City, Iowa, USA Hintergrund: Reduziert die Gabe von Avasopasem Mangan die Inzidenz schwerer oraler Mukositis bei Patienten mit Kopf-Hals-Tumoren, die Chemoradiotherapie erhalten?
Studiendesign
• 69 Zentren, Kanada und USA
N = 407 Patienten mit Plattenepithel-Tumoren im Kopf-Hals-Bereich, lokal fortgeschritten
Therapie: Intensitätsmodulierte Strahlentherapie (IMRT) + Cisplatin, 7 Wochen
N = 241, Avasopasem 90 mg N = 166, Placebo
60 minütige Infusion, Montag-Freitag, endet eine Stunde vor 60 minütige Infusion, Montag-
der Bestrahlung Freitag, endet eine Stunde vor der
Bestrahlung
• Primärer Endpunkt: Inzidenz schwerer oraler Mukositis (Grad 3 und 4) während der Radiotherapie
• Sekundäre Endpunkte: Dauer der schweren Mukositis, Inzidenz und Dauer von Mukositis Grad 4,
Sicherheit und Verträglichkeit
6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally
advanced, nonmetastatic head and neck cancer (LAHNC).
Carryn M. Anderson et al., Iowa City, Iowa, USAErgebnisse
Inzidenz schwere
Mukosits Δ 10 %
6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally
advanced, nonmetastatic head and neck cancer (LAHNC).
Carryn M. Anderson et al., Iowa City, Iowa, USAErgebnisse 6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally advanced, nonmetastatic head and neck cancer (LAHNC). Carryn M. Anderson et al., Iowa City, Iowa, USA
Ergebnisse 6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally advanced, nonmetastatic head and neck cancer (LAHNC). Carryn M. Anderson et al., Iowa City, Iowa, USA
Ergebnisse 6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally advanced, nonmetastatic head and neck cancer (LAHNC). Carryn M. Anderson et al., Iowa City, Iowa, USA
Fazit
Avasopasem 90 mg verringert statistisch signifikant und klinisch bedeutsam
schwere orale Mukositis:
↓ Inzidenz
↓ Dauer
↓ Schweregrad (Inzidenz von OM Grad 4)
↑ Zeitlicher Beginn der schweren oralen Mukositis
Bei der FDA zur Zulassung eingereicht
6005: ROMAN: Phase 3 trial of avasopasem manganese (GC4419) for severe oral mucositis (SOM) in patients receiving chemoradiotherapy (CRT) for locally
advanced, nonmetastatic head and neck cancer (LAHNC).
Carryn M. Anderson et al., Iowa City, Iowa, USAAus dem State of the art Vortrag von Prof. Bokemeyer, ASCO Direct
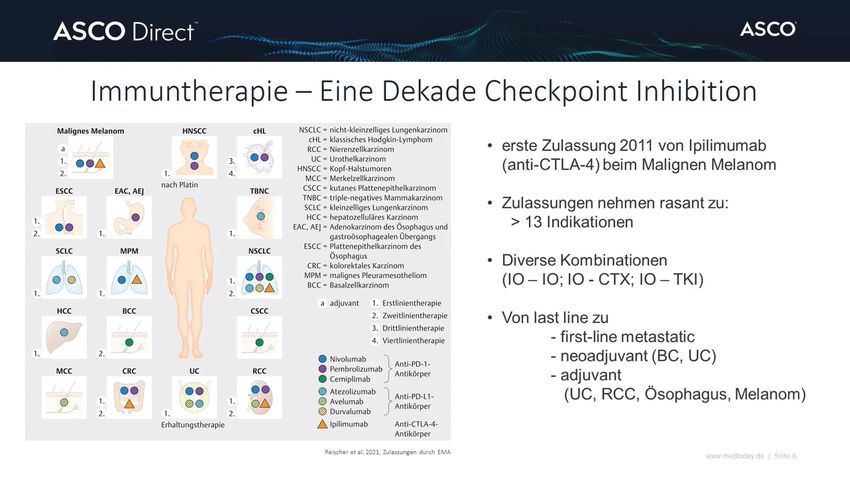
Einfluss supportiver Co-Medikation auf das Ansprechen von
Immuncheckpoint-Inhibitoren
Chalabi M. et al., Ann Oncol. 2020; 31(4):525-531;
Chalabi M. et al., Ann Oncol. 2020
(Retrospektive Analyse, 2 Studien, 1.512 Patienten)
Protonenpumpeninhibitoren bzw. Antibiotika in der Begleitmedikation bei NSCLC und Therapie
unter Atezolizumab:
Reduziertes Gesamtüberleben: 8,5 versus 14,1 Monate
(HR: 1,45; 95 % KI: 1,20-1,75; P = 0,0001)
43/44Studie und Hintergrund 12000: Impact of acetaminophen on the efficacy of immunotherapy in patients with cancer. Alban Bessede et al., Bordeaux, Frankreich Hintergrund: Hat die Schmerztherapie mit Paracetamol (Acetaminophen, APAP) bei fortgeschrittenem Tumorleiden Einfluss auf die Wirksamkeit der Immuntherapie? WHO empfiehlt seit 2015: vor und nach der Impfung kein Paracetamol
Studiendesign
Patienten mit fortgeschrittenen Tumorerkrankungen
CheckMate 025 Studie, Institutionelles Biomarker- Institutionelles Biomarker-
n = 297 Programm BIP, n = 34 Programm PREMIS, n = 297
N = 628, Untersuchung der Paracetamol-Exposition durch Plasma-Analyse
⇩
Korrelation mit klinischem Outcome
ASCO 2022: Alban Bessede et al., 12000: Impact of acetaminophen on the efficacy of immunotherapy in patients with cancer22
Results
• Publicly available serum metabolomics data from
297 patients with advanced renal cell carcinoma and
treated with nivolumab in the context of the
randomized phase III trial CheckMate 025
(NCT01668784)
• Patients with detectable levels of acetaminophen
or acetaminophen glucuronide had significantly
worse OS than patients without detectable APAP
levels at treatment onset
PRESENTED BY:23
Results
Quantitative approach
PREMIS STUDY
On multivariate analysis, presence of
acetaminophen or acetaminophen
glucuronide is independently associated
with worse PFS and OS
PRESENTED BY:Ergebnisse
• Nachweisbare APAP-Level im Plasma zu Behandlungsbeginn mit Immuncheckpoint-Inhibitoren
Signifikant schlechteres klinisches Outcome
• Unabhängig von anderen prognostischen Faktoren
– Alter, Performance-Status, Anzahl der vorherigen Behandlungen, Tumorart, Anzahl der
Metastasen, LDH Level
Starke klinische Evidenz für die Rolle von Paracetamol als potentieller
Suppressor der antitumoralen Immunität (wohl über direkten oder indirekten
Effekt der Treg Zellen)
Einsatz bei Immuncheckpoint-Inhibitor-Therapie mit Vorsicht
ASCO 2022: Alban Bessede et al., 12000: Impact of acetaminophen on the efficacy of immunotherapy in patients with cancerAusblick ASCO 2022: Alban Bessede et al., 12000: Impact of acetaminophen on the efficacy of immunotherapy in patients with cancer
Studie und Hintergrund 2001: Randomized phase II/III trial of veliparib or placebo in combination with adjuvant temozolomide in newly diagnosed glioblastoma (GBM) patients with MGMT promoter hypermethylation (Alliance A071102). Jann Nagina Sarkaria et al., New York, USA Hintergrund: PolyADP-Ribose-Polymerase (PARP) „Veliparib“ als Modulator der DNA- Reparatur nach einer Therapie mit Temozolomid Besteht für Patienten mit Glioblastom einen Überlebensvorteil, wenn Temozolomid (TMZ) zusammen mit dem PARP-Inhibitor Veliparib verabreicht wird?
Studiendesign
N = 429
Patienten mit neu diagnostiziertem Glioblastom und MGMT-Promotor-Hypermethylierung
Bestrahlung + Temolzolomid
N = 212; Adjuvante Therapie mit N = 217; Adjuvante Therapie mit
Temozolomid (d1-5, q28) + Temozolomid (Tage 1-5, q28) +
Placebo (Tage 1-7, q28) für bis zu 6 Zyklen Veliparib (Tage 1-7, q28) für bis zu 6 Zyklen
• Primärer Endpunkt: Gesamtüberleben (Overall Survival, OS)
• Sekundärer Endpunkt: Progressionsfreies Überleben (Progression-free survival, PFS)
2001: Randomized phase II/III trial of veliparib or placebo in combination with adjuvant temozolomide in newly diagnosed glioblastoma (GBM) patients
with MGMT promoter hypermethylation (Alliance A071102). Jann Nagina Sarkaria et al., New York, USAErgebnisse – Toxizität unter Veliparib 2001: Randomized phase II/III trial of veliparib or placebo in combination with adjuvant temozolomide in newly diagnosed glioblastoma (GBM) patients with MGMT promoter hypermethylation (Alliance A071102). Jann Nagina Sarkaria et al., New York, USA
Ergebnisse – Primärer Endpunkt Overall Survival
Kein Unterschied:
Overall Survival
(p = 0,15; HR 0,89 (0,71-1,11)
Medianes Overall Survival 28,1
vs. 24,8 Monate für
TMZ+Veliparib vs.
TMZ+Placebo)
Trend zu einem verlängerten
Overall Survival unter
TMZ+Veliparib zwischen 24 und
42 Monaten
(3-Jahres-OS 36,6 % vs. 28,9 %
unter TMZ+Placebo, p = 0,09).
2001: Randomized phase II/III trial of veliparib or placebo in combination with adjuvant temozolomide in newly diagnosed glioblastoma (GBM) patients
with MGMT promoter hypermethylation (Alliance A071102). Jann Nagina Sarkaria et al., New York, USA
TMZ - TemozolomidFazit
• Kein Unterschied in Hinblick auf primären Endpunkt Gesamtüberleben
• Überleben zu mittleren Zeitpunkten (24-42 Monate) länger mit
Temozolomid + Veliparib
• Temozolomid-Rechallange im Rezidiv in Verbindung mit
Temozolomid+Veliparib in Primärtherapie signifikant längeres
Gesamtüberleben (post hoc Analyse)
2001: Randomized phase II/III trial of veliparib or placebo in combination with adjuvant temozolomide in newly diagnosed glioblastoma (GBM) patients
with MGMT promoter hypermethylation (Alliance A071102). Jann Nagina Sarkaria et al., New York, USAPankreas: Neuroendokrine Neoplasien
Studie und Hintergrund 4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors: Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA Effektivität von Capecitabin und Temozolomid bei Patienten mit fortgeschrittenen neuroendokrinen Tumoren der Bauchspeicheldrüse und MGMT Status als prädiktiver Biomarker (finale Analyse) Hintergrund: Capecitabin könnte synergistisch mit Temozolomid wirken möglicherweise über die Downregulation des DNA Reparatur Enzyms MGMT
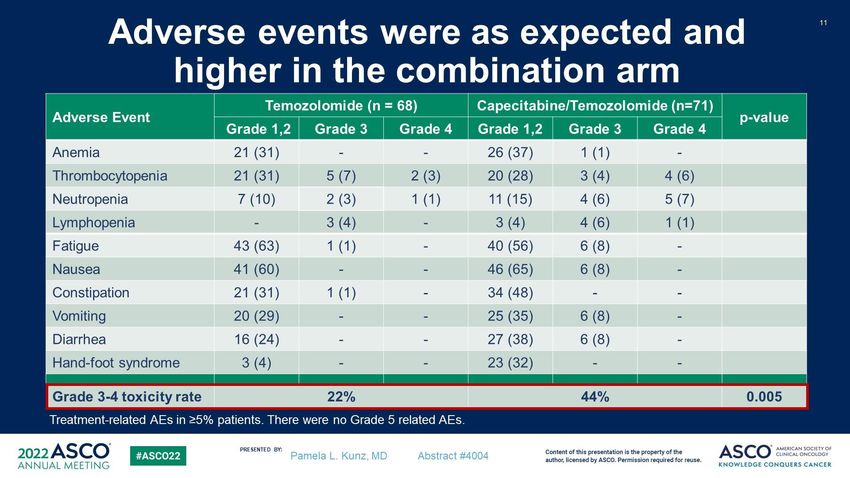
Fazit
• Capecitabin/Temozolomid zeigt eine signifikante Verbesserung des Pogressionsfreien
Überlebens im Vergleich zu Temozolomid allein (22,7 Monate vs. 14,4 Monate; HR 0,59, p =
0,022)
• Es gibt einen klinisch bedeutsamen Trend zur Verbesserung des Gesamtüberlebens (5 Monate
Unterschied), der jedoch keine statistische Signifikanz erreicht.
• Die Kombination aus Capecitabin und Temozolomid sollte als Standardtherapieoption für
Patienten mit fortgeschrittenen pankreatischen NETs aufgenommen werden und ist ein
verlässlicher Vergleichsarm in zukünftigen randomisierten Studien
• Ein MGMT-Defizienz ist signifikant mit dem Ansprechen auf Temozolomid verbunden, dies gilt
auch in Verbindung mit dem Progressions-freien Überleben und dem Gesamtüberleben
• MGMT könnte bei nueroendokrinen Tumoren des Pankreas ebenso prognostisch sein, wie beim
Glioblastom
• Routine-Testung auf MGMT wird derzeit nicht empfohlen
4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors:
Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.Anhang
Ergebnisse - Patientencharakteristika 4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors: Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.
Ergebnisse – Progressionfreies Überleben, Interimanalyse (2018)
Progressionsfreies
Überleben:
14,4 Monate
Temozolomid
versus
22,7 Monaten
Capecitabin/
Temozolomid
(HR = 0,58)
4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors:
Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.Ergebnisse – Progressionfreies Überleben, Interimanalyse
Medianes
Gesamtüberleben:
53,8 Monate
Temozolomid
Statistisch n.s.,
vs.
klinisch aber bedeutsam
58,7 Monate
Temozolomid/Cape.
(HR = 0.82, p = 0.42)
Ansprechrate:
34 % Temozolomid
vs.
40 %
Temozolomide/Cape.
(p = 0.59).
4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors:
Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.Ergebnisse – MGMT Defizienz und Ansprechen 4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors: Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.
Ergebnisse – MGMT Defizienz und Ansprechen 4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors: Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.
Ergebnisse – MGMT Defizienz und PFS und OS 4004: A Randomized Study of Temozolomide or Temozolomide and Capecitabine in Patients with Advanced Pancreatic Neuroendokrine Tumors: Final Analysis of Efficacy and Association with MGMT (ECOG-ACRIN E2211). Pamela L. Kunz et al., New Haven, Connecticut, USA.
You can also read