Bermuda Triangle for the liver: Alcohol, obesity, and viral hepatitis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
bs_bs_banner
doi:10.1111/jgh.12207
REVIEW
Bermuda Triangle for the liver: Alcohol, obesity, and
viral hepatitis
Samir Zakhari
Division of Metabolism and Health Effects, NIAAA, NIH, Bethesda, MD, USA
Abstract
Despite major progress in understanding and managing liver disease in the past 30 years,
it is now among the top 10 most common causes of death globally. Several risk factors,
such as genetics, diabetes, obesity, excessive alcohol consumption, viral infection, gender,
immune dysfunction, and medications, acting individually or in concert, are known to
precipitate liver damage. Viral hepatitis, excessive alcohol consumption, and obesity are
the major factors causing liver injury. Estimated numbers of hepatitis B virus (HBV) and
hepatitis C virus (HCV)-infected subjects worldwide are staggering (370 and 175 million,
respectively), and of the 40 million known human immunodeficiency virus positive sub-
jects, 4 and 5 million are coinfected with HBV and HCV, respectively. Alcohol and HCV
are the leading causes of end-stage liver disease worldwide and the most common indica-
tion for liver transplantation in the United States and Europe. In addition, the global obesity
epidemic that affects up to 40 million Americans, and 396 million worldwide, is accom-
panied by an alarming incidence of end-stage liver disease, a condition exacerbated by
alcohol. This article focuses on the interactions between alcohol, viral hepatitis, and
Key words obesity (euphemistically described here as the Bermuda Triangle of liver disease), and
Alcohol, viral hepatitis, liver, oxidative stress, discusses common mechanisms and synergy.
free radicals, CYP2E1.
Accepted for publication 25 April 2013.
Correspondence
Samir Zakhari, Division of Metabolism and
Health Effects, NIAAA, NIH, Bethesda, MD,
USA. Email: szakhari@mail.nih.gov
Organization, an estimated 2 billion people have been infected
The global burden with HBV, and more than 240 million have chronic liver infections
Liver cirrhosis and hepatocellular carcinoma (HCC) represent worldwide. About 600 000 people die every year from the acute or
end-stage liver disease (ESLD) and thus are associated with mor- chronic consequences of HBV infection, which is endemic in
tality. Globally, the incidence and prevalence of liver cirrhosis vary China and other parts of Asia, where most people become infected
markedly based largely on the causative factors. In the developed during childhood; 8–10% of the adult population is chronically
world, alcohol, hepatitis C virus (HCV), and nonalcoholic steato- infected. HBV-induced liver cancer is among the top three causes
hepatitis are the leading causes of cirrhosis, whereas viral hepatitis of death from cancer in men, and a major cause of cancer in
(especially hepatitis B virus [HBV]) is considered the leading women in this region. Globally, cirrhosis attributable to HBV or
cause in developing countries. Data from 2001 indicate that in HCV accounted for 30% and 27%, respectively, and HCC was
developed countries, cirrhosis was the sixth most common cause attributable to HBV (53%) or HCV (25%). Applied to 2002 world-
of death among adults, and in developing countries, it claimed wide mortality estimates, chronic HBV and HCV infections rep-
320 000 lives, ranking as the ninth most common cause of death. resent 929 000, including 446 000 cirrhosis deaths (HBV:
In the European Union alone, approximately 29 million individu- 235 000; HCV: 211 000) and 483 000 liver cancer deaths (HBV:
als suffer from chronic liver disease of whom 170 000 and 47 000 328 000; HCV: 155 000).3
die annually from cirrhosis and liver cancer, respectively.1 In the Nonalcoholic fatty liver disease (NAFLD) comprises a wide
United States, approximately 46 700 individuals died from liver spectrum of liver damage including steatosis, steatohepatitis,
cirrhosis and cancer in 2002.2 HBV and HCV infection are major fibrosis, and cirrhosis in patients who do not consume large
causes of morbidity and mortality. According to World Health amount of alcohol.4 NAFLD is a significant factor for serious liver
18 Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd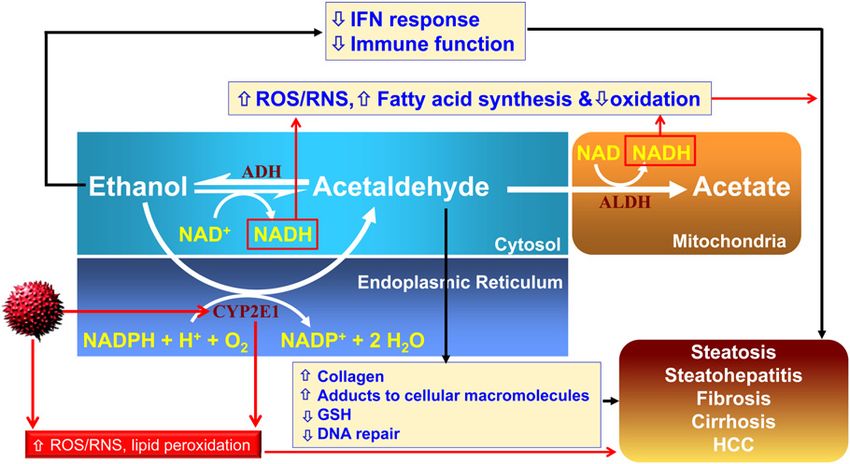
S Zakhari Bermuda Triangle for the liver
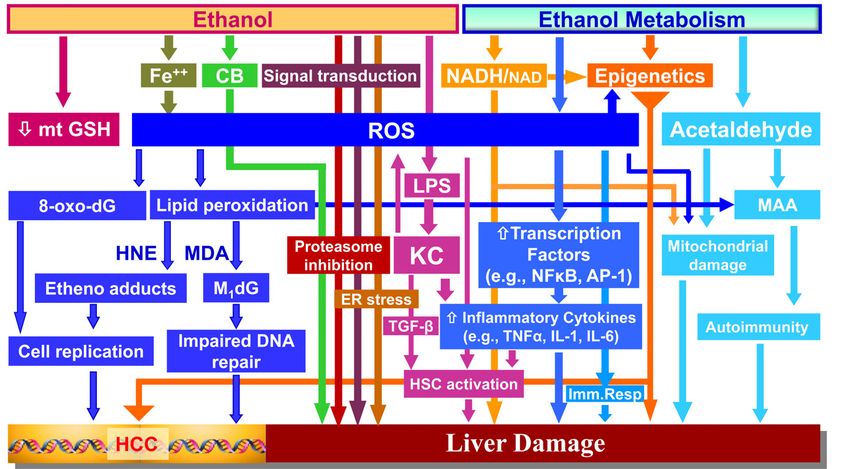
disease because of its rising prevalence in the general population,5 Mechanisms of ALD. Various mechanisms have been iden-
and the potential to progress to ESLD and HCC.6 NAFLD com- tified for ALD (Fig. 1) which are involved at various stages of
monly occurs in patients with obesity, diabetes, and hyperlipi- progression.
demia. In the past two decades, obesity in North America has more
than doubled and continues to rise worldwide. In 2005, 8% of men
and 12% of women were obese. By 2030, the number of obese Fatty liver. Both intrahepatic and extrahepatic mechanisms are
adults globally is projected to be 573 million individuals.7 involved in hepatic steatosis:
The combination of chronic heavy alcohol consumption, viral
a) Intrahepatic factors
hepatitis infection, and obesity represent a major assault on liver’s
health worldwide. Hepatic steatosis due to heavy alcohol consumption has been
attributed to a metabolic stress imposed by the fact that the liver is
the predominant site of ethanol metabolism. Possible mechanisms
include: (i) suppression of mitochondrial fatty acid b-oxidation;
Alcoholic liver disease (ALD) (ii) a limitation in the permeability of the outer mitochondrial
Chronic alcohol consumption results in liver disease which varies membrane pore protein voltage-dependent anion-selective chan-
extensively between individuals in severity and progression nel;10 (iii) enhancement of hepatic uptake of free fatty acids from
for comparable levels of alcohol consumption. This variability the circulation; (iv) increase in de novo synthesis of fatty acids and
could be attributed to variations in the expression and activity triglycerides; and (v) derailment of lipoprotein synthesis and
of individual isoforms of the alcohol-metabolizing enzymes: secretion.
alcohol dehydrogenase (ADH) and aldehyde dehydrogenase Chronic alcohol consumption induces a marked increase in
(ALDH), but is also influenced by variations in patterns of cytochrome P450 2E1 (CYP2E1) activity, with a resultant
alcohol intake (binge vs chronic drinking), nutritional status, increased demand for nicotinamide adenine dinucleotide phos-
gender, smoking, or abuse of other drugs. In addition, the onset phate (NADPH), an increased rate of formation of reactive oxygen
and severity of ALD is strongly influenced by other comorbid species (ROS), and a decrease in oxidative stress defense capacity.
conditions such as obesity or HCV infection. This increase At the same time, impairment of mitochondrial respiratory capac-
in susceptibility to ALD is not due solely to intrahepatic factors, ity caused by defects in the electron transport and ATP synthase
but may also involve alcohol-induced changes in other tissues, complexes results in further increase in ROS formation at the
such as adipose tissue, central nervous system, the gut, and the mitochondrial level.11 The ethanol-induced stress is further exac-
immune system. Factors contributing to alcohol-induced liver erbated by defects in the methionine cycle, resulting in a decrease
disease are thus complex and systemic.8 The spectrum of ALD in glutathione (GSH) synthesis, which contributes to the decline in
includes: oxidative stress defenses. Importantly, these conditions also reflect
an increase in endoplasmic reticulum (ER) stress, a common
1 Fatty liver (hepatic steatosis), characterized histologically by
response do the accumulation of defective proteins.12 The resulting
lipid droplets in hepatocytes. This condition is usually reversible
accumulation of stress conditions in hepatocytes causes an
upon cessation of alcohol consumption, and thus is thought to
increased susceptibility to cell death signals. Accompanying the
be a relatively innocuous side effect of heavy drinking.
structural and functional changes in subcellular organelles,
However, hepatic steatosis often develops in obesity, metabolic
chronic ethanol treatment results in significant changes in the
syndrome, and type 2 diabetes, clinical conditions that involve
profile of transcription factors that regulate lipid homeostasis in
significant metabolic defects. Thus, fatty liver by itself reflects a
the liver. Ethanol consumption elicits a decrease in peroxisome
condition of metabolic stress that is a risk factor for the devel-
proliferator-activated receptor (PPAR)-a activity, thereby sup-
opment of more severe forms of liver disease.
pressing the catabolic lipid metabolic pathways, including peroxi-
2 Alcoholic hepatitis, an inflammatory condition characterized by
somal and mitochondrial fatty acid oxidation. At the same time,
significantly increased serum levels of liver enzymes (alanine
ethanol increases the activity of sterol regulatory element-binding
aminotranferease and aspartate aminotransferase) and moderate
protein (SREBP)-1c and SREBP-2, which enhances lipid synthetic
to severe tissue damage, including necrotic foci with neutrophil
pathways. In addition, there has been some evidence that the
infiltration. Acute alcoholic hepatitis is a potentially fatal
adenosine monophosphate (AMP)-activated protein kinase
disease that develops in a significant fraction (30–40%) of
(AMPK) is inhibited by ethanol. However, it is difficult to distin-
chronic heavy drinkers.
guish direct and indirect effects of ethanol. For instance, AMPK
3 Liver fibrosis/cirrhosis, about 10–15% of chronic heavy drink-
activity in the liver is regulated not only by the availability of AMP
ers proceed to develop fibrosis and cirrhosis.
in the cell, but also responds to extracellular signals, including the
4 HCCs occur in about 2% of cirrhotic patients.
adipose tissue derived cytokine adiponectin.
Although factors that facilitate the development of hepatitis and A related regulatory pathway affected by ethanol may involve
cirrhosis are not well characterized, impairment in the cellular the deacetylase silent information regulator-1 (SIRT-1), which
stress defense mechanisms, (e.g. oxidative stress),9 or derailment requires activation by nicotinamide adenine dinucleotide (NAD+).
of the balance of autocrine or paracrine mediators that are critical Thus, the change in NAD redox state in the liver during ethanol
in maintaining normal homeostatic conditions are documented. In oxidation may facilitate inhibition of SIRT-1. It has been reported
addition, chronic alcohol consumption interferes with liver regen- that SIRT-1 activity in the liver of mice is decreased after ethanol
eration, which under normal conditions is a highly effective repair treatment.13 Among the targets of SIRT-1 are several key regulators
mechanism that avoids scar tissue formation. of lipid metabolism, including the transcriptional coregulators
Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25 19
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd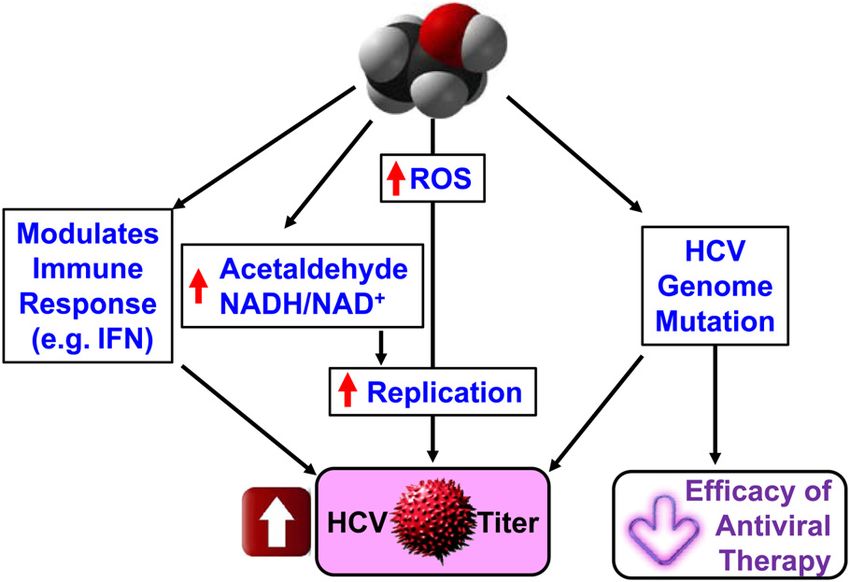
Bermuda Triangle for the liver S Zakhari
Figure 1 Known mechanisms of alcoholic liver damage. CB, cannabinoid receptor; ER, endoplasmic reticulum; Fe, Ferrous molecule; HCC,
hepatocellular carcinoma; HNE, 4-hydroxynonenal; HSC, hepatic stellate cell; KC, Kupffer cells; LPS, lipopolysaccharide; MAA, malondialdehyde-
acetaldehyde adduct; MDA, malondialdehyde; Mt GSH, mitochondrial glutathione; NAD, nicotinamide adenine dinucleotide; NADH, reduced NAD;
ROS, reactive oxygen species; TGF, transforming growth factor.
peroxisome proliferator-activated receptor gamma coactivator Whether circulating adiponectin levels are similarly correlated
1-alpha (PGC-1a). Its deacetylation by SIRT-1 allows it to stimu- with liver damage in human alcoholics remains unclear.15
late gene expression through its interactions with PPAR-a. Fur- Insulin plays a dominant role in integrating fatty acid and car-
thermore, SREBP-1c is a target for SIRT-1 and its acetylation state bohydrate metabolism in the liver with the energetic needs of
may affect its transcriptional activity. other tissues. Nonalcoholic hepatic steatosis that occurs in the
metabolic syndrome and type II diabetes is commonly associated
b) Extrahepatic factors
with insulin resistance, that is, a decreased capacity to respond
Lipid metabolism in the liver is integrated with a variety of to changes in circulating insulin, in multiple tissues including
signals, including circulating hormones, cytokines, nutrition, and liver and muscle. There is strong evidence that stress responses
other factors that impinge on the intrahepatic processes leading to mediated by free fatty acid accumulation or ER stress result
steatosis. While some of these factors are intrahepatic (e.g. cytok- in activation of stress response protein kinases, including
ines released from Kupffer cells, endothelial cells, or stellate protein kinase C and Jun-N-terminal kinase, which affect the
cells), others are dispatched by remote tissues. Of particular rel- intracellular signaling pathways through which insulin exerts
evance are hormones (e.g. insulin), adiponectin and leptin its effects.
(secreted from adipose tissue), and stress hormones and satiety
factors that act through the hypothalamus or other brain structures Alcoholic hepatitis. As described earlier, hepatic steatosis repre-
to regulate food intake. Chronic ethanol consumption has a notable sents a severe condition of increased oxidative stress, ER, and
impact on the synthesis and secretion of several of these factors, in metabolic stress. However, the mechanisms by which such stress
addition to affecting their capacity to impact lipid metabolic path- conditions can lead to a more severe inflammatory condition
ways in the liver. remain only partly understood. Increased cell death (by necrosis or
Adiponectin, one of the adipokines secreted by adipose tissue to apoptosis) sets in motion further pro-inflammatory responses in
regulate lipid homeostasis, acts on multiple tissues including the the liver by producing cytokines and chemokines that help mobi-
liver to sensitize the response to insulin and enhance fatty acid lize neutrophils and other inflammatory cells that further enhance
oxidation. In animal experiments, ethanol feeding tends to sup- liver damage. Also, it appears that overproduction of ROS by the
press adiponectin secretion from adipose tissue. However, the damaged mitochondria could play a salient role. Factors that may
effects of ethanol on adiponectin levels may depend on dietary be involved in the precipitation of alcoholic hepatitis are briefly
factors such as the content of saturated and unsaturated fat.14 discussed later.
20 Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd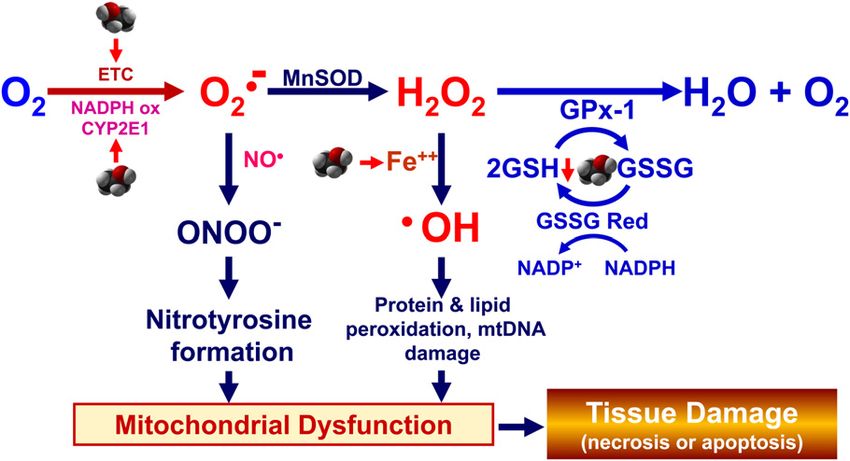
S Zakhari Bermuda Triangle for the liver
Figure 2 Hepatitis C virus (HCV), alcohol
metabolism, and liver damage. ALD, alcohol
dehydrogenase; ALDH, aldehyde dehydroge-
nase; GSH, glutathione; HCC, hepatocellular
carcinoma; IFN, interferon; NAD, nicotina-
mide adenine dinucleotide; NADH, reduced
NAD; NADP, nicotinamide adenine dinucle-
otide phosphate; RNS, reactive nitrogen
species; ROS, reactive oxygen species.
Oxidative alcohol metabolism in the liver. Only tion, acetaldehyde and malondialdehyde (a by-product of lipid
about 2–10% of the absorbed alcohol is eliminated via the lungs peroxidation) can combine and react with lysine residues on
and kidneys; the remaining 90% is metabolized mainly by oxida- proteins, giving rise to stable malondialdehyde-acetaldehyde-
tive pathways in the liver and by nonoxidative pathways in extra- protein adducts that are immunogenic and, thus, can contribute
hepatic tissues. Oxidative metabolism in the liver results in to immune-mediated liver damage.
extensive displacement of the liver’s normal metabolic substrates, b) Change in hepatocyte redox state (increase in NADH/NAD+
the production of acetaldehyde and ROS, and an increase in the ratio): both acute and chronic alcohol consumption shift the
NADH/NAD+ ratio (Fig. 2). redox state of the liver to a more reduced level,16,17 similar to
The major pathway of oxidative metabolism of ethanol in the but more pronounced than the shift observed in diabetes and
liver involves multiple isoforms of cytosolic ADH, which results in during starvation. Alcohol metabolism produces a significant
the production of acetaldehyde. Accumulation of this highly reac- increase in the hepatic NADH/NAD+ ratio in both the cytosol
tive and toxic molecule contributes to liver damage. The oxidation and the mitochondria, as evidenced by an increase in the
of ethanol is accompanied by the reduction of NAD+ to NADH lactate/pyruvate and b-hydroxybutyrate/acetoacetate ratios,
and, thereby, generates a highly reduced cytosolic environment in respectively,18 and vastly increases the availability of oxidiz-
hepatocytes. The cytochrome P450 isozymes, including CYP2E1, able NADH to the ETC in the mitochondria. The liver responds
1A2, and 3A4, which are predominantly localized to the ER, also to ethanol exposure in part by increasing the rate of oxygen
contribute to ethanol’s oxidation to acetaldehyde in the liver. uptake, which may lead to periods of hypoxia, particularly in
CYP2E1 is induced by chronic ethanol consumption and assumes the downstream (pericentral) parts of the liver lobule.
an important role in metabolizing ethanol to acetaldehyde at c) Formation of ROS, reactive nitrogen species (RNS), and oxi-
elevated alcohol concentration. It also produces ROS, including dative stress: Hepatic mitochondria produce ROS through the
hydroxyethyl, superoxide anion, and hydroxyl radicals. activity of the ETC as a by-product of oxidative phosphoryla-
Acetaldehyde, produced by ethanol oxidation, is rapidly metabo- tion. Normally, a small fraction of electrons entering the ETC
lized mainly by mitochondrial ALDH2 to form acetate and NADH. can prematurely escape from complexes I and III and directly
Mitochondrial NADH is reoxidized by the electron transport chain react with 1–3% of respiratory oxygen molecules to generate
(ETC). Most of the acetate resulting from ethanol metabolism the superoxide anion radical, which is then dismutated by the
escapes the liver to the blood and is eventually metabolized to CO2 mitochondrial manganese superoxide dismutase into hydrogen
by way of the tricarboxylic acid cycle in tissues such as heart, peroxide (H2O2). Mitochondrial glutathione peroxidase (GPx)
skeletal muscle, and brain, where mitochondria are capable of then converts H2O2 into water by using reduced glutathione
converting acetate to the intermediate acetyl coenzyme A. (GSH) as a cofactor. Thus, most of the ROS generated by the
ETC in the normal state are detoxified by the mitochondrial
antioxidant defenses. The nondetoxified portion of ROS dif-
Consequences of alcohol metabolism by
fuses out of mitochondria, and affects signal transduction path-
oxidative pathways.
ways and gene expression, triggering cytokines, hormones, and
a) Acetaldehyde generation/adduct formation: if accumulated to growth factors, which if excessive may lead to hepatic inflam-
high concentrations, acetaldehyde can form adducts with DNA mation, necrosis, and/or apoptosis. In addition, metals (e.g.
and RNA, and decrease DNA repair. It also has the capacity to iron and copper) can further react with H2O2 to produce
react with lysine residues on proteins including enzymes, hydroxyl radicals via the Fenton reaction (Fig. 3).
microsomal proteins, microtubules, and affect their function.
Formation of protein adducts in hepatocytes may contribute to Nitric oxide (NO), an RNS critical for hepatocyte biology, can
impaired protein secretion, resulting in hepatomegaly. In addi- interact with peroxides to generate peroxynitrite, which could be
Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25 21
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd
Bermuda Triangle for the liver S Zakhari
Figure 3 Alcohol, reactive oxygen species
(ROS), and mitochondrial dysfunction.
CYP2E1, cytochrome P450 2E1; GSH, glu-
tathione; GSSG, oxidized glutathione; H2O2,
hydrogen peroxide; MnSOD, manganese
superoxide dismutase; NO•, nitric oxide;
O2•–, speroxide; •OH, hydroxyl radical;
ONOO–, peroxinitrite.
detrimental to the liver depending on the amount and duration. NO HSCs and collagen formation (studies on isolated HSCs have
is produced by inducible nitric oxide synthase which is expressed demonstrated that ethanol alters their response to transforming
in all liver cells (i.e. hepatocytes, stellate cells, Kupffer cells, and growth factor (TGF-b) and IFN-g through effects on intracellular
vascular endothelial cells) and its expression is induced by inter- signaling pathways); and (iv) suppression of the regenerative
leukin (IL)-1b alone or in combination with tumor necrosis factor response to tissue damage that is an essential component of the
(TNF)-a, interferon (IFN)-g, and/or lipopolysaccharide (LPS). liver’s repair mechanism and thereby facilitates the deposition of
Ethanol-induced oxidative stress has been attributed to a scar tissue, which is the hallmark of fibrosis. This is probably
decrease in the NAD+ : NADH ratio, acetaldehyde formation, accompanied by a suppression of metalloproteases (e.g. by the
CYP2E1 induction, hypoxia, cytokine signaling, mitochondrial activation of inhibitor proteins, such as plasminogen activator
damage, LPS activation of Kupffer cells, reduction in antioxidants inhibitor-1 [PAI-1]), which normally would maintain the balance
particularly mitochondrial and cytosolic GSH, one electron oxida- of ECM deposition and resolution to facilitate tissue repair.21
tion of ethanol to 1-hydroxy ethyl radical, and the conversion of
xanthine dehydrogenase to xanthine oxidase.
Common factors involved in alcohol,
obesity, and viral infection
Fibrosis and cirrhosis Chronic heavy alcohol consumption, obesity, and viral infection
Fibrosis is a common response of the liver to a chronic inflamma- have some common features/mechanisms that may contribute to
tory condition, where hepatic stellate cells (HSC) play a critical exacerbation of liver damage when these conditions coexist.
(though not exclusive) role.19 HSCs exist in a quiescent state in the Several common mechanisms between two or more of these con-
normal liver, but can be activated directly or indirectly in response ditions have been advocated, including oxidative stress, CYP2E1
to apoptotic or necrotic cell death. Cytokines released in the tissue induction, increased fat synthesis and mobilization, selected gut
as a result of injury further contribute to HSC activation, resulting bacteria, free fatty acids, ER stress, immune response, among
in the expression of a myofibroblast phenotype and stimulating the others.22–25 Because of page limitations, only the first two mecha-
expression of extracellular matrix (ECM) proteins, in particular nisms (oxidative stress and CYP2E1 induction) will be discussed.
collagen type 1, which are not normally expressed in the liver. Oxidative stress due to alcohol has been discussed earlier.
Under conditions of an acute tissue injury, the deposition of
collagen fibers is a transient wound-healing response and is
followed by fibrinolysis mediated by metalloproteases that are
Obesity and oxidative stress
activated as damaged tissue is replaced by newly generated liver Obesity involves the accumulation of body fat and is a major risk
cells by the regenerative response. Continuous tissue damage and factor for metabolic syndrome, which is characterized by hyperg-
repair after chronic inflammation, and an imbalance in the normal lycemia, dyslipidemia, and hypertension.26 Increased oxidative
liver repair mechanisms results in excessive deposition of collagen stress in accumulated fat has been reported as a pathogenic mecha-
fibers.19 nism of obesity-associated metabolic syndrome. In nondiabetic
Chronic ethanol consumption can influence this process at mul- humans, systemic oxidative stress correlated positively with fat
tiple levels: (i) enhancement of the pro-inflammatory environment accumulation and negatively with plasma adiponectin levels. In
in the liver by stimulating the release of pro-inflammatory cytok- obese mice, ROS production was selectively increased in adipose
ines from macrophages and decreasing the activity of protective tissue, and was accompanied by enhanced expression of NADPH
cell types, including natural killer cells;20 (ii) enhancement of oxidase and decreased expression of anti-oxidative enzymes such
hepatocyte apoptosis and necrosis in response to oxidative stress as superoxide dismutase in white adipose tissue and GPx in liver.27
and shifting in stress defense signaling pathways; (iii) activation of In cultured adipocytes, mitochondrial and peroxisomal oxidation
22 Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty LtdS Zakhari Bermuda Triangle for the liver
of fatty acids activates NADPH oxidase resulting in increased increased in patients with nonalcoholic steatohepatitis, chronic
oxidative stress, which caused increase in messenger RNA alcoholism, or morbid obesity. To study the correlation between
(mRNA) expression of inflammatory (PAI-1, TNF-a, IL-6, and obesity and CYP2E1, Emery et al.40 assessed hepatic CYP2E1
monocyte chemotactic protein-1), and suppression of mRNA and activity—by determining the clearance of chlorzoxazone (CLZ),
secretion of anti-inflammatory (adiponectin, leptin) adipocytok- a CYP2E1-selective probe—in morbidly obese subjects with
ines. Conversely, in obese KKAy mice, treatment with apocynin, varying degrees of hepatic steatosis, and normal-weight controls.
an NADPH oxidase inhibitor, reduced ROS production in adipose Obese subjects were evaluated at baseline and 1 year after gastro-
tissue, increased plasma adiponectin levels, and improved hyper- plasty, a procedure that leads to weight loss. Compared with con-
lipidemia and hepatic steatosis. Because oxidative stress underlies trols, oral CLZ clearance was elevated approximately threefold in
the pathophysiology of hepatic steatosis,28 these results suggest morbidly obese subjects, and was significantly higher among sub-
that increased oxidative stress in obese individuals could be further jects with steatosis involving > 50% of hepatocytes. One year after
exacerbated by oxidative stress due to chronic heavy alcohol gastroplasty, the median body mass index decreased by 33%, and
consumption. total oral CLZ clearance declined by 46%. Thus, hepatic CYP2E1
activity is upregulated in morbidly obese subjects, and the positive
association between the degree of steatosis and CYP2E1 activity
Viral infection and oxidative stress preoperatively suggests that CYP2E1 induction is related to
Infection with HCV, in most cases, develops into chronic disease morbid obesity.40 Similar results were obtained in genetically
which is manifested by steatosis and fibrosis, as well as HCC. obese Zucker rats fed a normal diet (OB) when compared with
HCV replication induces oxidative stress (Figure 2), which con- normal Zucker rats fed a high-fat diet (HF). CYP2E1 induction
tributes to insulin and interferon resistance, as well as disorders was greater in both liver and fat of OB rats than in those of HF rats.
of iron metabolism. Specifically, virus core and nonstructural The induction of CYP2E1 in liver and fat of obese patients may
NS5A proteins increase ROS levels through alteration of calcium potentially alter the pharmacokinetics of lipophilic drugs metabo-
homeostasis29 via a primary effect on the uniporter,30 and the lized by CYP2E1.41
induction of NADPH oxidase 4.31 In addition, E1 and E2 and the In a recent study, Cederbaum reported that CYP2E1 induction
transmembrane protein NS4B increase ROS generation via potentiated liver injury in obese mice, and the elevated oxidative
ER stress and unfolded protein response,32,33 and activates the stress could be blunted by CYP2E1 inhibitors.38 In addition,
antioxidant defense regulated by NF-E2-related factor 2.34 S-Adenosyl-L-methionine decreased oxidative stress, steatosis,
Furthermore, HCV causes mitochondrial damage and induction liver injury, and mitochondrial dysfunction in the pyrazole-treated
of double-stranded DNA breaks mediated by NO and ROS, obese mice, an important finding with therapeutic implications in
which is abolished by NO and ROS inhibitors.35 HCV-induced obesity-induced metabolic complications.
ROS causes hepatic iron accumulation in mice by reducing
hepcidin transcription, further magnifying ROS production,36 and
regulating TGF-b1.37
CYP2E1, HCV, and oxidative stress
CYP2E1 expression in the liver of patients with chronic hepatitis
C correlated with the progression of hepatic disease (both lobular
CYP2E1, alcohol, and oxidative stress inflammation and fibrosis indices), and observed variations were
As mentioned earlier, alcohol-induced oxidative stress is a major consistent with the preferential distribution of CYP2E1 in the
mechanism by which ethanol causes liver injury. Of the many lobular zone.42 The effect of alcohol metabolism on HCV replica-
suggested pathways by which ethanol induces a state of oxidative tion and the antiviral action of IFN was studied in Huh-7 cells that
stress, induction of CYP2E1 is a central one. Levels of CYP2E1 harbor HCV replication and metabolize ethanol via the introduced
are increased after acute and chronic alcohol treatment. CYP2E1 expression of CYP2E1. Alcohol (up to 100 mmol/L) significantly
generates ROS such as the superoxide anion radical and hydrogen increased HCV replication, which was dependent on CYP2E1
peroxide and, in the presence of iron catalysts, produces the expression and alcohol-induced oxidative stress, and attenuated
hydroxyl radical, a powerful oxidant (Figure 3). The role of the anti-HCV action of IFN.43 In chronic hepatitis C patients,
CYP2E1 in chronic ethanol-induced liver injury was studied in cross-reactivity between CYP2E1 and specific sequences in HCV-
wild-type (WT) mice, CYP2E1 knockout (KO) mice and human- NS5b protein can promote the development of auto-antibodies
ized CYP2E1 knockin (KI) mice. Alcohol produced oxidant stress targeting conformational epitopes on the CYP2E1 surface that
and steatosis in WT mice, but these effects were blunted in the KO might contribute to hepatic injury.44
mice and restored in the KI mice. These studies show that CYP2E1 Alcohol’s elevation of HCV titer in patients and increase of
contributes to ethanol-induced oxidant stress and liver injury.38 HCV RNA in replicon cells suggest that HCV replication is
For a discussion of the biochemical and toxicological properties increased in the presence and absence of the complete viral repli-
of CYP2E1 and possible therapeutic implications for treatment of cation cycle. Seronello et al.45 used Huh7 human hepatoma cells
ALD by CYP2E1 inhibitors, the reader is referred to the review that naturally express comparable levels of CYP2E1 as human
article by Lu and Cederbaum.39 liver to demonstrate that ethanol, at physiologically relevant con-
centrations, enhances complete HCV replication. Acetaldehyde,
the first metabolite of ethanol, also enhanced HCV replication.
CYP2E1, obesity, and oxidative stress They reported that elevated NADH/NAD+ is required for the
As discussed earlier, CYP2E1 is an important factor in liver potentiation of HCV replication by ethanol, and inhibiting
disease. Several studies suggest that hepatic CYP2E1 activity is CYP2E1 or ALDH suppressed replication. Thus, alteration of
Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25 23
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty LtdBermuda Triangle for the liver S Zakhari
Figure 4 Summary of alcohol and HCV
interactions. HCV, hepatitis C virus; IFN,
interferon; ROS, reactive oxygen species.
cellular NADH/NAD ratio is likely to play a critical role in the 6 Bugianesi E. Non-alcoholic steatohepatitis and cancer. Clin. Liver
potentiation of HCV replication by ethanol (Fig. 4). Dis. 2007; 11: 191–207, x–xi.
7 Kelly T, Yang W, Chen CS, Reynolds K, He J. Global burden of
obesity in 2005 and projections to 2030. Int. J. Obes. (Lond) 2008;
Concluding remarks 32: 1431–7.
8 Gao B, Bataller R. Alcoholic liver disease: pathogenesis and new
Chronic heavy alcohol consumption in the presence of obesity and therapeutic targets. Gastroenterology 2011; 141: 1572–85.
viral hepatitis could be damaging for the liver. While moderate 9 Fernandez-Checa JC, Kaplowitz N. Hepatic mitochondrial
alcohol consumption was associated with decreased prevalence of glutathione: transport and role in disease and toxicity. Toxicol. Appl.
steatohepatitis in patients with NAFLD,46 heavy alcohol consump- Pharmacol. 2005; 204: 263–73.
tion is discouraged whether an individual has NAFLD or not. The 10 Holmuhamedov E, Lemasters JJ. Ethanol exposure decreases
presence of common mechanisms for liver damage due to viruses, mitochondrial outer membrane permeability in cultured rat
obesity, or chronic heavy alcohol consumption is relevant and hepatocytes. Arch. Biochem. Biophys. 2009; 481: 226–33.
11 Hoek JB, Cahill A, Pastorino JG. Alcohol and mitochondria:
may exacerbate damage to the liver when these three conditions
a dysfunctional relationship. Gastroenterology 2002; 122:
exist. Further research is needed to clarify the interaction, if any, 2049–63.
between moderate drinking, NAFLD, and viral hepatitis. 12 Kaplowitz N, Than TA, Shinohara M, Ji C. Endoplasmic reticulum
stress and liver injury. Semin. Liver Dis. 2007; 27: 367–77.
13 You M, Liang X, Ajmo JM, Ness GC. Involvement of mammalian
Conflict of interests sirtuin 1 in the action of ethanol in the liver. Am. J. Physiol.
The author does not have any conflicting interests to declare. Gastrointest. Liver Physiol. 2008; 294: G892–8.
14 You M, Considine RV, Leone TC, Kelly DP, Crabb DW. Role of
adiponectin in the protective action of dietary saturated fat against
References alcoholic fatty liver in mice. Hepatology 2005; 42: 568–77.
15 Adachi M, Ishii H. Hyperadiponectinemia in alcoholic liver disease:
1 Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, friend or foe? J. Gastroenterol. Hepatol. 2009; 24: 507–8.
Roudot-Thoraval F. The burden of liver disease in Europe: a review 16 Smith ME, Newman HW. The rate of ethanol metabolism in fed and
of available epidemiological data. J. Hepatol. 2013; 58: 593–608. fasting animals. J. Biol. Chem. 1959; 234: 1544–9.
2 Lim YS, Kim WR. The global impact of hepatic fibrosis and 17 Rawat AK. Effects of ethanol infusion on the redox state and
end-stage liver disease. Clin. Liver Dis. 2008; 12: 733–46, vii. metabolite levels in rat liver in vivo. Eur. J. Biochem. 1968; 6:
3 Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The 585–92.
contributions of hepatitis B virus and hepatitis C virus infections to 18 Cunningham CC, Bailey SM. Ethanol consumption and liver
cirrhosis and primary liver cancer worldwide. J. Hepatol. 2006; 45: mitochondria function. Biol. Signals Recept. 2001; 10: 271–82.
529–38. 19 Friedman SL. Mechanisms of hepatic fibrogenesis. Gastroenterology
4 Sanyal AJ. AGA technical review on nonalcoholic fatty liver disease. 2008; 134: 1655–69.
Gastroenterology 2002; 123: 1705–25. 20 Jeong WI, Park O, Gao B. Abrogation of the antifibrotic effects
5 Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic of natural killer cells/interferon-gamma contributes to alcohol
syndrome among US adults: findings from the third National Health acceleration of liver fibrosis. Gastroenterology 2008; 134:
and Nutrition Examination Survey. JAMA 2002; 287: 356–9. 248–58.
24 Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty LtdS Zakhari Bermuda Triangle for the liver 21 Arteel GE. New role of plasminogen activator inhibitor-1 in and independent mechanisms in HUH7 cells. PLoS ONE 2011; 6: alcohol-induced liver injury. J. Gastroenterol. Hepatol. 2008; 23 e24957. (Suppl. 1): S54–9. 35 Machida K, Cheng KT, Sung VM et al. Hepatitis C virus induces 22 Volynets V, Kuper MA, Strahl S et al. Nutrition, intestinal toll-like receptor 4 expression, leading to enhanced production of permeability, and blood ethanol levels are altered in patients with beta interferon and interleukin-6. J. Virol. 2006; 80: 866–74. nonalcoholic fatty liver disease (NAFLD). Dig. Dis. Sci. 2012; 57: 36 Nishina S, Hino K, Korenaga M et al. Hepatitis C virus-induced 1932–41. reactive oxygen species raise hepatic iron level in mice by 23 Sakaguchi S, Takahashi S, Sasaki T, Kumagai T, Nagata K. reducing hepcidin transcription. Gastroenterology 2008; 134: Progression of alcoholic and non-alcoholic steatohepatitis: common 226–38. metabolic aspects of innate immune system and oxidative stress. 37 Lin W, Tsai WL, Shao RX et al. Hepatitis C virus regulates Drug Metab. Pharmacokinet. 2011; 26: 30–46. transforming growth factor beta1 production through the generation 24 Choi J, Ou JH. Mechanisms of liver injury. III. Oxidative stress in of reactive oxygen species in a nuclear factor kappaB-dependent the pathogenesis of hepatitis C virus. Am. J. Physiol. Gastrointest. manner. Gastroenterology 2010; 138: 2509–18, 2518 e1. Liver Physiol. 2006; 290: G847–51. 38 Cederbaum AI. CYP2E1 potentiates toxicity in obesity and after 25 Malhi H, Kaufman RJ. Endoplasmic reticulum stress in liver disease. chronic ethanol treatment. Drug Metabol. Drug Interact. 2012; 27: J. Hepatol. 2011; 54: 795–809. 125–44. 26 Spiegelman BM, Flier JS. Obesity and the regulation of energy 39 Lu Y, Cederbaum AI. CYP2E1 and oxidative liver injury by alcohol. balance. Cell 2001; 104: 531–43. Free Radic. Biol. Med. 2008; 44: 723–38. 27 Furukawa S, Fujita T, Shimabukuro M et al. Increased oxidative 40 Emery MG, Fisher JM, Chien JY et al. CYP2E1 activity before and stress in obesity and its impact on metabolic syndrome. J. Clin. after weight loss in morbidly obese subjects with nonalcoholic fatty Invest. 2004; 114: 1752–61. liver disease. Hepatology 2003; 38: 428–35. 28 Roskams T, Yang SQ, Koteish A et al. Oxidative stress and oval cell 41 Khemawoot P, Yokogawa K, Shimada T, Miyamoto K. accumulation in mice and humans with alcoholic and nonalcoholic Obesity-induced increase of CYP2E1 activity and its effect on fatty liver disease. Am. J. Pathol. 2003; 163: 1301–11. disposition kinetics of chlorzoxazone in Zucker rats. Biochem. 29 Okuda M, Li K, Beard MR et al. Mitochondrial injury, oxidative Pharmacol. 2007; 73: 155–62. stress, and antioxidant gene expression are induced by hepatitis C 42 Haufroid V, Ligocka D, Buysschaert M, Horsmans Y, Lison D. virus core protein. Gastroenterology 2002; 122: 366–75. Cytochrome P4502E1 (CYP2E1) expression in peripheral blood 30 Li Y, Boehning DF, Qian T, Popov VL, Weinman SA. Hepatitis C lymphocytes: evaluation in hepatitis C and diabetes. Eur. J. Clin. virus core protein increases mitochondrial ROS production by Pharmacol. 2003; 59: 29–33. stimulation of Ca2+ uniporter activity. FASEB J. 2007; 21: 2474–85. 43 McCartney EM, Semendric L, Helbig KJ et al. Alcohol metabolism 31 de Mochel NS, Seronello S, Wang SH et al. Hepatocyte NAD(P)H increases the replication of hepatitis C virus and attenuates oxidases as an endogenous source of reactive oxygen species during the antiviral action of interferon. J. Infect. Dis. 2008; 198: hepatitis C virus infection. Hepatology 2010; 52: 47–59. 1766–75. 32 Chan SW, Egan PA. Hepatitis C virus envelope proteins regulate 44 Sutti S, Vidali M, Mombello C et al. Breaking self-tolerance toward CHOP via induction of the unfolded protein response. FASEB J. cytochrome P4502E1 (CYP2E1) in chronic hepatitis C: possible role 2005; 19: 1510–12. for molecular mimicry. J. Hepatol. 2010; 53: 431–8. 33 Santos CX, Tanaka LY, Wosniak J, Laurindo FR. Mechanisms and 45 Seronello S, Ito C, Wakita T, Choi J. Ethanol enhances hepatitis C implications of reactive oxygen species generation during the virus replication through lipid metabolism and elevated unfolded protein response: roles of endoplasmic reticulum NADH/NAD+. J. Biol. Chem. 2010; 285: 845–54. oxidoreductases, mitochondrial electron transport, and NADPH 46 Dunn W, Sanyal AJ, Brunt EM et al. Modest alcohol consumption is oxidase. Antioxid. Redox Signal. 2009; 11: 2409–27. associated with decreased prevalence of steatohepatitis in patients 34 Ivanov AV, Smirnova OA, Ivanova ON et al. Hepatitis C virus with non-alcoholic fatty liver disease (NAFLD). J. Hepatol. 2012; proteins activate NRF2/ARE pathway by distinct ROS-dependent 57: 384–91. Journal of Gastroenterology and Hepatology 2013; 28 (Suppl. 1): 18–25 25 © 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd
You can also read

















































