Cardiovascular Risk Factors in Patients with Type 2 Diabetes in Germany
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MEDICINE
ORIGINAL ARTICLE
Cardiovascular Risk Factors
in Patients with Type 2 Diabetes
in Germany
Heiner K. Berthold, Ioanna Gouni-Berthold, Kurt Bestehorn,
Michael Böhm, Wilhelm Krone
SUMMARY
Introduction: Data for quality of care in patients with diabetes mellitus type 2 are lacking in
Germany. Methods: To estimate the potential for cardiovascular prevention, the authors compared
the proportion of patients (total n = 51,053) meeting guideline-based targets for glycemia,
arterial hypertension, and dyslipidemia, with expenditure on drug therapy. We used data of the
DUTY registry (diabetes mellitus needs unrestricted evaluation of patient data to yield treatment
progress). Results: 86%, 74.1%, or 33.2% of the patients received hypoglycemic,
antihypertensive, or lipid-lowering medications, respectively. Only 25.5% of the study population
received a statin. The target in glycosylated hemoglobin (HbA1c< 7%) was met in 45.9%, only
7.6% reached their target blood pressure values of < 130/80 mmHg, and the target goal of
LDL-C < 100 mg/dl (< 2.6 mmol/l) was achieved in only 15.8%. Discussion: Given the convincing
evidence for the efficacy of antihypertensive and lipid-lowering drug therapy in lowering
cardiovascular event rates, and the poor evidence for effectiveness of hypoglycemic treatment
alone in reducing cardiovascular event rates, these data suggest that guideline implementation
must be improved, in particular for treatment of dyslipidemia and hypertension.
Dtsch Arztebl 2007; 104(13): A 861–7.
Key words: diabetes mellitus type 2, guideline, health services research, registry, cardiovascular
risk factor
M ore than 5 million people in Germany suffer from type 2 diabetes mellitus (DM2).
Persons with DM2 have a two- to fourfold elevation of the risk of coronary heart
disease (CHD) compared to the general population, and a correspondingly increased
mortality (1). Most deaths of DM2 patients are due to secondary macrovascular disease (2).
Haffner et al. (1) were the first to show the importance of giving primary preventive
treatment to type 2 diabetics that is just as intensive as the treatment of non-diabetics after
myocardial infarction (so-called secondary prevention). Current guidelines accordingly
treat DM2 as an equivalent risk factor for CHD (3–5). The target-value-oriented treatment
of risk factors such as hyperglycemia (HbA1c), dyslipoproteinemia, arterial hypertension,
overweight, and other parameters is beneficial both to patients with manifest DM2 and to
persons at high risk for DM2 (3). Evidence suggests, however, that cardiovascular risk
factors are inadequately treated in a large fraction of these patients (6). Only limited data
are available regarding the quality of care of patients with DM2 in Germany in comparison
to guideline recommendations, e.g., in a subgroup of the HYDRA study (a point prevalence
study) (7).
One may therefore suppose that the quality of care of DM2 patients might leave room for
improvement. In particular, it is unclear which areas of risk prevention suffer from the
greatest deficiencies, and in which ones a more consistent application of guideline
recommendations would lead to the greatest benefit. Guidelines for the treatment of diabetes
have been available in Germany for many years, including those of the German Diabetes
Society (e1) and the National Care Guidelines for diabetes published by the Care Guidelines
Program (Programm für Versorgungsleitlinien) of the German Medical Association (e2).
Geschäftsstelle der Arzneimittelkommission der deutschen Ärzteschaft, Berlin (Prof. Dr. med. Berthold); Klinik II und Poliklinik für
Innere Medizin der Universität zu Köln, Köln (Prof. Dr. Gouni-Berthold, Prof. Dr. med. Krone); MSD Sharp & Dohme GmbH, Haar
(Dr. med. Bestehorn); Klinik für Innere Medizin III, Kardiologie, Angiologie und Internistische Intensivmedizin, Universitätsklinikum
des Saarlandes, Homburg/Saar (Prof. Dr. med. Böhm)
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 1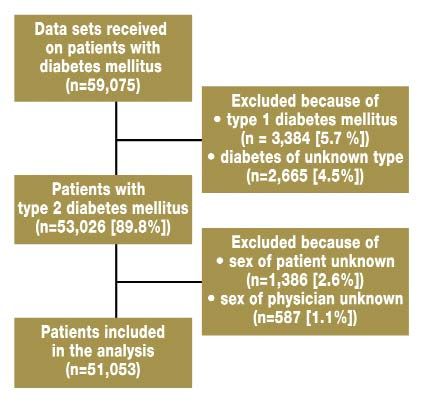
MEDICINE
TABLE 1
Patient characteristics (51,053 patients with type 2 diabetes)
Sex 51.4% female
Age (years) 65.2 ± 10.9 years*1
< 40 1.3 %
40–59 27.3 %
60–74 52.9 %
75 and older 18.5 %
Duration of diabetes (years) 6.7 ± 6.2 years*1
800 certificates/quarter) or large practices
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 2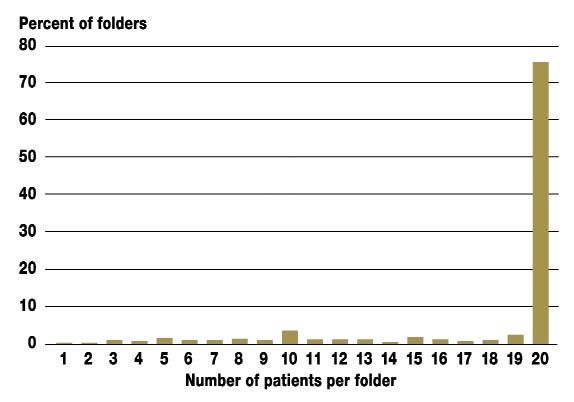
MEDICINE (> 1,200 certificates/quarter). Each participating physician was asked to fill out a four-page questionnaire for 20 consecutive patients with type 1 or type 2 diabetes (20 patients = 1 set of questionnaires) (see www.aerzteblatt.de/diabetes_questionnaire_german for questionnaire in German). For their documentation work, the physicians were paid 25 euros per patient. The following parameters were evaluated for each patient (quantitatively or "yes"/"no"): sex, date of birth, height, weight, type of diabetes, year of initial diagnosis, whether or not the patient received structured diabetes education, presence or absence of CHD and/or peripheral arterial occlusive disease (PAOD), history of stroke, heart failure, cigarette smoking, micro- or macroalbuminuria, fasting blood sugar, hemoglobin A1c, antihyperglycemic therapy (diet, oral antidiabetics, biguanides, sulfonylureas, glucosidase inhibitors, insulin), systolic and diastolic blood pressure, antihypertensive treatment (ACE inhibitors, AT1 antagonists, beta-blockers, calcium antagonists, diuretics, other), lipoprotein concentrations (total cholesterol, LDL-C, HDL-C, triglycerides), and lipid-reducing therapy (diet, statins, fibrates, other). Among the physicians who were asked to participate, 3,213 (48%) agreed to do so. The others were not asked again. The participating physicians returned 3,337 sets of questionnaires. The recruitment phase was terminated as soon as more than 50,000 data sets were obtained. Each set of questionnaires contained data on 17.4 patients (mean); more than 75% of the questionnaire sets contained data on 20 patients. The exact distribution of the number of patients per questionnaire set is shown in the additional diagram 1 (see additional material at the end of this article). Among the patients on whom data were obtained, 89.8% had DM2, 5.7% had DM1, and 4.5% had another or an unidentified type of diabetes. Only patients with DM2 were considered for evaluation in the present study. Cases in which the sex of the patient or the physician was unknown were excluded. The study population that resulted contained 51,053 persons, 48.6% male and 51.4% female. Characteristics of the patients studied are shown in the additional diagram 2. The target criteria were based on the current recommendations of the American Diabetes Association (3). The statistical methods that were applied were limited to descriptive statistics (mean, standard deviation). Category variables were reported as percentages of the study population. Results General findings The mean patient age and the distribution of patient ages are reported in table 1. The mean duration of diabetes in the study was 6.7 years; 16.6% of patients had newly developed diabetes within the past year, and approximately one-fifth had already suffered from diabetes for more than 10 years. Information regarding accompanying atherosclerotic disease, heart failure, smoking, body mass index, and the presence of micro- or macroalbuminuria is also reported in table 1. 41% of patients had received structured diabetes education. Glycemic control and antihyperglycemic therapy 53.3% of patients measured their own blood sugar; 27.9% did so regularly, 25.4% irregularly. Fasting blood sugar values were available for ca. 75% of patients. The values obtained for blood glucose and HbA1c and the antihyperglycemic treatments used are shown in table 2. Blood pressure and antihypertensive therapy The values obtained for blood pressure and the antihypertensive treatments used are shown in table 3. Lipoproteins and lipid-modifying therapy Table 4 contains information on average lipoprotein concentrations and the results of lipid-reducing therapy. Only 5.8% of patients reached all 3 target values for LDL-C, HDL-C and triglycerides (table 5), while 33.8% reached at least 2 target values. On the other hand, 25.9% reached none of the 3 target values. All in all, 33.3% of patients had an elevated LDL-C concentration and, at the same time, a low HDL-C concentration. Further information on the distribution of patient-related parameters (age, body mass index) and target values is contained in the additional diagram 3. Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 3
MEDICINE
Discussion
Because of their relatively brief duration, randomized, controlled trials (RCT's) often do
not adequately reflect the long-term course of chronic illness or the degree of effectiveness
of an intervention. Furthermore, relevant subgroups of patients (e.g., those with multiple
morbidities) are often inadequately represented. For these reasons, registry data are usually
more informative for an analysis of the quality of patient care that is delivered in actual
practice (9). The present study of type 2 diabetics shows that results of widely varying
quality were obtained with respect to three areas of risk factor control that are important for
the prevention of cardiovascular complications, namely glycemia, high blood pressure, and
lipid concentrations. Nearly half of all patients had adequate glycemic control, but far fewer
patients met the target values set by current guidelines for blood pressure and lipid
concentrations.
TABLE 2
Glycemia and antihyperglycemic therapy*1
Fasting blood glucose*2 148 ± 47 mg/dl (8.2 ± 2.6 mmol/l)*3
< 110 mg/dl (< 6.1 mmol/l) 17.3 %
< 120 mg/dl (< 6.7 mmol/l) 27.5 %
< 130 mg/dl (< 7.2 mmol/l) 40.0 %
Hemoglobin A1c 7.3 ± 1.3% *3
< 6.5 % 26.7 %MEDICINE
With respect to lipid concentrations, only a small percentage of patients was treated
(33.2%), and the number meeting the target values was correspondingly low (LDL-C
< 100 mg/dl [ 140 mmHg or diastolic > 90 mmHg 65.3 %
Systolic < 130 mmHg and diastolic < 80 mmHg 7.5 %
Systolic < 120 mmHg and diastolic < 80 mmHg 2.8 %
Antihypertensive therapy
Medical treatment overall 74.1 %
ACE inhibitors 43.3 %
AT1 antagonists 13.7 %
Beta-blockers 26.2 %
Calcium antagonists 16.4 %
Diuretics 22.8 %
Other 7.6 %
*1 Percentage of the study population of 51,053 patients with type 2 diabetes mellitus.
*2 Mean ± standard deviation.
DM2 is considered to be a risk factor equivalent for coronary heart disease, and it is
currently held that the risk factors of diabetics who have not experienced any cardiovascular
events should be treated just as intensively as those of post-infarct patients (4). Cardiovascular
events are the most common cause of death in persons with DM2 and are a major contributor
to morbidity. Smoking cessation (e5), acetylsalicylic acid (e6), and the treatment of
dyslipidemia (e7) and hypertension (e8) are the pillars of effective risk factor management.
The treatment of modifiable CHD risk factors (hypertension and dyslipoproteinemia) and
the administration of ACE inhibitors can reduce mortality in type 2 diabetics (11, 12). In the
HOPE study, for example, the "number needed to treat" among diabetics for the prevention
of one cardiovascular death was calculated to be 29 (over 4.5 years).
Hypertension
The target values for blood pressure were, in general, missed by a wide margin even though
74.1% of patients were treated with antihypertensive medication. One can only conclude
from these figures that the treatment given was inadequate. Target values below 130/80
mmHg should be aimed at, if this is tolerated. Blood pressure above 140/90 mmHg should,
in general, be treated with medications. Randomized studies have shown that effective
reduction of blood pressure reduces the frequency of cardiac events, stroke, and renal
dysfunction (13) (e9–e11). A reduced frequency of cardiac events has been documented
with the use of ACE inhibitors, AT1 antagonists, beta-blockers, diuretics, and calcium
antagonists. The guidelines mainly recommend diuretics and ACE inhibitors (as well as
AT1 antagonists) as agents of first choice. If a dual or multiple drug combination is used, a
diuretic should be one of the drugs given. This was rarely the case in the study group; thus,
diuretics were apparently underused. Furthermore, every diabetic with hypertension should
be treated with an ACE inhibitor (or, if poorly tolerated, with an AT1 antagonist). Though
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 5MEDICINE
approximately half of all patients received a medication from these classes, undertreatment
was present here as well. In view of the poor control of blood pressure that was achieved, it
seems probable that the doses of the drugs administered were often too low. An American
study showed that more than half of all patients with poorly controlled hypertension did not
receive a higher dose of medication despite repeated visits to physicians (14). It should be
noted, however, that hypertension can remain difficult to control in some patients despite
intensive medical treatment (15).
Dyslipoproteinemia
The primary goal of lipid-reducing treatment is an LDL concentration below 100 mg/dl
(2.6 mmol/l) or a reduction of the initial value by approximately 30% to 40%. The use of a
statin is recommended for patients above 40 years old or for younger patients at elevated
risk (3). Randomized studies have shown a significant reduction of the risk of cardiac and
cerebrovascular events in DM2 patients through the use of statins (11) (e12–e14). One such
study was the Heart Protection Study (HPS). In a group of more than 6,000 diabetics with
or without pre-existing cardiovascular disease, the use of 40 mg/day of simvastatin
significantly lowered the risk of fatal and nonfatal myocardial infarction (absolute risk
reduction [ARR], 4.9%; NNT over 5 years, 20) (16). The numbers of coronary deaths,
strokes, and revascularization procedures were also significantly reduced. Also, in the
CARDS study of type 2 diabetics without known cardiovascular disease, the use of
10 mg/day of atorvastatin significantly reduced the frequency of macroangiopathic events
(ARR 3.2%, NNT 31 over 4 years) (17).
TABLE 4
Lipoproteins and lipid-reducing therapy*1
Total cholesterol 224 ± 51 mg/dl (5.8 ± 1.3 mmol/l)*2
LDL cholesterol 135 ± 37 mg/dl (3.5 ± 0.96 mmol/l)*2
< 100 mg/dl (MEDICINE Blood sugar control Normoglycemia is the essential treatment goal for adequate control of diabetes. Randomized studies have shown that an improvement of the metabolic state lowers the frequency of microvascular complications (18, e15–e17). In the Veterans Administration Diabetes Trial, a cross-sectional analysis showed no association of HbA1c levels with macrovascular disease (19). Epidemiologic data suggest that glycemic control can, in fact, reduce the frequency of macrovascular complications, but supportive data from randomized studies are still sparse (e18). There are only a few prospective end-point studies on the use of antidiabetic agents, even though such studies are the most important instruments for the documentation of efficacy of medical treatment. 5 prospective, controlled studies took microvascular complications, macrovascular disease, and/or mortality as endpoints (e15, e19–e26). To sum up their results, it can be stated that, although cardiovascular endpoints were shown to be positively influenced by metformin, sulfonylureas, and insulin (by way of a reduction of blood glucose), no positive individual effect of any antidiabetic agent on cardiovascular endpoints has been demonstrated to date, except with metformin and (with certain reservations) pioglitazone (20). It is very difficult to separate the effects of medical intervention from those of dietary or behavioral changes, but the data do clearly indicate a weak beneficial effect of antihyperglycemic drug therapy on cardiovascular endpoints. A recent metaanalysis revealed that near-normal glycemic control reduces the frequency of macrovascular events to a far greater extent in DM1 than in DM2 (21). The efficacy of antihyperglycemic therapy in DM2 was also restricted to stroke and peripheral vascular disease; there was no statistically significant reduction of cardiac events. The goal of guideline-based treatment is to achieve near-normal blood glucose values, even if the individual specialty societies recommend slightly different target values for HbA1c (German Diabetes Society, < 6.5%; American Diabetes Association and German Disease Management Program, < 7.0%; new recommendations of the European Association for the Study of Diabetes, < 6.0%). Nonetheless, the value of these therapeutic measures with respect to the reduction of cardiovascular complications must be considered in comparison to the effects of lipid- and blood-pressure-reducing methods. It should not be forgotten that the guideline recommendations for the prevention of secondary complications mostly rely on surrogate parameters (HbA1c, LDL-C, and blood pressure). Certain measures, such as treatment with statins or ACE inhibitors, have been shown to have a beneficial effect on directly patient-related, "hard" endpoints, but findings of this type have not yet been reflected in the guidelines. Such endpoint studies are currently available only for statins, antihypertensive drugs (mostly ACE inhibitors) and acetylsalicylic acid. Particular attention should be paid to the treatment of diabetics with statins, because it is in this area that undertreatment is greatest. As far as the use of antihypertensive agents is concerned, more diligent follow-up assessment of the results of treatment in each patient would seem to be an appropriate way of better achieving the established goals. A paradox in the delivery of care It is paradoxical that the target values for lipids were, in general, not reached, while better results were obtained for blood sugar control. The latter depends on the interaction of multiple different factors, including complex medication regimens (oral antidiabetic agents, insulin) that may have significant side effects, dietary measures, and exercise. Patient compliance seems to play a much larger role in blood sugar control than, for example, in the management of an elevated LDL-C. The latter can generally be adequately treated with the daily use of a statin – a relatively simple measure. It is thus surprising that the guideline recommendations were not met in this area, particularly in view of the fact that the reduction of lipid concentrations to the target values is known to reduce mortality. Limitations of the study We cannot exclude systematic bias in the selection of the participating physicians, because they were not chosen at random, but rather by representatives of the sponsoring pharmaceutical firm. Data acquisition in large-scale cross-sectional databases (registries) can lead to problems in data quality that are not found in prospective, controlled studies. In the present study, this potential difficulty was compensated for, at least partially, by sampling of the participating medical practices for data verification. On the other hand, data from registries Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 7
MEDICINE
TABLE 5
Percentage of patients who achieved one, two, or three of lipid/lipoprotein target values
LDL/cholesterol HDL and triglycerides Percentage Number of target
values reached
LDL-cholesterol < 100 mg/dl HDL 40 resp. 50 mg/dl ( 1.04 resp. 1.3 mmol/l) and 5.8 3
(< 2.6 mmol/l) TG < 150 mg/dl (< 1.7 mmol/l)
HDL 40 resp. 50 mg/dl ( 1.04 resp. 1.3 mmool/l) and 3.6 2
TG 150 mg/dl (1.7 mmol/l)
HDL < 40 resp. 50 mg/dl (< 1.04 resp. 1.3 mmol/l) and 2.3 2
TG < 150 mg/dl (< 1.7 mmol/l)
HDL < 40 resp. 50 mg/dl (< 1.04 resp. 1.3 mmol/l) and 3.8 1
TG 150 mg/dl ( 1.7 mmol/l)
LDL-cholesterol 100 mg/dl HDL 40 resp. 50 mg/dl ( 1.04 resp. 1.3 mmol/l) and 22.1 2
( 2.6 mmol/l) TG < 150 mg/dl (< 1.7 mmol/l)
HDL 40 resp. 50 mg/dl ( 1.04 resp. 1.3 mmol/l) and 28.8 1
TG 150 mg/dl ( 1.7 mmol/l)
HDL < 40 resp. 50 mg/dl (< 1.04 resp. 1.3 mmol/l) and 7.5 1
TG < 150 mg/dl (< 1.7 mmol/l)
HDL < 40 resp. 50 mg/dl (< 1.04 resp. 1.3 mmol/l) and 25.9 0
TG 150 mg/dl ( 1.7 mmol/l)
HDL, high-density lipoprotein; TG, triglycerides: LDL, low-density lipoprotein.
reflect the actual state of patient care more closely than controlled studies can, and
registries also provide a much more comprehensive sample. The present study, because it is
a cross-sectional study of surrogate parameters, cannot yield any conclusion regarding the
effect of the individual treatment measures on clinical endpoints. Furthermore, only a
monofactorial assessment of risk factors and treatment results could be performed. The
overall risk of individual patient groups can only be estimated in more comprehensive
studies than this one. The data for this study were acquired before the Disease Management
Program was introduced in Germany. It is possible that the DMP has already improved the
quality of care beyond what was found in this study, though no data are yet available that
would indicate this.
The American Diabetes Association estimates that optimal care of diabetic patients in
the United States over the next 30 years could result in the saving of 3.5 million lives, 18
million serious diabetic complications, and 325 billion dollars (22). Optimal care, in this
context, is defined as HbA1c < 7%, blood pressure < 130/80 mmHg, body mass index
< 25 kg/m2, daily use of acetylsalicylic acid and a statin, and refraining from cigarette smoking.
According to the data of the DUTY registry, far fewer than 5% of all type 2 diabetics in
Germany achieve these targets. The care of type 2 diabetics in this country is thus far from
optimal.
Conflict of Interest Statement
Prof. Dr. Gouni-Berthold has received lecture honoraria from Pfizer and Eli Lilly as well as research project support from MSD
Sharp & Dohme, Pfizer, Sanofi-Aventis, and Takeda. Dr. Bestehorn is employed by MSD Sharp & Dohme. Prof. Böhm has received
lecture honoraria from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, MSD Sharp & Dohme, Essex Pharma, Pfizer,
Servier, and Sanofi-Aventis. In addition, he serves as a consultant to AstraZeneca, Boehringer Ingelheim, MSD Sharp & Dohme,
Essex Pharma, Pfizer, Servier, and Sanofi-Aventis. Prof. Krone has received lecture honoraria from AstraZeneca, MSD Sharp &
Dohme, Essex Pharma, Pfizer, Solvay, Bayer, and Sanofi-Aventis. In addition, he serves as a consultant to MSD Sharp & Dohme
and Essex Pharma. Prof. Berthold states that he has no conflict of interest as defined by the Guidelines of the International
Committee of Medical Journal Editors.
Prof. Berthold emphasizes that the views and opinions expressed in this article are those of the first author and do not necessarily
represent the ones of the Drug Commission of the German Medical Association.
Manuscript received on 7 September 2006; final version accepted on 25 January 2007.
Translated from the original German by Ethan Taub, M.D.
REFERENCES
For e-references please refer to the additional references listed below.
1. Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M: Mortality from coronary heart disease in subjects with type
2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998; 339:
229–34.
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 8MEDICINE
2. Morrish NJ, Stevens LK, Head J, Fuller JH, Jarrett RJ, Keen H: A prospective study of mortality among middle-aged
diabetic patients (the London Cohort of the WHO Multinational Study of Vascular Disease in Diabetics) II: Associated
risk factors. Diabetologia 1990; 33: 542–8.
3. Standards of medical care for patients with diabetes mellitus. Diabetes Care 2000; 23 Suppl 1: S32–42.
4. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on
detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001; 285:
2486–97.
5. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr., Clark LT, Hunninghake DB et al.: Implications of recent clinical
trials for the national cholesterol education program adult treatment panel III guidelines. Circulation 2004; 110:
227–39.
6. Saydah SH, Fradkin J, Cowie CC: Poor control of risk factors for vascular disease among adults with previously
diagnosed diabetes. JAMA 2004; 291: 335–42.
7. Lehnert H, Wittchen HU, Pittrow D, Bramlage P, Kirch W, Bohler S et al.: Prevalence and pharmacotherapy of
diabetes mellitus in primary care. Dtsch Med Wochenschr 2005; 130: 323–8.
8. Krone W, Bohm M: Diabetes mellitus needs unrestricted evaluation of patient data to yield treatment progress.
The DUTY Register. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2004; 47: 540–6.
9. Bestehorn K: Medical registries. Med Klin (Munich ) 2005; 100: 722–8.
10. Bergenstal RM, Nag SS, Reusch JE, Sajjan SG, Alexander CM: Macrovascular risk factors in patients with diabetes:
physician treatment strategies and extent of control. Endocr Pract 2005; 11: 172–9.
11. Pyorala K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G: Cholesterol lowering with simvastatin
improves prognosis of diabetic patients with coronary heart disease. A subgroup analysis of the Scandinavian
Simvastatin Survival Study (4S). Diabetes Care 1997; 20: 614–20.
12. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G: Effects of an angiotensin-converting-enzyme inhibitor,
ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators.
N Engl J Med 2000; 342: 145–53.
13. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S et al.: Effects of intensive blood-pressure
lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal
Treatment (HOT) randomised trial. HOT Study Group. Lancet 1998; 351: 1755–62.
14. Moser M, Setaro JF: Resistant or difficult-to-control hypertension. N Engl J Med 2006; 355: 385–92.
15. Singer GM, Izhar M, Black HR: Goal-oriented hypertension management: translating clinical trials to practice. Hypertension
2002; 40: 464–9.
16. Collins R, Armitage J, Parish S, Sleigh P, Peto R: MRC/BHF Heart Protection Study of cholesterol-lowering with
simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 2003; 361: 2005–16.
17. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ et al.: Primary prevention of
cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study
(CARDS): multicentre randomised placebo-controlled trial. Lancet 2004; 364: 685–96.
18. Diabetes Control and Complications (DCCT) Research Group: The effect of intensive treatment of diabetes on the
development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes
Control and Complications Trial Research Group. N Engl J Med 1993; 329: 977–86.
19. Kirkman MS, McCarren M, Shah J, Duckworth W, Abraira C: The association between metabolic control and
prevalent macrovascular disease in type 2 diabetes: the VA Cooperative Study in diabetes. J Diabetes Complications
2006; 20: 75–80.
20. Seufert J: Kardiovaskuläre Endpunktstudien in der Therapie des Typ-2-Diabetes-mellitus. Dtsch Arztebl 2006; 103:
A934–42.
21. Stettler C, Allemann S, Juni P, Cull CA, Holman RR, Egger M et al.: Glycemic control and macrovascular disease in types
1 and 2 diabetes mellitus: Meta-analysis of randomized trials. Am Heart J 2006; 152: 27–38.
22. Kuehn BM: „Polypill“ could slash diabetes risks. JAMA 2006; 296: 377–80.
ADDITIONAL REFERENCES
e1. Leitlinien der Deutschen Diabetes Gesellschaft. http://www.ddg.info/. 2006.
e2. Bundesärztekammer, Arzneimittelkommission der deutschen Ärzteschaft, Deutsche Diabetes Gesellschaft,
Fachkommission Diabetes Sachsen, Deutsche Gesellschaft für Innere Medizin, AWMF: Ärztliche Zentralstelle
Qualitätssicherung (Hrsg.): Nationale Versorgungs-Leitlinie Diabetes mellitus Typ 2. Nationales Programm für die
Versorgungs-Leitlinien bei der Bundesärztekammer. 2002. http://www.versorgungsleitlinien.de/themen/pdf/
nvldiabetes.pdf
e3. Arzneimittelkommission der deutschen Ärzteschaft: Therapieempfehlungen zum Diabetes mellitus Typ 2.
Arzneiverordnung in der Praxis Supplement. 2002. http://www.akdae.de/35/85_Diabetes_ 2002_1Auflage.pdf
e4. Ärztliches Zentrum für Qualität in der Medizin: www.leitlinien.de 2006.
e5. Haire-Joshu D, Glasgow RE, Tibbs TL: Smoking and diabetes. Diabetes Care 1999; 22: 1887–98.
e6. Colwell JA: Aspirin therapy in diabetes. Diabetes Care 1997; 20: 1767–71.
e7. Haffner SM: Management of dyslipidemia in adults with diabetes. Diabetes Care 1998; 21: 160–78.
e8. Arauz-Pacheco C, Parrott MA, Raskin P: The treatment of hypertension in adult patients with diabetes. Diabetes
Care 2002; 25: 134–47.
e9. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr. et al.: The seventh report of the joint
national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report.
JAMA 2003; 289: 2560–72.
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 9MEDICINE
e10. UK Prospective Diabetes Study Group: Tight blood pressure control and risk of macrovascular and microvascular
complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ 1998; 317: 703–13.
e11. Adler AI, Stratton IM, Neil HA, Yudkin JS, Matthews DR, Cull CA et al.: Association of systolic blood pressure with
macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study.
BMJ 2000; 321: 412–9.
e12. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG et al.: The effect of pravastatin on coronary
events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events
Trial investigators. N Engl J Med 1996; 335: 1001–9.
e13. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a
broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID)
Study Group. N Engl J Med 1998; 339: 1349–57.
e14. Collins R, Armitage J, Parish S, Sleigh P, Peto R: MRC/BHF Heart Protection Study of cholesterol-lowering with
simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 2003; 361: 2005–16.
e15. UK Prospective Diabetes Study (UKPDS) Group: Intensive blood-glucose control with sulphonylureas or insulin
compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK
Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352: 837–53.
e16. UK Prospective Diabetes Study (UKPDS) Group: Effect of intensive blood-glucose control with metformin on
complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS)
Group. Lancet 1998; 352: 854–65.
e17. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. The
Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research
Group. N Engl J Med 2000; 342: 381–9.
e18. Selvin E, Marinopoulos S, Berkenblit G et al.: Meta-analysis:
glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med 2004; 141: 421–31.
e19. Meinert CL, Knatterud GL, Prout TE, Klimt CR: A study of the effects of hypoglycemic agents on vascular
complications in patients with adult-onset diabetes. II. Mortality results. Diabetes 1970; 19 (Suppl): 830.
e20. The University Group Diabetes Program. A study of the effects of hypoglycemic agents on vascular complications
in patients with adult-onset diabetes. V. Evaluation of pheniformin therapy. Diabetes 1975; 24 (Suppl 1):
65–184.
e21. Effects of hypoglycemic agents on vascular complications in patients with adult-onset diabetes. VIII. Evaluation of
insulin therapy: final report. Diabetes 1982; 31(Suppl 5): 1–81.
e22. Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S et al.: Intensive insulin therapy prevents the
progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes
mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract 1995; 28: 103–17.
e23. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2
diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352: 854–65.
e24. Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O: Multifactorial intervention and cardiovascular
disease in patients with type 2 diabetes. N Engl J Med 2003; 348: 383–93.
e25. Charbonnel B, Dormandy J, Erdmann E, Massi-Benedetti M, Skene A: The prospective pioglitazone clinical trial in
macrovascular events (PROactive): can pioglitazone reduce cardiovascular events in diabetes? Study design and
baseline characteristics of 5238 patients. Diabetes Care 2004; 27: 1647–53.
e26. Dormandy JA, Charbonnel B, Eckland DJ, Erdmann E, Massi-Benedetti M, Moules IK et al.: Secondary prevention
of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone
Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet 2005; 366: 1279–89.
Corresponding author
Prof. Dr. med. Heiner K. Berthold
Geschäftsstelle der Arzneimittelkommission der deutschen Ärzteschaft
Herbert-Lewin-Platz 1
D-10623 Berlin, Germany
berthold@uni-bonn.de
Additional Material see next page
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 10MEDICINE
Additional Material
ADDITIONAL DIAGRAM 1
The number of patients in each folder (plotted against the corresponding percentage of
folders that were submitted). Each folder was supposed to contain up to 20 data sets
(i.e., data on up to 20 patients). The mean number of data sets per folder was 17.7.
More than 75% of all folders contained the full complement of data sets (20).
ADDITIONAL DIAGRAM 2
Flow diagram depicting the entry of data sets to the study after
exclusion of some data sets for various reasons. Of the 59,075 data
sets that were received, 51,053 were analyzed.
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 11MEDICINE
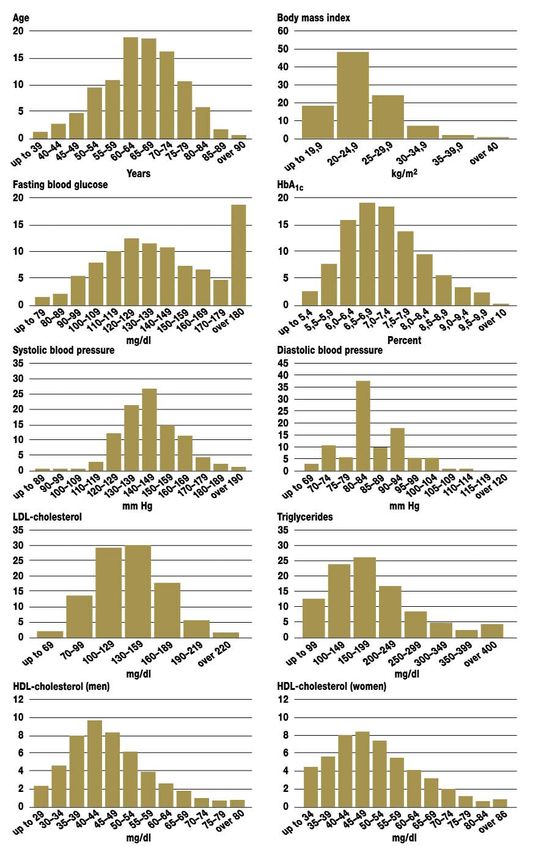
Categorized
ADDITIONAL DIAGRAM 3
frequency
distributions.
The percentages
given are in relation
to the overall study
population of
patients with type 2
diabetes, n=51,053
(for HDL-C, the
percentages given
are in relation to the
total number of
men, resp. women,
in the study).
Dtsch Arztebl 2007; 104(13): A 861–7 ⏐ www.aerzteblatt.de 12You can also read

















































