Clinical impact of NPM1-mutant molecular persistence after chemotherapy for acute myeloid leukemia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

American Society of Hematology
2021 L Street NW, Suite 900,
Washington, DC 20036
Phone: 202-776-0544 | Fax 202-776-0545
bloodadvances@hematology.org
Clinical impact of NPM1-mutant molecular persistence after chemotherapy for acute
myeloid leukemia
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
Tracking no: ADV-2021-005455R2
Ing Tiong (Austin Health and Olivia Newton John Cancer Research Institute, Australia) Richard Dillon
(Guy's Hospital, United Kingdom) Adam Ivey (The Alfred Hospital, Australia) James Kuzich (Austin Health
and Olivia Newton John Cancer Research Institute, Australia) Nisha Thiagarajah (Peter MacCallum Cancer
Centre, Australia) Kirsty Sharplin (Royal Adelaide Hospital, Australia) Chung Hoow Kok (South Australian
Health & Medical Research Institute (SAHMRI), Australia) Aditya Tedjaseputra (Monash Health, Australia)
James Rowland (Princess Alexandra Hospital, Australia) Carolyn Grove (Sir Charles Gairdner
Hospital/PathWest, Australia) Emad Abro (Princess Alexandra Hospital, Australia) Jake Shortt (Monash
University, Australia) Devendra Hiwase (Consultant Haematologist, Royal Adelaide Hospital, Australia)
Ashish Bajel (Peter MacCallum Cancer Centre, Australia) Nicola Potter (King's College, London, United
Kingdom) Matthew Smith (St Bartholomew's Hospital, United Kingdom) Claire Hemmaway (Auckland City
Hospital, New Zealand) Abin Thomas (Cardiff University, United Kingdom) Amanda Gilkes (Cardiff
University, United Kingdom) Nigel Russell (Guy's Hospital, United Kingdom) Andrew Wei (Alfred Hospital
and Monash University, Australia)
Abstract:
Monitoring of NPM1 mutant (mut) measurable residual disease (MRD) in acute myeloid leukemia (AML) has an
established role in patients treated with intensive chemotherapy. The European LeukemiaNet has defined
molecular persistence at low copy number (MP-LCN) as MRD transcript level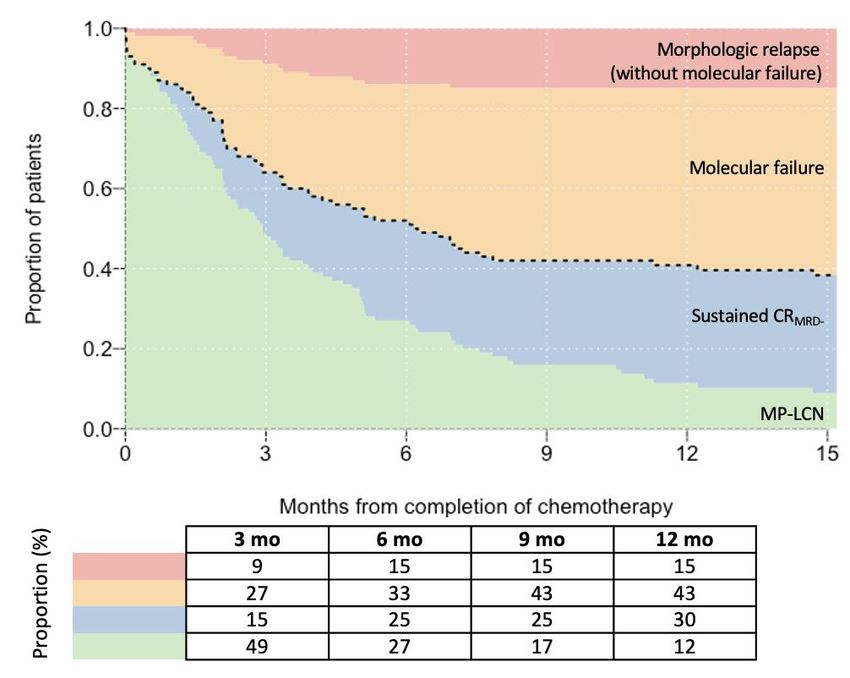
1 Title: Clinical impact of NPM1-mutant molecular persistence after chemotherapy for acute
2 myeloid leukemia
3
4 Running title: Clinical impact of NPM1mut molecular persistence
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
6 Authors: Ing S Tiong*,1,2,3 Richard Dillon*,4,5 Adam Ivey*,1 James A Kuzich,2 Nisha
7 Thiagarajah,3,6 Kirsty Sharplin,7 Chung Hoow Kok,8 Aditya Tedjaseputra,9 James Rowland,10
8 Carolyn S Grove,11 Emad Abro,10 Jake Shortt,9,12 Devendra Hiwase,7 Ashish Bajel,3,6 Nicola E
9 Potter,4 Matthew Smith,13 Claire Hemmaway,14 Abin Thomas,15 Amanda Gilkes,16 Nigel H
10 Russell#,5 and Andrew H Wei#1
11
12 * These authors contributed equally
13 # These authors contributed equally
14
15 Affiliations:
16 1. The Alfred Hospital and Monash University, Melbourne, Australia
17 2. Austin Health and Olivia Newton John Cancer Research Institute, Melbourne, Australia
18 3. Peter MacCallum Cancer Centre, Melbourne, Australia
19 4. Department of Medical and Molecular Genetics, King’s College, London, UK
20 5. Guy’s Hospital, London, United Kingdom
21 6. Royal Melbourne Hospital, Melbourne Australia
22 7. Royal Adelaide Hospital, Adelaide, Australia
23 8. Precision Medicine Theme, South Australian Health & Medical Research Institute,
24 Adelaide, Australia
25 9. Monash Health, Melbourne, Australia
26 10. Princess Alexandra Hospital, Queensland Australia
27 11. Sir Charles Gairdner Hospital and PathWest, Perth, Australia
28 12. School of Clinical Sciences at Monash Health, Monash University, Clayton
11 13. Department of Haematology, St Barts Hospital, London, UK
2 14. Department of Haematology, Auckland City Hospital, New Zealand
3 15. Centre for Trials Research, Cardiff University, Cardiff, UK
4 16. Department of Haematology Cardiff University, Cardiff, UK
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
6 Corresponding author:
7 Andrew H Wei, MBBS, PhD
8 Department of Haematology, The Alfred Hospital,
9 Australian Centre for Blood Diseases, Monash University
10 Melbourne, Victoria 3004, Australia.
11 T: +61 3 9076 3451
12 F: +61 3 9076 2298
13 E: a.wei@alfred.org.au
14
15 Abstract 199 (max 200)
16 Word counts 1378 (max 1200)
17 Figures/Tables 2 (max 2)
18 References 13 (max 25)
21 Key points
2
3 Main point #1: (140-character limit including spaces)
4 Of 100 patients MRD+ after chemo, 42% remain progression-free at 1yr, with spontaneous
5 CRMRD- in 30% or low-level NPM1mut persistence in 12%
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
6
7 Main point #2: (140-character limit including spaces)
8 Relapse is associated with FLT3-ITD and poor NPM1mut MRD response after
9 chemotherapy. MRD-directed pre-emptive therapy may prolong remission
10
11 Abstract [200 words; single paragraph]
12 Monitoring of NPM1 mutant (mut) measurable residual disease (MRD) in acute myeloid
13 leukemia (AML) has an established role in patients treated with intensive chemotherapy. The
14 European LeukemiaNet has defined molecular persistence at low copy number (MP-LCN) as
15 MRD transcript level1 Introduction
2 Acute myeloid leukemia (AML) with mutated (mut) NPM1 is the most common subtype of AML
3 with recurrent genetic abnormalities.1 Monitoring NPM1mut measurable residual disease
4 (MRD) has an established role in the evaluation of patients after intensive chemotherapy,2,3
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
5 and is an emerging regulatory approval endpoint.4 Approximately 25–50% of patients with
6 NPM1mut have persistent MRD at the end of treatment (EOT), associated with higher relapse
7 risk.2,5,6 The European LeukemiaNet (ELN) has defined molecular persistence at low copy
8 number (MP-LCN) as MRD positivity in complete remission (CR) with1 failure were not strictly met in two subjects: one for molecular progression not reaching a ≥1-
2 log10 increase, and another had molecular relapse without a confirmation sample. Survival
3 estimates were calculated from EOT to death (overall survival [OS]), and/or morphologic
4 relapse (relapse-free survival [RFS]), and/or molecular failure (event-free survival [EFS]). Cox
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
model was used for univariate and multivariate analyses.
6 Results and Discussion
7 A total of 100 patients had NPM1mut MRD detected at a median of 36 days (range 19–90)
8 from last course of chemotherapy (characteristics summarized in Supplemental Table S1 and
9 Figure S2). Median age was 50 years, 85% had normal karyotype, and 39% concurrent FLT3-
10 ITD at diagnosis (allelic ratio ≥0.5 in 17%). At EOT, the median NPM1mut level was 13 copies
11 (range 0.3–20,756; 5 were >2,000) and median reduction from baseline 4.5-log (range 1.8–
12 6.0; baseline missing in 7 patients). In this study cohort, MRD levels at EOT were comparable
13 irrespective of the number of chemotherapy courses (range 2–5) completed (Supplemental
14 Figure S3). Patients with longer time to EOT MRD assessment had inferior EFS and RFS
15 (Supplemental Figure S4), presumably due to longer time to hematologic recovery.
16 Patients were followed for a median of 23.5 months: 29 patients died, including 2 after pre-
17 emptive intensive salvage. A total of 41 patients experienced morphologic relapse, including
18 16 without detection of preceding molecular failure, with the interval from last MRD test to
19 relapse 6–73 days (n=8) or >90 days (n=3), extramedullary disease progression (n=1), NPM1
20 wild-type relapse (n=1), and no monitoring (n=3). Thirty-nine (40% of 97 monitored) had
21 subsequent MRD levels meeting the criteria for MP-LCN, with a 2-year EFS of 58%
22 (Supplemental Figure S5).
23 To study the clinical impact of persistent NPM1mut MRD detected at the EOT, we studied the
24 fate of patients at 3-month intervals. By the first landmark analysis at 3 months, 9% patients
25 had experienced morphologic relapse, 27% had molecular failure, and 15% spontaneously
51 achieved sustained CRMRD- (Figure 1). By the 12-month landmark, 15% had morphologically
2 relapsed, 43% had molecular failure, 30% CRMRD-, and 12% had MP-LCN (Figure 1). At final
3 follow-up, 9 patients (9%) had MP-LCN persisting for a median of 14 months (9–32 months)
4 and survived a median of 20.5 months (9–35 months). From study entry, 31 patients (32%)
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
spontaneously achieved CRMRD- that lasted >6 months, the majority (81%) within the first 6
6 months, with only one subsequent progression. Although MP-LCN is well recognized in core-
7 binding factor AML,9,10 previous groups have reported the persistence of NPM1mut transcript
8 up to 1000–2000 copies/105 ABL before significant risk of disease relapse,5,6 leading to the
9 adoption of this threshold by the ELN.7 We were unable to confirm this threshold as patients
10 in our cohort received pre-emptive therapy prior to reaching the threshold. However, 10
11 patients with molecular failure (>1-log rise) who did not receive pre-emptive therapy all
12 subsequently relapsed, without a critical MRD threshold observed. Of the patients who
13 remained event-free at last follow up (n=39), the highest recorded NPM1mut MRD level was
14 only 90 copies. Paired peripheral blood and bone marrow sampling was not performed on this
15 study. Therefore, the clinical relevance of MP-LCN in peripheral blood was not able to be
16 addressed.
17 Among the 43 patients (44%) who experienced molecular failure within the first 12 months, 33
18 (77%) received pre-emptive salvage therapy prior to morphologic relapse, resulting in a
19 significantly prolonged RFS (median 10.6 vs 0.7 months) (Supplemental Figure S6). Time to
20 molecular failure from EOT were similar between patients receiving pre-emptive therapy or
21 not (median 64 vs 99 days).
22 Median time to initiation of pre-emptive therapy after molecular failure was 27 days (range 9–
23 149; Supplemental Figure S7A), with therapy comprising FLAG-based chemotherapy (n=13),
24 venetoclax plus low dose cytarabine (n=11), immediate HSCT (n=5) or others (Supplemental
25 Figure S2). Of 10 patients not salvaged until morphologic relapse, median interval between
26 molecular failure and morphologic relapse was 21 days (range 11–89; Supplemental Figure
61 S7B); salvage therapy summarised in Supplemental Figure S2. Various MRD-directed pre-
2 emptive strategies have been employed, ranging from azacitidine to intensive salvage
3 chemotherapy;8,11 we previously reported the promising role of venetoclax based low-intensity
4 therapy in erasing NPM1mut MRD in 11/12 (92%) patients treated.12 The survival benefit of
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
pre-emptive therapy requires future prospective evaluation.
6 Next, we examined variables associated with molecular failure, morphologic relapse and
7 death (Supplemental Table S2). In univariate analysis, variables associated (p1 In conclusion, patients with NPM1mut MRD positivity after completing intensive chemotherapy
2 and not undergoing HSCT in first remission have a variable course, with a substantial fraction
3 (42%) remaining relapse-free at 1 year, either spontaneously achieving CRMRD- (30%) or
4 retaining low-level transcript in the bone marrow for ≥12 months (12%). Risk factors
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
associated with subsequent disease progression include concurrent FLT3-ITD at diagnosis
6 and suboptimal MRD response at the EOT. This information will be of value to clinicians using
7 NPM1mut MRD to make EOT transplant decisions. The role of pre-emptive treatment for
8 management of molecular failure remains to be determined.
81 Data sharing statement
2 For data sharing, contact the corresponding author: a.wei@alfred.org.au.
3 Acknowledgements
4 AHW: Medical Research Future Fund, Leukemia and Lymphoma Society (SCOR Strasser),
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
National Health and Medical Research Council.
6 RD and NHR: Cancer Research UK, Blood Cancer UK and the UK National Institute for
7 Health Research.
8 Authorship Contributions
9 IST, RD, AI, NHR and AHW designed research, analysed data and wrote the paper. CHK,
10 JAK, NT, KS, AT, JR, CG, EA, JS, DH, AB, NP, MS, CH, AT, and AG contributed patients or
11 analytical tools, interpreted data, and approved the final manuscript.
12 Disclosures of Conflicts of Interest
13 IST has served on speaker’s bureaus for Amgen, Servier; consultancy for Pfizer, Servier.
14 RD has served on advisory boards for Abbvie, Jazz, Menarini, Novartis, Pfizer; receives
15 research funding to the Institution from Abbvie, Amgen; serves on speaker’s bureaus for
16 Astellas, Novartis; consultancy for Abbvie, Astellas, Jazz, Pfizer.
17 CSS has served on advisory board for Abbvie.
18 NHR has served on advisory boards for Astellas, Pfizer; receives research funding to the
19 Institution from Jazz, Pfizer; serves on speaker’s bureaus for Jazz, Novartis.
20 AHW has served on advisory boards for Novartis, Janssen, Amgen, Roche, Pfizer, Abbvie,
21 Servier, Celgene-BMS, Macrogenics, Agios, Gilead; receives research funding to the
22 Institution from Novartis, Abbvie, Servier, Celgene-BMS, Astra Zeneca, Amgen; serves on
23 speaker’s bureaus for Abbvie, Novartis, BMS; receives royalty payments from the Walter
24 and Eliza Hall Institute of Medical Research related to venetoclax.
91 References
2
3 1. Swerdlow SH, Campo E, Harris NL, et al. WHO classification of Tumours of
4 Haematopoietic and Lymphoid Tissues (ed Revised 4th Edition). Lyon: International
5 Agency for Research on Cancer; 2017.
6 2. Ivey A, Hills RK, Simpson MA, et al. Assessment of Minimal Residual Disease
7 in Standard-Risk AML. N Engl J Med. 2016;374(5):422-433.
8 3. Balsat M, Renneville A, Thomas X, et al. Postinduction Minimal Residual
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
9 Disease Predicts Outcome and Benefit From Allogeneic Stem Cell Transplantation in
10 Acute Myeloid Leukemia With NPM1 Mutation: A Study by the Acute Leukemia
11 French Association Group. J Clin Oncol. 2017;35(2):185-193.
12 4. Kronos Bio speeds development of genetically targeted leukemia drug with
13 unique trial design. https://www.statnews.com/2021/03/04/kronos-bio-speeds-
14 development-of-genetically-targeted-leukemia-drug-with-unique-trial-design.
15 Accessed May 06, 2021. .
16 5. Kronke J, Schlenk RF, Jensen KO, et al. Monitoring of minimal residual
17 disease in NPM1-mutated acute myeloid leukemia: a study from the German-
18 Austrian acute myeloid leukemia study group. J Clin Oncol. 2011;29(19):2709-2716.
19 6. Shayegi N, Kramer M, Bornhauser M, et al. The level of residual disease
20 based on mutant NPM1 is an independent prognostic factor for relapse and survival
21 in AML. Blood. 2013;122(1):83-92.
22 7. Schuurhuis GJ, Heuser M, Freeman S, et al. Minimal/measurable residual
23 disease in AML: a consensus document from the European LeukemiaNet MRD
24 Working Party. Blood. 2018;131(12):1275-1291.
25 8. Dillon R, Hills R, Freeman S, et al. Molecular MRD status and outcome after
26 transplantation in NPM1-mutated AML. Blood. 2020;135(9):680-688.
27 9. Miyamoto T, Nagafuji K, Akashi K, et al. Persistence of multipotent
28 progenitors expressing AML1/ETO transcripts in long-term remission patients with
29 t(8;21) acute myelogenous leukemia. Blood. 1996;87(11):4789-4796.
30 10. Yin JA, O'Brien MA, Hills RK, Daly SB, Wheatley K, Burnett AK. Minimal
31 residual disease monitoring by quantitative RT-PCR in core binding factor AML
32 allows risk stratification and predicts relapse: results of the United Kingdom MRC
33 AML-15 trial. Blood. 2012;120(14):2826-2835.
34 11. Platzbecker U, Middeke JM, Sockel K, et al. Measurable residual disease-
35 guided treatment with azacitidine to prevent haematological relapse in patients with
36 myelodysplastic syndrome and acute myeloid leukaemia (RELAZA2): an open-label,
37 multicentre, phase 2 trial. The Lancet Oncology. 2018;19(12):1668-1679.
38 12. Tiong IS, Dillon R, Ivey A, et al. Venetoclax induces rapid elimination of NPM1
39 mutant measurable residual disease in combination with low-intensity chemotherapy
40 in acute myeloid leukaemia. Br J Haematol. 2021;192(6):1026-1030.
41 13. Lausen B, Schumacher M. Maximally Selected Rank Statistics.Biometrics.
42 Biometrics. 1992;48:73–85.
43
101 Figure Legends
2
3 Figure 1. Clinical impact of patients with detectable NPM1mut MRD at completion of
4 chemotherapy. Conversion from initial state (green) to different outcomes censored at first
5
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
event is illustrated: sustained complete molecular remission (CRMRD-; blue), molecular failure
6 (orange), or morphologic relapse without preceding molecular failure (red). Proportion of
7 patients in each category at specified time points are listed as a table below.
8
9 Figure 2. Kaplan-Meier analysis of (A) event-free and (B) overall survival according to
10 FLT3-ITD status at diagnosis and end of therapy (EOT) NPM1mut reduction (4.4-log) from
11 baseline.
11Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
Figure 1
Figure 1Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
Figure 2
Figure 1Downloaded from http://ashpublications.org/bloodadvances/article-pdf/doi/10.1182/bloodadvances.2021005455/1824055/bloodadvances.2021005455.pdf by guest on 25 November 2021
Figure 2
Figure 2You can also read