Consumer product-related injury: trampolines, bunk beds, button batteries
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hazard
(Edition No. 75)
Autumn 2013
Victorian Injury Surveillance Unit
(VISU)
www.monash.edu/miri/visu
Monash Injury Research Institute
(MIRI)
Consumer product-related injury:
trampolines, bunk beds, button batteries
Authors: Karen Ashby, Lesley Day & Emily Kerr
The Victorian Injury Surveillance Unit is now an
This issue of Hazard provides an update on trends in
injuries associated with trampolines and bunk beds, and
independent unit within the newly created Monash
discusses these in relation to the relevant standards. It also Injury Research Institute (MIRI) at Monash
highlights the relatively small but potentially serious injury University, operating separately from the Monash
issue associated with button battery ingestion. University Accident Research Centre (MUARC)
which is also part of MIRI. MUARC will now
concentrate solely on research related to transport
injury, whereas VISU is clustered with other centres
and units working in the home, sport and leisure
stream. For more information on MIRI go to:
www.monash.edu.au/miri/. THE NEW WEB
ADDRESS FOR VISU IS:
www.monash.edu/miri/visu
Summary continues to increase. Statistically significant
increases in admission rates were observed for
of multiple-user injuries, and injuries among
younger children, is becoming apparent as
persons aged 0-4, 5-9, 10-14 and 15-19 years. parents may allow freer access when they no
Trampolines longer fear children falling off the trampoline.
Falls off a trampoline remain the leading cause The number of multiple-user injuries is rising
Each year 1,500 persons are treated in of trampoline-related injury, and although they rapidly despite mandatory safety warnings
Victorian hospitals for an injury sustained are increasing in frequency, the rate of increase incorporated into AS 4989-2006 against this
while using a trampoline. Despite the is significantly less than that for all trampoline practice. Trampolines greater than 500 mm in
strengthening of regulations, mandating of injury, possibly attributable to the introduction height are not recommended for children aged
safety information for owners and users, of trampoline enclosures (nets). However, less than six years yet one-third of the injuries
and substantial design modifications to the the presence of enclosures may have had an reported were among children aged less than
trampoline, both the frequency and population unintended effect as an increase in the number 6 years.
rate of injury from trampoline use in Victoria
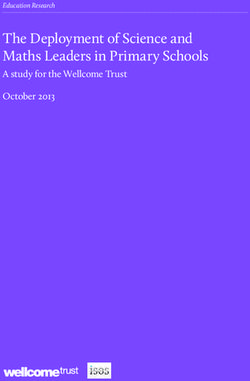
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 1It appears that there has been little impact of compartment of the item in which the batteries recommended that trampolines should not be and Materials ASTM standard in 2003, it
the 2006 revision to the Standard on the trend are housed and the battery packaging. Raising used at home or in routine physical education was not included in the 2006 revision of the Figure 1a ED presentations for trampoline injury by year and broad cause,
in the frequency of spring and frame injury. A parental awareness of the risk of button battery classes and argued that they should also have Australian Standard. Victoria, July 1, 2002 to June 30, 2011
less than desired uptake of the requirements ingestion should be a co-ordinated strategy no place in outdoor playgrounds (AAP, 1999).
in the voluntary Standard may be another with a consistent message regarding the An updated AAP policy statement released in This Hazard article examines the patterns
factor contributing to the absence of an overall potential for harm. 2012 re-iterated this stance citing that, despite of, and trends in, hospital-treated trampoline
decrease in trampoline injury. the implementation of safety measures such injury in Victoria during the period July 2002
as frame-padding and netting, the risk of to June 2011. Both fall and non-fall injury
Bunk Beds Introduction injury had not been substantially mitigated
(AAP, 2012). In 2007, the Canadian
are considered. Several aspects of trampoline
injury are investigated in greater detail to
Bunk beds are an injury risk for young Paediatric Society and Canadian Academy explore the impact of strengthened Standards
Consumer products are associated with a of Sports Medicine similarly called for a ban and design changes.
children, in particular if the bunk bed is
sizeable proportion of hospital treated injury. on recreational use in the domestic setting
used inappropriately (e.g. for playing) or if
Products may be involved in injuries through (Leonard and Joffee, 2009).
it has been poorly made. There are nearly
physical failure, inadequate design, inadequate
Methodology
300 injuries related to bunk beds treated in
instructions or safety warnings, misuse, and The response of the Australian injury
Victorian hospitals each year. Data were extracted from the Victorian
unforeseen human and environmental factors prevention sector was more measured and Admitted Episodes Dataset [Victorian hospital
(Hazard 63). Injury surveillance systems focused on revising the Australian Standard
Certainly there has not yet been a reduction admissions] and the Victorian Emergency
rarely, if ever, identify the level or type of for trampolines to include measurable safety
in the number of bunk bed related injuries Minimum Dataset [emergency department
involvement of products in injury causation. aspects designed to reduce the risk of injury.
associated with the introduction of the current presentations to 39 Victorian hospitals] for
However, broad overviews are possible, An Australian Standard, AS 4989–2003
mandatory Australian Standard for bunk beds the financial years 2002/3 to 2010/11. See
particularly for products that can be identified Trampolines—Safety aspects, was published
(AS/NZS 4220) which came into effect in Box 1 for details of the data sources and case
with a specific code. in 2003. The voluntary standard set out Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations)
April 2005 and covers requirements for the selection.
construction, design and labeling of bunk requirements for components and design as
It is seven years since consumer product- well as specifying information on assembly
beds. We were unable to determine if the Results: overview Figure 1b Hospital admitted trampoline injury by year and broad cause,
related injury has been a topic for Hazard. In and maintenance.
Standard might have arrested any previous Victoria, July 1, 2002 to June 30, 2011
this edition, we have selected two products
increasing trend in bunk-bed injury rates, as
(trampolines and bunk beds) for which The Standard was revised and improved in Frequency
pre-2005 data are not available.
standards have existed for sufficient length of October 2006 (AS 4989-2006: Trampolines—
time to start to have an impact on injury trends, Safety aspects) removing specifications for Over the nine-year period 2002/3 to 2010/11
While the ACCC generally recommend
if effective. These products were last covered frame design and focusing on safety aspects there were 13,814 trampoline-related injuries
against children under nine years old from
in Hazard 61, 2005 and Hazard 44, 2000 such as spring and frame-padding design, treated in Victorian hospitals. This number
using a bunk bed, our study found almost
respectively. Ongoing interest in trampolines protection of sharp edges, safety marking comprised 3,199 hospital admitted cases
three-quarters of fall-related admissions
and bunk beds from regulatory authorities and labeling, and consumer information. and 10,615 ED presentations with an annual
(73%) and ED presentations (73%) were for
suggested merit in updating the injury profiles. The Standard required that all recreational average of 355 admissions and 1,179 ED
children aged under nine years, and 49% and
In addition, the Australian standard for trampolines offered for sale on the Australian presentations.
50% respectively were for children aged under
trampolines is undergoing revision, making an market must be supplied with frame-
six years old.
updated profile particularly timely. Notable padding or a soft-edge system. It was also ED presentations climbed steadily in
increases in the frequency of button battery recommended that existing trampolines frequency each year over the study period
Button Batteries related injury and an increasing awareness of purchased prior to the release of the 2006 from 639 cases in 2002/3 to 1,711 cases in
the potentially serious nature of button battery Standard be retrofitted with a frame-padding 2010/11 (Figure 1a), whereas admitted cases
Button style batteries have been used in ingestion indicated a need to provide an injury system that complies with AS 4989 (Eager, followed a more staggered pattern but showed
a rapidly expanding range of common profile for this product type which has not 2007). A minimum level of consumer safety an overall increase from 293 in 2002/3 to 403
household items. They are often easy for been previously covered in Hazard. information was also mandated including in 2010/11 (Figure 1b).
children to access and their small size mean safety warnings on the trampoline packaging,
they are appealing to young children who may The profile for each product is presented The majority of hospital-treated trampoline Source: Victorian Admitted Episodes Dataset (VAED - hospital admissions)
instructions on installation, maintenance and
ingest these small items or insert them into separately, while the common datasets and safe use, including the need for active adult injuries were falls (97% admissions, 72%
their noses, or other body orifices, where they methods are summarized together. supervision. Further minor amendments were ED presentations). Among admissions, falls Forty-five percent of admissions and 41% of Children aged 0-4 years were the next most
can cause burns, hemorrhage, necrosis and life made in 2008 and 2010. dominated over the study period (Figure 1b). ED presentations occurred among children commonly injured group, representing 24%
threatening injury in as little as two hours. Among ED presentations, fall injury also aged 5-9 years. The predominance of children of admissions and 28% of ED presentations,
323 button batteries ingestions or insertions Trampoline Injury It was expected that the 2006 revisions to
the Standard would result in a reduction in
predominated, however the rate of increase in
non-fall injury presentations was greater than
in this age group was present for both fall (i.e.
both falls from the trampoline, falls onto the
followed by children aged 10-14 years (22%
of admissions and 23% of ED presentations).
were identified by VISU over a 12 year period, trampoline-related injury although it was not that for fall injury presentations (Figure 1a). suspension system or the frame), and non- There were 1,148 injured adults, aged 15 years
11% of which required admission to hospital. Karen Ashby and Lesley Day expected that the impact would be seen for fall (i.e. collisions with other persons, over- or older over the 9 year period, an average of
An overall increase in the frequency was several years, given the lifespan of existing Neither the VAED nor the VEMD data exertion injuries) (Table 1). 128 adults receiving hospital treatment for
observed. A third of the cases were children Introduction trampolines. Contemporaneously, trampolines provide sufficient information to definitively trampoline injuries per annum.
less than 2 years of age. Eighty-nine percent that have safety enclosure netting to minimise determine the style of trampoline implicated The mean age of the injured person was 9.0
of cases resulted from the child ingesting the In the 1990s, American Academy of Pediatrics
the risk of children falling off the equipment i.e. rectangle or round enclosed trampoline. years for admitted cases and 8.3 years for ED Males comprised 57% of admissions and 53%
battery. (AAP) called for the restriction of trampoline
to the ground —one of the most common The VEMD narratives suggest that less than presentations (Table 1). Non-fall injury had of ED presentations for trampoline injury, and
use in the United States to supervised training
mechanisms of injury— came onto the 1% of cases (n=39) were associated with mini- a slightly higher mean age at both levels of were particularly over-represented among
The ability of the child to access the battery programs, in response to the rising number of
Australian market. Unlike in the United States trampolines or rebounders, although their severity. admission for non-fall injury (64%) (Table 1).
readily and un-noticed requires attention to the serious paediatric trampoline-related injuries,
where the requirement for safety netting was involvement may not be consistently reported.
design of not only the battery, but the battery especially to the head and neck. The AAP
included in their American Society for Testing
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 2 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 3Circumstances and Outcomes 4-11 days). One each of head, internal organ • The pattern of injury across all body sites
Table 1 Hospital-treated trampoline injury, Victoria by age and gender, July 1, 2002 to June 30, 2011 and spinal injury accounted for the rest of the was similar among admissions and ED
of Injury
longest stays. presentations. Fall-related injury at both
The location of injury was unspecified for 70% Table 2 summarises the broad cause and type levels of severity were mostly associated
of admissions and 8% of ED presentations. of injury for hospital-treated trampoline- with injury to the upper limbs (67%
Of cases with a specified location, 87% of related injury for both fall and non-fall injury. admissions and 46% ED presentations),
admissions and 88% of ED presentations Key findings are: while non-fall-related injury was mostly
occurred in a home setting (own home or other associated with lower limb injury (38% of
persons home). A further 6% of admissions • Falls account for 97% of admissions and admissions and 56% of ED presentations)
reportedly occurred in areas for ‘sport and 72% of ED presentations. and the head and face (26% of admissions
recreation’ and another 4% of admissions and and 18% ED presentations).
2% of ED presentations occurred in ‘schools • Other causes of ED presentation include
or other public buildings’. over-exertion (13% of all trampoline– The single leading injury for fall admissions
related ED presentation) and collision with was fracture of the elbow and forearm
Eighty percent of admitted cases required a another person (6%). (n=1,300, 42% of all fall admissions). For
stay in hospital of less than two days, 19% non-fall admissions fractures of the knee and
required a stay of between two and seven • Fracture was the most common injury for lower leg were the leading injury (n=20, 25%
days and 1% (n=26) stayed 8-30 days. Most admissions accounting for 80% of fall and of non-fall admissions). For ED presentations
of the 26 patients with stays of 8-30 days 52% of non-fall-related admissions, and the leading fall-related injury was the same
(n=19, 73%) were for lower limb fracture and for 33% of fall-related ED presentations. as for admissions, fracture of the elbow
dislocation (range 8-24 days). A further three Dislocations and sprains/strains were the and forearm (n=1,097, 14% of all fall non-
long-stay cases (12%) were for upper limb most common non-fall ED presentation, admissions) and for non-falls the leading
Source: Victorian Admitted Episodes Dataset (VAED - hospital admissions)
Victorian Emergency Minimum Dataset (VEMD – ED presentations) fracture, dislocation and open wound (range followed by fracture. injury was dislocation, sprain and strain of the
ankle (n=503, 17%).
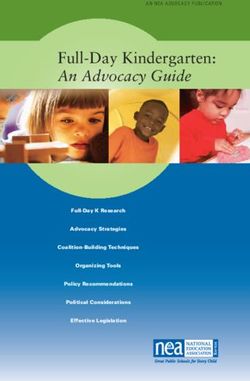
Figure 2 Figure 2: Trend in trampoline-related injury hospital admission rates
per 100,000 population, Victoria 2002/3 to 2010/11 Table 2 Hospital-treated trampoline injury profile, Victoria, July 1, 2002 to June 30, 2011
% Change Annual %
(95%CI) increase
27 (10, 46) 2.7%
101 (46, 159) 8.0%
71 (16, 140) 6.1%
149 (22, 345) 10.7%
NS NS
Source: Victorian Injury Surveillance Unit (VISU)
Rates and Trend Rates were increasing for all age groups, years), 2.7% (5-9 years), 9.4% (10-14 years)
except for those aged 20+ years (Figure 2). and 9.4% (15-19 years). For females aged 0-4
Figure 2 presents the trend in the rate of
The increasing trend was apparent for males in years the average annual percentage increase
hospital admissions for trampoline injury and *Suppressed due to small cell sizes
all age groups, except age 20+ years, and for was 6.5%.
clearly indicates that the 5-9 years age group Source: Victorian Admitted Episodes Dataset (VAED - hospital admissions)
females aged 0-4 years. The average annual
has the highest rate of admitted trampoline Victorian Emergency Minimum Dataset (VEMD – ED presentations)
percentage increase for males was 9.6% (0-4
injury.
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 4 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 5• Although in smaller numbers, increases
Table 3 ED treated trampoline injury by detailed cause group and severity, Victoria, July 1, 2002 to June 30, 2011 in “falls on” and “non-fall” injuries are Figure 4 ED-treated non-fall trampoline injury by cause, Victoria, July 1, 2002
noticeable from 2005/6, especially in ED to June 30, 2011
cases not admitted to hospital.
Further analysis of fall-related trampoline
injury is presented in a later section on the
impact of the Australian Standard. The
remainder of this section deals with non-fall
and other trampoline related injury issues.
Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations including admissions). Note NES = Not elsewhere specified. There were 3,237 injuries for causes other than
falls in the VEMD (220 admissions and 3,017
presentations) in the 9-year period 2002/3
Detailed external cause analysis Figure 3a ED presentations resulting in admission for trampoline injury by to 2010/11. The majority of these were for
detailed cause category and year, Victoria, July 1, 2002 to June 30, 2011 injuries associated with over-exertion while
Since falls are the major external cause of using the trampoline, including awkward
hospital treated trampoline injury further landings (n=1,498, 46% of non-fall injury
analysis was undertaken to elucidate more and 12% of all trampoline injury) (Figure Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations, includes admissions)
detail about the circumstances of the falls. 4). The age pattern of over-exertion injury is
The VEMD contains a free text narrative that similar to other trampoline injury (37% aged Figure 5a ED presentations resulting in admission for trampoline injury by detailed
allows further breakdown by detailed cause 5-9 years), however the gender pattern is quite cause category and main injury type, Victoria, July 1, 2002 to June 30, 2011
groups including the type of fall and categories different with females accounting for 56%
for non-fall injury. VEMD narrative analysis of over-exertion injury. The most common
was undertaken on both ED presentations and over-exertion injuries were sprains and strains
VEMD cases admitted to hospital. There is (n=816, 55% of all over-exertion injury) and
no narrative associated with the VAED so the ankle was the most commonly injured
this could not be performed for this dataset. body region (n=677, 45% of all over-exertion
Note that the number of ED admissions injury).
(n=1,653) does not match the VAED number
of admissions (n=3,199) as the VEMD is There were an increasing number of injuries
collected from a sample of 38 hospitals and occurring while attempting acrobatic
the VAED is a statewide collection. Thirteen manoeuvres, steadily increasing from 7 cases
percent of VEMD cases overall required an in 2003/4 to 53 cases in 2010/11. Injury
admission to hospital. whilst undertaking acrobatic manoeuvres
*Note: this figure is based on ED cases subsequently admitted as it is only the VEMD that allows further
breakdown of the narrative. NES = Not elsewhere specified. mostly occurred among males (69%) and
Table 3 shows that falls off the trampoline persons aged 10-14 years (46%, mean age =
Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations)
remain the leading cause of injury for both 12.8), and almost exclusively while doing a
VEMD admissions (62%) and presentations flip or tumble (96%). More than a third of Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations subsequently admitted)
(44%). For admitted cases, ‘fall on’ the Figure 3b ED presentations (non-admission), trampoline injury by detailed the injuries sustained when attempting such Note NES = Not elsewhere specified.
trampoline accounted for another 16% cause category and year, Victoria, July 1, 2002 to June 30, 2011 moves were neck injuries (n=73, 36%), of
of injuries and non-falls for 13%. For which three-quarters were sprains or strains or Figure 5b ED presentations (non-admission) for trampoline injury by detailed cause
presentations, non-falls represented 28% of other muscular injuries (n=55). category and main injury type, Victoria, July 1, 2002 to June 30, 2011
cases and ‘fall on’ injuries 19%.
Figures 5a and 5b depict the nature of main
Figures 3a & 3b show these cause categories injury of VEMD admissions and presentations
broken down by year and indicate that: by detailed cause of injury categories. Key
findings are as follows:
• All hospital treated trampoline injuries
have increased quite consistently over the • ‘Fall off’ injuries are predominantly
study period, particularly those treated in associated with fractures for both
the ED but not admitted to hospital. presentations (37%) and ED admissions
(81%).
• The trends in falls off the trampoline differ
from the trends for all trampoline injuries. • Two-thirds of ‘Fall on’ ED admissions were
For ED cases admitted to hospital, there for fractures, whereas one-third of ‘Fall on’
has been a departure from the same overall presentations were for dislocations, sprains
increasing trend from 2006/7 after which and strains. ‘Jump off’, ‘Fall NES (not
there has been a slight declining trend. For elsewhere classified)’ and ‘Non-fall’ injury
ED cases not admitted to hospital, the rate followed a similar pattern.
of increase has been much slower than that
Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations). Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations subsequently admitted)
for all trampoline ED cases not admitted to
Note NES = Not elsewhere specified. Note NES = Not elsewhere specified.
hospital, particularly from 2004/5.
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 6 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 7Results: impact of 1) Australian Standard: AS 4989-2003 It was anticipated that the 2006 Standard trampoline (influence of market-driven design
would result in a reduction in trampoline- modifications), and injuries associated with Figure 7 ED-treated spring and frame injury by year as a proportion of all trampoline
interventions to reduce The first Australian Standard, AS 4989– related injury, particularly injuries multiple-users (influence of Standard AS injury, Victoria, July 1, 2002 to June 30, 2011
injury 2003 Trampolines—Safety aspects from contact with rigid surfaces of the 4989-2006). Since data on trampolining
established requirements for components trampoline, the spring and frames. participation are not available, rates for the
The concept of the three Es: enforcement; and design and specified required different types of trampoline injury cannot
environment; and education are used in consumer information on assembly and 2) Market-driven design modifications be calculated to more accurately examine
injury prevention to describe the range of maintenance. Updated in 2006, the revised the impact of the Standards and market-
intervention efforts used to prevent injury. Standard focused on safety aspects: spring Concurrent to the Standards revisions in driven modifications. Here we examine
The first, enforcement, describes regulatory padding design; protection of sharp edges; the early 2000’s trampoline manufacturers trends in numbers of these types of injuries
or legislative change made to improve safety safety marking and labeling; and improved commenced selling “new” style in comparison with the trend in trampoline
and prevent injury. Environment relates consumer information. A key component trampolines that had safety nets in order injuries overall, as well as the trend in
to changing the environment, and includes was the requirement that trampolines be to reduce the risk of children falling off proportions.
design modification, to make a product supplied with frame-padding or a soft- the trampoline to the ground. Anecdotal
safer. Lastly education approaches deal with edge system. Retrofitting of spring and evidence from ED staff has suggested that Each of these three injury circumstances were
providing information to individuals in order frame-padding was also recommended. an unintended outcome of this modification reviewed using the available data. Given
to influence their behaviour to improve their has been an increase in collision injury the lack of narrative in the VAED, VEMD
safety. These three approaches are often A minimum level of consumer safety or other injury associated with multiple- admissions data, as well as ED presentation
most successful when used in conjunction, information was also mandated including users. data are reported. Figure 6 illustrates how
and indeed efforts at preventing trampoline safety warnings on the trampoline these categories relate to each other and it
injury have drawn on all three. Two major packaging, instructions on installation, With these two interventions in mind, further must be noted that they are not mutually
interventions worthy of assessment for any maintenance and safe use, including analysis of cause of injury categories may exclusive. For example, a person may collide
associated impact on the pattern of trampoline recommendations against allowing provide insight into any effects of these with another user of the trampoline (and be Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations, includes admissions)
injury are the introduction of an Australian multiple-users on the trampoline and the interventions. Three common injury scenarios counted as a multiple-user injury) but may
Standard for trampolines; and market driven need for active adult supervision. were further investigated to this end: injuries also then fall off the trampoline (and hence
design modifications to the trampoline. associated with frames and springs (influence also be counted as a ‘fall off). Spring and frame presentations were most severity levels, compared to proportions of
of Standard AS 4989-2006), falling off the common in children aged 5-9 years (n=219, 57% of all admissions and 53% of all non-
Impact of Australian Standard: 39%), as was the case for all trampoline admissions (Table 4).
Figure 6 Relationship between different injury circumstances associated with trampoline injury spring and frame injury (n=606) injury. However there was a higher proportion
of injury to children aged 10-14 years among Open wounds accounted for 38% of spring
The revised Standard AS 4989-2006 required spring and frame presentations (31%, n=176) and frame injury admissions and 35% of
that all trampolines be supplied with frame- compared to all trampoline injury (Table 4). non-admissions while representing just 4%
padding or a soft-edge system that covered This pattern held for admitted cases where the of admissions and 11% of non-admissions
Falls NES
840 the frame and springs of the trampoline. 10-14 year old age group accounted for 35% for all trampoline injury. Conversely there
Retrofitting of spring and frame-padding to of spring and frame admissions compared to are far fewer fractures and dislocation, sprain
existing trampolines was also recommended. 21% for all trampoline presentations. and strains among spring and frame injuries
Any impact of these requirements should compared to all trampoline injuries at both
be visible in the pattern of spring and frame Males were more highly represented making levels of severity (Table 4).
injury. up 60% of spring and frame injuries for both
Spring
Fall ON
and
There were 606 injury cases (5% of all VEMD
1,846 Figure 8 ED-treated injury related to multiple-users by year as a proportion of all
frame cases) where the free text mentioned the
346 trampoline injury, Victoria, July 1, 2002 to June 30, 2011
254 involvement of the springs, frame, edge or
4 2 metal part of the trampoline. Most (n=566,
93%) were presentations and 40 (7%) were
75 Collision Through admissions. More than two-thirds (69%) were
with person net
676 45 fall-related. Over the period 2002/3 to 2010/11
30
Multiple
there has been an 8.6% (95%CI 5.7%-10.8%)
45
jumper annual average increase in the frequency of
Fall from spring and frame injury, less than the overall
5,587 annual average increase of 12.6% (95% CI
10.3%-13.4%) for all trampoline injury. As
Over Exertion the confidence intervals for these estimates
1,453
overlap, this difference is not statistically
significant. It appears that any impact of the
2006 revision to the Standard on the trend in
Other the frequency of spring and frame injury has
1,050
been small to date. Figure 7 shows that as a
proportion of all trampoline injury over time,
spring and frame injuries decreased prior to
the 2006 revision to the Standard and there
has been no discernible trend in the proportion
Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations) since the Standard came into effect. Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations, includes admissions)
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 8 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 9Impact of Australian Standard: Figure 9 shows that falls off trampolines all trampoline falls. ‘Fall off’ injuries were
multiple-user injury (n=847) decreased as a proportion of trampoline mostly associated with fractures for both
injury during the study period. While the admissions (81%) and presentations (37%)
There were 847 injury cases (7% of all VEMD proportion has been decreasing, there has (Figures 5a and 5b).
cases) where the free text mentioned multiple- been, on average, an annual increase in the
users on the trampoline at the time of the frequency of 7.9% (95%CI 5.6%-9.5%). This There were proportionally more upper limb
injury. Most (n=793, 93%) were presentations is significantly less than the 12.6% (95% CI injuries in both admissions and presentations
and 64 (8%) were admissions. More than 10.3%-13.4%) average annual increase in all for falls off trampolines, compared to all
eighty percent (n=694, 81%) occurred when ED-treated trampoline injury. trampoline injury (74% vs. 63% for admissions
two or more, jumpers collided, another 7% and 52% vs. 37% for presentations. Fractures
occurred when the injured person was double The mean age of persons injured by a fall off of the elbow and forearms were the leading
bounced. Figure 8 shows that as a proportion a trampoline was younger than for trampoline injury for ‘falls off’ for both admissions
of all trampoline injury over time, multiple- falls overall (7.6 years vs. 8.0 years) and for (n=539, 53%) and presentations (n=806,
user injuries have increased. In addition, all trampoline injury (8.3 years). The sex and 17%).
the frequency of multiple- user injuries has nature of injury patterns were comparable to
increased by an average of 18.1% (95%CI
14.4%-18.8%) annually, significantly higher Figure 9 ED-treated falls off a trampoline injury by year as a proportion of all
than the all ED treated trampoline injury trampoline injury, Victoria, July 1, 2002 to June 30, 2011
ED-treated trampoline injury profile by selected causes, admissions and presentations, Victoria, July 1, 2002 to June 30, 2011
annual increase of 12.6% (95% CI 10.3%-
13.4%).
The pattern of multiple-user-related injury
shows some variation from that of all
trampoline injury. Young children aged 0-4
years represented a higher proportion of
multiple-user presentations (35%) compared
to all trampoline presentations (28%)
(Table 4).
Among admissions, dislocation and strain or
sprain injuries, neck injuries and lower limb
injuries were proportionally higher in multiple-
user events compared to all trampoline injury
events (Table 4).
Impact of market-driven
design modifications: falls off
trampolines (n=5,662)
Falls off trampolines to the ground or another Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations, includes admissions)
surface (n=5,662) represent 46% of all cases
reported in the VEMD (admissions and
Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations, includes admissions)
presentations) (Table 3). Although most
(82%) were presentations, the potential for
serious injury is great; they account for more
than 60% of admitted cases reported on the
VEMD. The AAP (2012) stated that a fall off
a trampoline is the most obvious of risks as
jumpers have the ability to propel themselves
to greater heights off a trampoline than from
a jump on the ground. The introduction of
enclosed trampolines should eliminate falls
off the trampoline, unless the zipper opening
is not secured or the netting or zipper is
compromised. In most instances a previous
incident that may have led to a fall off the
trampoline, should, on an enclosed trampoline,
result in a more benign collision with the net
with the user remaining on the surface of the
trampoline instead of falling to the ground.
*Suppressed due to small cell sizes
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 10
Table 4Discussion Falls off a trampoline remain the leading
cause of trampoline-related injury in Victoria,
children who are lighter, have less developed
coordination and lack necessary motor skills
knowledge and intervention regarding risk
behavior with trampoline use (AAP, 2012).
with the results being published in CHOICE
(Ciaramidaro, 2012). The 12 trampolines were
the cases identified in the VEMD are an
underestimate of the true number of cases
although they are decreasing as a proportion of for balance, estimating that the lightest person tested to the part of AS 4989:2006 that deals presenting to EDs.
Safe trampolining remains a persistent
all trampoline injury because their annual rate on the trampoline is 5-14 times more likely to The Victorian data also shows an increase in with requirements for areas of the trampoline
challenge. Over the study period an annual
of increase is not as great as for other causes be injured (Wootton and Harris, 2009; Bogacz, injuries sustained while attempting acrobatic where impact attenuation (padding) is VAED admissions data was selected by
average of 1,500 persons were treated in
of trampoline injury. This pattern is similar to 2012). The Victorian data shows that children manoeuvres and a predominance of older necessary. Testing involved dropping a 4.6kg a combined strategy of selecting for an
Victorian hospitals for an injury sustained
that reported in other Australian states (Sandler aged under five years are over-represented children being injured while doing flips and hemispherical head form from a height of 1.5 ‘External Cause’ code for falls alone and an
while using a trampoline. Despite the
et al, 2011) and in New Zealand (Chalmers et among multiple-user injuries. somersaults. This may also be linked to riskier metres and measuring the shock severity as ‘Activity’ code to account for non-fall injury.
strengthening of regulations, mandating of
al. 1994). Interestingly this is in contrast to behaviour while on the trampoline as the fear it impacted the padding or soft-edge system We assume this to be an accurate and total
safety information for owners and users,
reports from the northern hemisphere (US, The mandatory safety information included of falling from the trampoline (by child and in three different locations on each of the 12 picture of admissions recorded on the VAED.
and substantial design modifications to the
Canada and United Kingdom) where injuries in trampoline packaging that advises against parent) is dampened by the presence of nets. trampolines. Only one model tested passed
trampoline, both the frequency and population
rate of injury from trampoline use in Victoria
occurring on the body of the trampoline
predominate (Furnival et al. 1999; Alexander
multiple-users also states that trampolines
greater than 500 mm in height are not
Importantly there were higher proportions
of neck injuries reported among both the
in terms of the effectiveness of the spring
and frame-padding in preventing injury to the
Recommendations
continues to increase. Statistically significant
et al. 2010; Bogacz, 2009; Wootton and recommended for children aged less than six multiple-user and ‘attempted acrobatic’ injury child’s brain. Test failure indicates that in the The following recommendations relate to
increases in admission rates were observed for
Harris, 2009). This may be attributable to the years. Our current investigations shows that groups, a trend which should be monitored. case of a fall there is an unacceptable risk for the trampoline placement, assembly and
persons aged 0-4, 5-9, 10-14 and 15-19 years,
earlier recommendations for trampoline safety more than one-third of the injuries treated (35% While cervical spine injury is fortunately not potential injury to the child’s brain, a result maintenance, and to the safety features to look
for males in each of these age groups and
enclosures that have been part of the ASTM of admissions and 36% of ED presentations) the most commonly reported trampolining obtained for 11 of the 12 models tested. for in a trampoline and recommendations for
among females aged 0-4 years.
since 2003. Thus, in Victoria, the reduction were among children aged less than 6 years. injury, such injuries are the major cause of safe use. Many of these recommendations
Similar trends have been observed in other in “fall off” injuries is perhaps attributable Without complete details of the injury scenario neurological sequelae and death (AAP, 2012; Also of note are the reported decreases are drawn from the recent CHOICE article
developed nations. Chalmers et al. (1994) to the introduction of trampoline enclosures we can only speculate that, despite safety Leonard and Joffee, 2009; Chalmers et al. in quality and longevity of trampoline (Ciaramidaro, 2012).
reported a three-fold increase in the admission (nets). Other findings however may contend information to the contrary, parents perceive 1994). Leonard and Joffee (2009) and Furnival components. The International Trampoline
rate in New Zealand in the decade to 1998, against this. Examination of the effectiveness enclosed trampolines as safe for younger, and et al. (1999) note that cervical spine injuries Industry Association, as reported by Alexander Placement
Smith (1998) noted a 98% increase in child of frame-padding and enclosures in preventing multiple, users as the potential to fall off the frequently occur on the trampoline mat, rather et al. (2009), estimate that a trampoline sold
trampoline injury presenting to EDs in the injury was undertaken by Alexander et al. trampoline is eliminated. Some support for than from a fall off the trampoline, often when in 1989 had an expected life of 10 years; by • Ensure you have sufficient space for a
United States in the period 1990-1995, and (2010) using US data from 2002-2007. The this assumption is provided by Eager et al. failed flips or somersaults cause hyperflexion 2004 this had decreased to 5 years. Warranties trampoline. There should be a clearance
similarly Leonard and Joffe (2009) reported authors found that in the US there was no (2012a) who surveyed a customer dataset of or hyperextension of the cervical spine (AAP, for frames and mats are consistently longer of two metres on all sides and five metres
a 374% increase in child presentations to significant change in the downward trend of owners of one ‘soft edge’ model of trampoline 2012). Furnival et al. (1999) reported a strong than that for padding and enclosures with the overhead to avoid inadvertent contact with
EDs for trampoline injury in Canada over the ‘fall off injuries’ and insufficient evidence of a that had been designed to remove equipment- association between spinal injury and flips or expectation that these will be replaced during fixed structures such as walls, trees etc.
period 1990 to 1998. change in spring and frame injury, despite the related injury. The authors surveyed owners other complex mechanisms of injury (PSafety Features Maintenance Conclusion Chalmers DJ, Hume PA and Wilson BD.
(1994) ‘Trampolines in New Zealand:
• Ensure frame-padding is present to limit • Check the trampoline regularly for tears, a decade of injuries’. British Journal of
Trampolining is a fun way for children and
injuries from contact with the metal frame. worn areas and bending in the bed, frame Sports Medicine, 28; 4: 234-238.
adults to engage in active recreation, the
and safety enclosure. need for which is becoming increasingly
• Ensure netting is present and appropriately Ciaramidaro, R. (2012) ‘Trampoline reviews
important, and aids in the development of co-
assembled. • Inspect the frame and springs regularly for and safety tests’. CHOICE 12/12/2012.
ordination, balance and motor skills. Despite
surface rust, corrosion and deterioration. continuing efforts to improve the safety of
• Consider buying models that have safety Eager D. (2007) ‘Trampoline Standard AS
trampolines for users the overall number of
netting that assembles on the inside of • Rotate the safety padding to minimise 4989-2006’. Australasian Parks and
hospital- treated injuries continues to climb.
the padding system. This configuration degradation at the enclosure entrance and Leisure. Autumn: 7-8.
As we do not have participation rates for
reduces the likelihood of hitting the sun exposure if some parts are protected trampolining we cannot compare the injury
trampoline edges in the case of a fall. by shade during the day. This will increase Eager DB, Scarrott C, Nixon J and
risks of trampolining injury with other forms
the life of the padding. Alexander K. (2012a) ‘Injury survey of
of active recreation. Regulation and design
a non-traditional ‘soft-edged’ trampoline
Safe Use modification have progressed; however user
designed to lower equipment hazards’.
• Consider the benefits of retrofitting older behavior may adjust as a consequence with
trampolines with a frame padding system International Journal of Injury Control
• Trampolines are not recommended for an unintended relationship between safety
that is compliant with the current standard. and Safety Promotion, DOI:10.1080/1745
children under six years. developments and parents allowing increased
7300.2012.674041
risk-taking by users as parents perceive
• Before using, check that the area around Other Things to Consider trampolines to be safer for their children.
Eager DB, Scarrott C, Nixon J and Alexander
and under the trampoline is free from Of particular concern is the one-third of the
K. (2012b) ‘Survey of injury sources for
obstacles. • In-ground installation is an option to injured population who were younger than the
a trampoline with equipment hazards
reduce fall heights and possible injury. recommended minimum age for use who are
designed out’. Journal of Paediatrics and
• Discourage children from playing However digging in a trampoline will sustaining injuries sufficiently serious enough
underneath the trampoline, particularly involve quite a lot of preparation (for to require hospital treatment. The Australian
Child Health, 48: 571-581.
Bunk Bed Injury The current mandatory Australian Standard
for bunk beds (AS/NZS 4220) came into
while a jumper is using the trampoline. example, pit drainage is essential). Standard is currently under review and it will
Furnival RA, Street KA and Schunk effect in April 2005 (ACCC 2007). It covers
be important to ensure that any developments
JE. (1999) ‘Too Many Paediatric Emily Kerr and Lesley Day requirements for the construction, design and
• Ensure netting enclosures are zipped • NSW Fair Trading state that if a child be accompanied by an intensive education
Trampoline Injuries’. Pediatrics, 103; 5. labelling of bunk beds and states that:
closed while the user is on the trampoline is unable to get up independently onto campaign to raise the parental awareness of
Available at: www.pediatrics.org/cgi/ Introduction
to avoid falls through the unzipped door. the trampoline then they may not be at the risks associated with failing to maintain
content/full/103/5/e57 • All bunk beds must have permanently fixed
the right developmental stage to use a trampoline components and allowing risk Bunk beds comprise a set of components
guardrails on all four sides and ends, with
• Only allow one child at a time to use the trampoline, hence access via a ladder taking use. assembled into beds that are stacked one over
Leonard H and Joffe AR. (2009) ‘Children a minimum distance of 260mm between
trampoline to avoid collision and other should be restricted. The opposing view the other, or are elevated beds where the top
presenting to a Canadian hospital with the upper surface of the mattress base and
injury associated with multiple-users. is that a ladder could be a useful aid to of the mattress base is at 800mm or more
help children get on and off a trampoline Acknowledgements trampoline-related cervical spine injuries’.
Paediatrics and Child Health, 14; 2: 84-88.
above floor level (Australian Competition &
the upper surface of the guardrail;
• Set, maintain and enforce clear safety safely, but it should be removed when the Consumer Commission (ACCC) 2012a). They
We would like to thank Associate Professor • There must not be any gaps large enough
rules: “one at a time,” “bare feet only,” trampoline is not in use as this will remove are often used in children’s bedrooms, as they
David Eager from the University of Morrongiello BA and Major K. (2002) to trap a child’s head or limbs;
and “do not use when wet” are good the risk of unsupervised access to the allow for more floor space.
Technology Sydney for reviewing this article ‘Influence of safety gear on parental
boundaries to establish. trampoline.
prior to publishing. perceptions of injury risk and tolerance for • There must be no protrusions from the
Bunk beds are an injury risk for young
children’s risk taking’. Injury Prevention, bunk bed measuring over 8mm which may
• Supervise children while they are using children, in particular if the bunk bed is used
Further Research 8: 27-31.
inappropriately (e.g. for playing) or if it has
snag a child’s clothing; and
the trampoline.
While surveillance data provides us with
References Sanders G, Nguyen L, Lam L, Manglick MP,
been poorly made. Initial research into bunk
• Bunk beds must come with a marking
• Encourage use of the middle of the bed injury came about after a number of
a good minimum count of the number of Alexander K, Eager D, Scarrott C and Soundappan SV and Holland AJA (2011) indicating the maximum mattress height
trampoline mat for safe jumping and climb fall-related fracture injuries were reported,
persons injured, further research is required Sushinsky G (2010) ‘Effectiveness of pads ‘Trampoline Trauma in Children: Is It on the upper bunk bed when the height of
rather than jumping off the trampoline as well as some cases of asphyxiation due
to better understand the issues associated and enclosures as safety interventions on Preventable?’. Pediatric Emergency Care, the guardrail is less than 360mm.
when finished. to entrapment in the bunk bed (Watson et al
with continuing increases in trampoline injury consumer trampolines’. Injury Prevention, 27; 11: 1052-1056.
1997). Falling is the leading cause of injury
numbers. Areas worthy of further research 16: 185-189. Product Safety Australia generally
• Don’t let jumpers bounce against the hospitalisation among children in Victoria, and
include: the gathering of population exposure Smith GA. (1998) ‘Injuries to Children in recommends against children under nine years
netting intentionally. falls from beds or chairs are the second most
data to apply injury rates to hours of use; American Academy of Paediatrics (2012) the United States Related to Trampolines, old using an upper bunk bed, and definitely
frequent type of fall among young children
and a follow-up study of people injured on ‘Trampoline Safety in Childhood and 1990-1995: A National Epidemic’. advises against the use of these beds for
• Teach your child to focus their eyes on the (Ashby & Corbo 2000). Fall injuries are the
trampolines to ascertain the type of trampoline, Adolescence’. Pediatrics, 130; 4: 774- Pediatrics, 101; 3: 406-412. children under six years old (2012a).
trampoline as a means of controlling the most common type of bunk bed injury (Barker
the extent to which the trampoline meets the 779. Changes to hospital data coding have
bounce. et al 2008), and children can suffer serious
relevant Standard and the general condition of Wootton M and Harris D. (2009) enhanced our ability to specifically monitor
injury from falling from the top bunk. Other
the trampoline. American Academy of Paediatrics (1999) ‘Trampolining injuries presenting to bunk bed-related injury and hence, this Hazard
• Do not attempt or allow advanced serious bunk bed-related injury can occur if a
‘Trampolines at Home, School and a children’s emergency department’. article examines the patterns of, and trends in,
acrobatic manoeuvres such as somersaults child gets caught between gaps in and around
Recreational Centers’. Pediatrics, 103; 5: Emergency Medicine Journal, 26: 728-731 hospital-treated bunk bed injury in Victoria
or flips. Inverted manoeuvres should the bunk bed, and injury can also occur if bunk
1053-1056. during the period July 2006 to June 2011.
only be attempted under trained adult beds are placed in rooms with low ceilings, as
supervision. children may hit the ceiling or be struck by fan
Bogacz A. (2009) ‘Trampoline injuries: how
blades (Barker et al 2008).
to avoid injury’ [letter]. British Medical
Journal, 338: b2197.
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 14 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 15Table 1 Hospital-treated bunk bed injury in Victoria by year, July 1, 2006 to June 30, 2011
Method
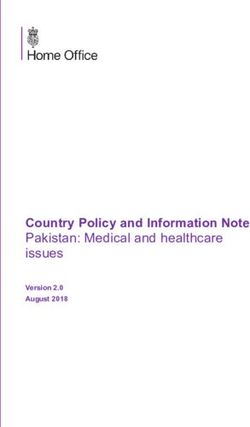
Figure 1 Trend in bunk bed-related injury hospital admission rates per 100,000
Data were extracted from the Victorian population, Victoria 2006/7 to 2010/11
Admitted Episodes Dataset [Victorian hospital
admissions] and the Victorian Emergency
Minimum Dataset [emergency department
presentations to 39 Victorian hospitals] for
the financial years 2006/7 to 2010/11. See
Box 1 for details of the data sources and case
selection.
Results
Frequency
Over the five-year period 2006/7 to 2010/11
there were 1,491 bunk bed-related injury
cases identified in Victorian hospitals. These
comprised 362 hospital admitted cases
Source: Victorian Admitted Episodes Dataset (VAED - hospital admissions)
and 1,129 emergency department (ED)
Victorian Emergency Minimum Dataset (VEMD – ED presentations)
presentations (excluding admissions), with an
annual average of 72 admissions and 226 ED
Table 2 Hospital-treated bunk bed injury in Victoria by age and gender, July 1, 2006 to June 30, 2011 presentations over the five years (Table 1). Source: Victorian Admitted Episodes Dataset (VAED – hospital admissions)
There was a general increase in the frequency
of admitted cases over the study period, while mean age for non-fall-related ED presentations • The location of injury was unspecified
there was no clear trend for ED presentations. was higher, at 11.7 years. There were 145 for 23% of admissions and 4% of ED
adults injured (aged 15 years or older) over the presentations. Of cases with a specified
The admissions (VAED) dataset only has a five-year period, an average of 29 per annum. location, 90% of both admissions and ED
code for falls from bunk beds; however the presentations occurred in a home setting
ED dataset (VEMD) has a text “description of Males comprised 58% of admissions and 54% (own or other person’s home).
injury event” variable which can be searched of non-admissions for bunk bed injury (Table
for any injury involving a bunk bed and thereby 2). • Fracture was the most common injury
allowing analysis of the type of injury event. among fall-related admissions and ED
Of ED presentations for bunk bed-related
Rates and Trend presentations, accounting for 58% of
injury, 87% were fall-related, including falls admissions and 26% of ED presentations.
from the bunk bed, jumps off the bunk bed, For non-fall-related ED presentation cases,
Figure 1 presents the trend in the rate of
and being pushed or pulled off the bunk bed. open wounds were the most common
hospital admissions for bunk bed injury.
Non-fall injuries included: collisions with or injury type (45%).
The 5-9 year age group had the highest rate
striking the bunk bed; being struck by part of
of admitted bunk bed injury. There were no
the bunk bed or by a ceiling fan (when on top • Among fall-related bunk bed injury
statistically significant trends in bunk bed
of bunk); or being caught or jammed in the admissions, the upper limb was the
injury admission rates over the five-year
bunk. most commonly injured body region,
period.
accounting for 49% of admitted cases.
Among admissions, children (aged 0-14 Among fall-related ED presentations,
years) accounted for 89% of cases, with the
Circumstances and outcomes of
injury the head or face was the most commonly
highest number involving children aged four injured body region (36%), followed by
years and five years (both 12% of admitted the upper limb (35%). Among non-fall-
cases) (Table 2). Table 3 summarises the cause and type of
related ED presentations, the head or face
injury for hospital-treated bunk bed injury for
was the most commonly injured body
Among fall-related ED presentations, children both fall and non-fall injury. Key findings are:
region (57%).
accounted for 92% of all cases; however it
was two-year-olds (13%), four-year-olds • Falls accounted for 87% of ED
• 84% of admitted cases required a hospital
(12%) and three-year-olds (10%) that were presentations identified as being associated
stay of less than two days.
most commonly injured. Among non-fall- with bunk beds.
related ED presentations, there were higher
proportions of injury to the older age groups • Of the 147 non-fall-related ED presentation
(Table 2). cases, 66% were caused by being struck by
or colliding with an object and 16% were
*Suppressed due to small cell sizes caused by a cutting or piercing object.
The mean age of the injured person was 9.7
Source: Victorian Admitted Episodes Dataset (VAED - hospital admissions) years and 7.7 years for admitted cases and fall-
Victorian Emergency Minimum Dataset (VEMD – ED presentations, non-admissions)
related ED presentations respectively. The
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 16 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 17Table 3 Hospital-treated bunk bed injury profile, Victoria, July 1, 2006 to June 30, 2011
**Note: This table includes ED cases subsequently admitted as it is only the VEMD that includes a narrative which allows further breakdown of external cause.
ED-treated bunk bed injury by detailed cause and nature of main injury, Victoria, July 1, 2006 to June 30, 2011
*Suppressed due to small cell sizes
Source: Victorian Admitted Episodes Dataset (VAED - hospital admissions)
Victorian Emergency Minimum Dataset (VEMD – ED presentations, non-admissions)
Source: Victorian Emergency Minimum Dataset (VEMD – ED presentations, includes admissions)
The single leading injury for fall-related number of admissions (n=362) as the VEMD (20%). Among ED admissions, falls from
admissions was fracture of the elbow and is only collected from a sample of 38 hospitals the bunk most commonly resulted in
forearm (n=117, 32% of all fall admissions). and the VAED is a state-wide collection. fractures (57%) and intracranial injuries.
For all (fall and non-fall-related) ED
presentations, open wounds to the head Table 4 shows the detailed cause of injury • Among non-fall ED presentations
were the leading injury (n=114, 12% of all categories and the associated nature of (n=147), the specified causes of injury
fall presentations; n=52, 35% of all non-fall main injury of VEMD admissions and ED were colliding with or striking the bunk
presentations). presentations for bunk bed-related injury. Key bed (e.g. running into the bunk bed) (65%),
findings are as follows: being struck by part of the bunk bed (e.g.
Detailed analysis: external cause part of bunk bed falling onto person)(9%),
• Among both ED presentations (non- being caught or jammed in the bunk bed
There is no narrative available in the VAED admissions) and admitted cases, the (7%) , and being struck by a ceiling fan
so VEMD narrative analysis was undertaken leading cause of injury was a fall from a (5%).
on all ED presentations including admitted bunk bed (87% overall; 80% and 91%
cases, to allow description of external cause to respectively). • Among ED non-fall presentations,
a more detailed level than that possible when colliding with or striking the bunk bed
relying on the routinely available external • Among ED presentations, falls from the most commonly resulted in open wounds
cause codes. Note that the number of ED bunk most commonly resulted in fractures (48%), superficial injuries (16%) and
*Suppressed due to small cell sizes
admissions (n=169) does not match the VAED (26%) and dislocations, sprains and strains dislocations, sprains and strains (12%).
VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 75 page 18
Table 4You can also read