Correlation between Prostate-Specific Antigen Kinetics and Overall Survival in Abiraterone Acetate-Treated Castration-Resistant Prostate Cancer ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Cancer Therapy: Clinical Clinical
Cancer
Research
Correlation between Prostate-Specific Antigen
Kinetics and Overall Survival in Abiraterone
Acetate–Treated Castration-Resistant Prostate
Cancer Patients
Xu S. Xu1, Charles J. Ryan2, Kim Stuyckens3, Matthew R. Smith4, Fred Saad5,
Thomas W. Griffin6, Youn C. Park1, Margaret K. Yu6, An Vermeulen3,
Italo Poggesi3, and Partha Nandy1
Abstract
Purpose: We constructed a biomarker-survival modeling populations. The model-based posttreatment PSADT had the
framework to explore the relationship between prostate-specific strongest association with OS (HR 0.9 in both populations).
antigen (PSA) kinetics and overall survival (OS) in metastatic The models could accurately predict survival outcomes. After
castration-resistant prostate cancer (mCRPC) patients following adjusting for PSA kinetic endpoints, the treatment effect of AA
oral administration of 1,000 mg/day of abiraterone acetate (AA). on survival was no longer statistically significant in both studies,
Experimental Design: The PSA-survival modeling framework and the Prentice criteria of surrogacy were met for the PSA kinetic
was based on data from two phase III studies, COU-AA-301 (che- endpoints. A strong correlation was also observed between PSA
motherapypretreated,n¼ 1,184)andCOU-AA-302(chemotherapy and radiographic progression-free survival.
na€ve, n ¼ 1,081), and included a mixed-effects tumor growth Conclusions: The analysis revealed a consistent treatment
inhibition model and a Cox proportional hazards survival model. effect of AA on PSA kinetics and strong associations between PSA
Results: The effect of AA on PSA kinetics was significant (P < kinetics and OS in chemotherapy-pretreated and -na€ve patients,
0.0001) and comparable between the chemotherapy-na€ve and thereby providing a rationale to consider PSA kinetics as surrogacy
-pretreated patients. PSA kinetics [e.g., PSA nadir, PSA response endpoints to indicate clinical benefit in AA-treated patients with
rate (30%, 50%, and 90%), time to PSA progression, PSA mCRPC regardless of chemotherapy treatment. Clin Cancer Res; 1–8.
doubling time (PSADT)] were highly associated with OS in both 2015 AACR.
Introduction Abiraterone acetate (AA) is the prodrug of abiraterone, a first-
in-class therapy that selectively and irreversibly inhibits 17a-
Prostate cancer, especially metastatic castration-resistant
hydroxylase/C17, 20-lyase [cytochrome P450C17 (CYP17)], a
prostate cancer (mCRPC; ref. 1), accounts for a large proportion
key enzyme in androgen biosynthesis (3, 4). Abiraterone sup-
of the global cancer burden (2). As androgen signaling remains
presses adrenal and tumoral androgens, resulting in undetectable
important to mCRPC progression, androgen suppression ther-
serum testosterone concentrations (3–6). AA plus prednisone has
apy remains a rational therapeutic approach. Questions, how-
been shown to improve overall survival (OS) and radiographic
ever, remain about how to more accurately predict therapeutic
progression-free survival (rPFS) in patients with chemotherapy-
benefit and long-term survival outcomes for patients with
pretreated (study COU-AA-301) or chemotherapy-na€ve (study
mCRPC.
COU-AA-302) mCRPC (7–9).
The surrogacy and predictive performance of prostate-spe-
cific antigen (PSA) kinetics in mCRPC patients has not been
1
Janssen Research & Development, Raritan, New Jersey. 2Helen Diller established and contradictory findings have been reported (10–
Family Comprehensive Cancer Center, University of California, San 15). However, the previous evaluations were based mainly on
Francisco, California. 3Janssen Research & Development, Beerse,
Belgium. 4Harvard Medical School, Massachusetts General Hospital the data from studies for treatment of mCRPC with che-
Cancer Center, Boston, Massachusetts. 5University of Montreal, Mon- motherapies. The significant antitumor effect of AA confirms
treal, Quebec, Canada. 6Janssen Research & Development, Los that mCRPC remains hormonally driven and dependent on
Angeles, California.
androgen receptor signaling (16). Because PSA kinetics may be
Note: Supplementary data for this article are available at Clinical Cancer related to activity at the androgen receptor (17), the data (i.e.,
Research Online (http://clincancerres.aacrjournals.org/).
PSA, and clinical outcomes) collected in two phase III studies,
Corresponding Author: Xu S. Xu, Janssen Research & Development, US 920 COU-AA-301 and COU-AA-302, provided a unique opportu-
Route 202, Raritan, NJ 08869. Phone: 908-927-4979; Fax: 908-203-1527; nity to apply quantitative modeling to understand the interplay
E-mail: sxu26@its.jnj.com
between kinetics of PSA following treatment and survival in
doi: 10.1158/1078-0432.CCR-14-1549 mCRPC patients following treatment with AA, a noncytotoxic
2015 American Association for Cancer Research. agent.
www.aacrjournals.org OF1
Downloaded from clincancerres.aacrjournals.org on March 12, 2021. © 2015 American Association for Cancer
Research.Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Xu et al.
PSA kinetic model
Translational Relevance A longitudinal PSA kinetic model was developed to describe
As cancer is a heterogeneous disease, it may be difficult to PSA kinetics, the antitumor effect of abiraterone, and treatment
demonstrate survival advantage with novel agents. Modeling resistance after AA administration. The models were developed
analysis may be useful to predict treatment effect of cancer using data from patients who received at least one dose of study
agents by contributing to the understanding of the underlying drug and for whom a minimum of one post-treatment PSA
disease and determining who may derive clinical benefit. On measurement was available. Initial analysis showed that a
the basis of a biomarker-survival model of the data from two tumor growth inhibition model (18–21) best described the
pivotal metastatic prostate cancer phase III trials of abiraterone longitudinal pharmacodynamic PSA response instead of a
acetate, the first-in-class androgen biosynthesis inhibitor, we biexponential model (22), a mixed exponential and linear
show that survival outcomes can be adequately predicted model (23), or a mixed Weibull and linear model (23, 24).
through prostate-specific antigen (PSA) kinetics and that the Details on this model are in Supplementary Appendix SI
Prentice criteria for surrogacy were met for these PSA kinetic (Supplementary Table S1).
endpoints. This model also suggests possible novel
approaches to PSA beyond its routine use as an intermediate Survival model
biomarker, that is, considering PSA kinetics as an early readout Cox proportional hazards (PH) analyses were performed
at interim/futility analysis to indicate clinical benefit in met- using the survival package in R 2.14.0 (25). Univariate Cox
astatic prostate cancer patients treated with agents whose models were developed for individual model-predicted PSA
activity is dependent on androgen receptor signaling. kinetic endpoints. Multivariate Cox PH models were con-
structed from selected PSA kinetic endpoints and baseline
covariates. Prentice criteria (26) for surrogacy were evaluated
using the methods previously described (27). As rPFS was the
We constructed a biomarker-survival modeling framework to coprimary endpoint in COU-AA-302, the association between
link OS with PSA kinetics following AA administration in patients PSA endpoints and rPFS was also explored using univariate Cox
with mCRPC. PH models. For the COU-AA-301 and -302, PSA kinetics were
estimated separately. Details of this analysis are in Supplemen-
tary Appendix SII.
Materials and Methods
Study design and data collection
COU-AA-301 and COU-AA-302 were phase III, multicenter, Results
randomized, double-blind, placebo-controlled studies evaluating PSA kinetic model
the efficacy and safety of 1,000 mg daily AA plus 5 mg twice-daily The PSA kinetic model provided an overall excellent adherence
prednisone (abiraterone arm) versus placebo plus prednisone to individual PSA concentrations, indicated by a diagnostic plot of
(prednisone arm) in chemotherapy-pretreated and -na€ve patients the observed and predicted PSA concentrations for individual
with mCRPC, respectively. In COU-AA-301, 1,195 patients were subjects (Supplementary Fig. S1) as the data are uniformly and
randomized (2:1) into the abiraterone and prednisone arms, closely distributed around the line of identity. The parameter
whereas in COU-AA-302, 1,088 patients were randomized estimates of the final PSA kinetic models for chemotherapy-
(1:1). Patients were kept on study treatment until radiographic pretreated and -na€ve patients are listed in Supplementary Table
or clinical evidence of disease progression. Per protocol, PSA S1. On the basis of the model, the estimated drug effect (AA þ
progression was not used as the sole indicator for disease pro- prednisone vs. prednisone) was similar in both populations.
gression or as a criterion for treatment discontinuation. Compared with prednisone alone, treatment effect of AA on the
For COU-AA-301, the scheduled PSA measurements were PSA kinetics increased by 1.21-fold (0.93–1.53) and by 1.44-fold
conducted at screening, every three cycles (day 1 of cycles 1, 4, (1.14–1.77) for chemotherapy-pretreated and -na€ve patients,
7), and at the end-of-treatment visit. For COU-AA-302, PSA respectively.
measurements were taken at screening, day 1 of cycles 1, 3, 5, 7, A wide range of model-predicted PSA summary endpoints
and 10, every three cycle after cycle 10, and at the end-of- based on the PSA kinetic model (Supplementary Appendix SI)
treatment visit. The median number of cycles of AA treatment were derived to explore the relationship between OS and PSA
given was 8 and 15 for COU-AA-301 and COU-AA-302, respec- kinetics. In addition, PSA response rates (30, 50, and 90%)
tively. Serum PSA concentrations were assessed, with a median based on the observed data were investigated. The descriptive
of three and six measurements (range, 1–13 measurements) statistics of these PSA endpoints are summarized in Table 1.
collected per patient. No PSA values were collected after pro- Predicted PSA response rates 30, 50, and 90% at week 12
gression on either of the clinical trials. The COU-AA-301 and were greater in the abiraterone versus prednisone arms for
COU-AA-302 datasets contained 552 (46.2%) and 333 both chemotherapy-na€ve and -pretreated patients as well
(30.6%) mortality events, respectively. as with other PSA response endpoints evaluated [e.g., max-
Details on the study designs have been described previously imal% PSA decline, time to PSA nadir, time to progression by
(7, 9). Patients with neuroendocrine differentiation were explic- both the PSA Working Group 1 (PSAWG1) and Prostate
itly excluded from these studies. Both studies were approved by Cancer Working Group 2 (PCWG2) criteria, PSA nadir dou-
the Institutional Review Boards of the participating institutions bling time and PSA doubling time from baseline (PSADT),
and were conducted in accordance with the ethical principles of observed PSA response rate (30, 50, and 90%)]. PSA value at
the World Medical Association Declaration of Helsinki. All the end of treatment was higher (203.9 641.0 vs. 757.1
patients provided written informed consent. 1,389.8 for chemotherapy na€ve vs. -pretreated, respectively)
OF2 Clin Cancer Res; 2015 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on March 12, 2021. © 2015 American Association for Cancer
Research.Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Abiraterone PSA-Survival Model Predicts Survival Outcomes
Table 1. Summary statistics of model-predicted and observed PSA kinetic endpoints
Chemotherapy-na€ve Chemotherapy-pretreated
Prednisone (n ¼ 539) Abiraterone (n ¼ 542) Prednisone (n ¼ 394) Abiraterone (n ¼ 790)
Maximum% PSA decline 25.5 33.1 64 35.6 9.2 21.1 37.6 37.8
Time to PSA nadir (mo) 2.6 3.8 5.6 5.2 0.9 1.8 2.9 2.7
Nadir PSA value (ng/mL) 99.6 236.4 50.7 172.6 357.4 681.8 257.6 581.5
PSA response rate at wk 12 (30%), n (%) 167 (31.0) 400 (74.2) 64 (11.9) 247 (45.9)
PSA response rate at wk 12 (50%), n (%) 112 (20.8) 343 (63.7) 38 (7.1) 185 (34.3)
PSA response rate at wk 12 ( 90%), n (%) 23 (4.3) 119 (22.1) 4 (0.8) 67 (12.5)
Time to PSA progression (mo)a 8.7 9.6 16.7 16.1 4.0 4.3 7.8 6.1
Time to PSA progression (mo)b 7.0 7.7 13.8 13.8 3.4 3.2 6.5 5.0
PSA nadir doubling time (mo) 7.7 8.5 12.4 9.1 5.9 3.6 8.5 4.2
PSA doubling time from baseline (PSADT) (mo) 13.2 13.6 25.2 22.4 6.8 5.6 12.8 9.8
PSA value (EOT; ng/mL) 203.9 641 101.7 288.3 757.1 1,389.8 504.0 1,035.6
PSA response rate (30%), n (%)c 164 (30.4) 377 (69.9) 46 (8.6) 197 (36.5)
PSA response rate (50%), n (%)c 129 (24) 334 (62) 30 (5.6) 158 (29.4)
PSA response rate (90%), n (%) c
41 (7.6) 167 (31) 7 (1.3) 74 (13.8)
Abbreviation: EOT, end of treatment.
a
PSA progression defined by PSAWG1; defined as a 50% increase in PSA above nadir for patients who experienced a PSA decline of 50% on treatment, a 25% increase
in PSA above nadir for patients who experienced a PSA declinePublished OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Xu et al.
Table 3. Final multivariate Cox PH model for OS
Prognostic factor HR (95% CI) P Partial R2 (%)
Chemotherapy-na€ve
Predicted posttreatment PSADT (mo) 0.90 (0.88–0.92)Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Abiraterone PSA-Survival Model Predicts Survival Outcomes
Table 4. Treatment effect after adjusting for PSA endpoints
Chemotherapy-na€ve (n ¼ 1,081) Chemotherapy-pretreated (n ¼ 1,184)
HR (95% CI) P HR (95% CI) P
Maximum% PSA decline 1.37 (1.08–1.75) 0.01 1.09 (0.92–1.31) 0.3
Time to PSA nadir (mo) 1.59 (1.25–2.01)Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Xu et al.
breast cancer (23, 31) to predict the impact of drug activity on AA on 31 PSA kinetics in the two populations, and revealed a
survival and to examine study designs before the start of expensive strong association between PSA kinetics and survival in both
trials. Therefore, methods of connecting treatment use and expo- populations. Also, the effect of AA on survival was no longer
sure to survival outcomes early on may benefit the therapeutic statistically significant after adjusting for most PSA kinetic
decision-making process. As the mechanism of action of abirater- endpoints in both studies. Therefore, the Prentice criteria were
one involves the disruption of androgen signaling, PSA kinetics is met for those PSA endpoints in both chemotherapy-pretreated
a rational readout for patient outcomes, further validated by and -na€ve populations.
similar associations observed between PSA and OS in chemo- In a recent analysis of the TROPIC trial, a phase III trial of
therapy-pretreated and -na€ve patients in this analysis, and by cabazitaxel in patients with mCRPC with prior docetaxel expo-
good predictive performance of survival outcome with PSA as the sure, Halabi and colleagues noted that PSA kinetics (e.g., 50%
intermediate biomarker. PSA declines) failed to satisfy the Prentice criteria (14). Halabi and
Although surrogacy of PSA metrics as a clinical endpoint has colleagues explained that the benefit of cabazitaxel in improving
not been established (10–13), PSA is routinely used as an inter- OS may not be mediated through PSA-dependent mechanisms.
mediate biomarker, and posttreatment changes in PSA have been As a direct inhibitor of androgen biosynthesis rather than a
associated with OS in mCRPC clinical trials (26, 27, 29, 32–36). cytotoxic chemotherapy, abiraterone may have a more PSA-
Current survival models confirm that PSA kinetics are an inter- dependent mechanism than cabazitaxel, as PSA kinetics may be
mediate endpoint predictive of OS in both chemotherapy-pre- related to activity at the androgen receptor (17). In other words,
treated and -na€ve patients with mCRPC following AA adminis- changes in PSA kinetics may be a direct consequence of the clinical
tration. Multiple commonly used PSA summary measures can be activity of AA. Our analysis of the Prentice criteria further supports
derived from longitudinal measurements. It is not surprising that this hypothesis regarding the PSA-dependent mechanism of
PSA endpoints that include later progression phase (e.g., PSADT) abiraterone.
tend to have stronger correlation with OS as they may carry richer In chemotherapy-na€ve patients, a significant, but opposite
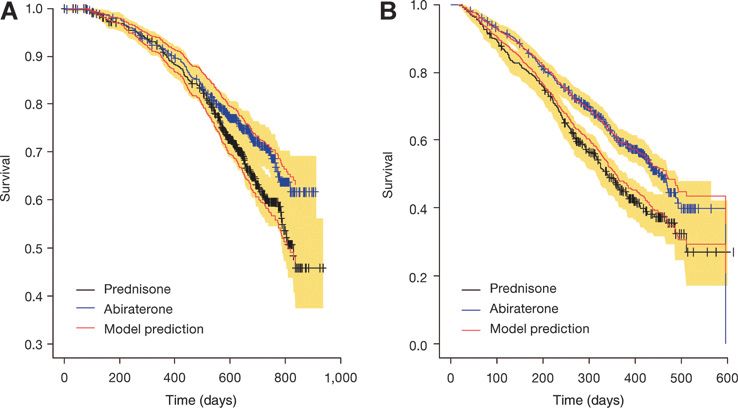
and more complete prognostic information for survival. Howev- treatment effect (i.e., HR >1) remained after adjusting for six PSA
er, the time needed to capture the later progression phase is endpoints (four PSA progression measures, time to PSA nadir, and
usually quite long and does not allow for an early readout. PSA nadir), indicating that these PSA endpoints may slightly
Although PSA response endpoints represent only part of the overpredict the treatment effect in COU-AA-302. For example,
information available in the longitudinal data (e.g., the initial Fig. 1 shows that the treatment effect was slightly overpredicted by
declining phase due to treatment; refs. 10, 12), they may provide PSADT between days 200 and 600 in COU-AA-302. The treatment
early indication of magnitude of long-term survival benefit. The effect on OS in COU-AA-302 might be confounded by switching
current analysis suggests that the PSA response endpoints were therapies after radiographic progression, since more patients in
sufficient to explain the variability in OS due to the treatment the prednisone arm (74%) than in the abiraterone arm (59%)
effect (Table 4 and Supplementary Fig. S1) although their corre- received subsequent therapies. The use of subsequent therapies
lation with OS was not as strong as that of PSADT and time to PSA may reduce the size of the expected effect of the therapies being
progression (Table 2). PSA response rates have been utilized as an evaluated (7, 9, 39, 40) and therefore may explain the model
early readout of clinical benefit at interim/futility analysis of overprediction and the opposite treatment effect after adjusting
phase III clinical trials for novel investigational agents for treat- for some PSA endpoints.
ment of patients with metastatic prostate cancer (37). It should be rPFS by PCWG2 criteria has been commonly used as a key
mentioned that early PSA flare/rise may occur in some patients endpoint in recent phase III trials (41). Along with OS, rPFS was
after AA treatment (38). PCWG2 recommends evaluating PSA the coprimary endpoint in study COU-AA-302 (9, 41, 42).
response after 12 weeks (29). The model-based analysis generated Previous analysis of COU-AA-302 data has shown a strong,
additional useful data for further evaluation of PSA surrogacy positive correlation (0.72) between rPFS and OS using Spear-
using meta-analysis. The PSA kinetic model suggests a similar man correlation coefficient estimated through the Clayton
treatment effect on PSA kinetics for patients with different treat- copula, which takes censoring into account (41). A recent study
ment experiences (chemotherapy-pretreated vs. -na€ve). The treat- suggested that rPFS was significantly associated with OS in
ment effects on OS were also similar for the chemotherapy- patients with mCRPC receiving first-line docetaxel-based che-
pretreated (HR, 0.65; 95% CI, 0.54–0.77; P < 0.0001; ref. 7) and motherapy or post-docetaxel therapy (43). Our present analysis
-na€ve (HR, 0.75; 95% CI, 0.61–0.93; P ¼ 0.0097) patients (9), also suggests that PSA kinetics had a stronger association with
indicating that PSA kinetics may have value as a surrogate end- rPFS than with OS. Therefore, PSA kinetics (e.g., PSA response
point (18). rates) could be an early indication of long-term clinical benefit
Prentice has proposed a set of statistical conditions ("Pren- for both rPFS and OS.
tice criteria"; ref. 26) for demonstrating surrogacy using data In summary, we identified a consistent effect of AA on PSA
from a single study. This includes the caveats that the treatment kinetics and strong associations between PSA kinetics and OS
must have a statistically significant effect on the biomarker in chemotherapy-pretreated and -na€ve patients. Simulations
endpoint and on survival; the biomarker endpoint must be showed that the PSA-survival model could reasonably predict
statistically significantly prognostic for survival; and, in a mul- the survival outcome in studies COU-AA-301 and COU-AA-302.
tivariate model, there must not remain a statistically significant These results support the use of PSA as a bridging endpoint to
treatment effect on survival when the model is adjusted for the determine survival benefit following AA treatment. Furthermore,
biomarker endpoint. Significant treatment effects were found this model-based analysis suggests that similar models may be
on survival in both chemotherapy-pretreated and -na€ve popu- useful for predicting the treatment effect of other prostate cancer
lations, consistent with previous analyses (7, 9). The current agents that exert their antitumor activity through PSA-dependent
analysis demonstrated a significant, similar treatment effect of mechanisms.
OF6 Clin Cancer Res; 2015 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on March 12, 2021. © 2015 American Association for Cancer
Research.Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Abiraterone PSA-Survival Model Predicts Survival Outcomes
Disclosure of Potential Conflicts of Interest Administrative, technical, or material support (i.e., reporting or organizing
C.J. Ryan reports receiving speakers bureau honoraria from Janssen. M.R. data, constructing databases): X.S. Xu, T.W. Griffin, I. Poggesi, P. Nandy
Smith is a consultant/advisory board member for Janssen. F. Saad is a consul- Study supervision: T.W. Griffin, I. Poggesi, P. Nandy
tant/advisory board member for and reports receiving a commercial research Other (provided clinical data and analysis): Y.C. Park
grant from Janssen. T.W. Griffin is an employee of Johnson and Johnson. No
potential conflicts of interest were disclosed by the other authors. Acknowledgments
The authors thank S. Thomas, of PAREXEL, for providing writing assistance,
which was funded by Janssen Global Services, LLC. ClinicalTrials.gov:
Authors' Contributions NCT00638690 and NCT00887198.
Conception and design: X.S. Xu, C.J. Ryan, M.R. Smith, F. Saad, T.W. Griffin,
P. Nandy
Development of methodology: X.S. Xu, C.J. Ryan, T.W. Griffin, A. Vermeulen, Grant Support
I. Poggesi, P. Nandy The analyses and studies described in this report were funded by Johnson &
Acquisition of data (provided animals, acquired and managed patients, Johnson Pharmaceutical Research & Development and Janssen Global Services,
provided facilities, etc.): X.S. Xu, C.J. Ryan, K. Stuyckens, F. Saad, T.W. Griffin LLC funded the writing support.
Analysis and interpretation of data (e.g., statistical analysis, biostatistics, The costs of publication of this article were defrayed in part by the payment of
computational analysis): X.S. Xu, C.J. Ryan, K. Stuyckens, M.R. Smith, F. Saad, page charges. This article must therefore be hereby marked advertisement in
T.W. Griffin, Y.C. Park, A. Vermeulen, I. Poggesi, P. Nandy accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Writing, review, and/or revision of the manuscript: X.S. Xu, C.J. Ryan,
K. Stuyckens, M.R. Smith, F. Saad, T.W. Griffin, M.K. Yu, A. Vermeulen, Received June 17, 2014; revised March 9, 2015; accepted March 11, 2015;
I. Poggesi, P. Nandy published OnlineFirst March 31, 2015.
References
1. Feldman BJ, Feldman D. The development of androgen-independent 14. Halabi S, Armstrong AJ, Sartor O, de BJ, Kaplan E, Lin CY, et al. Prostate-
prostate cancer. Nat Rev Cancer 2001;1:34–45. specific antigen changes as surrogate for overall survival in men with
2. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of metastatic castration-resistant prostate cancer treated with second-line
worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer chemotherapy. J Clin Oncol 2013;31:3944–50.
2010;127:2893–917. 15. Petrylak DP, Ankerst DP, Jiang CS, Tangen CM, Hussain MH, Lara PN Jr,
3. Attard G, Reid AH, A'Hern R, Parker C, Oommen NB, Folkerd E, et al. et al. Evaluation of prostate-specific antigen declines for surrogacy in
Selective inhibition of CYP17 with abiraterone acetate is highly active in the patients treated on SWOG 99-16. J Natl Cancer Inst 2006;98:516–21.
treatment of castration-resistant prostate cancer. J Clin Oncol 2009;27: 16. Hou X, Flaig TW. Redefining hormone sensitive disease in advanced
3742–8. prostate cancer. Adv Urol 2012;2012:978531.
4. Ryan CJ, Smith MR, Fong L, Rosenberg JE, Kantoff P, Raynaud F, et al. Phase 17. Kim J, Coetzee GA. Prostate specific antigen gene regulation by androgen
I clinical trial of the CYP17 inhibitor abiraterone acetate demonstrating receptor. J Cell Biochem 2004;93:233–41.
clinical activity in patients with castration-resistant prostate cancer who 18. Bruno R, Claret L. On the use of change in tumor size to predict survival in
received prior ketoconazole therapy. J Clin Oncol 2010;28:1481–8. clinical oncology studies: toward a new paradigm to design and evaluate
5. Ang JE, Olmos D, de Bono JS. CYP17 blockade by abiraterone: further phase II studies. Clin Pharmacol Ther 2009;86:136–8.
evidence for frequent continued hormone-dependence in castration-resis- 19. Bruno R, Lu JF, Sun YN, Claret L. A modeling and simulation framework to
tant prostate cancer. Br J Cancer 2009;100:671–5. support early clinical drug development decisions in oncology. J Clin
6. Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, et al. Phase I Pharmacol 2011;51:6–8.
clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms 20. Claret L, Girard P, O'Shaughnessy P, Hoff P, Van Cutsem E, Blum J, et al.
that castration-resistant prostate cancer commonly remains hormone Model-based predictions of expected anti-tumor response and survival in
driven. J Clin Oncol 2008;26:4563–71. phase III studies based on a phase II data of an investigational agent. J Clin
7. de Bono JS, Logothetis CJ, Molina A, Fizazi K, North S, Chu L, et al. Oncol 2006;24(18S):6025. suppl.; abstract
Abiraterone and increased survival in metastatic prostate cancer. N Engl J 21. Claret L, Girard P, Hoff PM, Van CE, Zuideveld KP, Jorga K, et al. Model-
Med 2011;364:1995–2005. based prediction of phase III overall survival in colorectal cancer on the
8. Fizazi K, Scher HI, Molina A, Logothetis CJ, Chi KN, Jones RJ, et al. basis of phase II tumor dynamics. J Clin Oncol 2009;27:4103–8.
Abiraterone acetate for treatment of metastatic castration-resistant prostate 22. Subtil F, Rabilloud M. Robust non-linear mixed modelling of longitudinal
cancer: final overall survival analysis of the COU-AA-301 randomised, PSA levels after prostate cancer treatment. Stat Med 2010;29:573–87.
double-blind, placebo-controlled phase 3 study. Lancet Oncol 2012;13: 23. Wang Y, Sung C, Dartois C, Ramchandani R, Booth BP, Rock E, et al.
983–92. Elucidation of relationship between tumor size and survival in non-small-
9. Ryan CJ, Smith MR, de Bono JS, Molina A, Logothetis CJ, de SP, et al. cell lung cancer patients can aid early decision making in clinical drug
Abiraterone in metastatic prostate cancer without previous chemotherapy. development. Clin Pharmacol Ther 2009;86:167–74.
N Engl J Med 2013;368:138–48. 24. Gomeni R, Merlo-Pich E. Bayesian modelling and ROC analysis to
10. Armstrong AJ, Eisenberger MA, Halabi S, Oudard S, Nanus DM, Petrylak predict placebo responders using clinical score measured in the initial
DP, et al. Biomarkers in the management and treatment of men with weeks of treatment in depression trials. Br J Clin Pharmacol 2007;
metastatic castration-resistant prostate cancer. Eur Urol 2012;61: 63:595–613.
549–59. 25. R Development Core Team. R: A language and environment for statistical
11. Collette L, Burzykowski T, Carroll KJ, Newling D, Morris T, Schroder FH. Is computing. In: The R foundation for statistical computing [Internet].
prostate-specific antigen a valid surrogate end point for survival in hor- [accessed Oct 8, 2013]. Available from: http://www.R-project.org/.
monally treated patients with metastatic prostate cancer? Joint research of 26. Prentice RL. Surrogate endpoints in clinical trials: definition and opera-
the European Organisation for Research and Treatment of Cancer, the tional criteria. Stat Med 1989;8:431–40.
Limburgs Universitair Centrum, and AstraZeneca Pharmaceuticals. J Clin 27. Armstrong AJ, Garrett-Mayer E, Ou Yang YC, Carducci MA, Tannock I, de
Oncol 2005;23:6139–48. WR, et al. Prostate-specific antigen and pain surrogacy analysis in meta-
12. Collette L, Burzykowski T, Schroder FH. Prostate-specific antigen (PSA) static hormone-refractory prostate cancer. J Clin Oncol 2007;25:3965–70.
alone is not an appropriate surrogate marker of long-term therapeutic 28. Bubley GJ, Carducci M, Dahut W, Dawson N, Daliani D, Eisenberger M,
benefit in prostate cancer trials. Eur J Cancer 2006;42:1344–50. et al. Eligibility and response guidelines for phase II clinical trials in
13. Collette L. Prostate-specific antigen (PSA) as a surrogate end point for androgen-independent prostate cancer: recommendations from the Pros-
survival in prostate cancer clinical trials. Eur Urol 2008;53:6–9. tate-Specific Antigen Working Group. J Clin Oncol 1999;17:3461–7.
www.aacrjournals.org Clin Cancer Res; 2015 OF7
Downloaded from clincancerres.aacrjournals.org on March 12, 2021. © 2015 American Association for Cancer
Research.Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Xu et al.
29. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Group Trials 9346 (Intergroup Study 0162) and 9916. J Clin Oncol
Design and end points of clinical trials for patients with progressive 2009;27:2450–6.
prostate cancer and castrate levels of testosterone: recommendations of 37. Sridhar SS, Freedland SJ, Gleave ME, Higano C, Mulders P, Parker C, et al.
the Prostate Cancer Clinical Trials Working Group. J Clin Oncol Castration-resistant prostate cancer: from new pathophysiology to new
2008;26:1148–59. treatment. Eur Urol 2014;65:289–99.
30. Schemper M. Predictive accuracy and explained variation. Stat Med 38. Burgio SL, Conteduca V, Rudnas B, Carrozza F, Campadelli E, Bianchi E,
2003;22:2299–308. et al. PSA flare with abiraterone in patients with metastatic castration-
31. Frances N, Claret L, Bruno R, Iliadis A. Tumor growth modeling from resistant prostate cancer. Clin Genitourin Cancer 2015;13:39–43.
clinical trials reveals synergistic anticancer effect of the capecitabine and 39. Parker C, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fossa SD, et al.
docetaxel combination in metastatic breast cancer. Cancer Chemother Alpha emitter radium-223 and survival in metastatic prostate cancer.
Pharmacol 2011;68:1413–9. N Engl J Med 2013;369:213–23.
32. Hu R, Dunn TA, Wei S, Isharwal S, Veltri RW, Humphreys E, et al. Ligand- 40. Scher HI, Fizazi K, Saad F, Taplin ME, Sternberg CN, Miller K, et al.
independent androgen receptor variants derived from splicing of cryptic Increased survival with enzalutamide in prostate cancer after chemother-
exons signify hormone-refractory prostate cancer. Cancer Res 2009;69: apy. N Engl J Med 2012;367:1187–97.
16–22. 41. Morris MJ, Molina A, Small EJ, de Bono JS, Logothetis CJ, Fizazi K, et al.
33. Panel on Handling Missing Data in Clinical Trials, National Research Radiographic progression-free survival as a response biomarker in meta-
Council. The prevention and treatment of missing data in clinical trials. static castration-resistant prostate cancer: COU-AA-302 results. J Clin
Washington, DC: National Academies Press; 2010. Oncol 2015:1348–55.
34. Proust-Lima C, Taylor JM. Development and validation of a dynamic 42. Ryan CJ, Morris M, Molina A, Piulats JM, De Souza P, Li J, et al. Association
prognostic tool for prostate cancer recurrence using repeated measures of of radiographic progression-free survival (rPFS) adapted from Prostate
posttreatment PSA: a joint modeling approach. Biostatistics 2009;10: Cancer Working Group 2 (PCWG2) consensus criteria (APCWG2) with
535–49. overall survival (OS) in patients (pts) with metastatic castration-resistant
35. Stein WD, Gulley JL, Schlom J, Madan RA, Dahut W, Figg WD, et al. Tumor prostate cancer (mCRPC): Results from COU-AA-302. Ann Oncol 2012;23
regression and growth rates determined in five intramural NCI prostate (suppl 9).
cancer trials: the growth rate constant as an indicator of therapeutic efficacy. 43. Sonpavde G, Pond GR, Armstrong AJ, Galsky MD, Leopold L, Wood BA,
Clin Cancer Res 2011;17:907–17. et al. Radiographic progression by Prostate Cancer Working Group
36. Hussain M, Goldman B, Tangen C, Higano CS, Petrylak DP, Wilding G, (PCWG)-2 criteria as an intermediate endpoint for drug development
et al. Prostate-specific antigen progression predicts overall survival in in metastatic castration-resistant prostate cancer. BJU Int 2014;114:
patients with metastatic prostate cancer: data from Southwest Oncology E25–31.
OF8 Clin Cancer Res; 2015 Clinical Cancer Research
Downloaded from clincancerres.aacrjournals.org on March 12, 2021. © 2015 American Association for Cancer
Research.Published OnlineFirst March 31, 2015; DOI: 10.1158/1078-0432.CCR-14-1549
Correlation between Prostate-Specific Antigen Kinetics and
Overall Survival in Abiraterone Acetate−Treated
Castration-Resistant Prostate Cancer Patients
Xu S. Xu, Charles J. Ryan, Kim Stuyckens, et al.
Clin Cancer Res Published OnlineFirst March 31, 2015.
Updated version Access the most recent version of this article at:
doi:10.1158/1078-0432.CCR-14-1549
Supplementary Access the most recent supplemental material at:
Material http://clincancerres.aacrjournals.org/content/suppl/2015/04/01/1078-0432.CCR-14-1549.DC1
E-mail alerts Sign up to receive free email-alerts related to this article or journal.
Reprints and To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Subscriptions Department at pubs@aacr.org.
Permissions To request permission to re-use all or part of this article, use this link
http://clincancerres.aacrjournals.org/content/early/2015/05/28/1078-0432.CCR-14-1549.
Click on "Request Permissions" which will take you to the Copyright Clearance Center's
(CCC)
Rightslink site.
Downloaded from clincancerres.aacrjournals.org on March 12, 2021. © 2015 American Association for Cancer
Research.You can also read

















































